Mounting evidence suggests the delta variant is the most contagious strain in the world, spreading about 225 percent faster than the original version of the virus. A small study published online July 7 may help explain why, NPR reported.
The delta variant, first identified in India, grows faster in people’s respiratory tracts and to much higher levels, according to researchers at the Guangdong Provincial Center for Disease Control and Prevention in China.
They analyzed virus levels in 62 people infected during China’s first delta variant outbreak between May 21 and June 18. They compared their findings to virus levels in 63 patients infected in 2020 by an earlier version of the virus.
On average, viral load was about 1,000 times higher for people infected with delta, compared to those infected with the earlier strain, researchers found. It also took about four days on average for delta to reach detectable levels in study participants, compared to six days for the other strain. This finding suggests people with delta likely become infectious sooner and are spreading the virus earlier in the course of their infection, researchers said.
Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
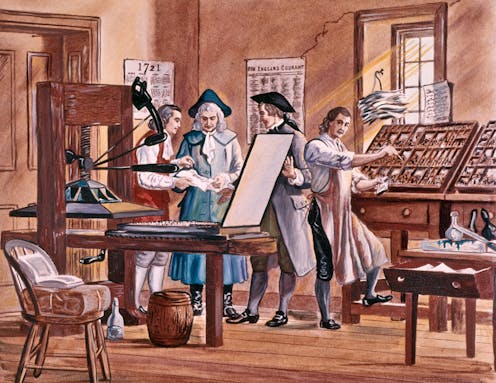
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
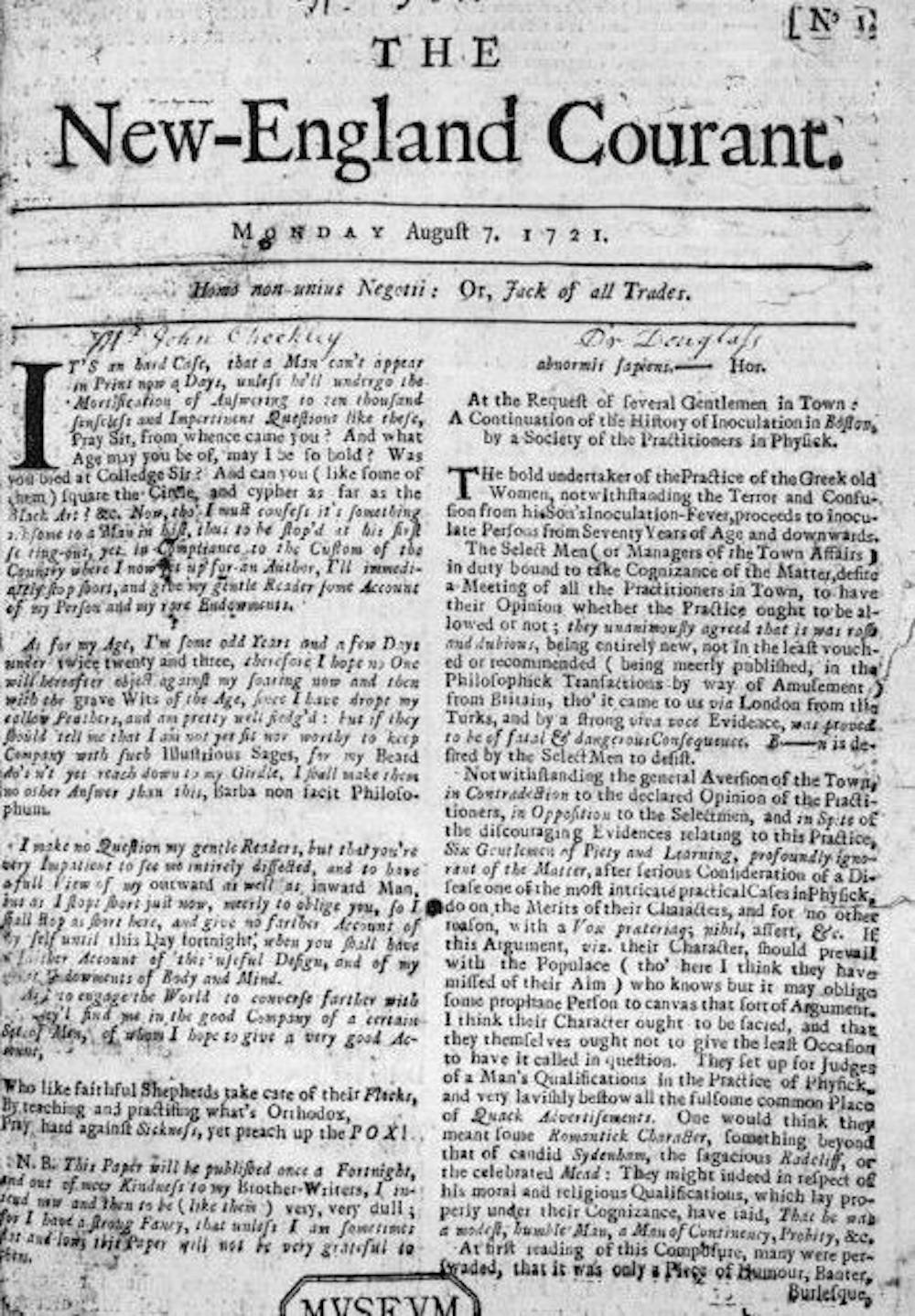
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
An argument for humility in the face of pandemic forecasting unknown unknowns.
“Are we battling an unprecedented pandemic or panicking at a computer generated mirage?” I asked at the beginning of the COVID-19 pandemic on March 18, 2020. Back then the Imperial College London epidemiological model’s baseline scenario projected that with no changes in individual behaviors and no public health interventions, more than 80 percent of Americans would eventually be infected with novel coronavirus and about 2.2 million would die of the disease. This implies that 0.8 percent of those infected would die of the disease. This is about 8-times worse than the mortality rate from seasonal flu outbreaks.
Spooked by these dire projections, President Donald Trump issued on March 16 his Coronavirus Guidelines for America that urged Americans to “listen to and follow the directions of STATE AND LOCAL AUTHORITIES.” Among other things, Trump’s guidelines pressed people to “work or engage in schooling FROM HOME whenever possible” and “AVOID SOCIAL GATHERINGS in groups of more than 10 people.” The guidelines exhorted Americans to “AVOID DISCRETIONARY TRAVEL, shopping trips and social visits,” and that “in states with evidence of community transmission, bars, restaurants, food courts, gyms, and other indoor and outdoor venues where people congregate should be closed.”
Let’s take a moment to recognize just how blindly through the early stages of the pandemic we—definitely including our public health officials—were all flying at the time. The guidelines advised people to frequently wash their hands, disinfect surfaces, and avoid touching their faces. Basically, these were the sort of precautions typically recommended for influenza outbreaks. On July 9, 2020, an open letter from 239 researchers begged the World Health Organization and other public health authorities to recognize that COVID-19 was chiefly spread by airborne transmission rather than via droplets deposited on surfaces. The U.S. Centers for Disease Control and Prevention (CDC) didn’t update its guidance on COVID-19 airborne transmission until May 2021. And it turns out that touching surfaces is not a major mode of transmission for COVID-19.
The president’s guidelines also advised, “IF YOU FEEL SICK, stay home. Do not go to work.” This sensible advice, however, missed the fact that a huge proportion of COVID-19 viral transmission occurred from people without symptoms. That is, people who feel fine can still be infected and, unsuspectingly, pass along their virus to others. For example, one January 2021 study estimated that “59% of all transmission came from asymptomatic transmission, comprising 35% from presymptomatic individuals and 24% from individuals who never develop symptoms.”
The Imperial College London’s alarming projections did not go uncontested. A group of researchers led by Stanford University medical professor Jay Bhattacharya believed that COVID-19 infections were much more widespread than the reported cases indicated. If the Imperial College London’s hypothesis were true, Bhattacharya and his fellow researchers argued, that would mean that the mortality rate and projected deaths from the coronavirus would be much lower, making the pandemic much less menacing.
The researchers’ strategy was to blood test people in Santa Clara and Los Angeles Counties in California to see how many had already developed antibodies in response to coronavirus infections. Using those data, they then extrapolated what proportion of county residents had already been exposed to and recovered from the virus.
Bhattacharya and his colleagues preliminarily estimated that between 48,000 and 81,000 people had already been infected in Santa Clara County by early April, which would mean that COVID-19 infections were “50-85-fold more than the number of confirmed cases.” Based on these data the researchers calculated that toward the end of April “a hundred deaths out of 48,000-81,000 infections corresponds to an infection fatality rate of 0.12-0.2%.” As I optimistically reported at the time, that would imply that COVID-19’s lethality was not much different than for seasonal influenza.
Bhattacharya and his colleagues conducted a similar antibody survey in Los Angeles County. That study similarly asserted that COVID-19 infections were much more widespread than reported cases. The study estimated 2.8 to 5.6 percent of the residents of Los Angeles County had been infected by early April. That translates to approximately 221,000 to 442,000 adults in the county who have had the infection. “That estimate is 28 to 55 times higher than the 7,994 confirmed cases of COVID-19 reported to the county by the time of the study in early April,” noted the accompanying press release. “The number of COVID-related deaths in the county has now surpassed 600.” These estimates would imply a relatively low infection fatality rate of between 0.14 and 0.27 percent.
Unfortunately, from the vantage of 14 months, those hopeful results have not been borne out. Santa Clara County public health officials report that there have been 119,712 diagnosed cases of COVID-19 so far. If infections were really being underreported by 50-fold, that would suggest that roughly 6 million Santa Clara residents would by now have been infected by the coronavirus. The population of the county is just under 2 million. Alternatively, extrapolating a 50-fold undercount would imply that when 40,000 diagnosed cases were reported on July 11, 2020, all 2 million people living in Santa Clara County had been infected by that date.
Los Angeles County reports 1,247,742 diagnosed COVID-19 cases cumulatively. Again, if infections were really being underreported 28-fold, that would imply that roughly 35 million Angelenos out of a population of just over 10 million would have been infected with the virus by now. Again turning the 28-fold estimate on its head, that would imply that all 10 million Angelenos would have been infected when 360,000 cases had been diagnosed on November 21, 2020.
COVID-19 cases are, of course, being undercounted. Data scientist Youyang Gu has been consistently more accurate than many of the other researchers parsing COVID-19 pandemic trends. Gu estimates that over the course of the pandemic, U.S. COVID-19 infections have roughly been 4-fold greater than diagnosed cases. Applying that factor to the number of reported COVID-19 cases would yield an estimate of 480,000 and 5,000,000 total infections in Santa Clara and Los Angeles respectively. If those are ballpark accurate, that would mean that the COVID-19 infection fatality rate in Santa Clara is 0.46 percent and is 0.49 percent in Los Angeles. Again, applying a 4-fold multiplier to take account of undercounted infections, those are both just about where the U.S. infection fatality rate of 0.45 percent is now.
The upshot is that, so far, we have ended up about half-way between the best case and worst case scenarios sketched out at the beginning of the pandemic.
The country is reopening. What does the future hold?
The story of the American pandemic has unfolded in three chapters.The first began last January, when the coronavirus emerged and the world was plunged into uncertainty about how covid-19 could be treated, how the virus spread, and when it might be defeated. The second started on the morning of November 9, 2020, when Pfizer-BioNTech announced the extraordinary efficacy of its vaccine. Those results made clear that this pandemic would end not through infection but vaccination. Our goals shifted from merely slowing the spread to beginning immunization as quickly as possible. In America, much of the past half year has been devoted to administering vaccines and gathering evidence on how well they work in the real world.
Earlier this month, the Centers for Disease Control and Prevention ushered in the American pandemic’s third chapter. The agency announced that vaccinated people could go without masks or social distancing indoors and outside, in crowds large and small. It carved out a few exceptions—for hospitals, public transportation, and the like—and noted that people still needed to obey federal and local laws. But the broad message was that vaccinated Americans could resume their pre-pandemic lives. The C.D.C. is an agency known for caution, and its new guidance shocked many public-health experts; just two weeks earlier, it had issued far more restrictive recommendations. During the same period, a survey of nearly six hundred epidemiologists found that more than three-quarters of them believed that indoor mask-wearing might remain necessary for another year or more. Still, immediately after the announcement, a number of states lifted their mask mandates. Others will surely follow, as the pressure to return to normal grows. America is now moving swiftly toward reopening.
Despite the C.D.C.’s early stumbles on communication, masks, and tests, it remains perhaps the world’s preëminent public-health agency. Its recommendations carry unparalleled scientific force in the U.S. and beyond. Ultimately, the C.D.C.’s decision reflects real shifts in the weight of the evidence on several fundamental epidemiological questions: Are the vaccines as effective as they were in the trials? Can they protect us against the coronavirus variants? And do they prevent not just illness but transmission? The answers to these questions give us good reason to think that the pandemic’s newest chapter will be its last. Read The New Yorker’s complete news coverage and analysis of the coronavirus pandemic.
On the first question, the nationwide rollout of covid-19 vaccines has proved, beyond any doubt, that they are astonishingly effective at preventing serious illness, even for the most vulnerable people. So-called breakthrough infections, in which the virus weaves its way around some of an individual’s immune system, do occur. But such infections are extremely rare, and—because a person almost always has some effective antibodies and other immune-system defenses—they usually cause mild or no symptoms. In one study, the C.D.C. examined post-vaccination infections among nearly fifteen thousand nursing-home residents and staff members, and discovered only two covid-19 hospitalizations and one death. Another study, involving half a million health-care workers from around the country, found that getting two shots reduced the risk of a symptomatic infection by ninety-four per cent. Moving forward, we should expect to continue seeing breakthrough infections from time to time—but, for the most part, we shouldn’t worry about them. (At the same time, the covid vaccines have proved exceptionally safe. Few dangerous side effects have been linked to the vaccines from Pfizer-BioNTech or Moderna, and the over-all risk of concerning blood clots after receiving Johnson & Johnson’s vaccine is rare—as of last week, when more than nine million doses had been administered, there were thirty confirmed cases.)
The most striking vaccine-efficacy statistic draws on data shared by state governments. Around a hundred and thirty million Americans are fully vaccinated, and the C.D.C. has said that it has received reports of fewer than fourteen hundredcovid-19 hospitalizations and three hundred deaths among them. This means that, after vaccination, one’s chances of dying of covid-19 are currently about two in a million, with the likelihood of being hospitalized only slightly higher. Statistics reported by hospitals tend to be accurate; still, even if state governments have missed a few cases here and there, the results are staggeringly good. “The evidence on vaccines just keeps getting better and better,” Robert Wachter, a physician and the chair of medicine at the University of California, San Francisco, told me. “When the trial results first came out, I thought, They can’t actually be this good. The real world is always messier than the trials. What we’ve learned since then is that the vaccines are probably even more spectacular than we initially believed.”
The answer to the second question—whether the vaccines work against the major coronavirus variants—is also now clear. Earlier this month, a study conducted in Qatar, where the B.1.1.7 and B.1.351 variants predominate, found that the Pfizer-BioNTech vaccine was ninety-seven per cent effective at preventing severe disease. Vaccines from Moderna and Johnson & Johnson also appear to be highly effective against the variants; in fact, these vaccines are already successfully fighting them here in the United States. The B.1.1.7 variant, which is vastly more contagious than the original virus and caused a devastating surge in the U.K. this past winter, now accounts for three-quarters of new U.S. cases—and yet, largely thanks to vaccination, daily infections in this country have fallen by nearly ninety per cent since their peak in January, and are now lower than at any point in the past eight months. The existence of more contagious variants isn’t a reason to doubt the vaccines but to vaccinate people as quickly as possible.
As for the final question—whether vaccinated people can spread the virus to others, especially unvaccinated people, including children—the evidence is similarly encouraging. Because vaccinated people are unlikely to contract the virus, the vast majority won’t be passing it on. And even the small number of vaccinated people who experience breakthrough infections have much less of the virus circulating in their bodies, and may be less infectious. Real-world data from Israel, which has mounted one of the world’s fastest and most effective vaccination campaigns, is instructive. The country’s progress in immunizing its adults has been linked to significant declines in infections among unvaccinated people; according to one preliminary estimate, each twenty-percentage-point increase in adult vaccination rates reduces infections for unvaccinated children by half. When vaccinated people remove their masks, they pose little threat to others, and they face little peril themselves.
The shift toward reopening is not without risk. The first issue is timing. Less than half of Americans have received even one shot of a covid-19 vaccine, and only around four in ten have been fully vaccinated. This means that the majority of the country remains susceptible to infection and disease. Meanwhile, the pace of vaccinations has slowed: in April, the U.S. was routinely vaccinating about three million people per day, but the daily average is now nearly two million. It’s unclear whether the new guidance will encourage or deter unvaccinated Americans from getting immunized. In a recent survey, unvaccinated Republicans said that they would be nearly twenty per cent more likely to get the shots if it meant that they wouldn’t have to wear a mask anymore. We’ll now find out how they really feel.
Vaccine hesitancy is only part of the picture. Some thirty million Americans—a group larger than anti-vaxxers or the vaccine-hesitant—say that they want to get immunized but haven’t yet done so. Some face language barriers, or fear immigration problems; others have difficulty navigating the health system, or can’t take time off from work. Many of the willing-but-unvaccinated are working-class Americans; four in five don’t have a college degree. The Biden Administration has sent billions of dollars to health centers serving low-income populations, offered tax credits to businesses that provide paid time off for employees to get immunized, and helped assemble thousands of volunteers—known as the covid-19 Community Corps—to assist with vaccine outreach to underserved populations. States, too, are trying to reduce barriers to vaccination, and offering incentives—including payments in Maryland, a lottery in Ohio, and a “Shot and a Beer” program in New Jersey—for residents who remain on the fence. There are, in short, real efforts under way to sway the vaccine-hesitant and make vaccines more accessible.
Still, the new C.D.C. guidance makes these efforts even more urgent. Until now, unvaccinated people have been shielded from high levels of viral exposure by government mandates and social norms that have kept their friends, neighbors, and colleagues masked and distanced, to varying degrees. But, in the coming weeks, those protections will likely erode. For unvaccinated Americans, this could be the most dangerous moment in the pandemic. In most contexts, there is no reliable mechanism for verifying who has and hasn’t been vaccinated. Inevitably, against the C.D.C.’s advice, many unvaccinated people will resume normal life, too, threatening their own health and that of others. When asked how businesses are to know which customers can enter unmasked, Anthony Fauci, the nation’s top infectious-disease expert, told CNN, “They will not be able to know. You’re going to be depending on people being honest enough to say whether they were vaccinated or not.”
“Unvaccinated people are now going to have much higher levels of exposure,” Wachter told me. “That’s especially true in places with lots of community spread and in places where more contagious variants are circulating.” Wachter suggested that the C.D.C. could be making an epidemiological bet. The move “will cause some additional covid cases that otherwise would not have occurred,” he said—but, “if it leads to even a small uptick in vaccination, it will save lives in aggregate.”
Since the start of the pandemic’s second chapter, public-health officials have been working to prevent a catastrophic collision between the ship of reopening and the iceberg of the unvaccinated. By slowing the speed of the ship or shrinking the size of the iceberg, we have sought to reduce the force of the collision. But barring a hundred-per-cent vaccination rate, or something close to it—an outcome that the U.S. was never likely to achieve—a crash of some sort has been inevitable.India’s collision has been titanic—it reopened with a population of more than a billion, even though hardly anyone was vaccinated. In the U.S., the situation is different. Our iceberg has been melting, and we’ve been approaching it slowly. Now we’re taking off the brakes.
The C.D.C. issues guidance, not laws; there are several quantitative measures that states, counties, cities, companies, and individuals can consult in pacing their reopening and squaring the agency’s broad recommendations with local realities. A community’s immunization rate is perhaps the most obvious statistic to track. Experts have argued for meeting a seventy-per-cent immunity threshold before relaxing masking and distancing requirements. No states have got there yet, although some, such as Vermont and Maine, are well on their way. The Biden Administration has said that it hopes to hit the seventy-per-cent target for first shots by the Fourth of July.
Because the vaccines prevent almost all cases of severe covid-19, the number of covid-19 hospitalizations is another good metric to watch. “With vaccines, cases become uncoupled from severe disease,” Monica Gandhi, an infectious-disease doctor at the University of California, San Francisco, who has studied asymptomatic coronavirus transmission, told me. Gandhi was among the first researchers to show that masks protect not just others but wearers, too; when we spoke, before the C.D.C.’s announcement, she said that, in her view, most precautions could end when half of Americans had received their first shot and covid-19 hospitalizations had fallen below sixteen thousand nationally, or about five per hundred thousand people. (At the peak of most flu seasons, the U.S. records five to ten influenza hospitalizations per hundred thousand.) Hospitalizations appear to be falling, unevenly, across the country. However, there are currently thirty thousand Americans hospitalized with covid-19—roughly a quarter of the January peak, but still about twice Gandhi’s threshold.
Herd immunity offers a third benchmark for reopening. The idea is that, once about eighty per cent of the population has been vaccinated or infected, the virus will struggle to spread. Recently, some experts have argued that we might never get to herd immunity because of variants, vaccine hesitancy, and the fact that children under twelve, who make up some fifteen per cent of the U.S. population, are unlikely to be immunized for some time. But the C.D.C.’s recommendation could change the equation. As states lift restrictions and unvaccinated people face higher levels of exposure, more of them are likely to get infected, pushing us closer to the herd immunity threshold. In all likelihood, the U.S. will be able to reach sixty-per-cent vaccination in the coming weeks; meanwhile, perhaps a third of Americans have already been infected. Even assuming significant overlap between the two groups, the combination of vaccination and infection is likely to make it harder for the virus to find new hosts. Marc Lipsitch, the director of Harvard’s Center for Communicable Disease Dynamics, emphasized that, because some parts of the country may reach herd immunity, or something close to it, before others—Connecticut’s current covid-19 immunization rate, for instance, is nearly twice Mississippi’s—unvaccinated adults will face different levels of risk depending on where they live. “There won’t be one national end,” Lipsitch told me. “We’re going to see a fundamental change in terms of what it means to live in this country, but there’s also going to be a lot of local variation.”
Covid-19 deaths give us another way of tracking the pandemic. Experts have argued that the U.S., with a population of three hundred and thirty-two million, should aim for fewer than a hundred coronavirus deaths daily—roughly the toll of a typical flu season. Right now, America is seeing about six hundred covid-19 deaths each day; according to the Institute for Health Metrics and Evaluation, which generates one of the country’s most widely cited pandemic models, that number will likely fall to about a hundred in August. “Things will look very good this summer,” Christopher Murray, the director of the I.H.M.E., told me. “A lot of people will think that we’re done, that it’s all over. But what happens in the fall is the tricky part.” Murray believes that a confluence of factors—the spread of variants, in-person schooling, meaningful numbers of still-unvaccinated people, and the seasonality of the virus—will produce a small winter spike, concentrated in communities with low vaccination rates. It won’t be the apocalyptic surge of New York City in the spring of 2020—or, more recently, those of India or Brazil—but, each week, several thousand unvaccinated Americans could die.
It’s possible, given all this, to imagine a plausible scenario for the conclusion of the American pandemic. The coronavirus disease toll continues to fall throughout the summer. States do away with mask mandates and capacity restrictions; people increasingly return to bars, spin classes, and airports, then to stadiums, movie theatres, and concerts. By midsummer, in communities with high vaccination rates, covid-19 starts to fade from view. In those places, even people who remain unvaccinated are protected, because so little of the virus circulates. But, in other parts of the country, low immunization rates combined with reopening allow the disease to register again. Hospitals aren’t overwhelmed—there’s no need to build new I.C.U.s or call in extra staff—but the collision between ship and iceberg is forceful, and each week thousands of people fall ill and hundreds die. Some victims are vaccine-hesitant; others were unable, for whatever reason, to get vaccinated. Still, perhaps unfairly, these outbreaks come with an aura of culpability: to people in safe parts of the country, the ill seem like smokers who get lung cancer.
In the fall, many unvaccinated children return to school. Scattered infections among them capture headlines, but serious illnesses are exceedingly rare; the overwhelming majority of children remain safe, and, with time, they, too, are immunized. The U.S. approaches something like herd immunity. Some people may still fall ill and die of covid-19—perhaps they are immunocompromised, elderly, or just unlucky—but, by and large, America has gained the upper hand. Meanwhile, in poor nations with few vaccines, the pandemic continues. As crisis wanes in one country, catastrophe ignites in another. Every so often, we learn of a new variant that’s thought to be more contagious, lethal, or vaccine-resistant than the rest; we rush to institute travel bans, only to learn that the variant, or a close cousin, is already circulating in the U.S. and has been largely subdued by the vaccines, as all previous variants have been. In the fall, Americans line up for covid booster shots alongside flu vaccines. The pandemic’s final chapter comes to a close not through official decree but with the gradual realization that covid-19 no longer dominates our lives.
Reopening a country after a pandemic isn’t like flipping a giant switch. It’s more like lighting a series of candles, illuminating one part, then another, until the whole place shines. Many states, counties, cities, and businesses will further loosen their restrictions; others will wait. Communities and individuals will approach the end of the crisis differently, as they’ve approached the rest of it. Some unvaccinated people have already been forgoing precautions; on the other hand, I’ve been vaccinated for months and, since the C.D.C. announcement, have yet to leave my mask behind—whether because of a lingering, irrational fear or simply to avoid dirty looks, I can’t say. Social norms take time to change, even when one of the world’s most respected public-health agencies is telling you to change them.
The pandemic has created not just chaos and suffering but uncertainty. It’s easy, therefore, to be doubtful about the fortunate position in which we seem to find ourselves now. As a physician, I spent the early months of the pandemic caring for covid-19 patients in New York City; they streamed into the hospital day after day, deathly ill. We raced to build covid wards, I.C.U.s, and hospice units. At the time, we had little to offer. There were no proven therapies, and certainly no vaccines. There were weeks when thousands of New Yorkers died, many of them alone in their final moments, while more people were dying across the world. I felt fear, anxiety, and sometimes despair. The scale of the damage—the lives lost, businesses shuttered, dreams shattered, children orphaned, seniors isolated—was crushing, and the path forward was both frightening and unknown.
As good news began to arrive, I greeted it with a blend of guarded skepticism and cautious optimism. First came evidence that outdoor transmission was unlikely. Then we learned that contaminated surfaces rarely spread disease; that some patients can breathe better simply by lying on their bellies; that P.P.E. works; that dexamethasone saves lives. We discovered that immunity lasts many months, perhaps years; that repeat infections are unlikely; and that variants present a surmountable challenge.
Now, study after study, in country after country, has shown that the vaccines are capable of transforming a lethal pathogen into a manageable threat. Examining and reëxamining the vaccine results, I’ve gone through stages, too—caution, hope, and, finally, clarity. We really are that close. The beginning of the end is here.
The World Health Organization said Monday that the coronavirus variant first identified in India last year will be reclassified as a “variant of concern,” indicating that it has become a global health threat.
The B.1.617 variant has been found to spread more easily than the original virus, with some evidence indicating that it may evade some of the protections provided by the vaccines, according to a preliminary study. But the shots are still considered effective. The agency will provide more details on Tuesday.
The highly contagious, triple-mutant variant is also the fourth variant to be designated as a global concern, prompting enhanced tracking and analysis. The other variants are those first detected in Britain, South Africa and Brazil.
“We are classifying this as a variant of concern at a global level,” said Maria Van Kerkhove, WHO technical lead on COVID-19, per Reuters. “There is some available information to suggest increased transmissibility.”
A variant is labeled as “of concern” if it is shown to be more contagious, more deadly or more resistant to current vaccines and treatments, according to the WHO.
The global agency said the predominant lineage of B.1.617 was first identified in India in December, although an earlier version was spotted in October 2020.
The variant has already spread to other countries, and many nations – including the U.S. – have moved to end or restrict travel from India.
“Even though there is increased transmissibility demonstrated by some preliminary studies, we need much more information about this virus variant and this lineage and all of the sub-lineages,” said Maria Van Kerkhove, the WHO’s technical lead for COVID-19.
India reported a record-high of daily coronavirus cases, averaging about 391,000 new daily cases and about 3,879 deaths per day, according to Johns Hopkins University data.
When the Centers for Disease Control and Prevention last week issued guidelines for what vaccinated people can safely do, the agency employed the word “risk” 43 times.
The word often carried a modifier, like so: increased risk, residual risk, low risk, potential risk, minimal risk, higher risk. The CDC did not define “low,” “minimal” or “higher,” instead using broad brushstrokes to paint a picture of post-vaccination life.
For example: “Indoor visits or small gatherings likely represent minimal risk to fully vaccinated people.”
On Wednesday, CDC director Rochelle Walensky said she could not give a definitive answer to what a “small” gathering is, because there are too many variables.
“If we define a small- and medium-sized gathering, we actually also have to define the size of the space that it’s in, the ventilation that is occurring, the space between people. And so, I think we should get back to the the general concepts,” Walensky said.
The situation has left people where they’ve been since the start of the pandemic: forced to play the role of amateur epidemiologist.
In the early days of the pandemic, we wondered if we could catch the coronavirus from a passing jogger and if our groceries, fresh from the store and resting on the kitchen counter, threatened to kill us. Science has attenuated some of our earliest fears. But more than a year into this crisis, we’re still trying to perform complicated risk calculations while relying on contradictory research and shifting CDC guidance.
Risk analysis is not something humans are necessarily good at. We rely on anecdotes more than scientific data. The questions we ask rarely have a simple yes or no answer. Risk tends to be on a sliding scale. Outside of self-isolation, there is no obvious way to drive the risk of viral transmission to zero, nor is risky behavior guaranteed to result in a dire outcome. We have no choice but to live probabilistically.
The risk landscape keeps changing as well.The virus is mutating, and there are many different variants in circulation. Many people are now fully vaccinated, some only partially vaccinated (in between shots, for example), some unvaccinated and some armored with a level of immunity through natural infection. Add the extreme variation in disease severity because of age and underlying conditions, and the risk equations get so long we may run out of chalkboard.
The restrictions imposed by governments have sometimes made little sense. Casinos were open before schools in some states. Mask mandates outdoors remained in place even when indoor dining became permitted.
“It seems to me if we are going to have indoor dining, we should have mask-free jogging,” Harvard epidemiologist Marc Lipsitch said in an email.
One thing that is incontrovertibly true: The coronavirus vaccines are remarkably safe and effective, and people should get vaccinated if possible.
“These are off-the-scale good,” said Amesh Adalja, an infectious-disease doctor and senior scholar at the Johns Hopkins Center for Health Security. “These are much better than vaccines that we rely on every year, like the flu vaccine.”
Even for people sold on vaccines, there remain lingering questions about what is and isn’t safe, and what is and isn’t the proper way to go about daily life in an increasingly vaccinated society. Here, we present some answers, with the caveat that our knowledge of the coronavirus, SARS-CoV-2, is still evolving, as is the virus itself.
Q: Why do I still need to wear a mask after I’m fully vaccinated?
A: You don’t need to wear a mask outdoors when fully vaccinated, except in crowds (such as at a sports stadium or a concert), nor do you have to wear one indoors among other vaccinated people or members of your own household.
But there are situations where you still need to mask up. You could still get infected with the coronavirus, and although it would most likely be mild or asymptomatic, you could transmit the virus to another person. Again, the odds of that happening are low, and there is encouraging data from Israel that suggests vaccinations dramatically reduce community spread.
But remember: A vaccination campaign is not simply about protecting the vaccinated individual. The goal is to build immunity broadly. Moreover, many communities still require masks in public settings — so it’s the law. It’s also polite — you don’t want to make people guess if you’ve been vaccinated or not. That probably will change when infection rates plummet and vaccinations are far more widespread.
“It is also a show of solidarity that we are still in this together,” said Maria Van Kerkhove, technical lead for the World Health Organization’s covid-19 response. “It’s about you and your community, your family, your friends, your workplace, your loved ones. It’s not just about you.”
At some point, viral transmission will plummet. We’re a long way from that point. As long as the virus is circulating in our communities, we need to use what we can to limit the spread and drive down the infection rate.
“Because [the vaccines] are not perfect, that’s precisely why we are urging people to be cautious,” Surgeon General Vivek H. Murthy said in a recent White House covid-19 task force news briefing. “We have great confidence in vaccines. We understood they are not perfect.”
Q: If you’re vaccinated, are you definitely protected against the coronavirus?
A: You’re very likely protected from symptomatic illness. That’s why Adalja, echoing the consensus, said, “These vaccines are something that will change your life.”
In clinical trials, the Pfizer and Moderna vaccines were about 95 percent effective in blocking symptomatic illness after two shots. The one-shot Johnson & Johnson vaccine was not quite as effective but just as good at preventing severe illness and death — which is the highest public health priority in a pandemic like this.
Q: But aren’t there also breakthrough infections?
A: As of April 26, the CDC had documented 9,245 breakthrough infections among fully vaccinated people. But look at the denominator: Those cases were among more than 95 million people. That’s fewer than 1 in 10,000 people vaccinated. (The agency noted that this is probably an undercount because of lack of testing and surveillance.) Of those rare breakthrough cases known to the CDC, 27 percent were asymptomatic and only 9 percent required hospitalization.
Adalja said people need to focus on probabilities and not anecdotes.
“This is kind of a cognitive bias that people have with many kinds of risk. It’s just like when there’s a shark attack in Australia. How much coverage does that get?” he said.
Q: Should people who got the Johnson & Johnson vaccine worry about blood clots?
A: If you notice unusual and serious side effects, such as severe headaches, contact your doctor. But the risk is extremely low. Federal regulators reauthorized the use of the vaccine after a 10-day pause, having found 15 cases of a serious clotting disorder among the 7 million people who had received the vaccine at that time. By any calculation, the risk of a bad vaccine reaction is much less than the risk of getting a serious case of covid-19.
Paul A. Offit, a pediatrician at Children’s Hospital of Philadelphia who is an expert on vaccination, suggests that the Johnson & Johnson coronavirus vaccine suffers from bad timing. Had it been approved first, before the Pfizer and Moderna vaccines, its many virtues would have been celebrated and the rare side effects minimized.
He noted that the Johnson & Johnson vaccine is “refrigerator stable” for up to five weeks. The vaccine is appealing to public health officials because it’s one-and-done and can be more easily deployed in remote locations and in places where recipients are homebound.
Q: How long will natural or vaccine-induced immunity last?
A: No one knows, but the initial evidence is encouraging, said Alessandro Sette, a professor of immunology at the La Jolla Institute for Immunology. A research paper published by Sette and fellow researchers in January showed that 90 percent of people who recovered from a coronavirus infection had robust levels of immunity eight months after they became sick. Immunity did not suddenly drop after eight months — that was merely the limit of the research period.
“Ninety percent having a good immune response also means 10 percent don’t. That is a reason for vaccinating and being careful even if you had the disease,” Sette said.
Immunity post-vaccination also appears durable, and there is less variability in levels of antibodies and other immune system cells following a vaccination than following a natural infection, Sette said.
Because this is a novel disease, and vaccines have not been widely deployed for very long, it is too soon to know how long antibodies will last. But Sette pointed out that the immune system has other weapons against invasive viruses, including “killer T-cells,” which continue to be able to recognize infected cells and kill them, preventing viral replication.
Q: Do the vaccines work against these new virus variants? And shouldn’t we be worried about a new variant that has even scarier, vaccine-evading mutations?
A: The immune response generated by vaccines is sufficiently protective against coronavirus variants to prevent most people from getting seriously ill.
Infectious-disease experts do worry about future mutations that could allow the virus to exhibit vaccine evasion. That said, there are limits to how much the virus can mutate — how much it can change its structure — and still function, according to Sette.
“The virus has to walk a tightrope,” he said. The virus can mutate to escape the effect of a specific antibody, but “it can’t change too much.”
He added, “While the virus has surprised us this year in a number of ways, the data we’ve seen so far does not suggest there’s an infinite number of ways the virus can mutate and escape immune recognition and still be as infectious.”
Q: When will we reach herd immunity?
A: No one knows what level of immunity would throttle virus transmission, and it probably varies from one environment to another and from one season of the year to another. But in the United States, at least, vaccinations have already had an effect. The virus increasingly is slamming into immune-system walls. Eventually, with enough vaccinations, most of the people who get infected will be dead-end alleys for the virus.
The virus appears destined to pop up in smaller outbreaks that could be more easily contained. But the virus won’t disappear, especially because it continues to spread at catastrophic rates in many countries that have low levels of vaccination. The only infectious disease-causing virus ever eradicated is smallpox.
For now, successful navigation of the pandemic may simply mean taking steps to reduce the threat of a serious case of covid-19 (as best as anyone can determine it) to the level of other threats that we typically tolerate, and which don’t tend to keep us awake at night.
The trope is currently abuzz in anti-vaccine circles, said Nicole Baldwin, MD, a pediatrician who has been a target of attacks by the anti-vaxxer community.
“It’s amazing, and sad, what people will believe,” Baldwin told MedPage Today.
Essentially, they believe that people who’ve had the vaccine can somehow shed the spike protein, which in turn can cause menstrual cycle irregularities, miscarriages, and sterility in other women just by being in close proximity.
“This is a new low, from the delusional wing of the anti-vaxx cult,” said Zubin Damania, MD, a.k.a. ZDoggMD, in a video he recently posted to bust vaccine shedding myths.
Damania said the misinformation originates from an earlier claim that syncytin, a protein involved in placental formation, bears some structural similarities to the spike protein, and therefore vaccination would interfere with women’s reproductive systems. Many a fact check has shown that vaccines don’t target the protein.
Once injected, the vaccines prompt cells to make the spike protein, but it’s usually cleared in 24 to 48 hours, leaving little opportunity for “shedding,” even if it could occur — which it can’t, Damania emphasized.
Another logical fallacy he pointed out: “Why, then, wouldn’t natural spike protein do the same thing? Wouldn’t you be more scared of natural coronavirus infection? Oh, but it’s ‘natural.'”
Damania noted that there are legitimate questions and research about whether the coronavirus itself and vaccines have an impact on women’s menstrual cycles. Since the beginning of the pandemic, women who’ve had COVID-19 reported changes to their menstrual cycle, and Damania said that researchers are assessing reports of changes to the menstrual cycle following vaccination.
Regarding the potential relationship to vaccination, “we don’t understand, first, if it’s true, and if it were true, what is the mechanism?” he said. “Anything that causes stress, inflammation, and an immune response may have an effect on the menstrual cycle. … Could it be that the vaccine causes a temporary change in menses? Sure, it’s possible, and it’s being looked at.”
Leila Centner, co-founder and CEO of Centner Academy, the Miami school that has banned vaccinated employees, told NBC News in a statement that “tens of thousands of women all over the world” have reported reproductive issues from being around someone who has been vaccinated.
Baldwin pointed out an Instagram video, now marked as misinformation, in which a nurse, Maureen McDonnell, RN, and a physician, Lawrence Palevsky, MD, discuss the effect of vaccines on women’s menstrual cycles.
“This isn’t just a trivial thing,” Damania said. “It’s quite harmful.”
One hesitates to elevate obviously bad arguments, even to point out how bad they are. This is a conundrum that comes up a lot these days, as members of the media measure the utility of reporting on bad faith, disingenuous or simply bizarre claims.
If someone were to insist, for example, that they were not going to get the coronavirus vaccine solely to spite the political left, should that claim be elevated? Can we simply point out how deranged it is to refuse a vaccine that will almost certainly end an international pandemic simply because people with whom you disagree think that maybe this is a good route to end that pandemic? If someone were to write such a thing at some attention-thirsty website, we certainly wouldn’t want to link to it, leaving our own readers having to figure out where it might be found should they choose to do so.
In this case, it’s worth elevating this argument (which, to be clear, is actually floating out there) to point out one of the myriad ways in which the effort to vaccinate as many adults as possible has become interlaced with partisan politics. As the weeks pass and demand for the vaccine has tapered off, the gap between Democratic and Republican interest in being vaccinated seems to be widening — meaning that the end to the pandemic is likely to move that much further into the future.
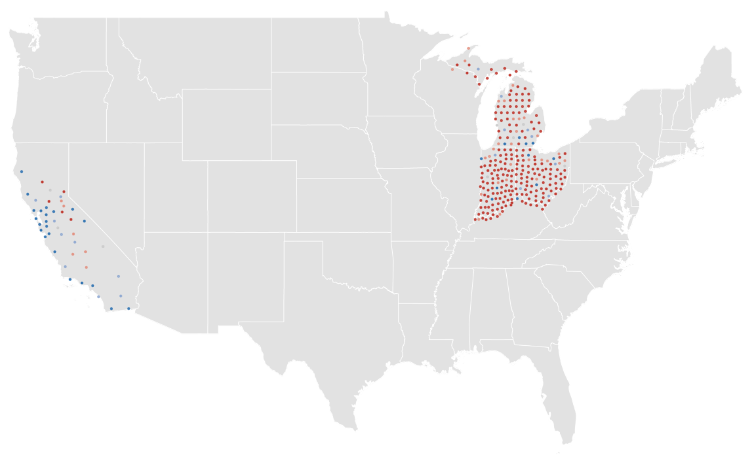
Consider, for example, the rate of completed vaccinations by county, according to data compiled by CovidActNow. You can see a slight correlation between how a county voted in 2020 — the horizontal axis — and the density of completed vaccinations, shown on the vertical. There’s a greater density of completed vaccinations on the left side of the graph than on the right.
If we shift to the percentage of the population that’s received even one dose of the vaccine, the effect is much more obvious.
This is a relatively recent development. At the beginning of the month, the density of the population that had received only one dose resulted in a graph that looked much like the current density of completed doses.
If we animate those two graphs, the effect is obvious. In the past few weeks, the density of first doses has increased much faster in more-Democratic counties.
If we group the results of the 2020 presidential contest into 20-point buckets, the pattern is again obvious.
It’s not a new observation that Republicans are less willing to get the vaccine; we’ve reported on it repeatedly. What’s relatively new is how that hesitance is showing up in the actual vaccination data.
A Post-ABC News poll released on Monday showed that this response to the vaccine holds even when considering age groups. We’ve known for a while that older Americans, who are more at risk from the virus, have been more likely to seek the vaccine. But even among seniors, Republicans are significantly more hesitant to receive the vaccine than are Democrats.
This is a particularly dangerous example of partisanship. People 65 or older have made up 14 percent of coronavirus infections, according to federal data, but 81 percent of deaths. That’s among those for whom ages are known, a subset (though a large majority) of overall cases. While about 1.8 percent of that overall group has died, the figure for those aged 65 and over is above 10 percent.
As vaccines have been rolled out across the country, you can see how more-heavily-blue counties have a higher density of vaccinations in many states.
This is not a universal truth, of course. Some heavily Republican counties have above-average vaccination rates. (About 40 percent of counties that preferred former president Donald Trump last year are above the average in the CovidActNow data. The rate among Democratic counties is closer to 80 percent.) But it is the case that there is a correlation between how a county voted and how many of its residents have been vaccinated. It is also the case that the gap between red and blue counties is widening.
Given all of that, it probably makes sense to point out that an argument against vaccines based on nothing more than “lol libs will hate this” is an embarrassing argument to make.












{kind=link}