The Supreme Court on Friday upheld a key Affordable Care Act requirement that insurance companies cover certain preventative measures recommended by an expert panel.
Justices upheld the constitutionality of the provision in a 6-3 decision and protected access to preventative care for about 150 million Americans.
The justices found that the secretary of the Department of Health and Human Services has the power to appoint and fire members of the U.S. Preventative Services Task Force (USPSTF).
The cases started when a small business in Texas and some individuals filed a lawsuit against the panel’s recommendation that pre-exposure prophylaxis (PreP) for HIV be included as a preventative care service.
They argued that covering PreP went against their religious beliefs and would “encourage homosexual behavior, intravenous drug use, and sexual activity outside of marriage between one man and one woman.”
The plaintiffs further argued that the USPSTF mandates are unconstitutional because panel members are “inferior officers” who are not appointed by the president or confirmed by the Senate.
While the panel is independent, they said that since their decisions impact millions of people members should be confirmed.
A U.S. district judge in 2023 ruled that all preventative-care coverage imposed since the ACA was signed into law areinvalid and a federal appeals court judge ruled in agreement last year.
The Biden administration appealed the rulings to the Supreme Court, and the Trump administration chose to defend the law despite its long history of disparaging Obamacare.
Though public health groups celebrated the ruling Friday, some noted another potential outcome.
“While this is a foundational victory for patients, patients have reason to be concerned that the decision reaffirms the ability of the HHS secretary, including our current one, to control the membership and recommendations of the US Preventive Services Task Force that determines which preventive services are covered,” Anthony Wright, executive director of Families USA, said in a statement.
“We must be vigilant to ensure Secretary Kennedy does not undo coverage of preventive services by taking actions such as his recent firing of qualified health experts from the CDC’s independent vaccine advisory committee and replacing them with his personal allies.”
In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
Two pioneers of mRNA research — the technology that helped the world tame the virus behind the Covid-19 pandemic — won the 2023 Nobel Prize in medicine or physiology on Monday.
Overcoming a lack of broader interest in their work and scientific challenges, Katalin Karikó and Drew Weissman made key discoveries about messenger RNA that enabled scientific teams to start developing the tool into therapies, immunizations, and — as the pandemic spread in 2020 — vaccines targeting the SARS-CoV-2 coronavirus. Moderna and the Pfizer-BioNTech partnership unveiled their mRNA-based Covid-19 shots in record time thanks to the foundational work of Karikó and Weissman, helping save millions of lives.
Karikó, a biochemist, and Weissman, an immunologist, performed their world-changing research on the interaction between mRNA and the immune system at the University of Pennsylvania, where Weissman, 64, remains a professor in vaccine research. Karikó, 68, who later went to work at BioNTech, is now a professor at Szeged University in her native Hungary, and is an adjunct professor at Penn’s Perelman School of Medicine.
The duo will receive 11 million Swedish kronor, or just over $1 million. Their names are added to a list of medicine or physiology Nobel winners that prior to this year included 213 men and 12 women.
The award was announced by Thomas Perlmann, secretary general of Nobel Assembly, in Stockholm. Perlmann said he had spoken to both laureates, describing them as grateful and surprised even though the pair has won numerous awards seen as precursors and had been tipped as likely Nobel recipients at some point.
Every year, the committee considers hundreds of nominations from former Nobel laureates, medical school deans, and prominent scientists from fields including microbiology, immunology, and oncology. Members try to identify a discovery that has altered scientists’ understanding of a subject. And according to the criteria laid out in Alfred Nobel’s will, that paradigm-shifting discovery also has to have benefited humankind.
The Nobel committee framed Karikó and Weissman’s work as a prime example of complementary expertise, with Karikó focused on RNA-based therapies and Weissman bringing a deep knowledge about immune responses to vaccines.
But it was not an easy road for the scientists. Karikó encountered rejection after rejection in the 1990s while applying for grants. She was even demoted while working at Penn, as she toiled away on the lower rungs of academia.
But the scientists persisted, and made a monumental discovery published in 2005 based on simply swapping out some of the components of mRNA.
With instructions from DNA, our cells make strands of mRNA that are then “read” to make proteins. The idea underlying an mRNA vaccine then is to take a piece of mRNA from a pathogen and slip it into our bodies. The mRNA will lead to the production of a protein from the virus, which our bodies learn to recognize and fight should we encounter it again in the form of the actual virus.
It’s an idea that goes back to the 1980s, as scientific advances allowed researchers to make mRNA easily in their labs. But there was a problem: The synthetic mRNA not only produced smaller amounts of protein than the natural version in our cells, it also elicited a potentially dangerous inflammatory immune response, and was often destroyed before it could reach target cells.
Karikó and Weissman’s breakthrough focused on how to overcome that problem. mRNA is made up of four nucleosides, or “letters”: A, U, G, and C. But the version our bodies make includes some nucleosides that are chemically modified — something the synthetic version didn’t, at least until Karikó and Weissman came along. They showed that subbing out some of the building blocks for modified versions allowed their strands of mRNA to sneak past the body’s immune defenses.
While the research did not gain wide attention at the time, it did catch the attention of scientists who would go on to found Moderna and BioNTech. And now, nearly 20 years later, billions of doses of mRNA vaccines have been administered.
For now, the only authorized mRNA products are the Covid-19 shots. But academic researchers and companies are exploring the technology as a potential therapeutic platform for an array of diseases and are using it to develop cancer vaccines as well as immunizations against other infectious diseases, from flu to mpox to HIV. An mRNA vaccine is highly adaptable compared to earlier methods, which makes it easier to alter the underlying recipe of the shot to keep up with viral evolution.
As she gained global fame, Karikó has been open about the barriers she encountered in her scientific career, which raised broader issues about the challenges women and immigrants can face in academia. But she’s said she always believed in the potential of her RNA research.
“I thought of going somewhere else, or doing something else,” Karikó told STAT in 2020, recalling the moment she was demoted. “I also thought maybe I’m not good enough, not smart enough. I tried to imagine: Everything is here, and I just have to do better experiments.”
The highly contagious disease dates to ancient times and spread easily in households and classrooms—until the development of a vaccine.
Chickenpox is a highly contagious disease caused by the varicella-zoster virus that leads to itchy skin eruptions, which are sometimes compared to a “dew drop on a rose petal.”
Until the development of a chickenpox vaccine in the late 20th century, the disease was a common childhood illness that could cause serious health problems in people who didn’t contract the disease until adulthood. More than four million people got chickenpox every year in the United States, resulting in more than 10,000 hospitalizations and 100 deaths. Since vaccinations began, those numbers dropped significantly.
The CDC reports that fewer than 350,000 people contract the disease per year, and that there are fewer than 1,700 hospitalizations and 20 deaths annually from chickenpox.
Where Did Chicken Pox Come From?
There’s evidence of chickenpox dating back to ancient times, and the earliest known use of the term “chickenpox” dates to 1691—although it’s not clear how it got this name. It’s believed the disease was brought to the Americas in the 15th century by European explorers and settlers. Once on the continent, it (and other diseases) spread among Native Americans since Indigenous people had not previously been exposed to the virus.
Before the 18th century, diseases that appeared to produce “pox,” or skin eruptions, were commonly lumped together. This included chickenpox, smallpox and syphilis, which was known as “large pox” or the “great pox.” The first scientist to provide a detailed description of chickenpox differentiating it from smallpox was the English physician William Heberden. In 1767, he noted the physical differences between the two diseases, and also recorded that people who’d had chickenpox “were not capable of having it again.”
It wasn’t until later that scientists realized chickenpox was related to shingles. In the late 19th and early 20th centuries, Hungarian pediatrician James von Bokay observed several instances in which younger people seemed to contract chickenpox after being exposed to someone with shingles, a disease that can cause nerve damage if not treated properly. This led him to suggest that there was a link between the two diseases.
Scientists later confirmed this theory by discovering that after a person recovers from chickenpox, the varicella-zoster virusstays in his or her body, and can cause the person to develop shingles later on.
Chicken Pox Virus Is ID’d in the 1950s
In the 1950s, scientists isolated the varicella-zoster virus for the first time, paving the way for efforts to vaccinate against chickenpox and shingles. After that, it took several decades to develop and distribute vaccines for these illnesses. The U.S. Food and Drug Administration approved the first chickenpox vaccine in 1995 and the first shingles vaccine in 2006.
Compared to other childhood vaccines, the chickenpox vaccine was a relatively late development. Maurice Hilleman, who helped develop a measles vaccine in the 1960s, had also tried to push for a chickenpox vaccine around that time. However, diseases ended up receiving higher priority depending on the rate of death and disability associated with them, writes epidemiologist René Najera, editor of The History of Vaccines, an online resource by The College of Physicians of Philadelphia, in an email to HISTORY.
“As a result, chickenpox fell toward the bottom of the list because it is a relatively mild disease in children,” he says. As new vaccines helped control more severe childhood diseases, chickenpox moved higher up on the list.
Contagiousness of Chickenpox
The CDC estimates that a person with chickenpox can spread it to up to 90 percent of the people with whom they come into contact who haven’t previously had chickenpox or the vaccine. In addition, the period in which a person is contagious lasts for several days. It begins one or two days before the chickenpox eruptions begin to show, and lasts until all the fluid-filled skin lesions have scabbed over. Typically, chickenpox lasts for 4 to 7 days.
Before the vaccine, chickenpox spread easily in households and classrooms, and was especially dangerous for adults who had never had it. Both children and adults may experience fever, fatigue and body aches with chickenpox, but in adults these symptoms can be more severe. Adults are 25 percent more likely than children to die from chickenpox, according to the National Foundation for Infectious Diseases. The disease can lead to health complications like bacterial infections, swelling of the brain and pneumonia.
Although the chickenpox vaccine has greatly slowed the spread of the disease in schools, outbreaks occur in some parts of the United States where parents have declined to vaccinate their children. This is similar to the way that childhood diseases like measles, which went from common to uncommon in the late 20th century, began to break out in schools again in the 21st century.
Still, with the widespread adoption of the chickenpox vaccine, the disease “has joined polio and measles in the list of infectious diseases that are candidates for eradication,” Najera says. So far, the only human disease that vaccines have globally eradicated is smallpox, but scientists and doctors hope to one day add more to the list of diseases that have been vanquished by vaccines.
Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
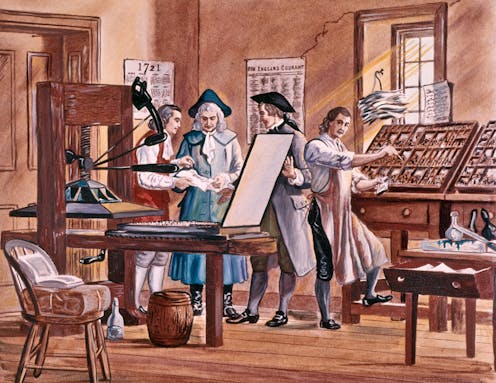
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
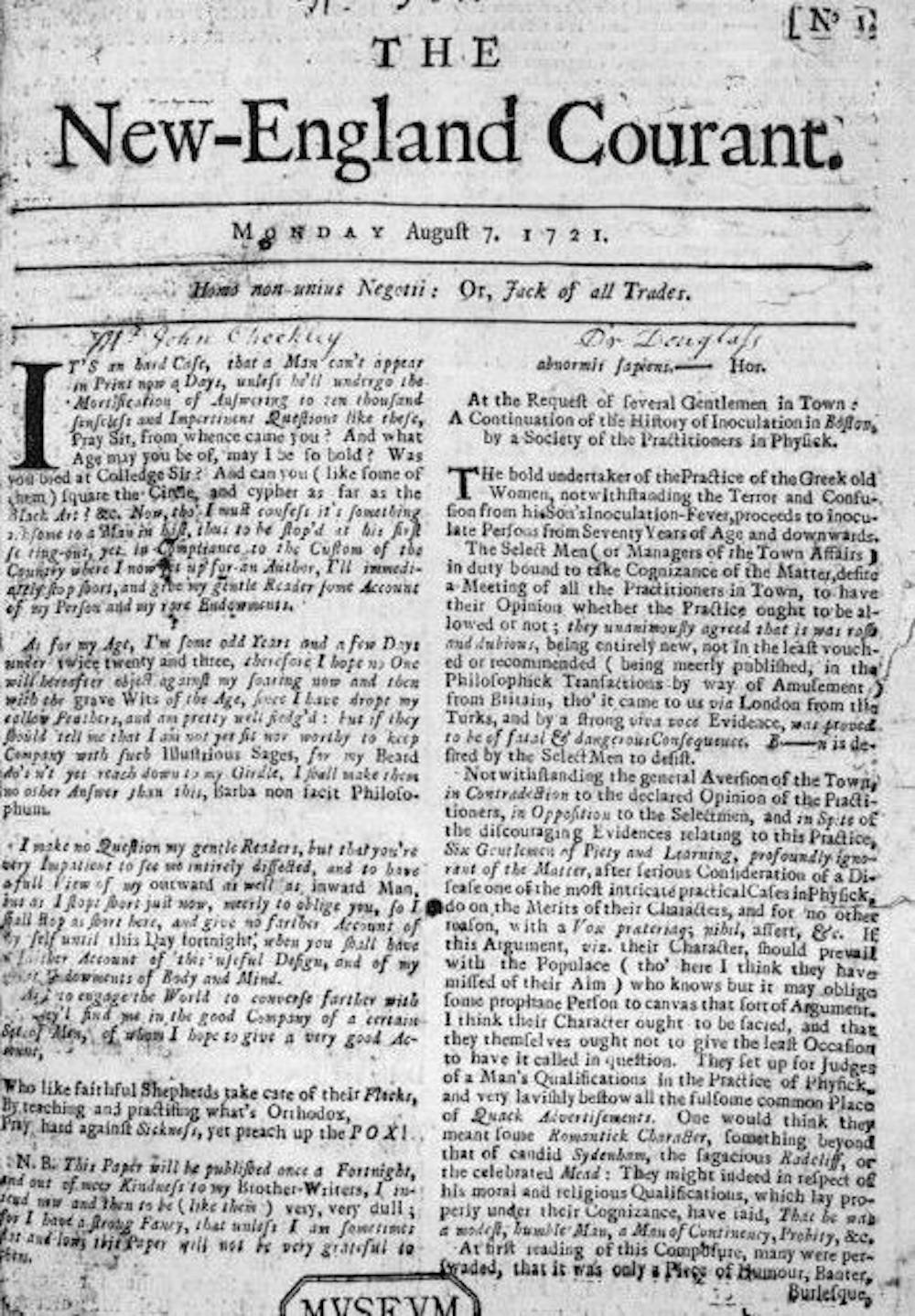
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
Part one of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation, dives into the history of variolation, exploring the beginning of the long road that led to vaccines as we know them today.
The following, which originally appeared on the Drivers of Health blog, is authored by Luke Testa, Program Assistant, The Harvard Global Health Institute.
In 2018, a short video circulated on WhatsApp claiming that the MMR vaccine was designed by Indian Prime Minister Narendra Modi to stop the population growth of Muslims. Subsequently, hundreds of madrassas across western Uttar Pradesh refused to allow health departments to vaccinate their constituents.
In 2020, a three-minute video claiming that the coronavirus vaccination campaign was secretly a plan by Bill Gates to implant trackable microchips in people wasone of the most widely shared pieces of misinformation online. Alongside a torrent of online COVID-19 vaccine falsehoods and conspiracy theories, sources of medical mis- and disinformation are fostering distrust in COVID-19 vaccines, undermining immunization efforts, and demonstrating how poor information is a determinant of health.
Medical misinformation, referring to inaccurate or unverified information that can drive misperceptions about medical practices or treatments, has flooded the infosphere (all types of information available online). Examples can vary from overrepresentations of anecdotes claiming that complications occurred following inoculation to misinterpretations of research findings by well-meaning individuals.
Considering the many ways in which medical misinformation can shape health behaviors, researchers at the Oxford Internet Institute recently suggested that the infosphere should be classified as a social determinant of health (SDOH) (designated alongside general socioeconomic, environmental, and cultural conditions). This classification, they argue, properly accounts for the correlation between exposure to poor quality information and poor health outcomes.
The connection between information quality and health has been especially pronounced during the COVID-19 pandemic. A 2021 study found that amongst those who indicated that they would definitely take a COVID-19 vaccine, exposure to misinformation induced a decline in intent of 6.2% in the U.K. and 6.4% in the U.S. Further, misinformation that appeared to be science-based was found to be especially damaging to vaccination intentions. These findings are particularly concerning considering the fact that during the pandemic, the 147 biggest anti-vaccine accounts on social media (which often purport to be science-based) gained 7.8 million followers in the first half of 2020, an increase of 19%.
During an unprecedented health crisis, medical misinformation within the infosphere is leaving both individuals and communities vulnerable to poor health outcomes.Those who are unvaccinated are at a higher risk of infection and increase the likelihood of community transmission. This places undue burden on those who cannot get vaccinated—due to inequities and/or preexisting conditions—and increases opportunities for variants to continue to mutate into more infectious and/or deadly forms of the virus. Poor quality information within the infosphere is undermining immunization efforts and threatens to prolong the ark of the pandemic.
Leveraging Healthcare Provider Influence in the Battle Against Poor Quality Information
Healthcare providers are uniquely suited to respond to this challenge. Throughout the pandemic, majorities of U.S. adults have identified their doctors and nurses as the most trustworthy sources of information about the coronavirus. In fact, 8 in 10 U.S. adults said that they are very or somewhat likely to turn to a doctor, nurse, or other healthcare provider when deciding whether or not to get a COVID-19 vaccine.
This influence is especially pertinent considering the state of vaccine resistance across the globe. In March 2021, a Kaiser Family Foundation poll found that 37% of U.S. respondents indicated some degree of resistance to vaccination. If that percentage of Americans remain unvaccinated, the country will be short of what is needed to achieve herd immunity (likely 70% or more vaccinated). Similar levels of resistance to vaccination remain high in countries across the globe, such as Lebanon, Serbia, Paraguay, and France.
Although medical misinformation is contributing to high rates of refusal, it is important to note that drivers of vaccine resistance are complex and intersectional. Vaccine distrust or refusal may be rooted in exposure to anti-vaccine rhetoric, racial injustice or medical exploitation in healthcare, fears that vaccine development was rushed, and/or other drivers. For this reason, responses must be tailored to unique individual or communal motivations. For example, experts have pressed the critical need for vaccine distrust within Black communities to be approached not as a shortcoming of community members, but as a failure of health systems to prove themselves as trustworthy.
With regard to resistance rooted in anti-COVID-19 vaccine misinformation, healthcare providers are leveraging their unique influence through novel, grassroots approaches to encourage vaccine uptake. In North Dakota, providers are recording videos and sending out messages to their patients communicating that they have been vaccinated and explaining why it is safe to do the same. On social media, a network of female doctors and scientists across various social media pages, such as Dear Pandemic (82,000 followers) and Your Local Epidemiologist (181,000 followers), are collaborating to answer medical questions, clear up misperceptions about COVID-19 vaccines, and provide communities with accurate information about the virus. Similarly, the #BetweenUsAboutUs online campaign is elevating conversations about vaccines with Black doctors, nurses, and researchers in an effort to increase vaccine confidence in BIPOC communities.This campaign is especially critical considering the fact that BIPOC communities are often the target of anti-vaccine groups in an effort to exploit existing, rational distrust in health systems.
In addition to these timely responses, evidence-based interventions offer promising opportunities for healthcare providers to improve vaccine uptake amongst their patients.For example, there is a growing consensus around the practice of motivational interviewing (MI).
MI is a set of patient-centered communication techniques that aim to enhance a patient’s intrinsic motivation to change health behaviors by tapping into their own arguments for change. The approach is based on empathetic, nonjudgmental patient-provider dialogue. In other words, as opposed to simply telling a patient why they should get vaccinated, a provider will include the patient in a problem-solving process that accounts for their unique motivations and helps them discover their own reasons for getting vaccinated.
When applying MI techniques to a conversation with a patient who is unsure if they should receive a vaccine, providers will use an “evoke-provide-evoke” approach where they will ask patients: 1) what they already know about the vaccine; 2) if the patient would like additional information about the vaccine (if yes, then provide the most up to date information); and 3) how the new information changes how they are thinking or feeling about vaccination. During these conversations, the MI framework encourages providers to ask open-ended questions, practice reflective listening, offer affirmations, elicit pros and cons of change, and summarize conversations, amongst other tools.
Numerous studies show motivational interviewing to be effective in increasing vaccine uptake. For example, one randomized controlled trial found that with parents in maternity wards, vaccine hesitancy fell by 40% after participation in an educational intervention based on MI. Given its demonstrated effectiveness, MI is likely to help reduce vaccine hesitancy during the COVID-19 pandemic.
With infectious disease outbreaks becoming more likely and resistance to various vaccines increasing across the globe, continuing to leverage healthcare providers’ unique influence through grassroots campaigns while honing motivational interviewing skills as a way to combat mis- and disinformation in the infosphere may prove critical to advancing public health now and in the future.
Part five of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation, continues to explore the history of societal backlash against vaccination, with particular attention to vaccine-adjacent incidents and misinformation.











{kind=link}