As Danville, Pa.-based Geisinger Health awaits the closure of a deal that will make it the first health system to join Kaiser Permanente’s new nonprofit organization, Risant Health, President and CEO Jaewon Ryu, MD, said the system must remain focused on driving its strategy forward with “the same rigor to address the challenging headwinds our industry and our communities continue to face.”
Oakland-based Kaiser said in a May 15 financial report that it expects its deal to acquire Geisinger to close in 2024, pending regulatory approval.
The newly created Risant Health, which will be headquartered in Washington, D.C., aims to “expand and accelerate the adoption of value-based care in “diverse, multipayer, multiprovider, community-based health system environments.”
Dr. Ryu will transition to the role of Risant Health CEO as the deal approaches closure. He recently connected with Becker’s about why Geisinger joined Risant and how the new organization will measure success.
Editor’s note: Responses have been lightly edited for brevity and clarity.
Q: Geisinger is the first health system to join Risant Health. How did Geisinger get involved and why did it decide to be the first to join?
Dr. Jaewon Ryu: This came on the heels of strategic planning work that we had started over four years ago, when we were looking at ways that we might accelerate our goal — to make better health easier for the communities we serve. This path with Kaiser Permanente through Risant Health presented a great way to join with a fellow nonprofit, mission-aligned organization that is like minded and focused on improving health outcomes, affordability and access. Kaiser Permanente has been a best-in-class organization of this approach for quite some time, often viewed as the gold standard in value-based care, with operations across eight states and the District of Columbia, 39 hospitals, and top-notch physician groups. And Geisinger has been similarly committed to advancing innovation and value-based care models, partnering with other payers and other physician groups and health systems to do so.
Being part of Risant Health will allow Geisinger to access tools, capabilities and investments required to accelerate our charitable mission and strategy and continue to expand our impact to our communities.
Q: What is the most exciting aspect of joining Risant?
JR: In addition to accelerating our ability to deliver on our mission and carrying forth the vision of our founder Abigail Geisinger, we’re excited to have a broader impact in healthcare.
We’ve always believed Geisinger’s model in Pennsylvania — with a focus on value-based care leveraging multipayer and multiprovider capabilities — could be scaled to other places and benefit more people and communities. This “pluralistic” approach to value-based care, across communities less dense than more urban areas, is a capability that complements Kaiser Permanente’s other capabilities. Through Risant Health, we see an opportunity to further enhance our model and add to the suite of Risant Health capabilities so that more communities can benefit. As the first health system to become part of Risant Health, Geisinger will participate in building out the organization’s strategy and operational model. Working with Kaiser Permanente and connecting with like-minded health systems through Risant Health will allow us to be a part of the solution for the industry’s challenges in a rapidly changing healthcare environment.
Q: The deal is now awaiting regulatory approval. As that process unfolds, what is Geisinger doing to prepare for the transition?
JR: Geisinger remains focused on delivering on our mission of making better health easier for the communities that we serve. In other words, our good work continues. Should the acquisition be approved, Risant Health’s model will be designed to support local ownership over operations and regional strategy while also preserving strong community engagement. This local ownership means that while we await a regulatory decision, but even beyond, we must remain focused on driving our strategy forward with the same rigor to address the challenging headwinds our industry and our communities continue to face.
Q: You will be transitioning into the role of Risant CEO. Will that be in addition to your role at Geisinger, or will the system be getting a new CEO? If the latter, is there a succession plan in place?
JR: I’m focused on my role as the president and CEO of Geisinger, ensuring our organization is delivering on our stated mission. Should we receive the necessary state and federal regulatory approvals, I will transition from my current role to serve as CEO of Risant Health as the transaction nears completion. While no definitive plans have been made, there will be a formal process to select a new CEO at the appropriate time, just as we have with prior leadership transitions.
Q: How will joining Risant benefit or enhance Geisinger’s health plan?
JR: Geisinger will deliver the same quality care programs, benefits coverage and prevention support. We will enhance our capabilities over time in areas such as digital tools that make things easier for our members, or using augmented data and analytic tools that help target care programs at the right time so that we can address clinical needs before disease worsens. So while Geisinger’s approach to care will remain one anchored around outcomes and caring, how we go about this work will be bolstered with these and other capabilities.
Q: How will the success of Risant Health be measured?
JR: Through Risant Health, Kaiser Permanente has shared its desire to seek out like-minded entities that are committed to quality care and improving access and affordability by promoting value-based care models through a “pluralistic” chassis, as mentioned earlier. In a very simple sense, success will be evaluated through better measures of health across more populations. For example, success could be lower blood sugars in diabetic patients, fewer ER or hospital visits for those with congestive heart failure or earlier detection of cancers through more effective preventive screening rates.
In the mid-1980’s, managed care advocate Dr. Paul Ellwood predicted that eventually, US healthcare would be dominated by perhaps a dozen vast national firms he called SuperMeds that would combine managed care based health insurance with care delivery systems. Ellwood was a leader of the “managed competition” movement which advocated for a private sector alternative to a federal government-run National Health Insurance system. Ellwood and colleagues believed that Kaiser Foundation Health Plans and other HMOs would be able to stabilize health costs and thus affordably extend care to the uninsured.
The US political system and market dynamics would not co-operate with Ellwood and his Jackson Hole Group’s vision. In the ensuing thirty-five years, healthcare has remained both highly fragmented and regional in focus. However, unbeknownst to most, during the past decade, as a result of a major merger and relentless smaller acquisitions, two SuperMeds were born- CVS/Aetna and UnitedHealth Group, that whose combined revenues comprise 14% of total US health spending.
CVS/Aetna is slightly larger than United, by dint of grocery sales in its drugstores and its vast Caremark pharmacy benefits management business. However, CVS’s Aetna health insurance arm is one third the size of United’s, and though CVS is rapidly scaling up its care delivery apparatus through its in-store Health Hubs, it remains is a tiny fraction of United’s care footprint. Despite being slightly smaller at the top line, United’s market capitalization is more than 3.5 times that of CVS.
United’s vast scope is difficult to comprehend because much of it is not visible to the naked eye, and the most rapidly growing businesses are partly nested inside United’s health insurance business.
United employs over 300 thousand people. At $287.6 billion total revenues in 2021, United exceeded 7% of total US health spending (though $8.3 billion are from overseas operations).
In 2021, United was $100 billion larger than the British National Health Service. It is more than three times the size of Kaiser Permanente, and five times the size of HCA, the nation’s largest hospital chain. United is both larger and richer than energy giant Exxon Mobil. United has over $70 billion in cash and investments, and is generating about $2 billion a month in operating cash flow.
Its highly regulated health insurance business is the visible tip of a rapidly growing iceberg. Revenue from United’s core health insurance business grew at 11% in 2021, compared to 14% growth in United’s diversified Optum subsidiary. Optum generated $155.6 billion in 2021 (of which 60% were from INSIDE United’s health insurance business). You can see the relationship of Optum’s three major businesses to United’s health insurance operations in Exhibit I.
Optum is the Key to United’s Growth
Understanding the role of Optum is key to understanding United’s business. It is remarkable how few of my veteran health care colleagues have any idea what Optum is or what it does. Optum was once a sort of dumping ground for assorted United acquisitions without a seeming core purpose. A private equity colleague once derided Optum as “The Island of Lost Toys”. Now, however, Optum is driving United’s growth, and generates billions of dollars in unregulated profits both from inside the highly regulated core health insurance business and from external customers.
Optum consists of three parts:Optum Health, its care delivery enterprise ($54 billion revenues in 2021), Optum Rx, its pharmacy benefits management enterprise ($91 billion revenues in 2021) and Optum Insight, a diversified business services enterprise ($12.2 billion in 2021). Virtually all of United’s acquisitions join one of these three businesses.
Optum Health: The Third Largest Care Delivery Enterprise in the US
By itself, Optum Health is almost the size of HCA ($54 billion in 2021 vs HCA’s $58.7 billion) and consists of a vast national portfolio of care delivery entities: large physician groups, urgent care centers, surgicenters, imaging centers, and now by dint of the recently announced $5.7 billion acquisition of LHC, home health agencies. Optum Health has studiously avoided acquiring beds of any kind: hospitals, nursing homes, etc. and likely will continue to do so. Optum Health’s physician groups not only generate profits on their own, but also provide powerful leverage for United to control health costs for its own subscribers, pushing down United’s highly visible and regulated Medical Loss Ratio (MLR), and increasing health plan profits.
Optum Health began in 2007 when United acquired Nevada-based Sierra Health, and thus became the new owner of a small multispecialty physician group which Sierra owned. The group did not belong in United’s health insurance business and came to rest over in Optum. Over the past twelve years, Optum Health has acquired an impressive percentage of the major capitated medical groups in the US- Texas’ WellMed, California’s HealthCare Partners (from DaVita), as well as Monarch, AppleCare and North American Medical Management, Massachusetts’ Reliant (formerly Fallon Clinic) and Atrius in Massachusetts (pending) , Kelsey Seybold Clinic (also pending) in Houston, TX and Everett Clinic and PolyClinic in Seattle.
Optum Health claims over 60 thousand physicians, though many of these are actually independent physicians participating in “wrap around” risk contracting networks. By comparison, Kaiser Permanente’s Medical Groups employ about 23 thousand physicians. United’s management claims that Optum Health provides continuing care to about 20 million patients, of whom 3 million are covered by some form of so-called “value based” contracts. Perhaps half of this smaller number are covered by capitated (percentage of premium-PMPM) contracts.
Optum Health straddles fierce competitive relationships between United’s health insurance business and competing health plans in well more than a dozen metropolitan areas. Almost half (44%) of Optum Health’s revenues come from providing care for health plans other than United.
When Optum acquires a large physician group, it acquires those groups’ contracts with United’s health insurance competitors, some of which contracts have been in place for decades. Premium revenues from other health plans, presumably capitation or per member per month (PMPM) revenues, are one-quarter of Optum Health’s $54 billion total revenues. These “external” premium revenues have quadrupled since 2018, largely for Medicare Advantage subscribers. Optum Health contributes about $4.5 billion in operating profit to United. It is impossible to determine from United’s disclosures how much of this profit comes from Optum Health’s services provided to United’s insured lives and how much from its medical groups’ extensive contracts with competing health plans.
Optum Health’s surgicenters and urgent care centers provide affordable alternatives to using expensive hospital outpatient services and emergency departments, potentially further reducing United medical expense. This creates obvious tensions with United’s hospital networks, since Optum Health can use its large medical practices and virtual care offerings to divert patients from hospitals to its own services, or else render those services unnecessary.
Though some observers have termed Optum/United’s business model “vertical integration”-ownership of the suppliers to and distributors of a firm’s product– Optum Health has actually grown less vertical since 2018, with revenues from competing health plans growing from 36% of total revenues in 2018 to 44% in 2021. A 2018 analysis by ReCon Strategy found at best a sketchy matchup between United’s health plan enrollment by market and its Optum Health assets (https://reconstrategy.com/2018/04/uniteds-medicare-advantage-footprint-and-optumcare-network-do-not-overlap-much-so-far/.
Optum Rx: The Nation’s Third Largest Pharmacy Benefits Management Business
Optum’s largest business in revenues is its Optum Rx pharmaceutical benefits management (PBM) business, which generates $91 billion in revenues, and processes over a billion pharmacy claims not only for United but also many competing insurers and employer groups. Pharmaceutical costs are a rapidly growing piece of total medical expenses, and controlling them is yet another source of largely unregulated profits for United; Optum Rx generated over $4.1 billion of operating profit in 2021.
Optum Rx is the nation’s third largest PBM business after Caremark, owned by CVS/Aetna and Express Scripts, owned by CIGNA, and processes about 21% of all scripts written in the US. Pharmacy benefits management firms developed more than two decades ago to speed the conversion of patients from expensive branded drugs to generics on behalf of insurers and self-funded employers. They were given a big boost by George Bush’s 2004 Medicare Part D Prescription Drug benefit, as a “pro-competitive” private sector alternative to Medicare directly negotiating prices with pharmaceutical firms.
Reducing drug spending is one key to United’s profitability. Since generics represent almost 90% of all prescriptions written, Optum Rx now relies on fees generated by processing prescriptions and on rebates from pharmaceutical firms to promote their costly branded drugs as preferred drugs on Optum Rx’s formularies. These rebates are determined based on “list” prices for those drugs vs. the contracted price for the PBMs, and are actual cash payments from manufacturers to PBMs.
Drug rebates represent a significant fraction of operating profits for health insurers that own PBMs, particularly for their older Medicare Advantage patients that use a lot of expensive drugs. Unfortunately, PBMs have incentives to inflate the list price, because rebates are caculated based on the spread between list prices and the contract pricel Unfortunately, this increases subscribers’ cash outlays, because patient cost shares are based on list prices.
Optum Rx generates about 39% of its revenues (and an undeterminable percentage of its profits) serving other health insurers and self-funded employers. Many of those self-funded employers demand that Optum pass through the rebates directly to them (even if it means being charged higher administrative fees!).
Unlike the situation with Optum Health, the “verticality” of Optum’s PBM business-the percentage of Optum revenues derived from serving United subscribers- has increased in the last seven years, to more than 60% of Optum Rx’s total business. What happens to the billions of dollars in rebates generated by Optum Rx is impossible to determine from United’s disclosures. However, our best guess is that pharmaceutical rebates represent as much as a quarter of United’s total corporate profits.
Optum Insight: “Intelligent” Business Solutions
The fastest growing and by far the most profitable Optum business is its business intelligence/business services/consulting subsidiary. Optum Insight was generated $12.2 billion in revenues in 2021, but a 27.9% operating margin, five times that of United’s health insurance business. Optum Insight is strategically vital to enhancing the profitability of United’s health insurance activities, but also generates outside revenues selling services to United’s health insurance competitors and hospital networks.
The core of Optum Insight is a business intelligence enterprise formerly known as Ingenix, which provided “big data” to United and other insurers about hospital and pricing behavior and utilization-crucial both for benefits design and administration. In 2009, Ingenix was accused by New York State of under reporting prices for out of network health services for itself and its clients, which had the effect of reducing its own medical reimbursements, and increasing patient cost shares. United signed a consent decree to alter Ingenix business practices and settled a raft of lawsuits filed on behalf of patients, physicians and employers. Its name was subsequently changed to Optum Insight.
By dint of aggressive acquisitions, Optum Insight has dramatically increased its medical claims management business, consulting services and business process outsourcing activities. . Most of United’s investment in artificial intelligence can be found inside Optum Insight. Big data plays a crucial role in United’s overall strategy. Optum Insight’s claims management software uses vast medical claims data bases and artificial intelligence/machine learning software to spot and deny medical claims for which documentation is inadequate or where services are either “inappropriate” or else not covered by an individual’s health plan. Providers also claim that the same software rejects as many as 20% of their claims, often for problems as tiny as a mis-spelled word or a missing data field.
Optum Insight software plays a crucial role in helping United’s health insurance plans manage their medical expense. Traditional health plan profitability is generated by reducing medical expense relative to collected premiums to increase underwriting profit. These profits are regulated, with highly variable degrees of rigor by state health insurance commissioners, and also by provisions of ObamaCare enacted in 2010.
Though its acquisition of Equian in 2019 and the proposed $13 billion acquisition of health information technology conglomerate Change Healthcare in 2021, United came within an eyelash of a near monopoly on “intelligent” medical claims processing software. The Justice Department challenged this latter acquisition and United may agree to divest Change’s claims processing software business as a condition of closing the deal. Even without the Change acquisition, Optum Insight processes hundreds of millions of medical claims annually not only for United’s health insurance business but for many of United’s competitors.
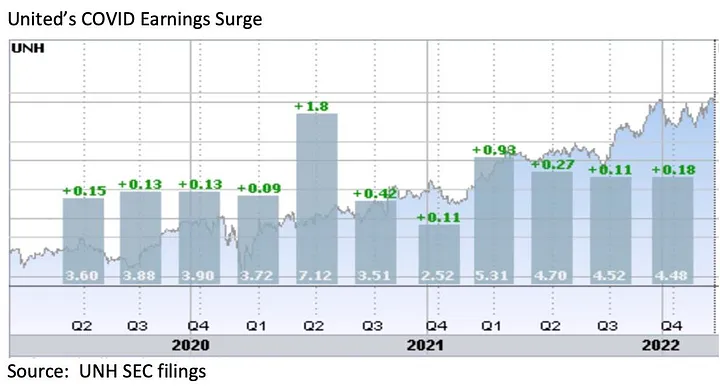
However, Optum Insight’s claims management system can also be used to increase MLR if medical expense unexpectedly declines, exposing the firm to federal requirement that it rebate excessive ‘savings’ to subscribers. This happened in 2020, when the COVID pandemic dramatically and unexpectedly added billions to United’s earnings due to hospitals suspending elective care. The chart below shows United’s 2Q2020 earnings per share almost doubling due to the precipitous drop in its medical claims expenses!
Hospital finance colleagues reported an immediate and substantial drop in medical claims denials from United and other carriers in the summer and fall of 2020. United’s quarterly profits dutifully and steeply declined in the subsequent two quarters, because its medical expenses sharply rebounded. The rise in
United’s medical expenses helped the firm avoid premium rebates to patients required by provisions of the ObamaCare legislation passed in 2010. The firm did voluntarily rebate about $1.5 billion to many of its customers in June, 2020.
However the most rapidly growing part of Optum Insight is its Optum 360 business process outsourcing business, which helps hospitals manage their billing and collections revenue cycle, as well as information technology operations, supply chain (purchasing and materials management) and other services. Through Optum 360, Optum Insight has signed five long term master contracts in the past two years’ worth many billions of dollars with care providers in California, Missouri and other states to provide a broad range of business services.
With all these different businesses, it is theoretically possible for one piece of Optum to be reducing a hospital’s cash flow by denying medical claims for United subscribers, while United’s health insurance network managers bargain aggressively to reduce the hospital’s reimbursement rates while yet another piece of Optum runs the billing and collection services for the same hospital and its employed physicians, while yet another piece of Optum competes with the hospital’s physicians and ambulatory services, diverting patients from its ERs and clinics, reducing the hospital’s revenues.
It is not difficult to imagine a future in which Optum/United offers hospital systems an Optum 360 outsourcing contract that run most of the business operations of a hospital system in exchange for preferred United health plan rates, an AI-enabled EZ pass on its medical claims denials and inpatient referrals from Optum physician groups and urgent care centers, at the expense of competing hospitals.
Managing these potential conflicts will be an increasing challenge as these various businesses grow, placing intense pressure on United’s leadership to get the various pieces of United to work together. To many anxious hospital executives, United resembles nothing so much as the Kraken, rising up out of the sea, surrounding and engulfing them- a powerful friend perhaps or a fearsome foe. As you might expect, United’s growing market power and growth has generated a fierce backlash in the hospital management community.
What Business is United Healthcare In?
United Healthcare is the most successful business in the history of American healthcare. The rapid growth of Optum and continued health insurance enrollment growth from government programs like Medicaid and Medicare has created a cash engine which generates nearly $2 billion a month in free cash flow. Optum’s portfolio has given United an impressive array of tools, unequalled in the industry, to improve its profitability and to reach into every corner of the US health system. United Healthcare is managed care on steroids.
United’s diversified portfolio of businesses gives the firm what a finance-savvy colleague termed “optionality”- the ability to redirect capital and management attention to areas of growth and away from areas that have ceased to grow, in the US or overseas. With its substantial investable capital, it will have the pick of the litter of the 11 thousand digital health companies as the overextended digital health market consolidates. United will be able to use its vast resources to build state-of-the-art digital infrastructure to reach and retain patients and manage their care.
United’s main short term business risks seem to be running out of accretive transactions effectively to deploy its growing horde of capital and managing the firm’s rising political exposure. United has had tremendous business discipline and has shied away from speculative acquisitions that are not immediately accretive to earnings. If its earnings growth falters, however, it will also encounter pressure from the investment community to increase dividends (presently about 1.2%) or share buybacks to bolster its share price, or else divest some or all of Optum in order to “maximize shareholder value”.
Answering the question, “What Business is United In” is simple: just about everything in health but hospitals and nursing homes.
Answering the questions- who are its customers and what do they want? — is a great deal harder. The customers United serves are in a sort of cold war with one another. United’s original business was protecting employers from health cost growth , and tempering the influence of hospitals and doctors by reducing their rates and utilization. By fostering so-called Consumer Directed Health Plans that expose many of their subscribers to very high front-end copayments, United and its health insurance brethren, have also increased their out-of-pocket costs, whether they have the savings to pay them or not.
There are also some ironies in United’s development. Optum Insight’s suite of hospital business services are designed to reduce administrative costs created in major part by United and other insurers’ medical claims data requirements. Its PBM business, originally intended to reduce drug spending by bargaining aggressively with pharmaceutical manufacturers has ended up pushing up drug list prices and consumer cost shares.
While presumably everybody benefits if United can somehow help patients become and remain healthy, it is still far from obvious how to do this. Managing all these markedly divergent customer needs will be a tremendous management challenge for whoever succeeds United’s reclusive (and very effective) 70 year old Chairman Stephen Hemsley.
What Does Society Get from this Vast Enterprise?
However, as Peter Drucker told a different generation of business giants, businesses are not entities unto themselves, accountable only to shareholders and customers. They are organs of society, and are expected to create social value. Americans are suspicious of vast enterprises, as businesses from Standard Oil, US Steel and ATT to Microsoft and Facebook have learned. As businesses grow and become more successful, public suspicion grows.
Private health insurers already face strident opposition from progressive Democrats, who believe that health coverage ought to be a public good, a right of citizenship provided publicly; in other words, that private health insurers have no business being in business. And large insurers like United also face intense opposition from hospitals and many physicians because they reduce their incomes and impose major administrative burdens upon them.
In the age of Twitter and TikTok, United is highly vulnerable to “event risks” that confirm the hostile narratives of the firm’s detractors that United is mainly about maximizing its own profits, not about improving the health of its subscribers or the communities it serves. It is not clear how many the tens of millions of United subscribers have warm and fuzzy feelings about their giant health insurer. Memories of the HMO backlash of the 1990’s reside in the firm’s corporate memory.
United has grown to its present immense scale largely without public knowledge. United has within its reach the capability of constraining overall health cost growth across dozens of metropolitan areas and regions, not merely cost growth for its own beneficiaries (roughly one in seven US citizens already get their health insurance through United). With its expanding digital health operations, it can deploy state of the art tools for helping United’s 50 million subscribers avoid illness and live healthier lives.
United also has the ability to damage the financial operations of beloved local hospitals and deny coverage to families, raising their out of pocket expenses. How United frames and defends its social mission and how it manages all the delicate and increasingly fraught customer relationships will determine its future, and in important ways, ours as well.
Kaiser Permanente on Wednesday announced it is acquiring Geisinger Health, and Geisinger will operate independently under a new subsidiary of Kaiser called Risant Health.
Deal details
The combination of the two companies will need to be reviewed by federal and state agencies, but if approved, the two companies will have more than $100 billion in combined annual revenue.
Geisinger will operate independently as part of Risant Health, which will be headquartered in Washington, D.C. and will be led by Geisinger president and CEO Jaewon Ryu. The health systems said they intend to acquire four or five more hospital systems to fold into Risant in an effort to reach $30 billion to $35 billion in total revenue over the next five years.
In an interview, Ryu and Kaiser chair and CEO Greg Adams said Risant will specifically target hospital systems already working to move into value-based care.
According to Adams, Risant Health “is a way to really ensure that not-for-profit, value-based community health is not only alive but is thriving in this country.”
“If we can take much of what is in our value-based care platform and extend that to these leading community health systems, then we extend our mission,” Adams said. “We reach more people, we drive greater affordability for health care in this country.”
Why we’re ‘cautiously optimistic’ about this acquisition
Just when you thought healthcare couldn’t get more interesting, Kaiser and Geisinger announce their union through newly established Risant Health. At first pass, it is hard to see a downside with this deal — and that’s something that raises my “spidey-senses.”
Kaiser and Geisinger are coming together through a vehicle that could allow them to clear an increasingly skeptical Federal Trade Commission. It affords two health systems — both in comparatively weaker financial positions than before the pandemic — the ability to get bigger through the merger. Its pitch is decidedly hospital- (and in the future provider) led, with Geisinger retaining its brand and elevating its CEO to the head of Risant. It also gives Geisinger and future partners the latitude to pursue their own payer relationships.
In addition, it is ostensibly a play to increase providers’ control over the nature and pace of value-based care (VBC) adoption. In its press release, Kaiser acknowledges that its closed network model of care management hasn’t scaled well to other markets. And Geisinger, with its own health plan and a track-record of developing its own VBC incentives, is no neophyte and brings a clear wealth of expertise.
Without a doubt, the offer to future partners is compelling: “Come for the size and stay for the value-based care.” But like all things in life, it’s all in the details. And that’s where my “spidey-sense” kicks in.
Partnership and affiliation models alone do not make the hard work of VBC easier. While this emerging group could become a valuable, provider-led clearing house for VBC concepts, applying them in communities remains a stubborn challenge that requires individual work and leadership.
The true test of the concept will come when the first new partner joins. How they decide to participate and whether the model has the right mix of scale and flexibility is what I’ll be watching closely. The overall objective and success measure of this endeavor remains somewhat opaque, but I would say that the concept has real legs here. Right now, I’m leaning toward “cautiously optimistic.”
Published in the April edition of Health Affairs Forefront, this piece unpacks why payers and other corporations have replaced health systems as the top bidders for primary care practices, driving up practice purchase prices from hundreds of dollars to tens of thousands of dollars per patient. While corporate players like UnitedHealth Group, Amazon, and Walgreens have spent an estimated $50B on primary care, it pales in comparison to the potential “$1T opportunity” in value-based care projected by McKinsey and Company.
The authors argue that this tantalizing opportunity exists because the Centers for Medicare and Medicaid Services (CMS) invited corporations to “re-insure” Medicare through capitated arrangements in Medicare Advantage (MA) and its Direct Contracting program.
While CMS intended to promote risk and value-based incentives to improve care quality and costs, the incentive structures baked into these programs have afforded payers record profits, despite neither improving patient outcomes nor reducing government healthcare spending.
The Gist: While the critiques of MA reimbursement structures in this piece are familiar, they are woven together into a convincing rebuke of the “unintended consequences” of CMS’s value-based care policy.
Through poorly designing incentives, CMS paved a runway for corporate America to capture the lion’s share of the financial returns of value-based care, paying prices for primary care that health systems can’t match.
Meanwhile, despite skyrocketing valuations for primary care practices, primary care services remain underfunded and inadequately reimbursed, pushing primary care groups closer to payers with excess profits to invest.
During one of our regular check-ins with a health system CEO this week, the conversation took a turn for the existential. Lamenting the difficult economic situation in the industry, the continued shift of care to ambulatory disruptors, and the mounting pressure to dial back money-losing services, he shared that he was starting to question the fundamental business model.
“Many years ago, we set out to become an integrated delivery system. But I’m not sure we’ve succeeded at any of those things: we’re not integrated enough, we don’t act like a system, and we don’t seem to be delivering the kind of care consumers want.” A stark admission, but one that could apply to many large health systems across the industry.
In theory, those three “legs of the stool” should create a virtuous flywheel: greater integration across the care continuum (perhaps in a risk-bearing model, but not necessarily) ought to allow systems to deliver quality care at the right place, right time. And a system-oriented approach ought to allow for efficiencies and cost-savings that enable care to be delivered at lower cost to patients.
Instead, the three components often create a vicious spiral: care that’s not coordinated across an integrated continuum, with little success at leveraging system-level efficiencies, resulting in unnecessary, duplicative, and variable-quality care delivery at excessive cost.
Capturing the value of integrated delivery systems will ultimately require hard work, and not just lip service, on all three pieces. Meanwhile, scaling a broken model will only exacerbate the problems of organizations that are neither integrated, nor systemic, nor delivering care that is high value.
Running a health system recently has proven to be a very hard job. Mounting losses in the face of higher operating expenses, softer than expected volumes, deferred capex, and strained C-suite succession planning are just a few of the immediate issues with which CEOs and boards must deal.
But frankly, none of those are the biggest strategic issue facing health systems. The biggest strategic issue is the reorganization of the American healthcare landscape into an ambulatory care business that emphasizes competing for covered lives at scale in lower cost and convenient settings of care. This shift in business model has significant ramifications, if you own and operate acute care hospitals.
Village MD and Optum are two of the organizations driving the business model shift. They are owned by large publicly traded companies (Walgreens and UnitedHealth Group, respectively). Both Optum and Village MD have had a string of announced major patient care acquisitions over the past few years, none of which is in the acute care space.
The future of American healthcare will likely be dominated by large well-organized and well-run multi-specialty physician groups with a very strong primary care component. These physician service companies will be payer agnostic and focused on value-based care, though will still be prepared to operate in markets where fee-for-service dominates. They will deliver highly coordinated care in lower cost settings than hospital outpatient departments. And these companies will be armed with tools and analytics that permit them to manage the care for populations of patients, in order to deliver both better health outcomes and lower costs.
At the same time this is happening, we are experiencing steady growth in Medicare Advantage. And along with it, a stream of primary care groups who operate purpose-built clinics to take full risk on Medicare Advantage populations. These companies include ChenMed, Cano Health and Oak Street, among others. These organizations use strong culture, training, and analytics to better manage care, significantly reduce utilization, and produce better health outcomes and lower costs.
Public and private equity capital are pouring into the non-acute care sectors, fueling this growth. As of the start of 2022, nearly three quarters of all physicians in the US were employed by either corporate entities (such as private equity, insurance companies, and pharmacy companies), or employed by health systems. And this employment trend has accelerated since the start of the pandemic. The corporate entities, rather than health systems, are driving this increasing trend. Corporate purchases of physician practices increased by 86% from 2019 to 2021.
What can health systems do? To succeed in the future, you must be the nexus of care for the covered lives in your community. But that does not mean the health system must own all the healthcare assets or employ all of the physicians. The health system can be the platform to convene these assets and services in the community. In some respects, it is similar to an Apple iPhone. They are the platform that convenes the apps. Some of those apps are developed and owned by Apple. But many more apps are developed by people outside of Apple, and the iPhone is simply the platform to provide access.
Creating this platform requires a change in mindset. And it requires capital. There are many opportunities for health systems to partner with outside capital providers, such as private equity, to position for the future – from both a capital and a mindset point of view.
The change in mindset, and the access to flexible capital, is necessary as the future becomes more and more about reorganizing into an ambulatory care business that emphasizes competing for covered lives at scale in lower cost and convenient settings of care.
The demise of Haven — a coalition of three big employers aiming to lower the cost of healthcare for their workers — was met with a surprising reaction from Jamie Dimon, CEO of JPMorgan Chase: “We want to do this again.”
A Dec. 6 report from Bloomberg details some of the aftermath of Haven’s end and also the origins of Morgan Health, the bank’s second go at lowering healthcare costs that was rolled out in spring 2021. While still in its early stages, one tenet of its strategy is a return to basics, including appointments between clinicians and patients that take at least 30 minutes if not an hour.
Haven was the healthcare partnership formed in 2018 by Amazon, JPMorgan Chase and Berkshire Hathaway with an aim to lower healthcare costs for their 1.2 million workers. It disbanded in 2021. As its end neared, Mr. Dimon set out to learn what had gone wrong.
When he asked the question of Bill Wulf, MD, CEO of Central Ohio Primary Care, the internist told the businessman the initiative had moved too slowly. A virtual care program drew in only 150 people in Ohio, for example, before it was scrapped.
Shortly after the debrief with Dr. Wulf, Mr. Dimon assigned a lieutenant to restart the work on lowering employer healthcare costs, this time focusing on JPMorgan Chase alone. That leader was Peter Scher, vice chairman with the bank, who had his doubts at first. “There are a lot of things we could be spending our time on,” he told Bloomberg. “I was perfectly prepared to go back to Jamie and the operating committee and say, ‘Listen, it was a good try.'”
Mr. Scher stuck with it and brought on Dan Mendelson, founder and former CEO of healthcare advisory group Avalere Health, to lay the groundwork for JPMorgan’s second healthcare attempt. Mr. Mendelson, who had been a skeptic of Haven, spent three months crafting a strategy and playbook that recognized where Haven had fallen short and avoided repeated mistakes. He signed on to lead the group, dubbed Morgan Health.
The group has made more headlines since its launch than its predecessor Haven, which premiered with much bravado but went nearly a year without releasing any news except for its name and a new website. In fall 2022, Morgan Health openedthree advanced primary care centers in Ohio for a total of five and formed a healthcare venture capital team targeting early- to later-stage healthcare companies with innovations in areas like genetic medicine, autoimmune diseases, cardiometabolic diseases and rare disorders. It also hired Cheryl Pegus, MD, Walmart’s executive vice president of health and wellness, as a managing director.
Morgan Health’s strategy is marked by what appears to be common sense and a return to basics, including the placement of clinics in office building atriums — “a full-service practice where employees can develop long-term relationships with primary-care providers, wellness coaches, mental health providers and care coordinators.”
All appointments are booked for at least 30 minutes with many going an hour, according to Bloomberg. Patients generally see the same practitioner for each visit to build long-term relationships. Clinicians’ payments are tied to goals like avoiding emergency room visits, providing cancer screenings and keeping high blood pressure in check. If it plays out as designed, JPMorgan says the investment in prevention and primary care will curb high-cost services and hospital stays, ultimately leading to meaningful savings.
The goal is to “identify high-risk patients and then bubble-wrap them,” Dr. Wulf told Ohio business leaders in an October meeting, Bloomberg reports. “How do we keep you out of the hospital?”
JPMorgan has opened five clinics in the area of Columbus, Ohio, which will also be open to other employers who want to sign on. The clinics and primary care centers are managed and staffed by Vera Whole Health and Central Ohio Primary Care. JPMorgan is seeking “like-minded” medical groups in markets like New York, Chicago and Dallas where it has hubs of workers, Bloomberg reports.
Driven in large part by the growth of Medicare Advantage, a number of startups are vying to create the next value-based care model for senior care in patients’ homes, Axios’ Sarah Pringle reports.
Why it matters: As we recently reported in our Elder Care Crisis Deep Dive, there is a shortfall of enough cash and caregivers to handle the massive amount of aging baby boomers reaching their senior years.
“The cool thing about value-based care?” General Atlantic managing director Robb Vorhoff said. “There’s hundreds of business models.”
Reality check: Scaling remains a challenge for new models looking to shake up the senior care market.
“There are a lot of options out there that you don’t know about,” Town Hall Venture’s Andy Slavitt says. “Some are the best-kept secrets; some are not worth knowing about.”
Be smart: While most elderly adults would prefer to age in place, there is still a need for institutional care settings like nursing homes, which presents its own major challenges, Sarah writes.
According to reporting from Bloomberg, primary care company VillageMD, which is majority-owned by Walgreens, is engaged in talks to merge with New Jersey-based Summit Health, a large medical group network and urgent care chain backed by private equity firm Warburg Pincus.
In 2019, Summit merged with CityMD, a New York City-based urgent care chain, and operates over 370 clinic locations based in and around New York City, as well as in central Oregon. The combined entity would be valued between $5B and $10B.
The Gist: Should this deal go through, it would epitomize recent trends in healthcare M&A:a well-established independent medical group using private equity funding to rapidly expand its operations before selling off to an industry giant.
If that industry giant ends up being VillageMD, Walgreens would finally have a physician practice with deep experience in managing risk, on which they can anchor their larger ambitions in care provision. And if the deal with Walgreens falls through, Summit, with its combination of mostly suburban value-based care practices and largely urban urgent care chains, is sure to attract plenty of other suitors, including any of the major national insurers.
The Biden administration is trying to jump start a Medicare program that pays health providers based on patient outcomes rather than by how many services they perform.
Why it matters: The alternative payment effort was created through the Affordable Care Act, but participation has plateaued since 2018 amid waning interest from providers.
Driving the news: The Biden administration finalized an overhaul of the initiative, known as the Medicare Shared Savings Program, on Tuesday. Changes include offering groups of providers in rural and other underserved areas upfront payments to help them start out in the program.
The rule includes other provisions to make it less financial risky for provider groups to join, and makes it easier for participants to earn money back from the government year after year — a central perk of joining the program.
Zoom out: Medicare traditionally pays on a “fee-for-service” basis pegged to the number of patients seen and volume of procedures performed.
But one of the main funding sources for Medicare is set to run dry in 2028 if the federal government doesn’t make changes. Advocates say the solution at least partially lies in value-based care programs, like the Shared Savings Program.
Under the program, doctors, hospitals and other providers join form groups known as accountable care organizations. ACOs take responsibility for the care of a set of traditional Medicare patients.
If ACOs reduce total care costs for their members, they can get back a portion of that savings from the government. ACOs at more advanced stages of the program must pay the government back if total patient spending crosses a threshold.
By the numbers: ACOs have saved the federal government more than $17 billion since 2012, according to the National Association of Accountable Care Organizations.
In 2022, 483 ACOs participated in the program and took care of more than 11 million Medicare enrollees. But that’s down from 517 ACOs participating in 2020.
CMS set a goal last year to bring all 63 million-plus Medicare beneficiaries into a value-based care model by 2030. ACOs are a key player in achieving the goal.
Go deeper: Providers and value-based care advocates are also pushing Congress to extend a 5% pay bump for providers that participate in advanced alternative payment models, including some tracks of the Medicare Shared Savings Program. The bonus expires Dec. 31.
“If the bonus is not continued, it will soften or dampen the momentum toward alternative payment models, because it would create this mentality, or the view, that we’re not serious about that transformation,” said Mara McDermott, vice president at McDermott+Consulting and executive director of the Value Based Care Coalition.
Losing the bonus would also make it harder to recruit new providers into alternative payment models, she added.
The American Medical Association and five other health care groups launched a separate coalition Tuesday to rally around an extension of the 5% bonus.
“Patients and the healthcare system in the United States quite literally cannot afford to return to the days before Medicare incentivized healthcare providers for generating good results,” Clif Gaus, CEO of the National Association of ACOs, said in a news release about the coalition.
Also notable: The rule finalized Tuesday outlines physician payment rates for 2023. Interventional radiologists and vascular surgeons will see the largest Medicare cuts among physician specialties next year, though the final cuts are slightly lower than what CMS proposed in July.
Congress could stave off the cuts when they come back to Washington later this month.
“The Medicare payment schedule released today puts Congress on notice that a nearly 4.5 percent across-the-board reduction in payment rates is an ominous reality unless lawmakers act before Jan. 1,” American Medical Association President Jack Resneck said in a statement.
CMS finalized a slew of other policy proposals Tuesday, including provisions to reduce barriers to behavioral health care.