On Tuesday, Novo Nordisk released the headline results of a large clinical trial demonstrating that its popular GLP-1 inhibitor Wegovy reduced the risk of heart attacks, strokes, and cardiovascular deaths by 20 percent. The SELECT trial enrolled roughly 17,600 non-diabetic adults aged 45 and older who were overweight or obese with established cardiovascular disease. It compared people in this population treated with the drug to those given a placebo, and tracked them for up to five years. The drugmaker said it plans to release the full trial results at a conference later this year. These results are similar to a previous study that found Wegovy sister drug Ozempic, also made by Novo Nordisk, reduced the risk of adverse cardiac events by 26 percent in adults with type 2 diabetes.
The Gist: The cardioprotective effects demonstrated in this study far exceeded researchers’ expectations. Though concerns still abound about the high costs of Wegovy (nearly $1,350 per month) and similar drugs, these results will certainly put pressure on Medicare and other insurers to provide coverage.
Questions remain around how the drug actually improves cardiovascular outcomes, and whether patients with cardiac disease who are not overweight or obese might also benefit from taking it.
Despite the fact that the data are still preliminary, the argument that obesity medications are solely “lifestyle” or “vanity drugs”—which some insurers and employers have been using to deny coverage—will now be much harder to defend.
Generative AI applications can already help health systems improve margins, yet only 6% have a strategy ready.
At a Glance
In the wake of their most challenging financial year since 2020, US hospitals are desperately searching for margin improvements.
Generative AI can increase productivity and cost efficiency, but only 6% of health systems currently have a strategy.
Leading providers and payers will start with highly focused, low-risk generative AI use cases, generating the funds and experience for more transformative future applications.
While Covid-19 may no longer be dominating the global news cycle, healthcare providers and payers are still feeling its reverberations. More than half of US hospitals ended 2022 with a negative margin, marking the most difficult financial year since the start of the pandemic.
CEOs and CFOs remember the challenges all too well: The Omicron surge halted nonurgent procedures in the first half of the year, government support tapered off, and labor expenses ballooned amid staffing shortages. There was also the record-high inflation that continues to intensify margin pressures today. According to a recent Bain survey of health system executives, 60% cite rising costs as their greatest concern.
Payers and providers are now on the hunt for margin improvements. In our experience, the most successful companies won’t merely reduce costs, but also ramp up productivity. When done right, modest technology investments can accomplish both.
Artificial intelligence (AI) may hold part of the answer. With the costs to train a system down 1,000-fold since 2017, AI provides an arsenal of new productivity-enhancing tools at a low investment.
Many executives recognize the growing opportunity, especially with the recent rise of generative AI, which uses sophisticated large language models (LLMs) to create original text, images, and other content. It’s inspiring an explosion of ideas around use cases, from reviewing medical records for accuracy to making diagnoses and treatment recommendations.
Our survey reveals that 75% of health system executives believe generative AI has reached a turning point in its ability to reshape the industry. However, only 6% have an established generative AI strategy.
It’s time to play offense—or be forced to play defense later. But choosing from the laundry list of generative AI applications is daunting. Companies are at high risk of overinvesting in the wrong opportunities and underinvesting in the right ones, undermining future profitability, growth, and value creation. A wait-and-see approach is a tempting prospect.
However, we believe the next generation of leading healthcare companies will start today, with highly focused, low-risk use cases that boost productivity and cost efficiency. Over the next three to nine months, these companies will improve margins and learn how to implement a generative AI strategy, building up the funds and experience needed to invest in a more transformative vision.
Endless potential—and high hurdles
The excitement around generative AI may feel akin to the hype around other recent digital and technology developments that never quite rose to their promised potential. Well-intentioned, well-informed individuals are debating how much change will truly materialize in the next few years. While developments over the past six months have been a testament to the breakneck speed of change, nobody can accurately predict what the next six months, year, or decade will look like. Will new players emerge? Will we rely on different LLMs for different use cases, or will one dominate the landscape?
Despite the uncertainty, generative AI already has the power to alleviate some of providers’ biggest woes, which include rising costs and high inflation, clinician shortages, and physician burnout. Quick relief is critical, considering that the heightened risk of a recession will only compound margin pressures, and the US could be short 40,800 to 104,900 physicians by 2030, according to the Association of American Medical Colleges.
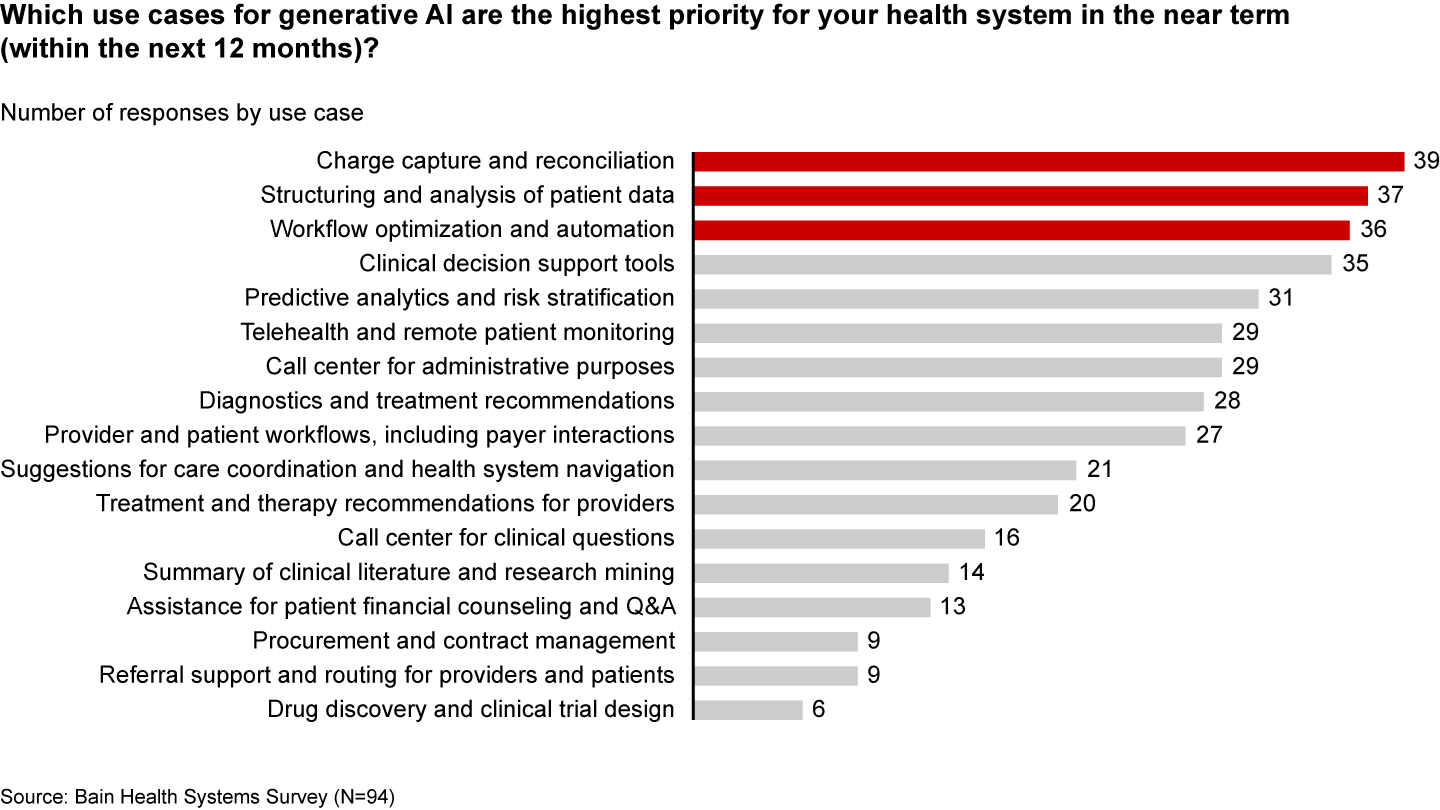
Many health systems are eyeing imminent opportunities to reduce administrative burdens and enhance operational efficiency. They rank improving clinical documentation, structuring and analyzing patient data, and optimizing workflows as their top three priorities (see Figure 1).
Figure 1
In the near term, generative AI can reduce administrative burdens and enhance efficiency
Some generative AI applications are already streamlining administrative tasks and allowing thinly stretched physicians to spend more time with patients. For instance, Doximity is rolling out a ChatGPT tool that can draft preauthorization and appeal letters. HCA Healthcare partnered with Parlance, a conversational AI-based switchboard, to improve its call center experience while reducing operators’ workload. And there are new announcements seemingly every week: Consider how healthcare software company Epic Systems is incorporating ChatGPT with electronic health records (EHRs) to draft response messages to patients, or how Google Cloud is launching an AI-enabled Claims Acceleration Suite for prior authorization processing.
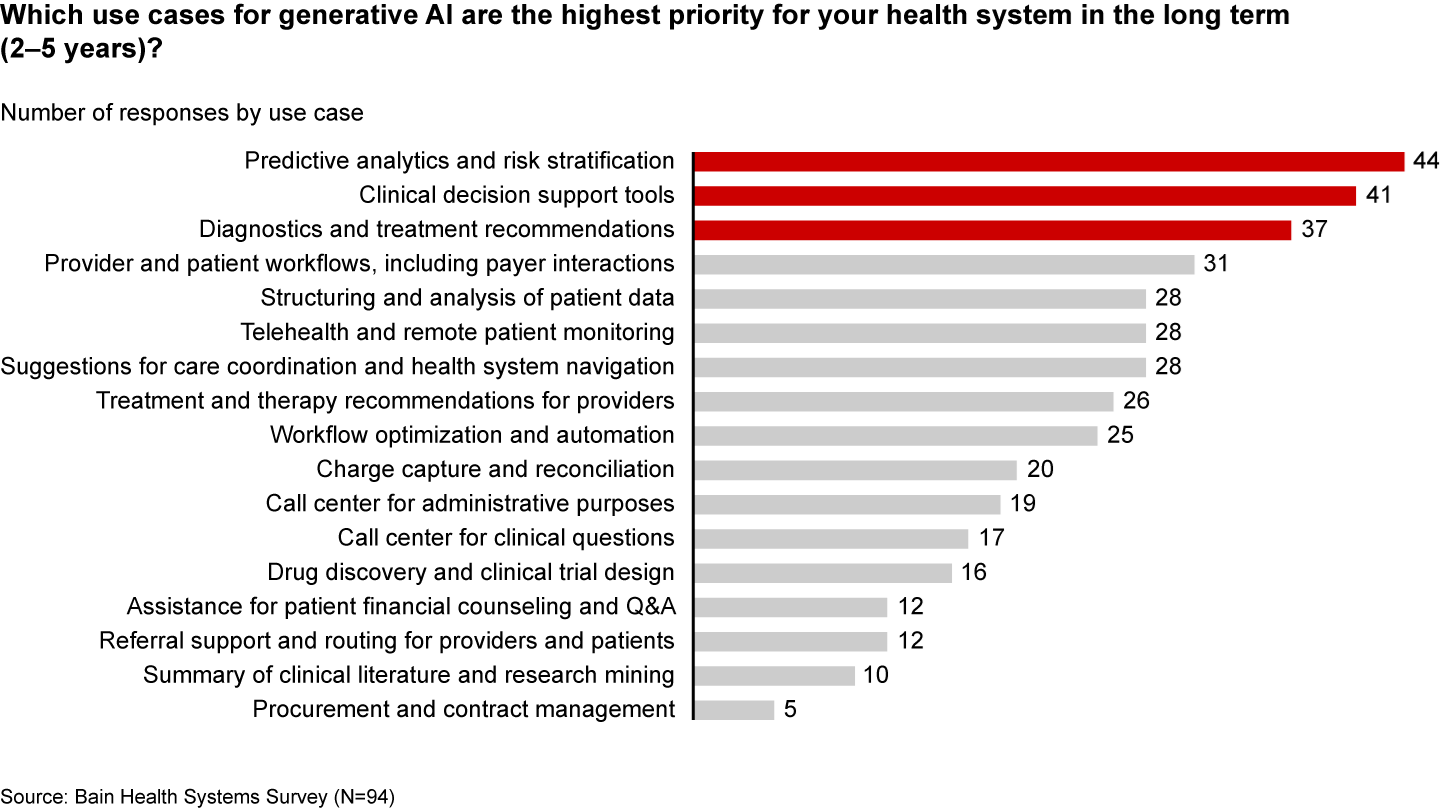
These applications only scratch the surface of potential. In the future, generative AI could profoundly transform care delivery and patient outcomes. Looking ahead two to five years, executives are most interested in predictive analytics, clinical decision support, and treatment recommendations (see Figure 2).
Figure 2
Predictive analytics, clinical decisions, and care recommendations are long-term generative AI priorities
It’s hard not to catch AI “fever.” But there are real challenges ahead. Some are already tackling the biggest questions: Organizations such as Duke Health, Stanford Medicine, Google, and Microsoft have formed the Coalition for Health AI to create guidelines for responsible AI systems. Even so, solutions to the greatest hurdles aren’t yet keeping up with the rapid technology development.
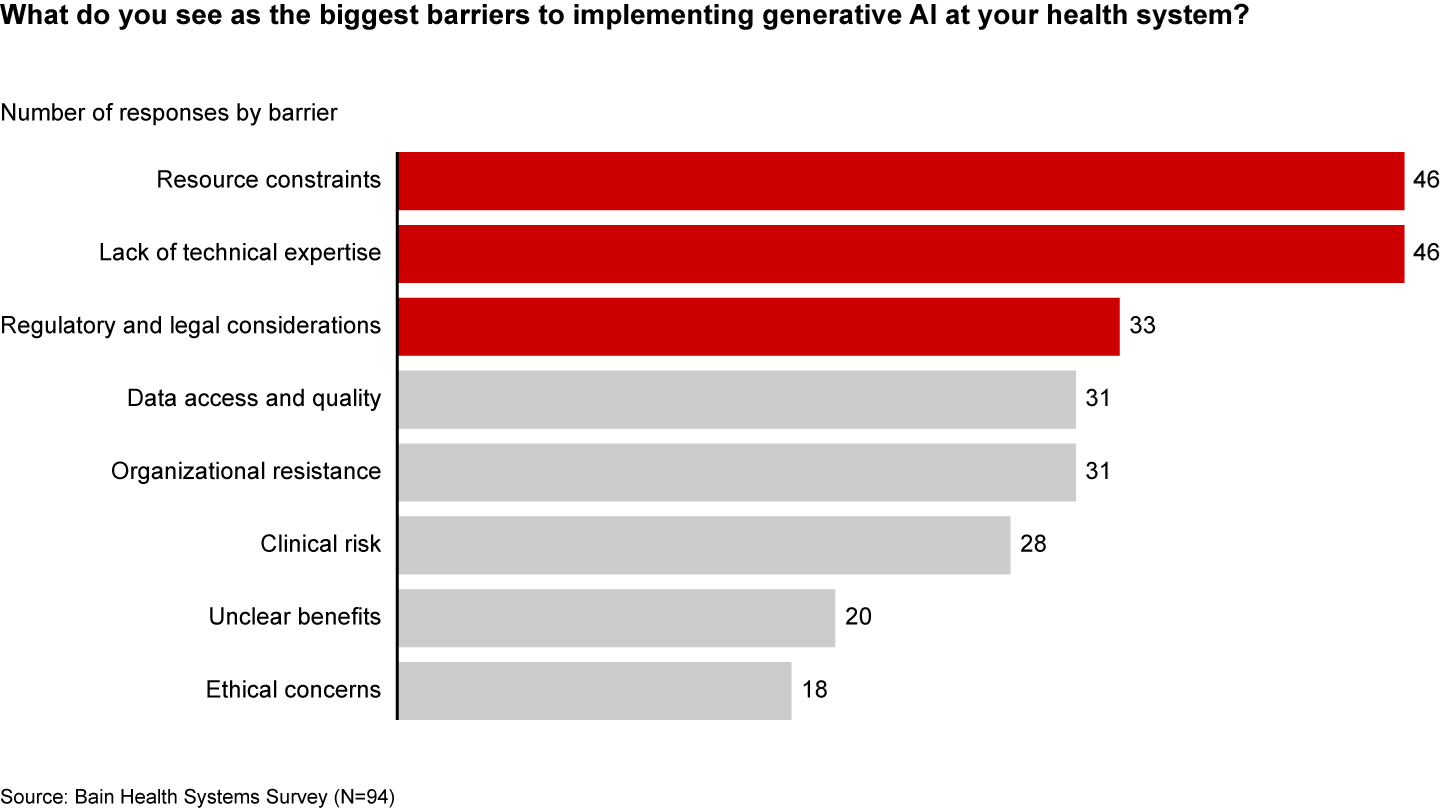
Resource and cost constraints, a lack of expertise, and regulatory and legal considerations are the largest barriers to implementing generative AI, according to executives (see Figure 3).
Figure 3
A lack of resources, expertise, and regulation are the biggest barriers to generative AI in healthcare
Even when organizations can overcome these hurdles, one major challenge remains: focus and prioritization. In many boardrooms, executives are debating overwhelming lists of potential generative AI investments, only to deem them incomplete or outdated given the dizzying pace of innovation. These protracted debates are a waste of precious organizational energy—and time.
Starting small to win big
Setting the bar too high is setting up for failure. It’s easy to get caught up, betting big on what seems like the greatest opportunity in the moment. But 12 months later, leaders often find themselves frustrated that they haven’t seen results or feeling as if they’ve made a misplaced bet. Momentum and investments slow, further hindering progress.
Leading companies are forming a more pragmatic strategy that considers current capabilities, regulations, and barriers to adoption. Their CEOs and CFOs work together to enforce four guiding principles:
Pilot low-risk applications with a narrow focus first. Tomorrow’s leaders are making no-regret moves to deliver savings and productivity enhancements in short order—at a time when they need it most. Gaining experience with currently available technology, they are testing and learning their way to minimum viable products in low-risk, repeatable use cases. These quick wins are typically in areas where they already have the right data, can create tight guardrails, and see a strong potential return on investment. Some, like call center and chatbot support, can improve the patient experience. However, given the current challenges around regulation and compliance, the most successful early initiatives are likely to be internally focused, such as billing or scheduling. Most importantly, executives prioritize initiatives by potential savings, value, and cost.
Decide to buy, partner, or build. CEOs will need to think about how to invest in different use cases based on availability of third-party technology and importance of the initiative.
Funnel cost savings and experience into bigger bets. As the technology matures and the value becomes clear, companies that generate savings, accumulate experience, and build organizational buy-in today will be best positioned for the next wave of more sophisticated, transformative use cases. These include higher-risk clinical activities with a greater need for accuracy due to ethical and regulatory considerations, such as clinical decision support, as well as administrative activities that require third-party integration, such as prior authorization.
Remember generative AI isn’t a strategy unto itself. To build a true competitive advantage, top CEOs and CFOs are selective and discerning, ensuring that every generative AI initiative reinforces and enables their overarching goals.
Some health systems are already seeing powerful results from relatively small, more practical investments. For instance, recognizing that clinicians were spending an extra 130 minutes per day outside of working hours on administrative tasks, the University of Kansas Health System partnered with Abridge, a generative AI platform, to reduce documentation burden. By summarizing the most important points from provider-patient conversations, Abridge is improving the quality and consistency of documentation, getting more patients in the door, and cutting down on pervasive physician burnout.
Although it will require some upfront investment, in the long run it will be more costly to underestimate the level and speed at which generative AI will transform healthcare. The next generation of leaders will start testing, learning, and saving today, putting them on a path to eventually revolutionize their businesses.
A number of healthcare organizations have recently closed medical departments or ended services at facilities to shore up finances, focus on more in-demand services or address staffing shortages.
Here are 45 closures or services ending, announced, advanced or finalized that Becker’s has reported since Feb. 2:
1. Vicksburg, Miss.-based Merit Health River Regionclosed its behavioral health unit on June 30.
2. Wilkes-Barre (Pa.) General Hospital moved up the date it planned to end childbirth services by about three weeks, with the care ending abruptly July 11.
3. Good Samaritan Hospital, operated by Nashville, Tenn.-based HCA Healthcare, plans to close the inpatient psychiatric facility at its Mission Oaks Hospital in Los Gatos, Calif., on Aug. 20.
4. Philadelphia-based Penn Medicine shut down one of its urgent care centers, Penn Urgent Care South Philadelphia, on June 30, as more patients are turning to telehealth for care.
5. Hartford City, Ind.-based IU Health Blackford Hospital announced it will close its emergency department and no longer offer inpatient services due to a reduction in patient volume.
6. The Illinois Health Facilities and Services Review Board on June 27 unanimously approved a request from HSHS St. Mary’s Hospital to shutter four of its units. The Decatur, Ill.-based hospital will wrap up its advanced inpatient rehabilitation, obstetrics and newborn nursery, pediatrics and inpatient behavioral health services.
7. Albany, N.Y.-based St. Peter’s Health Partners submitted a plan to the state Department of Health to shut down the maternity unit at Samaritan Hospital. If approved, the Troy, N.Y., hospital will close the unit in about four to six months.
8. Jackson, Miss.-based St. Dominic Health Services is ending its behavioral health services unit, citing financial difficulties. The unit stopped taking admissions after June 6.
9. Fort Wayne, Ind.-based Lutheran Hospital is closing its heart transplant and inpatient burn units due to low patient volumes. The inpatient burn unit stopped accepting new patients June 2.
10. Worcester, Mass.-based UMass Memorial Health plans to close the maternity ward at its HealthAlliance-Clinton Hospital Sept. 22 due to staff shortages and a declining number of births in the area.
11. Vancouver, Wash.-based PeaceHealth closed its pediatric cardiology clinic, sleep clinic, optometry clinic and optical shop July 21. It also ended its comprehensive outpatient palliative care May 26 and reduced staff to one nurse and one social worker for in-home care.
12. Milwaukee-based Froedtert closed the behavioral health unit at Froedtert Menomonee Falls (Wis.) May 12.
13. Welch (W.Va.) Community Hospitalannounced plans to close its long-term care unit. The closure of the 59-bed unit is part of the hospital’s transition to the West Virginia University Health System.
14. Peoria, Ill.-based OSF HealthCare is closing its labor and delivery services at OSF Heart of Mary Medical Center in Urbana, Ill. Starting in September, labor and delivery patients will be redirected to OSF Sacred Heart Medical Center in Danville, Ill. or OSF St. Joseph Medical Center in Bloomington, Ill.
15. Northern Maine Medical Center in Fort Kent closed its obstetrics unit May 26. The move comes as birth rates decline in the area along with staffing trouble.
16. Philadelphia-based Jefferson Health ended acute care, general surgery and emergency services at Einstein Medical Center Elkins Park (Pa.) and convert the facility solely into a physical rehabilitation provider.
17. CoxHealth closed the labor and delivery unit at Cox (Mo.) Monett Hospital, citing difficulties recruiting obstetricians and family practice physicians.
18. Warsaw, N.Y.-based Wyoming County Community Health Systemended its birthing services June 1 amid financial challenges and declining births in the area.
19. Alta Vista Regional Hospital in Las Vegas, N.M., ended intensive care unit services June 3. The hospital said the change would allow it to focus on its highly utilized medical-surgical unit.
20. Springfield, Ore.-based McKenzie-Willamette Medical Center closed its maternity health practice July 7. The for-profit McKenzie-Willamette hospital said the 11-employee midwifery program was “unsustainable.”
21. Renton, Wash.-based Providence ended labor and delivery at Petaluma (Calif.) Valley Hospital May 1 until further notice.
22. Gardner, Mass.-based Heywood Hospitalclosed its pulmonary unit in mid-April due to financial reasons.
23. Yale New Haven (Conn.) Hospital “ceased use” of its emergency use annex April 11 amid discussions to extend its certificate of occupancy.
24. Chelsea (Mich.) Hospitalclosed its inpatient behavioral health unit and moved 12 of its beds to Trinity Health Ann Arbor.
25. Danbury, Conn.-based Nuvance Health closedThompson House, a 100-bed rehabilitation facility in Rhinebeck, N.Y., and laid off its 102 employees, effective April 12.
26. Holly Springs, Miss.-based Alliance HealthCare System began transitioning to rural emergency hospital status March 31, meaning it will end all inpatient care services.
27. MercyOne North Iowaclosed its hospice facility in Mason City April 17 amid industry pressures of inflation and high labor costs.
28. Brewer, Maine-based Northern Light Health is no longer providing cataract, glaucoma and oculoplastic surgeries at Eastern Maine Medical Center in Bangor.
29. Plymouth, Ind.-based St. Joseph Health Systemclosed its New Beginnings Birthplace center because it has been unable to attract an obstetrician. It also closed its OB-GYN office March 31.
30. Springfield, Mass.-based Baystate Health and medical services provider Shields Healthclosed their urgent care clinic locations in Feeding Hills, Longmeadow and Westfield, Mass., on March 31.
31. Palomar Medical Center Poway (Calif.), part of Escondido, Calif.-based Palomar Health, closed its labor and delivery unit, at least temporarily, in June.
32. A combination of a loss of pediatricians, changing demographics and some of the strictest abortion laws in the country forced Sandpoint, Idaho-based Bonner General Hospital to end obstetrics services.
33. Cabell Huntington (W.Va.) Hospital, part of Mountain Health Network, closed its CHH Surgery Center April 28 and is phasing out its home health services to better align its resources and reduce costs amid financial headwinds.
34. The only hospital in Manitowoc, Wis., a city of nearly 35,000 — Froedtert Holy Family Memorial Hospital — stopped all obstetrics care June 1.
35. Citing a lack of provider coverage, Ocean Springs, Miss.-based Singing River Health Systemsaid it would end obstetric services, which include labor and delivery, at Singing River Gulfport (Miss.), at least temporarily. The move became effective April 1.
36. Astria Toppenish (Wash.) Hospital is one of many rural hospitals closing labor and delivery care due to costs, creating maternity deserts in areas that need care most, The New York Times reported.
37. Cleveland-based University Hospitalsended labor and delivery services at UH Lake West in Willoughby, Ohio, April 15. The hospital said services would be consolidated at TriPoint in Concord Township, which is about 15 miles away.
38. Jefferson, Mo.-based Capital Region Medical Center closed two clinics in Holts Summit and St. Elizabeth, Mo., April 15.
39. In February, Trinity Health Muskegon (Mich.)announced plans to temporarily close a 30-bed surgical floor due to staffing shortages.
40. St. Mark’s Medical Center in La Grange, Texas, cut nearly half its staff and various services as it looks to survive amid significant financial challenges. Service cuts include inpatient and surgical services, post-acute skilled rehab care, its orthopedic clinic, speech therapy and ambulatory care.
41. OhioHealth’s Shelby Hospitalstopped providing maternity services Feb. 28. Maternity services are provided 13 miles away at OhioHealth Mansfield Hospital.
42. Arcata, Calif.-based Mad River Community Hospitalcut 27 jobs as it suspends its home health services program. The program will be suspended upon the completion of services to the hospital’s existing patients, which was expected to be in April.
43. Oroville (Calif.) Hospitalclosed Golden Valley Home Health, the hospital’s home health business.
44. Ascension Providence Hospital-Southfield (Mich.)ended midwifery services in February.
45. Rumford (Maine) Hospitalclosed its maternity program March 31 after 97 years in service.
A bipartisan quartet of influential senators is tapping tax regulators within the U.S. Treasury for detailed information on nonprofit hospitals’ reported charity care and community investments, the latest in legislators’ increasing scrutiny of tax-exempt hospitals’ business practices.
In a pair of letters (PDF) sent Monday, Sens. Elizabeth Warren, D-Massachusetts, Raphael Warnock, D-Georgia, Bill Cassidy, M.D., R-Louisiana, and Chuck Grassley, R-Iowa, wrote they “are alarmed by reports that despite their tax-exempt status, certain nonprofit hospitals may be taking advantage of this overly broad definition of ‘community benefit’ and engaging in practices that are not in the best interest of the patient.”
They also outlined studies from academic and policy groups highlighting that the tax-exempt status of the nation’s nonprofit hospitals collectively was worth about $28 billion in 2020 and how this tally paled in comparison to the charity care most of those hospitals had provided during that same period.
Such studies have been quickly contested by the hospital lobby, which highlights that charity care is just one component of the broader activities that constitute a nonprofit hospital’s community benefit spending.
However, that ambiguity was squarely in the crosshairs of the legislators who said the long-standing community benefit standard “is arguably insufficient in its current form to guarantee protection and services to the communities hosting these hospitals.”
They cited a 2020 report from the Government Accountability Office that found oversight of nonprofit hospitals’ tax exemptions was “challenging” due to the vague definition of community benefit.
Though the IRS implemented several of the office’s recommendations from the report, “more is required to ensure nonprofit hospitals’ community benefit information is standardized, consistent and easily identifiable.” Included here could be additional updates to Form 990’s Schedule H, where nonprofits detail their community benefits and related activities.
To get a better handle on the agencies’ current oversight, the legislators requested from the IRS and the Treasury’s Tax Exempt & Government Entities Division a laundry list of information related to nonprofits’ tax filings from the last several years, including “a list of the most commonly reported community benefit activities that qualified a nonprofit hospital for tax exemptions in FY2021 and FY2022.”
They also sought lists of the nonprofit hospitals that were flagged, penalized or had their tax-exempt status revoked for violating community benefit standard requirements.
In another letter to the Treasury’s inspector general for tax administration, they asked the auditor to update their upcoming reviews to evaluate existing standards for financial assistance policy and other “practices that reduce unnecessary medical debt from patients who qualify for free or discounted care.”
The lawmakers also asked the inspector general to explore how often nonprofit hospitals bill patients with “gross charges” and to make sure the IRS is doing enough to ensure hospitals are making “’reasonable efforts’ to determine whether individuals are eligible for financial assistance before initiating extraordinary collection actions.”
Both letters from the senators gave the tax regulators 60 days to provide the requested information.
Kaiser Permanente built on 2023’s strong start with $2.08 billion of net income during the quarter ended June 30, bringing its midyear total to about $3.29 billion, the integrated system announced late Friday.
Operating income was also strong at $741 million (2.9% margin) and raised the organization’s six-month performance to $974 million (1.9% margin).
The numbers are both a sequential improvement and a stark turnaround from 2022. By the midpoint of that year, Kaiser Permanente was reporting a $1.3 billion net loss for the quarter and an $89 million operating gain (0.4% margin). Across 2022’s first half, the system had been down a total of $2.26 billion and added just $17 million from operations (0.0% margin).
The Oakland, California-based nonprofit is likely safe from repeating the nearly $4.5 billion net loss and $1.3 billion operating loss of full-year 2022.
Leadership, however, noted that the integrated system historically sees higher operating margins during the first half of the year “due in part to the annual enrollment cycle and seasonal care.”
“Our second-quarter financial results reflect operational improvements that, together with our ongoing expense reduction efforts, will help us face additional financial pressures in the second half of the year,” Kathy Lancaster, executive vice president and chief financial officer at Kaiser Permanente, said in a release. “The process of building our financial performance back to pre-pandemic levels requires that we continue to redesign our cost structure to support investments in our facilities, technology and people while staying competitive in a dynamic healthcare marketplace.”
Kaiser Permanente reported $25.17 billion in operating revenues for the second quarter, a 7.2% increase year over year. Operating expenses increased 4.5% year-over-year to $24.42 billion.
“Like all health systems, Kaiser Permanente is experiencing ongoing cost headwinds and volatility driven by inflation, labor shortages, and the lingering effects of the pandemic on access to care and service,” the system wrote in a release.
Kaiser Permanente’s membership has increased by more than 81,000 members since the start of the year and sits at almost 12.7 million as of June 30. The organization noted that it has kicked off an outreach campaign for Medicaid members “to ensure they have critical enrollment information as states go through the mandated process of eligibility redetermination.”
The largest impact on Kaiser Permanente’s bottom line came from investments. Owing to “favorable financial market conditions,” the organization recorded $1.34 billion in “other income and expense,” nearly a full reversal of the $1.39 billion loss on the same line item it’d logged during the same period last year.
The system’s capital spending reached $824 million for the quarter, which was up from $789 million during the second quarter of 2022 but a pullback from the first quarter of 2023’s $930 million.
“The post-pandemic financial pressures have led many in the industry to cut back on care and service,” CEO Greg Adams said in an accompanying statement. “At Kaiser Permanente, we remain focused on improving access and affordability for our patients, members and communities, which requires continued investment in care and coverage. … I want to thank all employees and physicians for turning the disruptions and challenges of the past three years into opportunities to make our healthcare system stronger and more equitable, with improved outcomes for all.”
Kaiser Permanente is the largest nonprofit health system in the country by revenue with more than $95 billion in annual revenues. As of June 30, it spanned 39 hospitals, 622 medical offices and 43 clinics in addition to its millions of covered health plan members.
Earlier in the year the system highlighted efforts to trim administrative and discretionary spending as well as a workforce push that improved clinical hiring by 15% year over year. It is in the midst of negotiating a new labor contract covering 85,000 unionized healthcare workers who are seeking workforce development investments and higher staffing levels across clinical settings.
The organization is also working toward its high-profile acquisition of fellow integrated nonprofit Geisinger Health, which Kaiser Permanente said would be the first step toward a cross-country value-based care organization called Risant Health.
Starting next month, UnitedHealthcare says it will move forward with plans to drop prior authorization requirements for a range of procedures, including dozens of radiology services and genetic tests, among others.
Why it matters:
UnitedHealth is among the health insurance giants who have announced plans to cut back on prior authorization as federal regulators consider tougher curbs on the practice.
Catch up quick:
Prior authorization is often criticized by patients and doctors, who complain they are an administrative burden or impede necessary care. Insurers, meanwhile, say prior authorization provides important guardrails against improper health care utilization, helping to keep costs down.
UnitedHealth, the largest commercial U.S. insurer, previously said its prior authorization removals will represent roughly 20% of its overall prior authorization volume.
Cigna and Aetna also announced plans to roll back some prior authorization requirements.
The Centers for Medicare and Medicaid Services proposed a rule to limit the amount of time insurers have to review requests on services for which they require prior approval, BenefitsPro previously reported.
Congress is also eyeing a plan to streamline and add transparency to the process by which Medicare Advantage plans can deny coverage for services via prior authorization.
Zoom in:
UnitedHealth says the removals will take effect Sept. 1 and Nov. 1 across the vast majority of its plans.
The company also spelled out which procedures would see prior authorization requirements removed. For instance, hundreds of codes for genetic testing — accounting for tens of thousands of prior authorization requests a year from commercial and Medicaid members — are among those that will be removed, officials said.
A code for cardiology stress test prior authorization for Medicare Advantage members will also be eliminated, reducing roughly 316,000 prior authorization requests a year.
The company next year also will roll out a “gold card” program eliminating most prior authorization requirements for doctors who have high approval rates.
Flashback: Earlier this summer, UnitedHealth walked back a controversial plan to require prior authorizations for colonoscopies and other endoscopic procedures.
A federal drug discount program for safety-net providers that’s been a perennial source of fierce disputes among health care industry powerhouses is back in the spotlight, with billions of dollars at stake.
The big picture:
Separate but coinciding issues are generating renewed focus on the decades-old 340B program, which requires that drugmakers give large discounts on outpatient drugs to health care providers serving low-income patients.
A Biden administration proposal to issue hefty back payments due to 340B providers, drugmakers’ efforts to limit discounts, and rebooted congressional interest in broader reforms are again igniting debate about the program’s scope.
Context:
The Supreme Court last year unanimously sided with hospitals who challenged a nearly 30% reduction to their 340B payments by the Centers for Medicare and Medicaid Services that began under the Trump administration.
In response to the court decision, CMS last month announced a $9 billion plan to repay 340B providers that’s generated some controversy. While 340Bhospitals are happy they’re getting paid back, industry groups are upset that the payments are funded by clawing back money to other hospitals.
Meanwhile, the Biden administration is battling drugmakers in court over restrictions they’ve placed on where hospitals can use their 340B discounts.
A bipartisan group of senators this summer also released a request for information on how to improve stability and oversight within the program.
Hospitals could face further cutbacks if Congress or the courts place new limits on 340B.
Flashback:
The 340B program began in 1992 to help providers serving patient populations who struggled to afford their prescription drugs. It allowshospitals and other safety-net providers like community health clinics to save an average of 25% to 50% on drug purchases, according to the federal government.
When hospitals partner with off-site pharmacies to dispense drugs, the pharmacies also benefit financially from 340B savings.
The program has grown significantly since its inception, increasing from 8,100 participating safety-net providers in 2000 to 50,000 in 2020.
Between the lines:
The expansive program growth has drawn lawmakers’ scrutiny and complaints from pharmaceutical companies, who accuse providers of using the program to pad their profits rather than help vulnerable patients. Providers dispute those accusationsand say the program helps them stretch limited federal resources.
More than 20 drug companies have placed restrictions on when providers can use 340B discounts at off-site pharmacies. Drug companies say the limits help prevent them from having to give duplicate discounts, which occurswhen both the provider and state Medicaid agency receive a discount on the same drug.
The Biden administration asked several drugmakers to lift their 340B restrictions and threatened fines if they don’t comply.
Several drugmakers have sued the administration, arguing federal officials didn’t have the right to stop them from limiting discounts. One appellate judge ruled in favor of drugmakers earlier this year, and two other cases are pending in federal appellate courts.Experts say the cases could go all the way to the Supreme Court.
As the legal fight plays out, 340B providers are urging Congress to approve new measures to prevent drugmakers from restricting access to discounts.
The other side: Drugmakers, meanwhile, want lawmakers to tightenhospital eligibility standards and place stronger limits on how 340B pharmacies can profit from the program.
Of note: Rural hospitals, some of which were spared from the 340B cuts made years ago, are especially concerned about the hit they would takefrom CMS’ proposed funding clawbacks.
Rural facilities today rely heavilyon 340B to offset other financial losses, Brock Slabach, chief operations officer at the National Rural Health Association, told Axios.
“You can’t get out of this problem without harming those who were helped,” Slabach said.
What we’re watching: Expect to keep hearing about 340B in the coming months.
CMS still needs to finalize the 340B repayment planafter the public comment ends Sept. 5.
The D.C. Circuit Court of Appeals and the 7th Circuit Court of Appeals will issue rulings on whether the Biden administration can reverse drugmakers’340B restrictions.
Congress could take up a serious reform effort following the Senate’s information request, though that would take time.
Seniors face more than $50 billion in unpaid medical bills, many of which they shouldn’t have to pay, according to a federal watchdog report.
In an all-too-common scenario, medical providers charge elderly patients the full price of an expensive medical service rather than work with the insurer that is supposed to cover it. If the patient doesn’t pay, the provider sends the bill into collections, setting off a round of frightening letters, humiliating phone calls and damaging credit reports.
That is one conclusion of a recent report titled Medical Billing and Collections Among Older Americans, from the Consumer Financial Protection Bureau.
The report recounts a horror story from a patient in southern Pennsylvania over a hospital visit, which should have been covered by insurance.
“I never received a bill from anyone,” the patient said in a 2022 complaint. Then came a phone call from a collection agency. “The woman on the phone started off aggressively screaming at me,” saying the patient owed $2,300.
“I told her there must be some mistake, that both Medicare and my supplement insurance would have covered it. It has in the past. She started screaming, very loud, ‘If you don’t pay me right now, I will put this on your credit report.’ I told her, ‘If you keep screaming at me, I will hang up.’ She continued, so I hung up.”
Nearly 4 million seniors reported unpaid medical bills in 2020, even though 98 percent of them had insurance, the report found. Medicare, the national health insurance program, was created to protect older Americans from burdensome medical expenses.
Total unpaid medical debt for seniors rose from $44.8 billion in 2019 to $53.8 billion in 2020, even though older adults reported fewer doctor visits and lower out-of-pocket costs in 2020.
Medical debt among seniors is rising partly because health care costs are going up, agency officials said. But much of the $53.8 billion is cumulative, they said, debt carried over from one year to the next. Figures for 2020 were the latest available.
Millions of older Americans are covered by both Medicare and Medicaid, a second federal insurance program for people of limited means. Federal and state laws widely prohibit health care providers from billing those patients for payment beyond nominal copays.
Yet, those low-income patients are more likely than wealthier seniors to report unpaid medical bills. The agency’s findings suggest that health care companies are billing low-income seniors “for amounts they don’t owe.” The findings draw from census data and consumer complaints collected between 2020 and 2022.
Many complaints depict medical providers and collection agencies relentlessly pursuing seniors for payment on bills that an insurance company has rejected over an error, rather than correcting the error and resubmitting the claim.
“Many of these errors likely are avoidable or fixable,” the report states, “but only a fraction of rejected claims are adjusted and resubmitted.”
When a patient points out the error, the creditors might agree to fix it, only to ignore that pledge and double down on the debt collection effort.
An Oklahoma senior recounted a collection agency nightmare that followed a hospital stay. After paying all legitimate bills, the patient discovered new charges from a collection agency on a credit report. In subsequent months, additional charges appeared.
The patient assembled billing statements and correspondence, hoping to clear the bogus charges. “I then proceeded to spend every weekday, all day, for two weeks on the phone, trying to find out who was billing me and why,” the patient said in a 2021 complaint.
The Oklahoman eventually paid the bills, “even though I don’t owe them.” Then, more charges appeared.
“Nice racket they have going,” the patient quipped.
As anyone with health insurance knows, medical providers occasionally charge patients for services that should have been covered by the insurer. Someone forgets to submit the claim, or types the wrong billing code or omits crucial documentation. Some providers charge patients more than the negotiated rate, a discounted fee set between the provider and insurer.
Americans spend hours of their lives disputing such charges. But many seniors aren’t up to the task.
“It’s tiring to have multiple conversations, sitting on the phone for an hour, chasing representatives,” said Genevieve Waterman, director of economic and financial security at the National Council on Aging.
“I think technology is outpacing older adults,” she said. “If you don’t have the digital literacy, you’re going to get lost.”
Older adults are more likely than younger people to have multiple chronic health conditions, which can require more detailed insurance documentation and face greater scrutiny, yielding more billing errors and denied claims, the federal report says.
Seniors are also more likely to rely on more than one insurance plan. As of 2020, two-thirds of older adults with unpaid medical bills had two or more sources of insurance.
Multiple insurers means a more complex billing process, making it harder for either patient or provider to file a claim and see that it is paid. With Medicaid, “you have 50 states, plus the territories,” said one official from the federal agency, speaking on condition of anonymity. “They each have their own billing system.”
In an analysis of Medicare complaints filed between 2020 and 2022, the agency found that 53 percent involved debt collectors seeking money the patient didn’t owe. In a smaller share of cases, patients reported that collection agents threatened punitive action or made false statements to press their case.
The complaints “illustrate how difficult it is to identify an inaccurate bill, learn where it originated, and correct other people’s mistakes,” the report states. “Some providers refuse to talk to consumers because the account has already been referred to collections. Even when providers seem willing to correct their own mistakes, debt collectors may continue attempting to collect a debt that is not owed and refuse to stop reporting inaccurate data.”
Rather than carry on a fight with collection agents over multiple rounds of calls and correspondence, many seniors become ensnared in a “doom loop,” the report says, convinced their appeal is hopeless. They pay the erroneous bill.
“I think some people get to the point where they just throw up their hands and give up a credit card number just to make the problem go away,” said Juliette Cubanski, deputy director of the Program on Medicare Policy at KFF.
Debt takes a toll on the mental and physical health of seniors, research has shown. Older adults with debt are more prone to a range of ailments, including hypertension, cancer and depression.
As the Oklahoma patient said, recalling a years-long battle over unpaid bills, “It nearly sent me back to the hospital.”
Healthcare is a capital intense industry: facilities, technologies, workforces, infrastructures and clinical breakthroughs require access to funding from banks willing to lend and investors willing to bet.
For most, being a limited partner in a private equity fund is an attractive hedge against inflation, especially a fund that targets healthcare wherein demand is increasing and shifting, costs are soaring and consumers are receptive to new alternatives.
Private equity is big business:
Private equity funds have nearly $2 trillion in dry powder to invest. The Securities and Exchange Commission (SEC) recently reported that private funds’ gross assets now surpass those of the commercial banking sector at more than $25 trillion–up from $9 trillion in 2012. And the American Investment Council reports that…
· 12 million are employed at Private Equity-Backed Companies.
· 32,041 Private Equity-Backed Businesses have been funded since 2017.
· 34 million Americans Depend on Private Equity to Support Their Retirements.
In 2021, the Medicare Payment Advisory Commission (MedPAC) released a report affirming that private equity investments “play an important role providing hospitals, nursing homes, and physician practices with capital and expertise to navigate an increasingly complex health care landscape” but offered Congress no recommendations about how to navigate its growing role.
The playbook for PE investing in healthcare services is widely-known:
· Thesis: Healthcare is expensive, wasteful and unsustainable in its current structure: Incumbents in healthcare services, especially hospitals and physicians, need capital to survive and are receptive to private money.
· Strategy:Land, Expand, and Exit in 5-7 years: Leverage debt at competitive rates to fund most of the deal; operate aggressively by lowering operating costs; grow revenue aggressively thru adjacency acquisitions and partnerships; price aggressively and avoid compliance penalties associated with safety or quality issues.
· Keys to success: Timing, attractive deal terms, a scalable operating platform, exceptional CEO and dispassionate exit strategy. And for navigating expectations of limited partners (high net worth individuals, pension funds, et al), the General Partner gets a 2% management fee and 20% of the value created in the enterprise at exit.
My take:
For the past decade, PE investments in distressed hospitals, medical specialties (radiology, dentistry, dermatology et al), outpatient surgery/ diagnostic facilities and logistics solutions have been popular targets. Going forward, opportunities in services will increasingly center on business models that produce significant, near-term cost-reduction compared to alternative solutions as issues around affordability and employer health costs mount. But three issues will impact the role and success of PE investing in healthcare services looking ahead:
1-Heightened Regulatory Scrutiny: There’s growing concern in Congress and among regulatory agencies about the role of private equity in healthcare services.
· In Congress and in some states, ownership restrictions and added disclosure requirements are being considered.
· The SEC is advancing changes to require added protections for investors in PE funds.
· The FTC is examining the correlation between PE ownership and business practices and consumer choices.
· CMS is considering analyzing the association between PE ownership and prices.
2-The Maturity Wall: “A maturity wall is fast approaching for PE funds that are nearing the end of their term life to distribute their capital back to investors through exits. PE investors will need to pick up their exit pace or will be confronted with 20% to 26% of the capital initially invested by funds to hit the maturity wall. The cumulative amount of still- held investments could grow to over $360 billion in the next 12 years.” (Pitchbook June 30, 2023). The maturity wall will be especially problematic in communities where medical practices and/ancillary services providers acquired thru PE-sponsored deals are forced to switch owners necessitating possible disruptions in care.
3-Heightened Competition among PE Funds: PE funds compete for good deals and satisfied investors. Bigger funds have advantages over smaller funds i.e., domain expertise, analytic models and access to effective executive talent. The deal landscape in healthcare services has slowed though opportunities remain. It’s a buyer’s market prompting intensified competition between funds and aggressive negotiations between buyers and sellers. Qualified investors are comparing fund performance and moving funds to the most successful.
The healthcare services market in the U.S. is worth $3.5 trillion and is forecast to increase at 5%/yr. for the next decade. It’s traditionally dominated by nonprofit operators and market conditions that favor incumbents over newbies, bigger over smaller and business to business (B2B) models over business to consumer (B2C). That’s changing. Investor-ownership in healthcare services is increasing. Distinctions between privately operated PE owned hospitals and services providers and investor-owned publicly traded operators are being scrutinized by regulators even as the tax-exempt status enjoyed by not-for-profits is under the microscope.
Access to capital that’s cost-effective is critical to the future of health services providers. PE will be increasingly part of that discussion and with it, added risk.
The U.S. health system is big and getting bigger. It is labor intense, capital intense, and highly regulated. Each sector operates semi-independently protected by local, state and federal constraints that give incumbents advantages and dissuade insurgents.
Competition has been intramural:
Growth by horizontal consolidation within sectors has been the status quo for most to meet revenue and influence targets. In tandem, diversification aka vertical consolidation and, for some, globalization in each sector has distanced bigger players from smaller:
insurers + medical groups + outpatient facilities + drug benefit managers
retail pharmacies + primary & preventive care + health & wellbeing services + OTC products/devices
regulated medical devices + OTC products for clinics, hospitals, homes, workplaces and schools.
The landscape is no man’s land for the faint of heart but it’s golden for savvy private investors seeking gain at the expense of the system’s dysfunction and addictions—lack of price transparency, lack of interoperability and lack of definitive value propositions.
What’s ahead?
Everyone in the U.S. health system is aware that funding is becoming more scarce and regulatory scrutiny more intense, but few have invested in planning beyond tomorrow and the day after. Unlike drug and device manufacturers with global markets and long-term development cycles, insurers and providers are handicapped. Insurers respond by adjusting coverage, premiums and co-pays annually. Providers—hospitals, physicians, long-term care providers and public health programs– have fewer options. For most, long-range planning is a luxury, and even when attempted, it’s prone to self-protection and lack of objectivity.
Changes to the future state of U.S. healthcare are the result of shifts in these domains:
They apply to every sector in healthcare and define the context for the future of each organization, sector and industry as a whole:
The Clinical Domain: How health, diseases and treatments are defined and managed where and by whom; how caregivers and individuals interact; how clinical data is accessed, structured and translated through AI enabled algorithms; how medication management and OTC are integrated; how social determinants are recognized and addressed by caregivers and communities: and so on. The clinical domain is about more than doctors, nurses, facilities and pills.
The Technology Domain: How information technologies enable customization in diagnostics and treatments; how devices enable self-care; how digital platforms enable access; how systemness facilitates integration of clinical, claims and user experience data; how operating environments shift to automation lower unit costs; how sites of care emerge; how caregivers are trained and much more. Proficiency in the integration of technologies is the distinguishing feature of organizations that survive and those that don’t. It is the glue that facilitates systemness and key to the system’s transformation.
The Regulatory Domain: How affordability, value, competition, choice, healthcare markets, not-for-profit and effectiveness are defined; how local, state and federal laws, administrative orders by government agencies and executive actions define and change compliance risks; how elected officials assess and mitigate perceived deficiencies in a sector’s public accountability or social responsibility; how courts adjudicate challenges to the status quo and barriers to entry by outsiders/under-served populations; how shareholder ownership in healthcare is regulated to balance profit and the public good; et al. Advocacy on behalf of incumbents geared to current regulatory issues (especially in states) is compulsory table stakes requiring more attention; evaluating potential regulatory environment shifts that might fundamentally change the way a system is structured, roles played, funded and overseen is a luxury few enjoy.
The Capital Domain: how needed funding for major government programs (Medicare, Medicaid, Children’s, Military, Veterans, HIS, Dual Eligibles et al) is accessed and structured; how private investment in healthcare is encouraged or dissuaded; how monetary policies impact access to debt; how personal and corporate taxes impact capitalization of U.S. healthcare; how value-based programs reduce unnecessary costs and improve system effectiveness; how the employer tax exemption fares long-term as employee benefits shrink; how U.S. system innovations are monetized in global markets; how insurers structure premiums and out of pocket payments: et al. The capital domain thinks forward to the costs of capital it deploys and anticipated returns. But inputs in the models are wildly variable and inconsistent across sectors: hospitals/health systems vs. global private equity healthcare investors vs. national insurers’ capital strategies vary widely and each is prone to over-simplification about the others.
The Consumer Domain: how individuals, households and populations perceive and use the system; how they assess the value of their healthcare spending; how they vote on healthcare issues; how and where they get information; how they assess alternatives to the status quo; how household circumstances limit access and compromise outcomes; et al. The original sin of the U.S, health system is its presumption that it serves patients who are incapable/unwilling to participate effectively and actively in their care. Might the system’s effectiveness and value proposition be better and spending less if consumerization became core to its future state?
For organizations operating in the U.S. system, staying abreast of trends in these domains is tough. Lag indicators used to monitor trends in each domain are decreasingly predictive of the future. Most Boards stay focused on their own sector/subsector following the lead of their management and thought leadership from their trade associations. Most are unaware of broader trends and activities outside their sector because they’re busy fixing problems that impact their current year performance. Environmental assessments are too narrow and short-sighted. Planning processes are not designed to prompt outside the box thinking or disciplined scenario planning. Too little effort is invested though so much is at risk.
It’s understandable. U.S. healthcare is a victim of its success; maintaining the status quo is easier than forging a new path, however obvious or morally clear. Blaming others and playing the victim card is easier than corrective actions and forward-thinking planning.
In 10 years, the health system will constitute 20% of the entire U.S. economy and play an outsized role in social stability. It’s path to that future and the greater good it pursues needs charting with open minds, facts and creativity. Society deserves no less.