A surge in coronavirus infections in Western Europe has experts and health authorities on alert for another wave of the pandemic in the United States, even as most of the country has done away with restrictions after a sharp decline in cases.
Infectious-disease experts are closely watching the subvariant of omicron known as BA.2, which appears to be more transmissible than the original strain, BA.1, and is fueling the outbreak overseas.
In all, about a dozen nations are seeing spikes in coronavirus infections caused by BA.2, a cousin of the BA.1 form of the virus that tore through the United States over the past three months.
In the past two years, a widespread outbreak like the one now being seen in Europe has been followed by a similar surge in the United States some weeks later. Many, but not all, experts interviewed for this story predicted that is likely to happen. China and Hong Kong, on the other hand, are experiencing rapid and severe outbreaks, but the strict “zero covid” policies they have enforced make them less similar to the United States than Western Europe.
A number of variables — including relaxed precautions against viral transmission, vaccination rates, the availability of antiviral medications and natural immunity acquired by previous infection — may affect the course of any surge in the United States, experts said.
Most importantly, it is unclear at this point how many people will become severely ill, stressing hospitals and the health-care system as BA.1 did.
Another surge also may test the public’s appetite for returning to widespread mask-wearing, mandates and other measures that many have eagerly abandoned as the latest surge fades and spring approaches, experts said.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” said Eric Topol, director of the Scripps Research Translational Institute in San Diego, who recently posted charts of the outbreak on Twitter. “There’s no question there’s a significant wave there.”
Topol noted that hospitalizations for covid-19, the disease caused by the virus, are rising in some places as well, despite the superior vaccination rates of many Western European countries.
At a briefing Monday, White House press secretary Jen Psaki said about 35,000 cases of BA.2 have been reported in the United States to date. But she offered confidence that “the tools we have — including mRNA vaccines, therapeutics and tests — are all effective tools against the virus. And we know because it’s been in the country.”
Kristen Nordlund, a spokeswoman for the Centers for Disease Control and Prevention, said in an email Tuesday that “although the BA.2 variant has increased in the United States over the past several weeks, it is not the dominant variant, and we are not seeing an increase in the severity of disease.”
The seven-day average of cases in the United States fell 17.9 percent in the past week, according to data tracked by The Washington Post, while the number of deaths dropped 17.2 percent and hospitalizations declined 23.2 percent.
Predicting the future course of the virus has proved difficult throughout the pandemic, and the current circumstances in Europe elicited a range of opinions from people who have closely tracked the pathogen and the disease it causes.
In the United States, just 65.3 percent of the population, 216.8 million people, are fully vaccinated, and only 96.1 million have received a booster shot, according to data tracked by The Post. In Germany, nearly 76 percent are fully vaccinated, according to the Johns Hopkins data, and the United Kingdom has fully vaccinated 73.6 percent.
That lower vaccination rate is very likely to matter as BA.2 spreads further in the United States, especially in regions where it is significantly lower than the national rate, several experts said. And even for people who are fully vaccinated and have received a booster shot, research data is showing that immunity to the virus fades over time. Vaccine-makers Pfizer and BioNTech asked the Food and Drug Administration on Tuesday for emergency authorization to offer a fourth shot to people 65 and older.
“Any place you have relatively lower vaccination rates, especially among the elderly, is where you’re going to see a bump in hospitalizations and deaths from this,” said Céline Gounder, an infectious-diseases physician and editor at large for public health at Kaiser Health News.
Similarly, as the public sheds masks — every state has dropped its mask mandate or announced plans to do so — another layer of protection is disappearing, several people tracking the situation said.
“Why wouldn’t it come here? Are we vaccinated enough? I don’t know,” said Kimberly Prather, a professor of atmospheric chemistry and an expert on aerosol transmission at the University of California at San Diego.
“So I’m wearing my mask still. … I am the only person indoors, and people look at me funny, and I don’t care.”
Yet BA.2 appears to be spreading more slowly in the United States than it has overseas, for reasons that aren’t entirely clear, Debbie Dowell, chief medical officer for the CDC’s covid-19 response, said in a briefing Saturday for clinicians sponsored by the Infectious Diseases Society of America.
“The speculation I’ve seen is that it may extend the curve going down, case rates from omicron, but is unlikely to cause another surge that we saw initially with omicron,” Dowell said.
One reason for that may be the immunity that millions of people acquired recently when they were infected with the BA.1 variant, which generally caused less-severe illness than previous variants. Yet no one really knows whether infection with BA.1 offers protection from BA.2.
“That’s the question,” said Jeffrey Shaman, an epidemiologist at the Columbia University Mailman School of Public Health. “Better yet, how long does it provide protection?”
Topol said the United States needs to improve its vaccination and booster rates immediately to protect more of the population against any coming surge.
“We have got to get the United States protected better. We have an abundance of these shots. We have to get them into people,” he said.
Biden administration officials said that whatever the further spread of BA.2 brings to the United States, the next critical step is to provide the $15.6 billion in emergency funding that Congress stripped from a deal to fund the government last week. That money was slated to pay for coronavirus tests, more vaccines and antiviral medications.
“That means that some programs, if we don’t get funding, could abruptly end or need to be pared back, Psaki said at Monday’s briefing. “And that could impact how we are able to respond to any variant.”
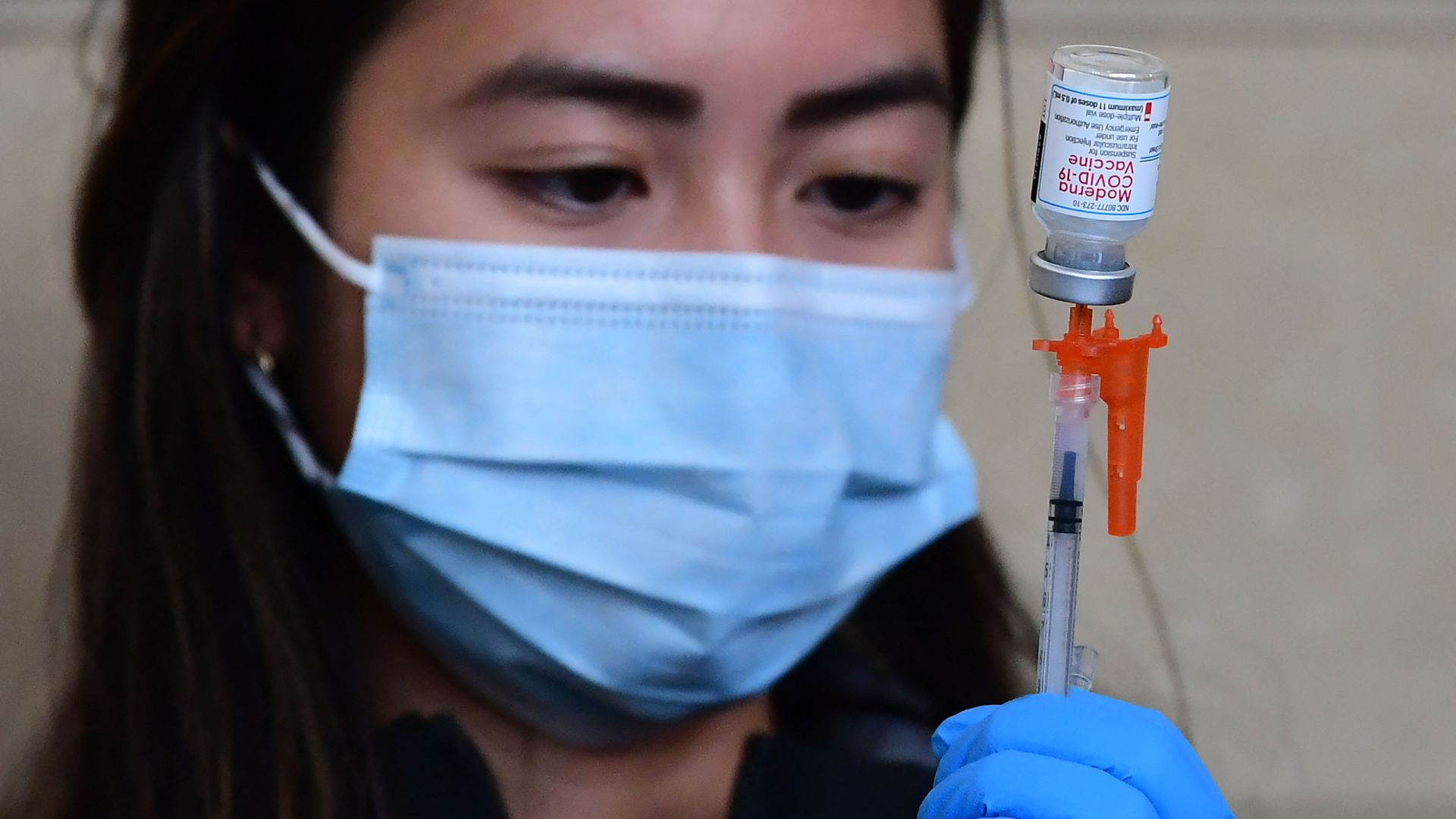
The Food and Drug Administration fully approved Moderna’s mRNA COVID-19 vaccine on Monday, saying it meets its safety and manufacturing requirements.
Why it matters: Moderna’s vaccine, which will now be marketed as Spikevax, is the second coronavirus vaccine to receive full approval after the FDA approved Pfizer-BioNTech’s vaccine in August.
Hundreds of millions of doses of Moderna’s vaccine have already been administered in the U.S. under the FDA’s emergency use authorization.
What they’re saying: “The public can be assured that Spikevax meets the FDA’s high standards for safety, effectiveness and manufacturing quality required of any vaccine approved for use in the United States,” acting FDA Commissioner Janet Woodcock said in a statement.
“The totality of real-world data and the full [Biologics License Application] for Spikevax in the United States reaffirms the importance of vaccination against this virus,” Moderna CEO Stéphane Bancel said.
The big picture: The rise of the Omicron variant forced vaccine makers to reevaluate the effectiveness of their vaccines, which were developed based on eaarlier forms of the virus.
Studies show that Moderna and Pfizer-BioNTech’s vaccines still overwhelmingly prevent severe disease and hospitalizations, especially when the first two doses are reinforced with a booster shot.
CMS is preparing to enforce its vaccine mandate for health care workers, but the agency may not have an accurate count of how many remain unvaccinated—and five health systems are pushing back on federal hospital vaccination data, calling it “extremely erroneous,” Cheryl Clark writes for MedPage Today.
Background
The Supreme Court earlier this month ruled that CMS could require most health care workers to be vaccinated against Covid-19—but U.S. officials currently do not know exactly how many workers remain unvaccinated, primarily due to a lack of reliable immunization data.
At the end of December, CDC reported that 77.6% of hospital workers were fully vaccinated. However, that figure was based on data from only about 40% of the nation’s hospitals. Hospitals currently send vaccination data to the agency on a voluntary basis, but beginning May 15, they will be required to send in weekly data, just like nursing homes have been.
According to Janis Orlowski, chief health care officer at the Association of American Medical Colleges (AAMC), CDC’s data is likely representative of providers nationwide, as an AAMC survey of 125 academic hospitals found similar results. More than 99% of doctors and close to 90% of nurses were vaccinated, she said, but vaccination rates dropped off to the 30% to 40% range for those in more operational roles, such as transportation and food service workers.
Is federal vaccination data for hospitals inaccurate?
Further adding to the confusion about health care workers’ vaccination rates are potential inaccuracies in a federal database that tracks Covid-19 vaccinations among workers in hospitals across the country. According to five health systems listed as having the highest numbers of unvaccinated workers, the database is “extremely erroneous,” Clark writes.
In the database, Adventist Health Orlando (AHO) is shown to have 18,576 unvaccinated workers, 637 partially vaccinated workers, and 25,253 fully vaccinated workers. However, Jeff Grainger, director of external communications for AdventHealth in Central Florida, said those numbers weren’t possible since the organization “[doesn’t] have 44,000 employees in one hospital.” He added that 96% of AHO’s team members have already complied with CMS’ mandate.
The University of Illinois Hospital (UI) was listed in the database as having 12,049 unvaccinated workers and 272 partially vaccinated workers. Jacqueline Carey, from health system’s public affairs department, disputed these numbers, saying UI had 6,530 workers as of Jan. 19, with 96% of them fully vaccinated. The remainder were either partially vaccinated or had approved exemptions.
The hospital with the third highest number of unvaccinated workers was Mount Sinai Hospital, Clark writes, but Lucia Lee, a hospital spokesperson, said the federal data was inaccurate. According to Lee, Mount Sinai Health System, of which the hospital is a part, has vaccinated 99% of its more than 43,000 employees.
A representative for Ochsner Medical Center, which is listed as having the fourth highest number of unvaccinated workers, also pushed back on the statistics in the database. Currently, 99.57% of Ochsner’s over 34,000 employees are compliant with its Covid-19 policy, with 95% of workers Ochsner Health and Ochsner LSU Health Shreveport fully vaccinated.
Finally, Kena Lewis, a spokesperson for Orlando Regional Medical Center, said that federal data showing the hospital has 44,154 workers is inaccurate. Instead, she said the hospital is one of 10 in the Orlando network, which has 23,709 total employees. Although Lewis did not give the health system’s vaccination rates, she said it “continues to review the guidelines regarding Covid-19 vaccination requirements for health care organizations and will take appropriate steps.”
Although it is not clear why there are discrepancies between the federal data and what these health systems are reporting regarding vaccination rates, there are some potential explanations, Clark writes.
According to Carey, the federal database only includes vaccination information provided by the UI health system and employee health services. This means that vaccinations workers received elsewhere, such as through a personal provider or pharmacy, are not included in the data, and they will show up as being unvaccinated.
Separately, a spokesperson for another of the five organizations told Clark on background that short-term nursing staff contracted through agencies may show up as unvaccinated in the federal database. Although the agencies assure employers the nurses are vaccinated, hospitals do not independently verify this information.
Workers in New Jersey healthcare facilities and high-risk congregate settings like hospitals and nursing homes will be required to be up to date with their COVID-19 vaccinations, including a booster, Gov. Phil Murphy announced Jan. 19.
Mr. Murphy said there would no longer be an option to opt out of vaccination through testing, except for the purposes of providing an accommodation for people exempt from vaccination.
New Jersey healthcare facilities’ covered workers subject to the CMS vaccination mandate for healthcare settings were already required to ensure covered employees received at least one vaccine by Jan. 27 and completed their primary vaccine series by Feb. 28. Mr. Murphy said the state is now requiring proof that these workers are up to date with their vaccination by Feb. 28, which also includes any booster shots for which they are eligible. Noncompliant workers risk losing their jobs.
Workers at covered healthcare settings not subject to the CMS mandate and covered high-risk congregate settings like prisons and jails have until Feb. 16 to receive their first dose of the primary vaccine series and must submit proof that they are up to date with their vaccination by March 30. Mr. Murphy said workers who become newly eligible for a booster after the two deadlines must submit proof of their booster shot within three weeks of becoming eligible.
“With the highly transmissible omicron variant spreading across the country and New Jersey, it is essential that we do everything we can to protect our most vulnerable populations,” Mr. Murphy said in a news release. “With immunity waning approximately five months after a primary COVID-19 vaccination, receiving a booster dose is necessary to protect yourself and those around you. It is critically important that we slow the spread throughout our healthcare and congregate settings in order to protect our vulnerable populations and the staff that care for them.”
The rule in New Jersey, which was issued through an executive order, comes after New York and California also announced booster requirements for healthcare staff.
The latest Omicron developments continue to be encouraging. New Covid-19 cases are plummeting in a growing list of places. The percentage of cases causing severe illness is much lower than it was with the Delta variant. And vaccines — particularly after a booster shot — remain extremely effective in preventing hospitalization and death.
I also think it’s time to begin considering what life after the Omicron wave might look like.
1. Plunging cases
Since early last week, new cases in Connecticut, Maryland, New Jersey and New York have fallen by more than 30 percent. They’re down by more than 10 percent in Colorado, Florida, Georgia, Massachusetts and Pennsylvania. In California, cases may have peaked.
“Let’s be clear on this — we are winning,” Mayor Eric Adams of New York said yesterday. Kathy Hochul, the governor of New York State, said during a budget speech, “We hope to close the books on this winter surge soon.”
If anything, the official Covid numbers probably understate the actual declines, because test results are often a few days behind reality.
The following data comes from Kinsa, a San Francisco company that tracks 2.5 million internet-connected thermometers across the country. It uses that data to estimate the percentage of Americans who have a fever every day. The declines over the past week have been sharp, which is a sign of Omicron’s retreat:
Many hospitals are still coping with a crushing number of patients, because Covid hospitalization trends often trail case trends by about a week. But even the hospital data shows glimmers of good news: The number of people hospitalized with Covid has begun declining over the past few days in places where Omicron arrived first:
The U.S. seems to be following a similar Omicron pattern as South Africa, Britain and several other countries: A rapid, enormous surge for about a month, followed by a rapid decline — first in cases, then hospitalizations and finally deaths.
Some of the clearest research on Covid’s risks comes from a team of British researchers led by Dr. Julia Hippisley-Cox of the University of Oxford. The team has created an online calculator that allows you to enter a person’s age, vaccination status, height and weight, as well as major Covid risk factors. (It’s based on an analysis of British patients, but its conclusions are relevant elsewhere.)
A typical 65-year-old American woman — to take one example — is five foot three inches tall and weighs 166 pounds. If she had been vaccinated and did not have a major Covid risk factor, like an organ transplant, her chance of dying after contracting Covid would be 1 in 872, according to the calculator. For a typical 65-year-old man, the risk would be 1 in 434.
Among 75-year-olds, the risk would be 1 in 264 for a typical woman and 1 in 133 for a typical man.
Those are meaningful risks. But they are not larger than many other risks older people face. In the 2019-20 flu season, about 1 out of every 138 Americans 65 and older who had flu symptoms died from them, according to the C.D.C.
And Omicron probably presents less risk than the British calculator suggests, because it uses data through the first half of 2021, when the dominant version of Covid was more severe than Omicron appears to be. One sign of Omicron’s relative mildness: Among vaccinated people in Utah (a state that publishes detailed data), the percentage of cases leading to hospitalization has been only about half as high in recent weeks as it was last summer.
For now, the available evidence suggests that Omicron is less threatening to a vaccinated person than a normal flu. Obviously, the Omicron wave has still been damaging, because the variant is so contagious that it has infected tens of millions of Americans in a matter of weeks. Small individual risks have added up to large societal damage.
3. Effective boosters
The final major piece of encouraging news involves booster shots: They are highly effective at preventing severe illness from Omicron. The protection is “remarkably high,” as Dr. Eric Topol of Scripps Research wrote.
Switzerland has begun reporting Covid deaths among three different groups of people: the unvaccinated; the vaccinated who have not received a booster shot; and the vaccinated who have been boosted (typically with a third shot). The first two shots still provide a lot of protection, but the booster makes a meaningful difference, as Edouard Mathieu and Max Roser of Our World in Data have noted:
The next stage
The Covid situation in the U.S. remains fairly grim, with overwhelmed hospitals and nearly 2,000 deaths a day. It’s likely to remain grim into early February. Caseloads are still high in many communities, and death trends typically lag case trends by three weeks.
But the full picture is less grim than the current moment.
Omicron appears to be in retreat, even if the official national data doesn’t yet reflect that reality. Omicron also appears to be mild in a vast majority of cases, especially for the vaccinated. This combination means that the U.S. may be only a few weeks away from the most encouraging Covid situation since early last summer, before the Delta variant emerged.
If that happens — and there is no guarantee it will, as Katherine Wu of The Atlantic explains — it will be time to ask how society can move back toward normalcy and reduce the harsh toll that pandemic isolation has inflicted, particularly on children and disproportionately on low-income children.
When should schools resume all activities? When should offices reopen? When should masks come off? When should asymptomatic people stop interrupting their lives because of a Covid exposure? Above all, when does Covid prevention do more harm — to physical and mental health — than good?
These are tricky questions, and they could often sound inappropriate during the Omicron surge. Now, though, the surge is receding.
Hospitals across the U.S. are feeling the wrath of the omicron variant and getting thrown into disarray that is different from earlier COVID-19 surges.
This time, they are dealing with serious staff shortages because so many health care workers are getting sick with the fast-spreading variant. People are showing up at emergency rooms in large numbers in hopes of getting tested for COVID-19, putting more strain on the system. And a surprising share of patients — two-thirds in some places — are testing positive while in the hospital for other reasons.
At the same time, hospitals say the patients aren’t as sick as those who came in during the last surge. Intensive care units aren’t as full, and ventilators aren’t needed as much as they were before.
The pressures are nevertheless prompting hospitals to scale back non-emergency surgeries and close wards, while National Guard troops have been sent in in several states to help at medical centers and testing sites.
Nearly two years into the pandemic, frustration and exhaustion are running high among health care workers.
“This is getting very tiring, and I’m being very polite in saying that,” said Dr. Robert Glasgow of University of Utah Health, which has hundreds of workers out sick or in isolation.
About 85,000 Americans are in the hospital with COVID-19, just short of the delta-surge peak of about 94,000 in early September, according to the Centers for Disease Control and Prevention. The all-time high during the pandemic was about 125,000 in January of last year.
But the hospitalization numbers do not tell the whole story. Some cases in the official count involve COVID-19 infections that weren’t what put the patients in the hospital in the first place.
Dr. Fritz François, chief of hospital operations at NYU Langone Health in New York City, said about 65% of patients admitted to that system with COVID-19 recently were primarily hospitalized for something else and were incidentally found to have the virus.
At two large Seattle hospitals over the past two weeks, three-quarters of the 64 patients testing positive for the coronavirus were admitted with a primary diagnosis other than COVID-19.
Joanne Spetz, associate director of research at the Healthforce Center at the University of California, San Francisco, said the rising number of cases like that is both good and bad.
The lack of symptoms shows vaccines, boosters and natural immunity from prior infections are working, she said. The bad news is that the numbers mean the coronavirus is spreading rapidly, and some percentage of those people will wind up needing hospitalization.
This week, 36% of California hospitals reported critical staffing shortages. And 40% are expecting such shortages.
Some hospitals are reporting as much as one quarter of their staff out for virus-related reasons, said Kiyomi Burchill, the California Hospital Association’s vice president for policy and leader on pandemic matters.
In response, hospitals are turning to temporary staffing agencies or transferring patients out.
University of Utah Health plans to keep more than 50 beds open because it doesn’t have enough nurses. It is also rescheduling surgeries that aren’t urgent. In Florida, a hospital temporarily closed its maternity ward because of staff shortages.
In Alabama, where most of the population is unvaccinated, UAB Health in Birmingham put out an urgent request for people to go elsewhere for COVID-19 tests or minor symptoms and stay home for all but true emergencies. Treatment rooms were so crowded that some patients had to be evaluated in hallways and closets.
As of Monday, New York state had just over 10,000 people in the hospital with COVID-19, including 5,500 in New York City. That’s the most in either the city or state since the disastrous spring of 2020.
New York City hospital officials, though, reported that things haven’t become dire. Generally, the patients aren’t as sick as they were back then. Of the patients hospitalized in New York City, around 600 were in ICU beds.
“We’re not even halfway to what we were in April 2020,” said Dr. David Battinelli, the physician-in-chief for Northwell Health, New York state’s largest hospital system.
Similarly, in Washington state, the number of COVID-19-infected people on ventilators increased over the past two weeks, but the share of patients needing such equipment dropped.
In South Carolina, which is seeing unprecedented numbers of new cases and a sharp rise in hospitalizations, Gov. Henry McMaster took note of the seemingly less-serious variant and said: “There’s no need to panic. Be calm. Be happy.”
Amid the omicron-triggered surge in demand for COVID-19 testing across the U.S., New York City’s Fire Department is asking people not to call for ambulance just because they are having trouble finding a test.
In Ohio, Gov. Mike DeWine announced new or expanded testing sites in nine cities to steer test-seekers away from ERs. About 300 National Guard members are being sent to help out at those centers.
In Connecticut, many ER patients are in beds in hallways, and nurses are often working double shifts because of staffing shortages, said Sherri Dayton, a nurse at the Backus Plainfield Emergency Care Center. Many emergency rooms have hours-long waiting times, she said.
“We are drowning. We are exhausted,” Dayton said.
Doctors and nurses are complaining about burnout and a sense their neighbors are no longer treating the pandemic as a crisis, despite day after day of record COVID-19 cases.
“In the past, we didn’t have the vaccine, so it was us all hands together, all the support. But that support has kind of dwindled from the community, and people seem to be moving on without us,” said Rachel Chamberlin, a nurse at New Hampshire’s Dartmouth-Hitchcock Medical Center.
Edward Merrens, chief clinical officer at Dartmouth-Hitchcock Health, said more than 85% of the hospitalized COVID-19 patients were unvaccinated.
Several patients in the hospital’s COVID-19 ICU unit were on ventilators, a breathing tube down their throats. In one room, staff members made preparations for what they feared would be the final family visit for a dying patient.
One of the unvaccinated was Fred Rutherford, a 55-year-old from Claremont, New Hampshire. His son carried him out of the house when he became sick and took him to the hospital, where he needed a breathing tube for a while and feared he might die.
If he returns home, he said, he promises to get vaccinated and tell others to do so too.
“I probably thought I was immortal, that I was tough,” Rutherford said, speaking from his hospital bed behind a window, his voice weak and shaky.
But he added: “I will do anything I can to be the voice of people that don’t understand you’ve got to get vaccinated. You’ve got to get it done to protect each other.”
Even as daily new COVID cases set all-time records and hospitals fill up, epidemiologists have arrived at a perhaps surprising consensus. Yes, the latest Omicron variant of the novel coronavirus is bad. But it could have been a lot worse.
Even as cases have surged, deaths haven’t—at least not to the same degree. Omicron is highly transmissible but generally not as severe as some older variants—“lineages” is the scientific term.
We got lucky. But that luck might not hold. Many of the same epidemiologists who have breathed a sigh of relief over Omicron’s relatively low death rate are anticipating that the next lineage might be much worse.
Fretting over a possible future lineage that combines Omicron’s extreme transmissibility with the severity of, say, the previous Delta lineage, experts are beginning to embrace a new public health strategy that’s getting an early test run in Israel: a four-shot regimen of messenger-RNA vaccine.
“I think this will be the strategy going forward,” Edwin Michael, an epidemiologist at the Center for Global Health Infectious Disease Research at the University of South Florida, told The Daily Beast.
Omicron raised alarms in health agencies all over the world in late November after officials in South Africa reported the first cases. Compared to older lineages, Omicron features around 50 key mutations, some 30 of which are on the spike protein that helps the virus to grab onto our cells.
Some of the mutations are associated with a virus’s ability to dodge antibodies and thus partially evade vaccines. Others are associated with higher transmissibility. The lineage’s genetic makeup pointed to a huge spike in infections in the unvaccinated as well as an increase in milder “breakthrough” infections in the vaccinated.
That’s exactly what happened. Health officials registered more than 10 million new COVID cases the first week of January. That’s nearly double the previous worst week for new infections, back in May. Around 3 million of those infections were in the United States, where Omicron coincided with the Thanksgiving, Christmas, and New Year holidays and associated traveling and family gatherings.
But mercifully, deaths haven’t increased as much as cases have. Worldwide, there were 43,000 COVID deaths the first week of January—fewer than 10,000 of them in the U.S. While deaths tend to lag infections by a couple weeks, Omicron has been dominant long enough that it’s increasingly evident there’s been what statisticians call a “decoupling” of cases and fatalities.
“We can say we dodged a bullet in that Omicron does not appear to cause as serious of a disease,” Stephanie James, the head of a COVID testing lab at Regis University in Colorado, told The Daily Beast. She stressed that data is still being gathered, so we can’t be certain yet that the apparent decoupling is real.
Assuming the decoupling is happening, experts attribute it to two factors. First, Omicron tends to infect the throat without necessarily descending to the lungs, where the potential for lasting or fatal damage is much, much higher. Second, by now, countries have administered nearly 9.3 billion doses of vaccine—enough for a majority of the world’s population to have received at least one dose.
In the United States, 73 percent of people have gotten at least one dose. Sixty-two percent have gotten two doses of the best mRNA vaccines. A third have received a booster dose.
Yes, Omicron has some ability to evade antibodies, meaning the vaccines are somewhat less effective against this lineage than they are against Delta and other older lineages. But even when a vaccine doesn’t prevent an infection, it usually greatly reduces its severity.
For many vaccinated people who’ve caught Omicron, the resulting COVID infection is mild. “A common cold or some sniffles in a fully vaxxed and boosted healthy individual,” is how Eric Bortz, a University of Alaska-Anchorage virologist and public health expert, described it to The Daily Beast.
All that is to say, Omicron could have been a lot worse. Viruses evolve to survive. That can mean greater transmissibility, antibody-evasion or more serious infection. Omicron mutated for the former two. There’s a chance some future Sigma or Upsilon lineage could do all three.
When it comes to viral mutations, “extreme events can occur at a non-negligible rate, or probability, and can lead to large consequences,” Michael said. Imagine a lineage that’s as transmissible as Omicron but also attacks the lungs like Delta tends to do. Now imagine that this hypothetical lineage is even more adept than Omicron at evading the vaccines.
That would be the nightmare lineage. And it’s entirely conceivable it’s in our future. There are enough vaccine holdouts, such as the roughly 50 million Americans who say they’ll never get jabbed, that the SARS-CoV-2 pathogen should have ample opportunities for mutation.
“As long as we have unvaccinated people in this country—and across the globe—there is the potential for new and possibly more concerning viral variants to arise,” Aimee Bernard, a University of Colorado immunologist, told The Daily Beast.
Worse, this ongoing viral evolution is happening against a backdrop of waning immunity. Antibodies, whether vaccine-induced or naturally occurring from past infection, fade over time. It’s not for no reason that health agencies in many countries urge booster doses just three months after initial vaccination. The U.S. Centers for Disease Control and Prevention is an outlier, and recommends people get boosted after five months.
A lineage much worse than Omicron could evolve at the same time that antibodies wane in billions of people all over the world. That’s why many experts believe the COVID vaccines will end up being annual or even semi-annual jabs. You’ll need a fourth jab, a fifth jab, a sixth jab, et cetera, forever.
Israel, a world leader in global health, is already turning that expectation into policy. Citing multiple studies that showed a big boost in antibodies with an additional dose of mRNA and no safety concerns, the country’s health ministry this week began offering a fourth dose to anyone over the age of 60, who tend to be more vulnerable to COVID than younger people.
That should be the standard everywhere, Ali Mokdad, a professor of health metrics sciences at the University of Washington Institute for Health, told The Daily Beast. “Scientifically, they’re right,” he said of the Israeli health officials.
If there’s a downside, it’s that there are still a few poorer countries—in Africa, mostly—where many people still struggle to get access to any vaccine, let alone boosters and fourth doses. If and when other richer countries follow Israel’s lead and begin offering additional jabs, there’s some risk of even greater inequity in global vaccine distribution.
“The downside is for the rest of the world,” Mokdad said. “I’m waiting to get my first dose and you guys are getting a fourth?”
The solution isn’t to deprive people of the doses they need to maintain their protection against future—and potentially more dangerous—lineages. The solution, for vaccine-producing countries, is to further boost production and double down on efforts to push vaccines out to the least privileged communities.
A sense of urgency is key. For all its rapid spread, Omicron has actually gone fairly easy on us. Sigma or Upsilon might not.
America was not prepared for COVID-19 when it arrived. It was not prepared for last winter’s surge. It was not prepared for Delta’s arrival in the summer or its current winter assault. More than 1,000 Americans are still dying of COVID every day, and more have died this year than last. Hospitalizations are rising in 42 states. The University of Nebraska Medical Center in Omaha, which entered the pandemic as arguably the best-prepared hospital in the country, recently went from 70 COVID patients to 110 in four days, leaving its staff “grasping for resolve,” the virologist John Lowe told me. And now comes Omicron.
Will the new and rapidly spreading variant overwhelm the U.S. health-care system? The question is moot because the system is already overwhelmed, in a way that is affecting all patients, COVID or otherwise. “The level of care that we’ve come to expect in our hospitals no longer exists,” Lowe said.
The real unknown is what an Omicron cross will do when it follows a Delta hook. Given what scientists have learned in the three weeks since Omicron’s discovery, “some of the absolute worst-case scenarios that were possible when we saw its genome are off the table, but so are some of the most hopeful scenarios,” Dylan Morris, an evolutionary biologist at UCLA, told me. In any case, America is not prepared for Omicron. The variant’s threat is far greater at the societal level than at the personal one, and policy makers have already cut themselves off from the tools needed to protect the populations they serve. Like the variants that preceded it, Omicron requires individuals to think and act for the collective good—which is to say, it poses a heightened version of the same challenge that the U.S. has failed for two straight years, in bipartisan fashion.
The coronavirus is a microscopic ball studded with specially shaped spikes that it uses to recognize and infect our cells. Antibodies can thwart such infections by glomming onto the spikes, like gum messing up a key. But Omicron has a crucial advantage: 30-plus mutations that change the shape of its spike and disable many antibodies that would have stuck to other variants. One early study suggests that antibodies in vaccinated people are about 40 times worse at neutralizing Omicron than the original virus, and the experts I talked with expect that, as more data arrive, that number will stay in the same range. The implications of that decline are still uncertain, but three simple principles should likely hold.
First, the bad news: In terms of catching the virus, everyone should assume that they are less protected than they were two months ago. As a crude shorthand, assume that Omicron negates one previous immunizing event—either an infection or a vaccine dose. Someone who considered themselves fully vaccinated in September would be just partially vaccinated now (and the official definition may change imminently). But someone who’s been boosted has the same ballpark level of protection against Omicron infection as a vaccinated-but-unboosted person did against Delta. The extra dose not only raises a recipient’s level of antibodies but also broadens their range, giving them better odds of recognizing the shape of even Omicron’s altered spike.In a small British study, a booster effectively doubled the level of protection that two Pfizer doses provided against Omicron infection.
Second, some worse news: Boosting isn’t a foolproof shield against Omicron. In South Africa, the variant managed to infect a cluster of seven people who were all boosted. And according to a CDC report, boosted Americans made up a third of the first known Omicron cases in the U.S. “People who thought that they wouldn’t have to worry about infection this winter if they had their booster do still have to worry about infection with Omicron,” Trevor Bedford, a virologist at Fred Hutchinson Cancer Research Center, told me. “I’ve been going to restaurants and movies, and now with Omicron, that will change.”
Third, some better news: Even if Omicron has an easier time infecting vaccinated individuals, it should still have more trouble causing severe disease. The vaccines were always intended to disconnect infection from dangerous illness, turning a life-threatening event into something closer to a cold. Whether they’ll fulfill that promise for Omicron is a major uncertainty, but we can reasonably expect that they will. The variant might sneak past the initial antibody blockade, but slower-acting branches of the immune system (such as T cells) should eventually mobilize to clear it before it wreaks too much havoc.
To see how these principles play out in practice, Dylan Morris suggests watching highly boosted places, such as Israel, and countries where severe epidemics and successful vaccination campaigns have given people layers of immunity, such as Brazil and Chile. In the meantime, it’s reasonable to treat Omicron as a setback but not a catastrophe for most vaccinated people. It will evade some of our hard-won immune defenses, without obliterating them entirely. “It was better than I expected, given the mutational profile,” Alex Sigal of the Africa Health Research Institute, who led the South African antibody study, told me. “It’s not going to be a common cold, but neither do I think it will be a tremendous monster.”
That’s for individuals, though. At a societal level, the outlook is bleaker.
Omicron’s main threat is its shocking speed, as my colleague Sarah Zhang has reported. In South Africa, every infected person has been passing the virus on to 3–3.5 other people—at least twice the pace at which Delta spread in the summer. Similarly, British data suggest that Omicron is twice as good at spreading within households as Delta. That might be because the new variant is inherently more transmissible than its predecessors, or because it is specifically better at moving through vaccinated populations. Either way, it has already overtaken Delta as the dominant variant in South Africa. Soon, it will likely do the same in Scotland and Denmark. Even the U.S., which has much poorer genomic surveillance than those other countries, has detected Omicron in 35 states. “I think that a large Omicron wave is baked in,” Bedford told me. “That’s going to happen.”
More positively, Omicron cases have thus far been relatively mild. This pattern has fueled the widespread claim that the variant might be less severe, or even that its rapid spread could be a welcome development. “People are saying ‘Let it rip’ and ‘It’ll help us build more immunity,’ that this is the exit wave and everything’s going to be fine and rosy after,” Richard Lessells, an infectious-disease physician at the University of KwaZulu-Natal, in South Africa, told me. “I have no confidence in that.”
To begin with, as he and others told me, that argument overlooks a key dynamic: Omicron might not actually be intrinsically milder. In South Africa and the United Kingdom, it has mostly infected younger people, whose bouts of COVID-19 tend to be less severe. And in places with lots of prior immunity, it might have caused few hospitalizations or deaths simply because it has mostly infected hosts with some protection, as Natalie Dean, a biostatistician at Emory University, explained in a Twitter thread. That pattern could change once it reaches more vulnerable communities. (The widespread notion that viruses naturally evolve to become less virulent is mistaken, as the virologist Andrew Pekosz of Johns Hopkins University clarified in The New York Times.) Also, deaths and hospitalizations are not the only fates that matter. Supposedly “mild” bouts of COVID-19 have led to cases of long COVID, in which people struggle with debilitating symptoms for months (or even years), while struggling to get care or disability benefits.
And even if Omicron is milder, greater transmissibility will likely trump that reduced virulence. Omicron is spreading so quickly that a small proportion of severe cases could still flood hospitals. To avert that scenario, the variant would need to be substantially milder than Delta—especially because hospitals are already at a breaking point. Two years of trauma have pushed droves of health-care workers, including many of the most experienced and committed, to quit their job. The remaining staff is ever more exhausted and demoralized, and “exceptionally high numbers” can’t work because they got breakthrough Delta infections and had to be separated from vulnerable patients, John Lowe told me. This pattern will only worsen as Omicron spreads, if the large clusters among South African health-care workers are any indication. “In the West, we’ve painted ourselves into a corner because most countries have huge Delta waves and most of them are stretched to the limit of their health-care systems,” Emma Hodcroft, an epidemiologist at the University of Bern, in Switzerland, told me. “What happens if those waves get even bigger with Omicron?”
The Omicron wave won’t completely topple America’s wall of immunity but will seep into its many cracks and weaknesses. It will find the 39 percent of Americans who are still not fully vaccinated (including 28 percent of adults and 13 percent of over-65s). It will find other biologically vulnerable people, including elderly and immunocompromised individuals whose immune systems weren’t sufficiently girded by the vaccines. It will find the socially vulnerable people who face repeated exposures, either because their “essential” jobs leave them with no choice or because they live in epidemic-prone settings, such as prisons and nursing homes. Omicron is poised to speedily recap all the inequities that the U.S. has experienced in the pandemic thus far.
Here, then, is the problem: People who are unlikely to be hospitalized by Omicron might still feel reasonably protected, but they can spread the virus to those who are more vulnerable, quickly enough to seriously batter an already collapsing health-care system that will then struggle to care for anyone—vaccinated, boosted, or otherwise. The collective threat is substantially greater than the individual one. And the U.S. is ill-poised to meet it.
America’s policy choices have left it with few tangible options for averting an Omicron wave. Boosters can still offer decent protection against infection, but just 17 percent of Americans have had those shots. Many are now struggling to make appointments, and people from rural, low-income, and minority communities will likely experience the greatest delays, “mirroring the inequities we saw with the first two shots,” Arrianna Marie Planey, a medical geographer at the University of North Carolina at Chapel Hill, told me. With a little time, the mRNA vaccines from Pfizer and Moderna could be updated, but “my suspicion is that once we have an Omicron-specific booster, the wave will be past,” Trevor Bedford, the virologist, said.
Two antiviral drugs now exist that could effectively keep people out of the hospital, but neither has been authorized and both are expensive. Both must also be administered within five days of the first symptoms, which means that people need to realize they’re sick and swiftly confirm as much with a test. But instead of distributing rapid tests en masse, the Biden administration opted to merely make them reimbursable through health insurance. “That doesn’t address the need where it is greatest,” Planey told me. Low-wage workers, who face high risk of infection, “are the least able to afford tests up front and the least likely to have insurance,” she said. And testing, rapid or otherwise, is about to get harder, as Omicron’s global spread strains both the supply of reagents and the capacity of laboratories.
Omicron may also be especially difficult to catch before it spreads to others, because its incubation period—the window between infection and symptoms—seems to be very short. At an Oslo Christmas party, almost three-quarters of attendees were infected even though all reported a negative test result one to three days before. That will make Omicron “harder to contain,” Lowe told me. “It’s really going to put a lot of pressure on the prevention measures that are still in place—or rather, the complete lack of prevention that’s still in place.”
The various measures that controlled the spread of other variants—masks, better ventilation, contact tracing, quarantine, and restrictions on gatherings—should all theoretically work for Omicron too. But the U.S. has either failed to invest in these tools or has actively made it harder to use them. Republican legislators in at least 26 states have passed laws that curtail the very possibility of quarantines and mask mandates. In September, Alexandra Phelan of Georgetown University told me that when the next variant comes, such measures could create “the worst of all worlds” by “removing emergency actions, without the preventive care that would allow people to protect their own health.” Omicron will test her prediction in the coming weeks.
The longer-term future is uncertain. After Delta’s emergence, it became clear that the coronavirus was too transmissible to fully eradicate. Omicron could potentially shunt us more quickly toward a different endgame—endemicity, the point when humanity has gained enough immunity to hold the virus in a tenuous stalemate—albeit at significant cost. But more complicated futures are also plausible. For example, if Omicron and Delta are so different that each can escape the immunity that the other induces, the two variants could co-circulate. (That’s what happened with the viruses behind polio and influenza B.)
Omicron also reminds us that more variants can still arise—and stranger ones than we might expect. Most scientists I talked with figured the next one to emerge would be a descendant of Delta, featuring a few more mutational bells and whistles. Omicron, however, is “dramatically different,” Shane Crotty, from the La Jolla Institute for Immunology, told me. “It showed a lot more evolutionary potential than I or others had hoped for.” It evolved not from Delta but from older lineages of SARS-CoV-2, and seems to have acquired its smorgasbord of mutations in some hidden setting: perhaps a part of the world that does very little sequencing, or an animal species that was infected by humans and then transmitted the virus back to us, or the body of an immunocompromised patient who was chronically infected with the virus. All of these options are possible, but the people I spoke with felt that the third—the chronically ill patient—was most likely. And if that’s the case, with millions of immunocompromised people in the U.S. alone, many of whom feel overlooked in the vaccine era, will more weird variants keep arising? Omicron “doesn’t look like the end of it,” Crotty told me. One cause for concern: For all the mutations in Omicron’s spike, it actually has fewer mutations in the rest of its proteins than Delta did. The virus might still have many new forms to take.
Vaccinating the world can curtail those possibilities, and is now an even greater matter of moral urgency, given Omicron’s speed. And yet, people in rich countries are getting their booster six times faster than those in low-income countries are getting their first shot. Unless the former seriously commits to vaccinating the world—not just donating doses, but allowing other countries to manufacture and disseminate their own supplies—“it’s going to be a very expensive wild-goose chase until the next variant,” Planey said.
Vaccines can’t be the only strategy, either. The rest of the pandemic playbook remains unchanged and necessary: paid sick leave and other policies that protect essential workers, better masks, improved ventilation, rapid tests, places where sick people can easily isolate, social distancing, a stronger public-health system, and ways of retaining the frayed health-care workforce. The U.S. has consistently dropped the ball on many of these, betting that vaccines alone could get us out of the pandemic. Rather than trying to beat the coronavirus one booster at a time, the country needs to do what it has always needed to do—build systems and enact policies that protect the health of entire communities, especially the most vulnerable ones.