President Trump declared a national emergency today, in response to the growing spread of coronavirus across the country. The administration had come under sharp criticism for its sluggish response to the coronavirus crisis, in particular the widespread shortage of tests. Dr. Antony Fauci, director of the National Institute of Health’s infectious disease branch, told Congress on Thursday that the government’s response on testing was “not really geared to what we need right now…That’s a failing. Let’s admit it.”
In response, the administration today announced a series of emergency steps to increase testing capacity, turning to private labs to support the effort. The emergency status frees up $50B in federal emergency funding. Trump also announced that the Health and Human Services (HHS) Secretary will be able to waive regulations around telemedicine licensing, critical access hospital bed requirements and length of stay, and other measures to provide hospitals with added flexibility. House Speaker Nancy Pelosi and Treasury Secretary Steven Mnuchin have negotiated a sweeping aid package that would strengthen safety net programs, and offer sick leave for American workers affected by the virus.
Meanwhile, the American economy likely entered a recession, as consumers continued to pull back on spending on airline travel, entertainment, and other discretionary areas, while financial markets experienced the worst one-day drop in more than 30 years. Many school districts and universities shut down and announced plans to convert to online instruction for the foreseeable future. Employers imposed broad travel restrictions on their employees, moved to teleworking where possible, and even began to lay off workers as demand for services cratered. Shoppers stocked up on staples, cleaning supplies, and (inexplicably) toilet paper, as shelves ran bare in many stores.
Epidemiologists and disease experts urged broad adoption of “social distancing”, restricting large gatherings and reducing the ability of the virus to spread person-to-person. The objective: “flattening the curve” of transmission, so that the healthcare delivery system does not become overwhelmed as the virus spreads exponentially.
Income inequality has become a central topic in our national political debate in the wake of the financial crisis. The gap between the “haves” and “have nots” has grown steadily, and addressing that gap has become a key priority for a new generation of politicians, economists, and policymakers. But inequality has also become a lucrative business opportunity in many parts of the economy, a phenomenon that New York Times economics reporter Nelson Schwartz entertainingly (and unsettlingly) describes in his new book, The Velvet Rope Economy: How Inequality Became Big Business.
Based on a series of Times articles by Schwartz from the past several years, the book describes life on both sides of the “velvet rope”: how services have become faster, better, and higher quality for those with the ability to pay extra, and how the rest of us are getting left behind. He describes how the familiar amusement-park “Fast Pass” approach has pervaded other parts of our lives, from school sports to social services to travel, and yes, to healthcare.
Across the economy, businesses increasingly cater to the top tier of customers, providing privileged access, concierge services, and special perks. As Schwartz describes it, “This pattern—a Versailles-like world of pampering for a privileged few on one side of the velvet rope, a mad scramble for basic service for everyone else—is being repeated in one sphere of American society after another.”
It’s a phenomenon we see in healthcare every day, as rural hospitals are shuttered, access to care is restricted for Medicaid patients, and wait times for new primary care appointments soar to six weeks or more, while concierge physician practices and cash-based, on-demand services proliferate. Most troubling, in Schwartz’s view: this intentional, class-based separation causes those on one side of the “velvet rope” to misunderstand, and even denigrate, those on the other.
That aptly describes our current political dynamic—Schwartz provides a useful (and highly readable) window into how businesses seek to profit from that division. Worth a read.
Republicans and Democrats alike are warning that a recent proposal from the Trump administration could lead to billions of dollars in cuts to Medicaid, forcing states to eliminate benefits, reduce enrollment or cut payments to health providers.
In a rare sign of unity, hospitals, insurers, patient advocates and members of both political parties are on the same page in their opposition to the Trump administration’s plan, and most have urged the administration to withdraw a proposal they say would “cripple” Medicaid, the federal-state partnership that provides health care for the poor.
The proposal hasn’t received as much attention as the administration’s other efforts to reform Medicaid, such as implementing work requirements, but it could have the most damaging effect because of how far-reaching it is, experts argue.
“This is high stakes,” said Matt Salo, executive director of the National Association of Medicaid Directors, whose board urged the administration to completely withdraw the proposal.
Trump allies have also voiced their concerns.
“The Medicaid fiscal accountability rule is a concern to my governor, and the stakeholders are worried the rule as proposed could lead to hospital closures, problems with access to care and threaten the safety net,” Sen. John Cornyn (R-Texas) told Department of Health and Human Services Secretary Alex Azar last week during a hearing on the agency’s fiscal 2021 budget request.
Sen. Mark Warner (D-Va.) warned during the same hearing that the proposal could “dramatically affect Medicaid eligibility” and “wreak havoc on budgets in red states and blue states all across the country.”
The proposal would overhaul the complex payment arrangements states use to raise money for their Medicaid programs — funding that is then matched by the federal government.
The administration argues some states use questionable methods of raising funds so they can leverage more money from Washington. One approach used by states consists of taxing providers who stand to benefit from more Medicaid funds flowing into the state.
But governors and state Medicaid directors argue those long-standing arrangements are both legal and necessary as states look for ways to keep up with escalating health care costs.
The proposal would allow the Centers for Medicare and Medicaid Services (CMS) to limit the extra payments from states to providers serving high numbers of uninsured patients or Medicaid patients. Opponents say such changes could result in providers deciding not to accept Medicaid patients.
Dozens of states wrote public comments to CMS Administrator Seema Verma, urging her to withdraw the proposal, including conservative states that are typically supportive of her work.
“If the rule is finalized as proposed, it will immediately disrupt the Medicaid program in Alabama and we believe across the country,” wrote Stephanie McGee Azar, commissioner of the Alabama Medicaid Agency, who is not related to Alex Azar. She added that it would have “unintended consequences that will affect access to care in Alabama to our most vulnerable populations.”
Florida Gov. Ron DeSantis’s (R) administration warned the effect of the proposal would be “immediate and crippling.”
Meanwhile, a letter signed by state Medicaid officials in Michigan, Missouri, New York, Oregon, Pennsylvania, South Carolina, Tennessee, Illinois, Louisiana, Colorado, Pennsylvania and Washington argued the proposal would likely “force states to cut Medicaid eligibility, benefits and/or provider payments, which would have the effect of decreasing low-income individuals’ access to important health care services.”
The public comment period closed Jan. 31. CMS now needs to go through the 4,000 comments before deciding whether to finalize the rule.
Verma and her supporters argue the proposal is not intended to cut Medicaid but instead aims to improve transparency and accountability in the $600 billion a year program.
“It’s not surprising providers and the states are objecting when they are getting federal money for free,” argued Brian Blase, who previously served on President Trump’s National Economic Council, where he worked on health care issues. “They don’t want transparency and they don’t want their financing gimmicks checked.”
Blase predicted the rule, if implemented as proposed, would reduce Medicaid spending by a “very small amount.”
Verma also pushed back on opponents, criticizing a study commissioned by the American Hospital Association that estimated the rule could reduce Medicaid funding by as much as $49 billion annually.
“This proposed rule is not intended to reduce Medicaid payments, and alarmist estimates that this rule, if finalized, will suddenly remove billions of dollars from the program and threaten beneficiary access are overblown and without credibility,” she wrote in a blog post last week.
Some experts disagree with her, pointing to other actions the administration has taken on Medicaid, including work requirements.
“I think one should view this rule not in isolation, but in combination with the broader agenda of this administration on Medicaid,” said Edwin Park, a research professor at Georgetown University McCourt School of Public Policy. “Their ultimate agenda is about cutting the Medicaid program, changing the Medicaid program as it currently stands.”
State officials have complained that they were not asked for their input before the proposal was released, nor did CMS conduct a regulatory analysis of potential effects.
A nonpartisan agency that advises Congress on Medicaid policy wrote to Alex Azar advising he not implement the rule because CMS has not fully assessed the possible effects.
“The Commission is concerned that the proposed changes could reduce payments to providers in ways that could jeopardize access to care for Medicaid enrollees,” the advisory group wrote.
For example, Maine’s Department of Health and Human Services has planned to make $86 million in supplemental payments to hospitals in fiscal 2020, which began July 1.
The rule “would require significant changes to MaineCare and could force the State to cut back on eligibility or services,” Jeanne Lambrew wrote in the department’s public comment.
The administration hasn’t given any signals that it plans to back down from the proposal, despite considerable pushback from stakeholders, states and bipartisan members of Congress.
“We will work with states to help them recreate their practices in ways that are in conformity with the statute and try to be fair and equitable in all our dealings with states,” Alex Azar told lawmakers last week on Capitol Hill.
Hospitals in the 340B drug discount program spent more on drugs for prostate and lung cancers compared to facilities not in the program, a new analysis found.
But the preliminary analysis from the Medicare Payment Advisory Commission (MedPAC) couldn’t find that the controversial program incentivizes hospitals to pursue higher-priced drugs. The analysis, released Friday as part of MedPAC’s monthly meeting, was requested by Congress on the program, which has faced major cuts by the Trump administration.
Some lawmakers have argued that 340B, which offers safety-net hospitals discounts on drugs, has not worked as intended and led to hospitals specifically choosing higher-priced drugs to get a big discount.
So MedPAC looked at the spending from 2013 to 2017 of 340B and non-340B hospitals as well as physicians’ offices for five types of cancers: breast, colorectal, prostate, lung and leukemia and lymphoma.
MedPAC’s analysis found that 340B hospitals spent between 2% and 5% higher on average on cancer drugs than non-340B hospitals. But there were mixed results when 340B hospitals were compared to physicians’ offices, with 340B facilities spending 1% lower to 7% higher than physicians’ offices on cancer drugs.
The reason 340B hospitals spent more on cancer drugs than hospitals not in the program was linked to two types of cancer: lung and prostate.
For lung cancer, a possible reason for the higher spending is that a larger share of patients in 340B hospitals received new immuno-oncology therapies that are more expensive, MedPAC said. Prostate cancer also had higher drug prices per unit for both drugs in Medicare Part B, which reimburses for physician-administered drugs, and Part D.
However, MedPAC staff cautioned they couldn’t conclude 340B is incentivizing the spikes in spending.
The reason is “we lack access to the discount data,” said MedPAC staffer Shinobu Suzuki at the commission’s meeting Friday in Washington, D.C.
MedPAC also didn’t find that gaining 340B status led to a spike in average cancer drug spending, suggesting that 340B discounts “may not have had any effects on them,” the report said.
The analysis also found that the higher cancer spending would likely have a small, if any, impact on cost sharing for Medicare patients depending on the type of cancer and supplemental coverage.
The study will be finalized and likely included in MedPAC’s March report to Congress. It comes with some caveats, including a small sample size and that it did not examine the impact of a 22.5% cut to 340B payments that went into effect in 2018.
The hospital industry has been fighting the Trump administration in court over the cuts, which the industry claims are unlawful.
Despite the caveats, MedPAC’s findings could play a major part in lawmaker deliberations on the program, which some Republicans claim has gotten too big and led to hospitals bilking the federal government.
The pharmaceutical industry has also led an extensive campaign to shed more light on the program. 340B requires pharmaceutical companies to provide discounts to safety-net hospitals in exchange for participating in Medicaid.
340B industry group 340B Health praised the findings.
“The thoughtful analysis MedPAC presented today sheds important light on the role 340B hospitals play in treating people living with cancer,” said Maureen Testoni, 340B Health president, in a statement.
Yesterday, a three-judge panel from the Fifth Circuit Court of Appeals struck down the Affordable Care Act (ACA)’s individual mandate. The judges agreed with a lower court decision issued in the case, Texas v. U.S., in December 2018 that the individual mandate is unconstitutional but, unlike the lower court, did not decide that the rest of the ACA is also unconstitutional. Instead, the judges remanded, or sent back, the decision to the same lower court judge to consider. California Attorney General Xavier Becerra, who is leading the 21 Democratic state attorneys general defending the law, along with the U.S. House of Representatives, immediately announced he would appeal the decision to the Supreme Court.
Whether the Supreme Court will decide to take the case now or wait for the decision of Judge O’Connor’s, of the lower court, is uncertain. If the Court decides to take the case now, they could expedite the briefing process and issue a decision in 2020. If it does not take the case now, a ruling will be delayed until after the 2020 presidential election.
No one knows how the Supreme Court will ultimately rule. But we do know that if the Court decides to strike down the ACA, the human toll will be immense and tragic. The law has granted unprecedented health security to millions:
18.2 million formerly uninsured people have gained coverage since 2010
53.8 million Americans with preexisting health conditions are now protected
12.7 million low-income people are insured through expanded Medicaid
10.6 million people have coverage through the ACA marketplaces, 9.3 million of whom receive tax credits to help them pay their premiums
5.5 million young adults have gained coverage, many by staying on their parents’ plans
45 million Medicare beneficiaries have much better drug coverage.
Such a decision will also trigger massive disruption throughout the U.S. health system. The health care industry represents nearly 20 percent of the nation’s economy; the ACA has touched every corner of it. The law restructured the individual and small-group health insurance markets, expanded and streamlined the Medicaid program, improved Medicare benefits, and reformed the way Medicare pays doctors, hospitals, and other providers. It was a catalyst for the movement toward value-based care and established a regulatory pathway for biosimilars — less expensive versions of biologic drugs. States have rewritten laws to incorporate the ACA’s provisions. Insurers, hospitals, physicians, and state and local governments have invested billions of dollars in adjusting to these changes.
The law’s popular preexisting health condition protections have made it possible for people with minor-to-serious health problems to apply for coverage in the same way healthier people have always done. These protections have given the estimated 53.8 million Americans with preexisting health conditions the peace of mind that they will never be denied health insurance because of their health.
More than 150 million people who get coverage through their employers now are eligible for free preventive care, and their children can stay on their policies to age 26.
The wide racial and income inequities in health insurance coverage that have been partly remedied by the ACA would return. Hospitals and providers, especially safety-net institutions, would struggle with mounting uncompensated care burdens and sicker and more costly patients who are not receiving the preventive care they need.
The ACA tore down financial barriers to health care for millions, many of whom were uninsured for most of their lives. It has demonstrably helped people get the health care they need in states across the country. Research indicates that Medicaid expansion has led to improved health status and lower mortality risk.
To date, neither the Trump administration, which has sided with the plaintiffs in the case, nor its Republican colleagues in Congress have offered a replacement plan in the event the law is struck down. The historic progress made by Americans, particularly those with middle and lower incomes and people of color, could unravel. Voters are already telling policymakers they are worried about their ability to afford health care. Yesterday’s decision and the uncertain path forward to the Supreme Court is certain to escalate those worries. With the nation entering the 2020 presidential election year, the Supreme Court may decide to take up the case this term.
UPDATE: Nov. 13, 2019: This brief has been updated to include comments from provider groups.
Dive Brief:
CMS proposed a new rule Tuesday that would establish stricter requirements for states to report information on supplemental Medicaid payments to providers in a bid to clamp down on spending and promote transparency.
The agency will also soon release guidance on how states can test alternative financing approaches in the safety net program like block grant and per-capita cap proposals for “certain optional adult populations,” CMS Administrator Seema Verma said Tuesday at the National Association of Medicaid Director’s annual conference in Washington, D.C.
Later this year, CMS will also issue guidance on how states can promote value-based payments and social determinants of health factors in Medicaid, Verma said. The Center for Medicare and Medicaid Innovation is currently developing several new payment models to push providers to take on more risk for their patient populations in those programs.
Dive Insight:
The moves are in line with sweeping changes from the Trump administration moving more power to the states and asking more from recipients. The CMS administrator teased late last month the agency would soon release new guidance for states to inject flexibility into their Medicaid programs.
“We shouldn’t ration care but instead make how we pay for care more rational,” Verma said Tuesday. “Medicaid must move toward value-based care.”
Speaking to the Medicaid directors Tuesday, Verma said the changes are aimed preserving Medicaid for future generations.
“Going forward there will be no new [State Innovation Model] grants, no more open-ended one-off district waivers,” she said. “We must move forward with a more unified, cohesive approach across payers, across CMS, across states.”
The proposed rule, called Medicaid Fiscal Accountability (MFAR), will add more scrutiny to supplemental payments, which are Medicaid payments to providers in addition to medical services rendered to Medicaid beneficiaries, such as payments supporting quality initiatives or bolstering rural or safety net providers.
Some states rely heavily on these additional payments to offset low Medicaid reimbursement or support struggling hospitals. Provider lobbies did not take kindly to the new rule.
“We share the government’s desire to protect patients and taxpayers with transparency in federal programs, but today’s proposal oversteps this goal with deeply damaging policies that would harm the healthcare safety net and erode state flexibility,” Beth Fledpush, SVP of policy and advocacy for America’s Essential Hospitals, said in a statement.
AEH, which includes more than 300 member hospital and health systems, many of which are safety net providers, asked CMS to withdraw the proposal. The American Hospital Association told Healthcare Dive it was still reviewing the rule and declined comment.
However, government oversight agencies like the Government Accountability Office and the Office of Inspector General have recommended changes to these payments, which have increased from 9.4% of Medicaid payments in 2010 to 17.5% in 2017, according to CMS.
MFAR would also propose new definitions for “base” and “supplemental” payments in order to better enforce statutory requirements around and eliminate vulnerabilities in program spending.
Verma has long teased CMS support of block grants, an idea popular with conservatives, but Tuesday’s speech solidifies the agency’s support of such proposals. A handful of red states have been mulling over capped spending to gain more clarity around budgets.
In September, Tennessee unveiled its plan to move to a block grant system that would set a floor for federal contributions adjusted on a per capita basis if enrollment grows. Any savings would be shared between the state and the government.
Tennessee must submit a formal application to CMS to later than Nov. 20. If approved, it would become the first state to use a block grant funding mechanism in Medicaid. Additionally, Utah submitted a waiver application seeking per-capita Medicaid caps in June; Oklahoma Gov. Kevin Stitt, a Republican, is reportedly considering such a program; and Alaska and Texas have both commissioned block grant studies.
The Trump administration finalized a hospital payment rule Friday that retains proposed cuts to off-campus clinics and the 340B drug discount program.
The changes outlined in the hospital Outpatient Prospective Payment System (OPPS) rule come despite both cuts being struck down in legal challenges and amid major pushback from providers.
Site-neutral payments
The agency decided to move ahead with the two-year phase-in of the cuts to outpatient services for clinic visits furnished in an off-campus hospital outpatient setting. The goal is to bring payments to off-campus clinics in line with standalone physicians’ offices.
“With the completion of the two-year phase-in, the cost sharing will be reduced to $9, saving beneficiaries an average of $14 each time they visit an off-campus department for a clinic visit in [calendar year] 2020,” the Centers for Medicare & Medicaid Services (CMS) said in a fact sheet.
However, the two-year project that was supposed to start in 2019 has been halted because of a federal court ruling.
CMS decided to move forward with the cuts for off-campus clinics.
“The government has appeal rights, and is still evaluating the rulings and considering, at the time of this writing, whether to appeal the final judgment,” the agency said.
The American Hospital Association (AHA) said that the site-neutral payment rule was misguided and that CMS ignored the recent court ruling.
“There are many real and crucial differences between hospital outpatient departments and the patient populations they serve and other sites of care,” said Tom Nickels, executive vice president of the AHA, in a statement.
CMS also finalized a proposed cut for the 340B program that cuts payments by 22.5% in 2020.
CMS has installed prior cuts in 2018 and 2019 to the program that requires drug companies to provide discounts to safety-net hospitals in exchange for getting their products covered on Medicaid.
However, a court ruling has struck down the cuts, and CMS is currently appealing the decision.
CMS said that it hopes to conduct a 340B hospital survey to collect drug acquisition cost data for 2018 and 2019, and the survey will craft a remedy if the appeal doesn’t go their way.
“In the event the 340B hospital survey data are not used to devise a remedy, we intend to consider the public input to inform the steps we would take to propose a remedy for CYs 2018 and 2019 in the CY 2021 rulemaking,” the agency said.
Hospital groups commented that CMS should drop both the 340B and site-neutral cuts because of the legal challenges.
Several groups weren’t happy that the cuts were still there.
“The agency also prolongs confusion and uncertainty for hospitals by maintaining unlawful policies it has been told to abandon in clear judicial directives,” said Beth Feldpush, senior vice president of policy and advocacy for America’s Essential Hospitals, in a statement Friday.
The hospital-backed group 340B Health added that CMS needs to stop this “unfunny version of ‘Groundhog Day’ and restore Medicare payments for 340B hospitals to their legal, statutory level.”
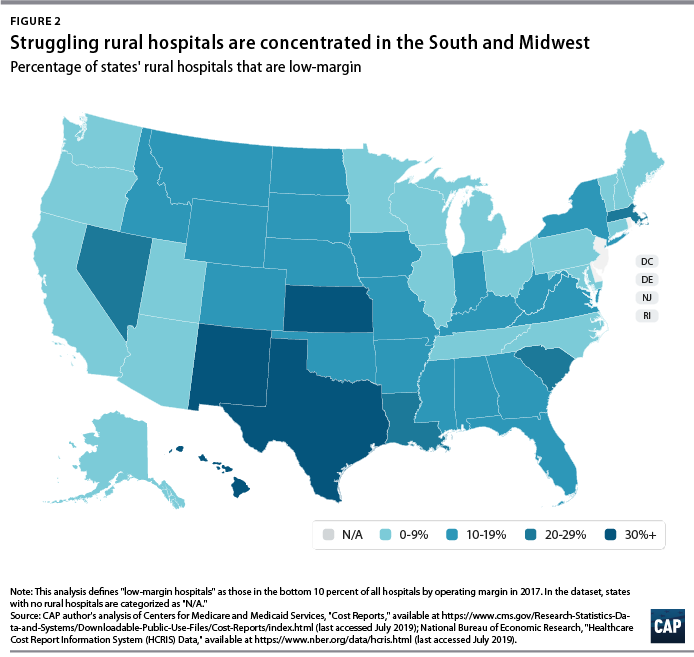
The number of rural hospital closures in the United States has increased over the past decade.1 Since 2010, 113 rural hospitals,2 predominantly in Southern states, have closed. This is a concerning trend, since hospital closures reduce rural communities’ access to inpatient services and emergency care.3 In addition, hospitals that are at risk financially are more likely to serve rural communities with higher proportions of vulnerable populations.4
Understanding the financial pressures facing rural hospitals is imperative to ensuring that America’s 60 million rural residents have access to emergency care.5 Rural hospitals are generally less profitable than urban ones, and those with the lowest operating margins maintain fewer beds and have lower occupancy rates. Low-margin rural hospitals are also more likely to be in states that have not expanded Medicaid under the Affordable Care Act (ACA). According to new analysis by the Center for American Progress, future hospital closures would reduce rural Americans’ proximity to emergency treatment. Among low-margin, rural hospitals—those most likely to close—the majority of those with emergency departments are at least 20 miles away from the next-closest emergency department.
This report first discusses the role that hospitals and emergency care play in rural health care as well as trends in hospital closures. It then uses federal data to examine differences in the financial viability of rural and urban hospitals and the availability of hospital-based emergency care in rural areas. The final section of this report offers policy recommendations to improve health care access and emergency care for rural residents.
Rural hospitals have been closing at an unprecedented rate
From 2013 to 2017, rural hospitals closed at a rate nearly double that of the previous five years.6 (See Figure 1) According to the Government Accountability Office (GAO), recent rural hospital closures have disproportionately occurred among for-profit and Southern hospitals. Southern states accounted for 77 percent of rural hospital closures over that time period but only 38 percent of all rural hospitals in 20137
Hospital closures may deepen existing disparities in access to emergency care. Closures are more likely to affect communities that are rural, low income, and home to more racial/ethnic minority residents.8 Although about half of acute care hospitals are located in rural communities and the other half are located in urban areas,9 rural residents live 10.5 miles from the nearest acute care hospital on average, compared with 4.4 miles for those in urban areas.10 According to a poll by the Pew Research Center, about one-quarter (23 percent) of rural residents said that “access to good doctors and hospitals” is a problem in their community, while only 18 percent of urban residents and 9 percent of suburban residents said it was a problem.11
A variety of factors influence hospitals’ sustainability. Thanks to medical and technological advances, conditions that once required hospitalization can now be treated in an ambulatory care center or a physician’s office. University of Pennsylvania professor and CAP nonresident senior fellow Ezekiel Emanuel has argued that one reason hospitals are closing is that “more complex care can safely and effectively be provided elsewhere, and that’s good news.”12 As a whole, the hospital industry remains highly profitable, and hospital margins are at their highest in decades.13
Evidence on the relationship between hospital closures and health outcomes is mixed. A 2015 study of nearly 200 hospital closures in Health Affairs found no significant changes in hospitalization rates or mortality in the affected communities, whether rural or urban.14 More recent studies have found an association between rural hospital closures and increased mortality. Harvard researcher Caitlin Carroll showed that rural hospital closures led to an overall increase in mortality rates for time-sensitive health conditions,15 and Kritee Gujral and Anirban Basu of the University of Washington found that rural hospital closures in California were followed by increases in mortality for inpatient stays.16
In rural areas, hospitals face additional challenges to their viability, including lower patient volumes; higher rates of uncompensated care; and physician shortages.17 In addition, rural patients tend to be older and lower income.18 Rural hospitals tend to be smaller, serve a higher share of Medicare patients, and have lower occupancy rates than urban hospitals.19 Rural hospitals commonly offer obstetrics, imaging and diagnostic services, emergency departments, as well as hospice and home care,20 but patients needing more complicated treatment are often referred to tertiary or specialized hospitals. In fact, rural patients are more likely to be transferred to another hospital than patients at urban hospitals.21
Most urban hospitals are reimbursed under the prospective payment systems (PPS) for Parts A and B of Medicare. Through both the inpatient and outpatient PPS, the Centers for Medicare and Medicaid Services (CMS) reimburse hospitals at a predetermined amount based on diagnoses, with adjustments—including those for local input costs and patient characteristics.22However, rural hospitals often face higher costs due to lower occupancy rates and provide care to a higher percentage of patients covered by Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). Such hospitals may be eligible to receive higher payments from Medicare if they qualify as a Sole Community Hospital (SCH) or Medicare-Dependent Hospital (MDH).23
Another form of financial relief for rural hospitals is obtaining designation as a Critical Access Hospital (CAH), which Medicare reimburses based on cost rather than on the PPS.24 To qualify as a CAH, a hospital must provide 24/7 emergency services; maintain no more than 25 beds; and serve a rural area that is 35 miles from another hospital.25 Medicare reimburses CAHs at 101 percent of reasonable costs, rather than through the inpatient and outpatient PPS structures.26 As of 2018, there were 1,380 CAHs nationwide,27 accounting for about two-thirds of all rural hospitals.28
Even with cost-based reimbursement, however, some CAHs are unable to sustain the costs required to maintain inpatient beds.29 The 25-bed limit for CAHs prevent participating hospitals from eliminating inpatient services and restrict their ability to expand in response to fluctuations in community populations or care volumes. Other challenges facing rural hospitals include lacking sufficient patient volume to maintain high-quality performance for certain procedures and pressure to drop high-value but poorly reimbursed services such as obstetrics while maintaining low-volume, high profit services such as joint replacement procedures. 30
A key way that states can support struggling rural hospitals is by expanding Medicaid under the ACA. Expanding Medicaid increases coverage among low-income adults, 31 which in turn reduces uncompensated care costs for hospitals32 and allows financially vulnerable hospitals to improve their viability.33 Consistent with other recent studies,34 the GAO concluded in a 2018 report on rural hospitals that those “located in states that increased Medicaid eligibility and enrollment experienced fewer closures.”35
Rural hospitals are cutting back on services
Rural hospitals in different states have responded to financial pressures in a variety of ways, trying to balance community needs with financial viability. For many hospitals this has meant cutting inpatient obstetric services, leaving more than half of rural counties without hospital obstetric services.36 For instance, in Wisconsin, falling birth rates led to 12 hospitals in the state closing their obstetric services in the past decade.37 In Grantsburg, Wisconsin, lower birth rates and an older community population led Burnett Medical Center to shut down its obstetrics services.38 In order to offer these services, Burnett Medical Center would have needed to keep a general surgeon on call to perform caesarean sections, and with just 40 deliveries in 2017, the hospital could not justify the expense.39 While the hospital will continue providing prenatal and postnatal care, it will refer patients to a facility in Minnesota for deliveries—a facility is almost 40 minutes away.40
In other communities, hospitals have been replaced by other types of health care facilities. For example, Appalachian Regional Healthcare System closed Blowing Rock Hospital in North Carolina in 2013. Three years later, it opened a 112-bed post-acute care center in Blowing Rock in response to demand for rehabilitation services and the aging population in the surrounding area.41
Financial data shows that rural hospitals are more likely to struggle
To compare the financial situations of rural and urban hospitals and examine how future rural hospital closures could affect the availability of emergency care, CAP analyzed data from the CMS Healthcare Cost Report Information System (HCRIS). The CMS requires all Medicare-certified hospitals to report their financial information annually. CAP used the HCRIS to examine the financial margins and other characteristics of 4,147 acute care hospitals for fiscal year 2017. Of these, 1,954 hospitals (47 percent) were in rural areas, while the remaining were in urban areas. Hospitals self-report their status in the HCRIS as either urban or rural, which the CMS defines as either inside or outside of a metropolitan statistical area, respectively.42 Further information about CAP’s hospital sample can be found in the Methodological appendix.
Hospital operating margins, which measure excess patient-related revenues relative to patient-related expenses, are often used as an indicator of financial health.43 A 2011 study by Harvard researchers Dan Ly, Ashish Jha, and Arnold Epstein found that the lowest 10 percent of hospitals by operating margin were 9.5 times more likely to close within two years compared to all others. 44 The same study concluded that hospitals with low operating margins were also more likely to be acquired or merge.45
In CAP’s hospital sample, the median operating margin was negative 2.6 percent among all hospitals, negative 0.1 percent for urban hospitals, and negative 4.9 percent for rural hospitals.46 Public hospitals and MDHs in the sample were more likely to have negative operating margins, consistent with what other studies have found.47 To analyze hospitals’ relative financial health across geographic areas, CAP ranked hospitals in the HCRIS sample based on operating margin, splitting them into three groups: the lowest 10 percent, the middle 80 percent, and the highest 10 percent. The range of operating margins for each group is shown in Table 1.
Rural hospitals are less likely to be financially healthy than urban hospitals. In 2017, rural hospitals comprised only 27.9 percent of the hospitals with operating margins in the highest decile but comprised 59.7 percent of the hospitals in the lowest decile. Southern and Midwestern states had the greatest proportion of rural hospitals with low operating margins, mimicking the geographic patterns in hospital closures that the GAO report identified. CAP finds that from 2015 through 2017, rural hospitals were consistently more likely than urban hospitals to fall in the bottom 10 percent of operating margins. CAP’s analysis also confirms that rural hospitals in states that expanded Medicaid had a higher median operating margin (negative 3.4 percent) than those in states that have not expanded Medicaid (negative 5.7 percent).
To examine commonalities among the hospitals most vulnerable to closure, CAP analyzed characteristics of the hospitals with low margins, defined as having an operating margin in the lowest 10 percent among all hospitals. Smaller, low-occupancy rural hospitals were most likely to struggle financially: nearly 1 in 6 (15 percent) of hospitals with 25 or fewer beds had low margins, and nearly one-fifth (17 percent) of hospitals with low-occupancy rates had low margins. (See Figure 3)
Emergency departments are on the front lines for rural health
In some emergency situations, hospital closures can be life-threatening, increasing the time and distance patients travel to receive care. Studies show that the probability of dying from a heart attack increases with distance from emergency care,48 and traumatic injuries are more likely to be fatal for rural residents than for urban ones.49
Rural residents are more likely than urban residents to visit the emergency department.50 A shortage of primary care providers; lack of public transportation infrastructure; shortages in preventive care; higher rates of smoking and obesity; and greater prevalence of chronic disease in rural areas all contribute to the greater utilization of emergency room care.51 As a result, emergency departments often stand in as the main source of care for vulnerable and low-income populations, especially for communities that face a shortage of primary care. 52 Among the dozens of rural hospitals that have closed in recent years, some served as the only emergency department in a community, according to MedPAC53
While freestanding emergency departments have proliferated,54 they are not filling the gap for rural emergency care. MedPAC found that, as of 2016, nearly all the country’s 566 stand-alone emergency departments were in urban areas and tended to be located in more affluent communities.55 Researchers at the North Carolina Rural Health Research Program found that the freestanding emergency department model was generally not viable in rural areas of the state due to low patient volumes, high rates of uninsured patients, and provider shortages.56 One limit on the growth of independent freestanding emergency centers is that they are not recognized in Medicare law and are therefore unable to bill the program, unlike hospital-affiliated off-campus emergency departments. 57
Future rural hospital closures would increase the distances that patients travel for emergencies
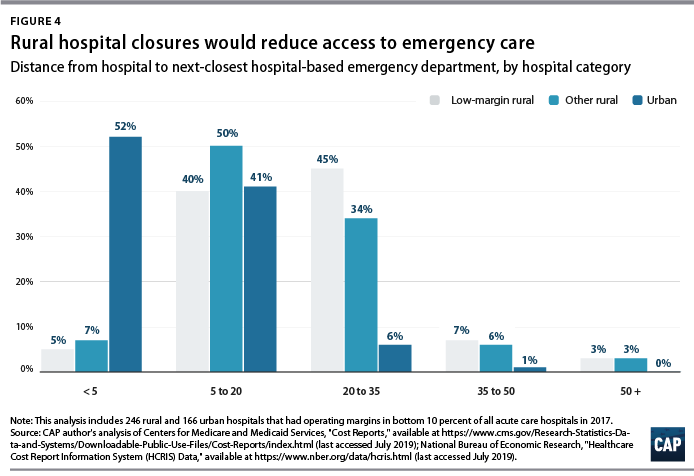
To better understand how future rural hospital closures could affect access to emergency care, CAP calculated hospitals’ distance to the next-closest hospital-based emergency department. CAP restricted its 2017 HCRIS data sample to the 3,616 acute care hospitals that provide 24-hour emergency services.58 Using addresses or coordinates provided in the HCRIS, CAP mapped each low-margin rural hospital to the next-closest hospital emergency department. Mapping strategies are detailed in the Methodological appendix.
Among the 222 low-margin rural hospitals, more than half (55 percent) were more than 20 miles away from the next-closest hospital-based emergency department, and one-tenth were more than 35 miles away. (See Figure 4). The average distance to the next-closest emergency department was 22 miles.
The disappearance of rural, low-margin hospitals would greatly increase patients’ travel distances for emergency care. Without other resources to fill the gap, some patients might forgo care they need and others would be forced to undertake an even longer journey to receive medical attention.
Policies to improve rural emergency and nonemergency care
As rural hospitals continue to close, it is crucial to preserve access to emergency care for rural Americans. The following section details a series of policy recommendations to support adequate emergency care and address care shortages in rural communities.
Expand Medicaid
Experience to date suggests that rural hospitals in those states that have not yet expanded their Medicaid programs under the ACA would benefit from Medicaid expansion through lower levels of uncompensated care and increased financial sustainability. Medicaid expansion is associated with improvements in health and a wide variety of other outcomes, including lower mortality, less uncompensated care, and lower rates of medical debt.59 According to the Kaiser Family Foundation, about 4.4 million adults would gain Medicaid eligibility if the remaining 14 nonexpansion states expanded their programs.60
Policymakers can also support rural communities and their hospitals by opposing efforts to repeal the ACA. If the Trump administration-backed lawsuit against the ACA were to succeed, 20 million Americans would lose health insurance coverage, and uncompensated care would rise by $50 billion, according to the Urban Institute.61
Create a greater number of rural emergency centers
To preserve access to emergency care, Congress could allow rural hospitals like CAHs to downsize to an emergency department and eliminate inpatient beds without giving up special Medicare reimbursement arrangements. Qualifying hospitals could transfer patients requiring inpatient admission to other hospitals, while continuing to offer some diagnostic imaging and other outpatient services.
One such proposal is the Rural Emergency Acute Care Hospital Act (REACH Act), bipartisan legislation proposed by Sen. Amy Klobuchar (D-MN) and Sen. Chuck Grassley (R-IA) that would create rural emergency centers.62 This designation would allow hospitals to provide only emergency care in rural communities and receive Medicare reimbursement at 110 percent of operating costs. Separately, MedPAC has recommended that rural hospitals located more than 35 miles from the nearest emergency department be allowed to convert to freestanding emergency departments while still being reimbursed at hospital rates.63
Institute global budgeting for rural hospitals
Under global budgeting, hospitals are paid a fixed amount rather than having their reimbursements based on the volume and types of services they provide.64 Global budgeting can reduce small, rural hospitals’ financial risk by providing them with a more predictable stream of revenue. In addition, payment reforms that include both hospital and nonhospital care can encourage communities to invest in services that are typically less generously reimbursed, such as preventive care.65
For example, in 2014, Maryland transitioned its acute hospitals from fee-for-service payments to a global budget.66 An evaluation of the global budget program showed that it reduced hospital expenditures relative to trend without transferring costs to other parts of the health care system.67 Future global budgets should emphasize improvements in population health and primary care,68 including ensuring that patients receive care in appropriate settings and reducing the number of avoidable hospital visits.
The Pennsylvania Rural Health Model is the first Medicare demonstration project to test the financial viability and community effects of a global budget for strictly rural hospitals.69 This six-year program aims to smooth out cash flow for 30 rural Pennsylvania hospitals on a monthly basis with the goal of enabling hospitals to meet community needs, especially for substance-use disorder and mental health services.70 With global budgets based on the previous year’s revenues, participating hospitals will have a more predicable stream of revenue. Importantly, the program allows hospitals to share in the savings that result from avoidable utilization.71
Improve transportation for rural residents
The lack of transportation infrastructure can lead rural residents to rely on ambulances and emergency rooms for nonemergency care. In nonemergency situations, patients often cite the lack of affordable transportation as a major barrier to care access.72 In order to fill the gap, payers and policymakers should consider efforts to utilize existing community transit resources for medical transportation or reimburse patients who use ride-sharing services in areas that lack public transit or taxi services. 73 Another option would be to formalize volunteer services for medical transit. Oregon offers a tax credit for volunteer rural emergency medical services (EMS) providers, who provide medical and transportation services analogous to those of volunteer firefighter programs.74 The CMS should also consider policies to better reimburse and expand the use of telehealth in remote areas to reduce patients’ burden of transportation.75Finally, the CMS should stop approving states’ requests to waive coverage of nonemergency medical transportation (NEMT) requirements under Medicaid.76 NEMT is vital to eligible beneficiaries’ access to care, including appointments for preventive care, chronic disease management, and substance-use disorder treatment.
Strengthen the rural health care workforce
Rural health care provider shortages contribute to poorer access to care and poorer quality of care in rural communities. While 20 percent of the U.S. population lives in rural areas, only 9 percent of primary care physicians practice in rural areas.77 Greater access to primary care providers in rural areas would improve quality of care and health outcomes while also reducing unnecessary emergency department visits.78
One way to assist rural areas would be to encourage health professionals to train and work in underserved communities. Federal funding for physician training should include reimbursements for community-based sites so that medical residents can rotate through nonhospital settings.79 Expanding the National Health Service Corps—which provides scholarships and student loan repayment for professionals who work in federally designated health professional shortage areas—could also help bolster the rural workforce. In addition, changes to immigration policy—such as expanding the Conrad 30 program that funnels immigrant doctors into rural and underserved communities, reforming H-1B visas to benefit high-need communities—could help alleviate rural areas’ shortage of medical professionals.80
Conclusion
Mounting closures of rural hospitals across the country are exacerbating the disparity in health care access between rural and urban areas. The financial vulnerability of the remaining rural hospitals suggests that the trend may continue, leaving shortages in emergency care and other hospital services.
Policymakers should support initiatives that allow remaining rural hospitals the flexibility to tailor their services to meet community needs and improve access to care for rural Americans.
Rural America is stuck in a cycle of increasingly vulnerable patients with declining access to health care.
Why it matters: Rural patients often can’t afford care, are being hounded by hospitals and collection agencies over their unpaid bills, and are facing the reality of life in communities where the last hospital has closed.
Rural Americans tend to be older, sicker and lower-income than urban Americans. They suffer from higher rates of obesity, mental health issues, diabetes, cancer and opioid addiction, as my colleagues Stef Kight and Juliet Bartz reported.
They’re also more likely to be uninsured or covered by Medicare or Medicaid, which pay doctors and hospitals less than private insurance does.
A small and shrinking population, mostly covered by insurance plans that don’t pay very much, many of whom need a lot of care, puts more financial pressure on providers, especially hospitals. Physician shortages are common.
What they’re saying: “Rural hospitals have long been right there on the edge on average, and we’re seeing more and more of them flip over to red,” said Mark Holmes, a professor at UNC-Chapel Hill and director of the Cecil G. Sheps Center for Health Services Research.
And hospital closures often exacerbate the problems communities were already facing.
Hospitals are often the largest or second-largest employer in a rural community.
These are disproportionately located in the South — the region with the nation’s worst health outcomes, and where most states haven’t expanded Medicaid — leaving hospitals with more uninsured patients.
A 2018 study in Health Affairs found that Medicaid expansion is “associated with improved hospital financial performance and substantially lower likelihoods of closure, especially in rural markets.”
The bottom line: “What we have here is not one root cause; there’s multiple things going on here,” Holmes said. “All these sort of modest kind of trends are adding up to something that’s quite considerable.”
Go deeper:
Bloomberg Businessweek reported on eastern Montana’s sole psychiatrist, despite being the state with the nation’s highest suicide rate.
The Washington Post detailed a hospital in Missouri’s practice of suing its patients for payment — money that the hospital needed but patients generally don’t have.
Kaiser Health News and NPR have profiled the fallout in a rural community in Kansas after its sole remaining hospital closed, which included a 2-week lapse in nearby emergency care.
Opponents of the public option have funded an analysis that warns more rural hospitals may close if Americans leave commercial plans for Medicare.
With the focus on rural hospitals, the Partnership for America’s Health Care Future brings a sensitive issue for politicians into its fight against a Medicare buy-in. The policy has gone mainstream among Democratic presidential candidates and many Democratic lawmakers.
Rural hospitals could lose between 2.3% and 14% of their revenue if the U.S. opens up Medicare to people under 65, the consulting firm Navigant projected in its estimate. The analysis assumed just 22% of the remaining 30 million uninsured Americans would choose a Medicare plan. The study based its projections of financial losses primarily on people leaving the commercial market where payment rates are significantly higher than Medicare.
The estimate assumed Medicaid wouldn’t lose anyone to Medicare, and plotted out various scenarios where up to half of the commercial market would shift to Medicare.
The analysis was commissioned by the Partnership for America’s Health Care Future, a coalition of hospitals, insurers and pharmaceutical companies fighting public option and single-payer proposals.
In their most drastic scenario of commercial insurance losses, co-authors Jeff Goldsmith and Jeff Leibach predict more than 55% of rural hospitals could risk closure, up from 21% who risk closure today according to their previous studies.
Leibach said the analysis was tailored to individual hospitals, accounting for hospitals that wouldn’t see cuts since they don’t have many commercially insured patients.
The spotlight on rural hospitals in the debate on who should pay for healthcare is common these days, particularly as politicians or the executive branch eye policies that could cut hospital or physician pay.
On Wednesday, Sen. Elizabeth Warren (D-Mass.) seemingly acknowledged this when she published her own proposal to raise Medicare rates for rural hospitals as part of her goal to implement single payer, or Medicare for All. She is running for the Democratic nomination for president for the 2020 election.
“Medicare already has special designations available to rural hospitals, but they must be updated to match the reality of rural areas,” Warren said in a post announcing a rural strategy as part of her campaign platform. “I will create a new designation that reimburses rural hospitals at a higher rate, relieves distance requirements and offers flexibility of services by assessing the needs of their communities.”
Warren is a co-sponsor of the Medicare for All legislation by Sen. Bernie Sanders (I-Vt.), who is credited with the party’s leftward shift on the healthcare coverage question. But she is trying to differentiate herself from Sanders, and the criticisms about the potentially drastic pay cuts to hospitals have dogged single-payer debates.
Most experts acknowledge the need for a significant policy overhaul that lets rural hospitals adjust their business models. Those providers tend to have aging and sick patients; high rates of uninsured and public pay patients over those covered by commercial insurance; and fewer patients overall than their urban counterparts.
But lawmakers in Washington aren’t likely to act during this Congress. The major recent changes have mostly been driven by the Trump administration, where officials just last week finalized an overhaul of the Medicare wage index to help rural hospitals.
As political rhetoric around the public option or single payer has gone mainstream this presidential primary season, rural hospitals will likely remain a talking point in the ideas to overhaul or reorganize the U.S.’s $3.3 trillion healthcare industry.
This was in evidence in May, when the House Budget Committee convened a hearing on Medicare for All to investigate some of the fiscal impacts. One Congressional Budget Office official said rural hospitals with mostly Medicaid, Medicare and uninsured patients could actually see a boost in a redistribution of doctor and hospital pay.
But the CBO didn’t analyze specific legislation and offered a vague overview of how a single-payer system might look, rather than giving exact numbers.
And it has worked to some extent. Both House and Senate committees have made concessions to their surprise billing proposals to mollify some lawmakers’ worries.