Cleveland Clinic ended the first three months of this year with higher revenue, but rising expenses offset those gains, according to financial documents released May 26.
The health system’s revenue climbed to $3.03 billion in the first quarter of this year, which ended March 31, up from $2.81 billion in the same period of 2021. The system’s net patient service revenue increased from $2.53 billion in the first quarter of 2021 to $2.73 billion in the same period this year.
“Operating revenues in the first quarter of 2022 were impacted by lower patients served, partially due to the postponement of nonessential surgeries and procedures during the month of January,” the system said in an earnings release.
In the first quarter of this year, Cleveland Clinic facilities had 57,864 inpatient admissions and 61,103 surgical cases. In the same period a year earlier, the system reported 60,338 inpatient admissions and 63,051 surgical cases.
Cleveland Clinic reported expenses of $2.96 billion in the first quarter of this year, up from $2.56 billion in the same quarter of 2021. The system saw expenses rise across all categories, including supplies and salaries, wages and benefits.
The hospital system ended the first quarter of 2022 with an operating loss of $104.5 million, compared to operating income of $61.7 million in the same period of 2021.
Cleveland Clinic posted a net loss of $282.46 million in the first quarter of this year, compared to net income of $350.26 million in the same period a year earlier.
The bill is coming due for federal loans given to hospitals early in the COVID-19 pandemic, adding to their financial woes, Oregon Public Broadcastingreported May 28.
The Medicare Accelerated and Advance Payment program offered hospitals short-term interest- free loans, according to the report. These loans are coming due as hospitals’ costs are rising quickly and revenue from patient stays and surgeries is growing more slowly.
The idea behind the program was that hospitals would be able to pay back the advance once the pandemic passed and operations returned to normal, according to the report. Hospitals are still dealing with the effects of the pandemic, but the federal government wants to recoup the money to keep Medicare funded.
In March 2021, HHS began recovering those cash advances by paying hospitals 25 percent less for Medicare reimbursement claims, according to the report. Earlier this year, HHS began paying hospitals 50 percent less for reimbursement claims.
Hospitals lobbied for the loans to be forgiven, but were unsuccessful, according to the report.
Here are 11 health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings, Moody’s Investors Service and S&P Global Ratings.
1. Morristown, N.J.-based Atlantic Health System has an “Aa3” rating and stable outlook with Moody’s. The health system has strong operating performance and liquidity metrics, Moody’s said. The credit rating agency expects Atlantic Health System to sustain strong performance to support capital spending.
2. Greensboro, N.C.-based Cone Health has an “AA” rating and stable outlook with Fitch. The health system has a leading market share and a favorable payer mix, Fitch said. The health system’s broad operating platform and strategic capital investments should enable it to return to stronger operating results, the credit rating agency said.
3. Falls Church, Va.-based Inova Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has a consistently strong operating cash flow margin and ample balance sheet resources, Moody’s said. Inova’s financial excellence will remain undergirded by its favorable regulatory and economic environment, the credit rating agency said.
4. Vineland, N.J.-based Inspira Health Network has an “AA-” rating and stable outlook with Fitch. The health system has strong operating performance, a leading market position in a stable service area and a growing residency program, Fitch said. The credit rating agency expects the system’s growing outpatient footprint and an increase in patient volumes to support its operating stability.
5. Oakland, Calif.-based Kaiser Permanente has an “AA-” rating and stable outlook with Fitch. The health system has a strong financial profile, and the system’s operating platform is “arguably the most emulated model” for nonprofit healthcare delivery in the U.S., Fitch said. By revenue base, Kaiser is the largest nonprofit health system in the U.S., and it is the most fully integrated healthcare delivery system in the country, according to the credit rating agency.
6. Mass General Brigham has an “Aa3” rating and stable outlook with Moody’s and an “AA-” rating and stable outlook with S&P. The Boston-based health system has an excellent clinical reputation, good financial performance and strong balance sheet metrics, Moody’s said. The credit rating agency said it expects Mass General Brigham to maintain a strong market position and stable financial performance.
7. Rochester, Minn.-based Mayo Clinic has an “Aa2” rating and stable outlook with Moody’s. The credit rating agency said Mayo Clinic’s strong market position and patient demand will drive favorable financial results. The health system “will continue to leverage its excellent reputation and patient demand to continue generating favorable operating performance while maintaining strong balance sheet ratios,” Moody’s said.
8. Methodist Health System has an “Aa3” rating and stable outlook with Moody’s. The Dallas-based system has strong operating performance, and investments in facilities have allowed it to continue to capture more market share in the fast-growing Dallas-Fort Worth, Texas, area, Moody’s said. The credit rating agency said it expects Methodist Health System’s strong operating performance and favorable liquidity to continue.
9. Traverse City, Mich.-based Munson Healthcare has an “AA” rating and stable outlook with Fitch. The health system has a strong market position, a good payer mix and robust cash-to-adjusted debt levels, Fitch said. The credit rating agency expects the system to weather an expected period of weakened operating cash flow margins.
10. Albuquerque, N.M.-based Presbyterian Healthcare Services has an “Aa3” rating and stable outlook with Moody’s and an “AA” rating and stable outlook with Fitch. Presbyterian Healthcare Services is the largest health system in New Mexico, and it has strong revenue growth and a healthy balance sheet, Moody’s said. The credit rating agency said it expects the health system’s balance sheet and debt metrics to remain strong.
11. University of Iowa Hospitals and Clinics has an “Aa2” rating and stable outlook with Moody’s. The Iowa City-based health system, the only academic medical center in Iowa, has strong patient demand and excellent financial management, Moody’s said. The credit rating agency said it expects the health system to continue to manage the pandemic with improved operating cash flow margins.
A friend called me for medical advice two weeks ago. He’s single, in his thirties and generally healthy, but he’d developed a dry cough with mild congestion. After a self-administered Covid-19 test turned up negative results, he remained suspicious he could be infected.
He was set to fly west in a couple of days for a conference and dreaded the thought of infecting other passengers. I recommended a PCR test if he wanted to be more certain. When the lab results came back positive, he spent the next five days at home alone (per CDC guidance).
If you were in his shoes, chances are you, too, would make a reasonable effort to avoid infecting others. In the near future, that won’t be the case.
Americans are playing it safe—for now
A whopping 91% of Americans no longer consider Covid-19 a “serious crisis.” Social distancing has reached a low point as public-health restrictions continue to ease up.
Yet, there’s still one aspect of the pandemic Americans are taking very seriously.
As a society, we still expect people who test positive for Covid-19 to stay home and minimize contact with others. As a result of these expectations, 4 in 10 workers (including 6 in 10 low-income employees) have missed work in 2022. Overall, the nation’s No. 1 concern related to Omicron is “spreading the virus to people who are at higher risk of serious illness.”
Most Americans are eager to move on from the pandemic, but those who are sick continue to avoid actions that may potentially spread the virus.
Call it what you will—group think, peer pressure or the fear of violating cultural taboos—people don’t want to put others in harm’s way. That’s true, according to polls, regardless of one’s party affiliation or vaccination status.
What’s immoral today will be appropriate tomorrow
Don’t get used to these polite and socially conscious behaviors. All of it is about to change in the not-distant future. Let me paint a picture of tomorrow’s new normal:
A factory worker tests positive over the weekend for Covid-19 and comes to work on Monday without a mask, informing no one of his infection.
A vacationer with mild Covid-19 symptoms refuses to postpone her spa weekend, availing herself of massages, facials and group yoga classes.
A couple plans an indoor wedding for 200-plus, knowing the odds are likely that dozens of people will get infected and that some of those guests will be elderly and immunosuppressed.
These actions, which seem inappropriate and immoral now, will become typical. It’s not that people will suddenly become less empathetic or more callous. They’ll simply be adjusting to new social mores, brought about by a unique viral strain and an inevitable evolution in American culture.
A crash course in a unique virus
To understand why people will behave in ways that seem so unacceptable today, you must understand how the Omicron variant spreads compared to other viruses.
Scientists now know that Omicron (and its many decimal-laden strains: BA.2, BA.2.12.1, BA.4, BA.5, etc.) is the most infectious, fastest-spreading respiratory virus in world history. The Mayo Clinic calls this Covid-19 variant “hyper-contagious.”
“A single case could give rise to six cases after four days, 36 cases after eight days, and 216 cases after 12 days,” according to a report in Scientific American. As a result, researchers predict that 100 million Americans will become infected with Omicron this year alone—via new infections, reinfections and vaccination breakthroughs.
In addition to Omicron’s high transmissibility, the virus is also season-less. Whereas influenza arrives each winter and exits in the spring, Americans will continue to experience high levels of Covid-19 infection year-round—at least for the foreseeable future.
With its 60-plus mutations, immense transmissibility and lack of seasonality, Omicron is an exceptional virus: one that will infect not only our respiratory systems but also our culture.
Over time, Omicron’s unique characteristics will drive Americans to deny and ignore the risks of infection. In the near future, they’ll make decisions and take actions that they’d presently deem wrong.
A culture shock is coming
Culture—which comprises the shared values, norms and beliefs of a group of people—doesn’t change because someone decides it should. It evolves because circumstances change.
The pandemic has no doubt been a culture-changing event and, as the circumstances of Covid-19 have changed, so too have our underlying values, beliefs and behaviors.
If 100 million Americans (one-third of the population) were to become infected with Omicron this year, we can expect that everyone will know someone with the disease. And when dozens of our friends or colleagues say they’ve had it, we will begin to see transmission as inevitable. And since, statistically, most Americans won’t die from Omicron, people will see infection as relatively harmless and they’ll be willing to drop their guard.
We’ll see more and more people going to work even when they’re infected. We’ll see more people on trains and planes, coughing and congested, having never taken a Covid-19 test. And we’ll see large, indoor celebrations taking place without any added safety measures, despite the risks to the most vulnerable attendees.
Amid these changes, health officials will continue to urge caution, just as they have for more than two years. But it won’t make a difference. Culture eats science for breakfast. Americans will increasingly follow the herd and stop heeding public-safety warnings.
The process of change has begun
Cultural shifts happen in steps. First, a few people break the rules and then others follow.
Recall my friend, the one who took two tests out of an abundance of caution. Next time, perhaps he’ll decide he’d rather not miss the conference. Perhaps when he returns home, he will tell his friends that he felt sick the whole trip. Perhaps they’ll ask, “Do you think you might have had Covid?” And perhaps he will reply: “What difference would it have made? I’m fully vaccinated and boosted.”
And so, it will go. The next time someone in his social circle feels under the weather, he or she won’t even bother to do the first test.
This change process has already begun. Take the White House Correspondents’ Dinner, for example. Last year, the event was cancelled. This year, guests had to show proof of vaccination or a negative same-day test. However, that rule didn’t apply to staff at the hotel who worked the event. Unsurprisingly, several high-profile attendees got Covid-19 but, so far, no reports of anyone being hospitalized. A year from now, assuming no major mutations cause the virus to become more lethal, we can expect all restrictions will be dropped.
Culture dictates how people behave. It influences their thoughts and actions. It alters their values and beliefs. The unique characteristics of Omicron will lead people to ignore the harm it inflicts. They won’t act with malicious intent. They’ll just be oblivious to the consequences of their actions. That’s how culture works.
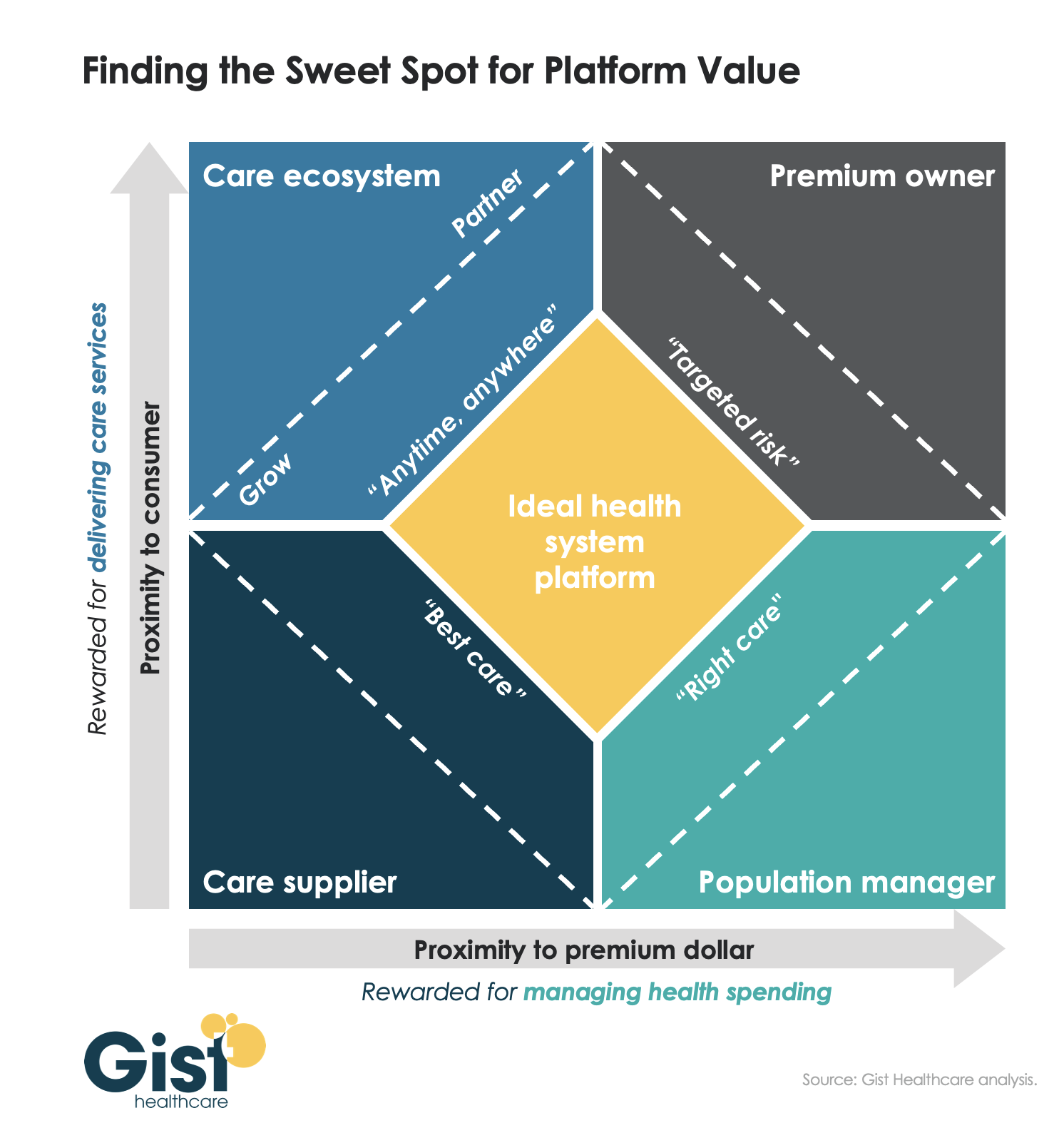
As we’ve been discussing over the past few years, several environmental forces—shifting consumer behavior, evolving demographics, new technology, and a flood of new market entrants—are pushing health systems to adopt a more consumer-centric business model. Systems must develop the capabilities needed to create an omnichannel consumer loyalty and population management platform. This platform will be the foundation for connecting consumers, curating providers, and coordinating care.
To achieve this vision, health systems must deliver value across two dimensions: increasing their proximity to the consumer (our y-axis) and their proximity to the premium dollar (our x-axis),as shown in the graphic above.Traditionally, health systems have operated primarily in the lower-left quadrant, as “care suppliers.” Some have spent considerable time and resources across the last decade, pushing closer to the premium dollar, to become “population managers.” But, importantly, managing population health is neither patient-facing, nor something consumers demand and seek.
To build deeper consumer loyalty, health systems must also move up the y-axis, creating a “care ecosystem” that provides “anywhere, anytime” care through multiple channels, including virtual and home-based solutions. And for certain populations, like Medicare Advantage, it will make sense for many systems to also explore becoming the “premium owner”, owning the full care budget and ensuring the incentives to design a consumer-centric offering.
The ideal health system platform should combine all four of these identities, tailored to the local market situation.
The momentum behind Medicare Advantage is only growing as more baby boomers age into eligibility, and experts don’t expect the energy around the program to slow down any time soon.
A recent analysis from the Kaiser Family Foundation found that a record 3,834 plans were available for the 2022 plan year in MA, which represents an 8% increase over 2021 and the largest number on the market in a decade.
Open enrollment for Medicare ended Dec. 7, and enrollment numbers will begin trickling out as the year winds down. In 2021, 26 million Medicare beneficiaries, or about 42% of those eligible for the program, were enrolled in an MA plan.
“As Medicare Advantage enrollment continues to grow, insurers seem to be responding by offering more plans and choices to the people on Medicare,” the KFF analysts said.
Part of the appeal of MA to an increasingly savvy consumer base is that it offers additional benefits beyond those afforded people in traditional Medicare, such as vision and dental coverage as well as supports for members’ social needs.
Sachin Jain, M.D., CEO of SCAN Health Plan, told Fierce Healthcare that people are increasingly shopping around for plans, building greater awareness of MA as a whole as well as of the different types of benefits beneficiaries could select.
“We’re seeing that consumers are more sophisticated today than they were a decade ago,” he said. “I think people are realizing that fee-for-service Medicare doesn’t cover a lot of things.”
The KFF report shows that more than 90% of non-group MA plans offer some kind of vision, hearing, telehealth or dental benefits and that most (89%) include prescription drug coverage as well.
Elena McFann, president of Medicare at Anthem, told Fierce Healthcare that throughout the open enrollment period, plans built with benefits that target the social determinants of health and promote whole-person care resonated strongly with members.
Anthem, for example, offers plans that include a slate of essential extra benefits that members can choose from based on what they need the most. Options include grocery cards, transportation benefits and in-home supports.
She said that the grocery benefits and flex cards that allow members to purchase additional hearing, vision and dental coverage have proven particularly popular in this enrollment season.
“What those all point to is the concept of flexibility and helping them lead healthier lives where they really need the help where they are in their journey,” McFann said.
As these benefits prove popular, an increasing number of plans are offering them in tandem. The Better Medicare Alliance released a survey late last month that found the number of plans including supplemental benefits grew by 43% for the 2022 plan year.
The Centers for Medicare & Medicaid Services (CMS) has issued additional flexibilities that allow MA plans to address members’ social determinants of health as the program’s enrollment continues to swell.
Jain said SCAN has seen similar interest in supplemental benefits, and that flexibility afforded to MA plans to adapt to seniors’ needs and expectations is a critical factor in the program’s success.
“When you’re in the business of serving seniors, a lot of what you have to do is anticipate needs that those seniors may not anticipate that they have, give them things they didn’t know they needed,” he said.
McFann said that beneficiaries value plans like these that unite brands they trust and recognize and that partners like Kroger enable insurers to more effectively meet seniors where they are. In its co-branded plans, members can access benefits like Healthy Grocery Cards and stipends to purchase over-the-counter health items.
She said that there has been significant “excitement” around those plans, which are available in four states, during the current enrollment period.
“It gives the Medicare eligibles a sense of familiarity and a sense of comfort, again meeting them on their terms,” McFann said.
However, while many established insurers have set ambitious growth targets in this market and new startups enter the space regularly, they still have plenty of work to do if they want to catch up with the market’s dominant forces: UnitedHealthcare, Humana and Blues plans.
UHC and Humana together account for 45% of the MA market in 2021, according to the KFF analysis. Humana offers plans in 85% of counties and UHC in 74% for 2022.
That means, 89% of Medicare eligibles have access to a Humana plan and 90% have access to a UHC MA plan if they choose, according to the report.
Competition is continuing to grow, though, and both McFann and Jain said they don’t feel the momentum around MA slowing down anytime soon.
“It is those extras and social drivers of health solutions that really have caught on with the Medicare-eligible segment and we expect to see that expand even further,” McFann said.
A recent piece in JAMA argues that policymakers need to be proactive in addressing how the rise of MA enrollment will affect the Medicare program as a whole, including its role in national quality and utilization measurement, rural healthcare access, and graduate medical education. The ability to monitor care delivered to the traditional, fee-for-service Medicare beneficiary population has been critical for assessing cost growth and shifting care patterns, distributing subsidies, and basing MA payments—all things that will become increasingly difficult as traditional Medicare becomes both smaller and less representative of the entire Medicare population.
The Gist: Traditional Medicare has been a springboard for national healthcare policy goals and industry-wide innovations. However, consumers’ preference for, and policy shifts supporting, the growth of Medicare Advantage are proving to be unstoppable.
Providers must prepare for a future in which a shrinking minority of beneficiaries are enrolled in traditional Medicare. If current trends continue, Medicare policymakers must bolster ongoing support for medical education, and build a higher standard of transparency and quality reporting for MA carriers and providers to maintain the sustainability of one of the country’s greatest healthcare data resources.
Only 10 days after a racially motivated mass shooting that killed 10 in a Buffalo, NY grocery store, 19 children and two teachers were murdered on Tuesday at an elementary school in Uvalde, TX. The Uvalde shooting was the 27th school shooting, and one of over 212 mass shootings, that have occurred this year alone.
Firearms recently overtook car accidents as the leading cause of childhood deaths in the US, and more than 45,000 Americans die from gun violence each year.
The Gist: Gun violence is, and has long been, a serious public health crisis in this country. It is both important to remember, yet difficult for some to accept, that many mass shootings are preventable.
Health systems, as stewards of health in their communities, can play a central role in preventing gun violence at its source, both by bolstering mental health services and advocating for the needed legislative actions—supported by a strong majority of American voters—to stem this public health crisis.
As Northwell Health CEO Michael Dowling said this week, “Our job is to save lives and prevent people from illness and death. Gun violence is not an issue on the outside—it’s a central public health issue for us. Every single hospital leader in the United States should be standing up and screaming about what an abomination this is. If you were hesitant about getting involved the day before…May 24 should have changed your perspective. It’s time.”