Inflation moderated as economists forecasted last month, according to the Federal Reserve’s favored inflation metric, bringing welcome news for investors, home buyers and consumers alike looking for interest rate cuts.
KEY FACTS
Americans spent 2.4% more in January than they did in January 2023, according to the personal consumption expenditures (PCE) price index released Thursday morning by the Bureau of Economic Analysis.
That meets consensus economist estimates of 2.4% annual PCE inflation and comes in lower than last month’s 2.6%.
It’s the lowest PCE reading since March 2021.
Core PCE inflation, which tracks expenditures for goods and services other than the less sticky food and services inputs, was 2.8% in January, in line with forecasts of 2.8%.
It’s similarly the lowest core PCE reading since March 2021 and checks in significantly lower than January 2023’s 4.7% inflation.
KEY BACKGROUND
Core PCE inflation, which is Fed Chairman Jerome Powell’s inflation measure of choice, is still well above the Fed’s long-term 2% target.
Earlier this month, PCE’s sister consumer price index (CPI)revealed far worse CPI inflation than economists projected, sending the S&P 500 stock index to its biggest loss in almost 12 months as sticky inflation would likely cause the Fed to delay the much-anticipated rate cuts until more tangible progress toward 2% inflation is apparent. CPI measures the average prices nationwide of a predetermined basket of goods and services, while PCE measures how much Americans actually spend monthly, earning the latter policymakers’ affection as it arguably paints a better picture of the health of Americans’ wallets.
The series of hotter than anticipated inflation data has dramatically pushed back expectations of when and by how much the Fed will slash rates in 2024. Higher inflation typically keeps rates higher for longer, making loans such as mortgages more expensive, exemplified by mortgage rates more than doubling over the last two years to their highest levels since the turn of the century.
The futures market currently prices in June as the most likely date of the first cut and 75 basis points of cuts as the most likely outcome, according to the CME Group’s FedWatch Tool, much softer than a month ago’s implied forecasts of the first reduction coming in May and 125 basis points of cuts.
STAT News today published an op-ed I coauthored with Dr. Philip Verhoef, president of Physicians for a National Health Program, making the point that investors are among the growing number of stakeholders who are souring on big, for-profit insurance companies like the ones I used to work for (Cigna and Humana).
We focused specifically on investors’ concerns about the continued profitability of Medicare Advantage plans most of the big insurers own and operate.
Several companies have lost billions of dollars in market capitalization over the past several weeks as they have reported what they maintain is higher than usual utilization of health care goods and services by seniors enrolled in MA plans.
Today, the companies–especially UnitedHealth Group, the market leader with 7.6 million Medicare Advantage enrollees–are losing billions more in market cap on the news, broke yesterday by the Wall Street Journal, that the Department of Justice is investigating UnitedHealth’s many acquisitions over the years.
UnitedHealth and most of the other companies are no longer just insurance companies. They’ve moved rapidly into health care delivery by buying physician practices and clinics, and three of them, UnitedHealth, Cigna and CVS/Aetna, control 80% of the pharmacy benefit management business.
Investors in MA insurance companies experienced a rude awakening in late January, with insurer stocks plummeting in the face of earnings reports showing profits falling far below expectations in the last quarter of 2023. Companies like CVS Health and UnitedHealth Group saw losses of 5.2% and 6.2% respectively, while Humana, whose business model relies heavily on the MA program, fell an astonishing 14.2%. These insurers cited higher than average health care utilization rates as the culprit and warned that 2024 would likely see more of the same. At the same time, private equity investment in MA has fallen, showing waning confidence in the program.
We went on to note that both Democrats and Republicans in Congress are increasingly concerned about MA insurers’ business practices and, among other things, have introduced bills to crack down on egregious overpayments to MA plans.
The WSJ reported yesterday that the Justice Department has launched an antitrust investigation into UnitedHealth, which has become not only the country’s biggest U.S. health insurer but also a leading manager of drug benefits “and a sprawling network of doctor groups.”
The investigators have in recent weeks been interviewing healthcare-industry representatives in sectors where UnitedHealth competes, including doctor groups, according to people with knowledge of the meetings.
The DOJ’s investigation of UnitedHealth is wide-ranging. Among other things, according to the Journal, “investigators have asked whether and how the tie-up between UnitedHealthcare [the insurance division] and Optum’s medical groups might affect its compliance with federal rules that cap how much a health-insurance company retains from the premiums it collects. (Optum is the company’s division that encompasses the pharmacy benefit manager Optum Rx and the many clinics and physician practices it owns.)
HEALTH CARE un-coveredexplained last month how UnitedHealth essentially is paying itself billions of dollars every month and circumventing the intent of a federal law that requires insurers to spend at least 80% of premium dollars on their health plan enrollees’ health care.
I know from sources within the Justice Department that investigators saw that piece, as well as the comprehensive analysis we published earlier of the scores of acquisitions UnitedHealth has made in recent years that have enabled it to catapult to the top five of the Fortune 500 list of American companies.
Those sources told me that the DOJ is very concerned about the consolidation within both the health insurance business and the hospital industry. Many U.S. hospitals, in an ongoing effort to negotiate from an enhanced position of strength with UnitedHealth and the other vertically integrated insurers, have merged with each other in recent years and become part of huge health-care delivery systems.
At the close of trading on the New York Stock Exchange yesterday, shares of UnitedHealth Group’s share were down $11.90 or 2.27%. Investors are continuing to head for the exits today. As I write this, the company’s stock price has fallen another $20 (4%) to $494.00. That’s way down from the company’s 52-week high of $554.70.
Shares of most of the other big publicly traded insurers (Centene, Cigna, CVS/Aetna, Elevance, Humana and Molina) are also down, ranging from $.83 at CVS to $11.51 at Humana.
Ruth Gottesman’s monumental $1 billion contribution to the Albert Einstein College of Medicine marks a groundbreaking moment, ensuring free tuition for both present and future students. David Begnaud delves into the significance of this generous gift and talks to a student directly impacted by this life-changing donation.
U.S. Hospital YTD Operating Margin Index November 2021-December 2023
The observations and questions from this chart are both interesting and required reading for hospital executives:
Why were hospitals profitable at the 4% plus level through the worst of the 2021 Covid period?
What exactly happened between December of 2021 and January of 2022 that resulted in a profitability decrease from a positive 4.2% to a negative 3.4%?
Despite the best efforts of hospital executives, overall operating margins were negative throughout calendar year 2022 and did not return to positive territory until March of 2023.
Hospital margins remained positive throughout 2023 and into 2024. However, overall margins have remained below those experienced in both 2021 and in the pre-Covid year of 2019.
The above questions and observations have proven interesting, and the ongoing numbers have proven quite useful in many quarters of healthcare. But recently I was talking with Erik Swanson, who is the leader of the Kaufman Hall Flash Report and our executive behind the data, numbers, and statistics. Erik and I were speculating about all of the above observations, but our key speculation was whether the 2023 operating margin results actually reflected a hospital financial turnaround or, in fact, were there “numbers behind the numbers” that told a different and much more nuanced story. So Erik and I asked different questions and took a much deeper dive into the Flash Report numbers. The results of that dive were quite telling:
Too many hospitals are still losing money. Despite the fact that the Operating Margin Index median for 2023 and into 2024 was over 2%, when you look harder at the Flash Report data, you find that 40% of American hospitals continue to lose money from operations into 2024.
There is a group of hospitals that have substantially recovered financially. Interestingly, the data shows over time that the high-performing hospitals in the country are doing better and better. They are effectively pulling away from the pack.
This leads to the key question: Why are high-performing hospitals doing better? It turns out that several key strategic and managerial moves are responsible for high-performing hospitals’ better and growing operating profitability:
Outpatient revenue. Hospitals with higher and accelerating outpatient revenue were, in general, more profitable.
Contract labor. Hospitals that have lowered their percentage of contract labor most quickly are now showing better operating profitability.
An important managerial fact.The Flash Report found that hospitals with aggressive reductions in contract labor were also correlated to rising wage rates for full-time employees. In other words, rising wage rates have appeared to attract and retain full-time staff which, in turn, has allowed those hospitals to reduce contract labor more quickly, all of which has led to higher profitability.
Average length of stay.No surprise here. A lower average length of stay is correlated to improved profitability. Those hospitals that have hyper-focused on patient throughput, which has led to appropriate and prompt patient discharge, have also proven this to be a positive financial strategy.
Lower financial performers have financially stagnated throughout the pandemic. The data shows that throughout the pandemic, hospitals with good financial results improved those results, but of more consequence, hospitals with poor financial performance saw that performance worsen. The Flash Report documents that the poorest financially performing hospitals currently show negative operating margins ranging from negative 4% to negative 19%. Continuation of this level of financial performance is not only unstainable but also makes crucial re-investment in community healthcare impossible.
The urban hospital/rural hospital myth. A popular and often quoted hospital comparison is that there is an observable financial divide between urban and rural hospitals. Erik Swanson and I found that recent data does not support this common perception. When you compare “all rurals” to “all urbans” on the basis of average operating margin, no statistically significant difference emerges. However, what does emerge—and is a very important statistical observation—is that the lowest performing 20% of rural hospitals are, in fact, generating much lower margins then their urban counterparts this year. It is at this lowest level of rural hospital performance where the real damage is being done.
Rural hospitals and obstetrics. The data does confirm one very important American healthcare issue: Obstetrics and delivery services are one of the leading money losers of all hospital service offerings. And the data further confirms that rural hospitals are closing obstetric departments with more frequency in order to protect the financial viability of the overall rural hospital enterprise. This is a health policy issue of major and growing consequence.
The point here is that data, numbers, and statistics matter both to setting long-term social health policy agendas and to the strategic management of complex provider organizations. But the other point is that the quality and depth of the analysis is an equally important part of the process. A first glance at the numbers may suggest one set of outcomes. However, a deeper, more careful and penetrating analysis may reveal critical quantitative conclusions that are much more telling and sophisticated and can accurately guide first-class organizational decision-making. Hopefully the analytics here are a good example of this very point.
Walgreens announced this week that it will be shutting down all of its Florida-based VillageMD primary care clinics. Fourteen clinics in the Sunshine State have already closed, with the remaining 38 expected to follow by March 15.
This move comes in the wake of a $1B cost-cutting initiative announced by Walgreens executives last fall, which included plans to shutter at least 60 VillageMD clinics across five markets in 2024.
Last month VillageMD exited the Indiana market, where it was operating a dozen clinics.
Despite downsizing its primary-care footprint, Walgreens says it remains committed to its expansion into the healthcare delivery sector, having invested $5.2B in VillageMD in 2021 and purchased Summit Health-CityMD for $9B through VillageMD in 2023.
The Gist:Having made significant investments in provider assets, Walgreens now faces the difficult task of creating an integrated and sustainable healthcare delivery model, which takes time.
Unlike long-established healthcare providers who feel more loyal to serving their local communities, nontraditional healthcare providers like Walgreens can more easily pick and choose markets based on profitability.
While this move is disruptive to VillageMD patients in Florida and the other markets it’s exiting, Walgreens seems to be answering to its investors, who have been dissatisfied with its recent earnings.
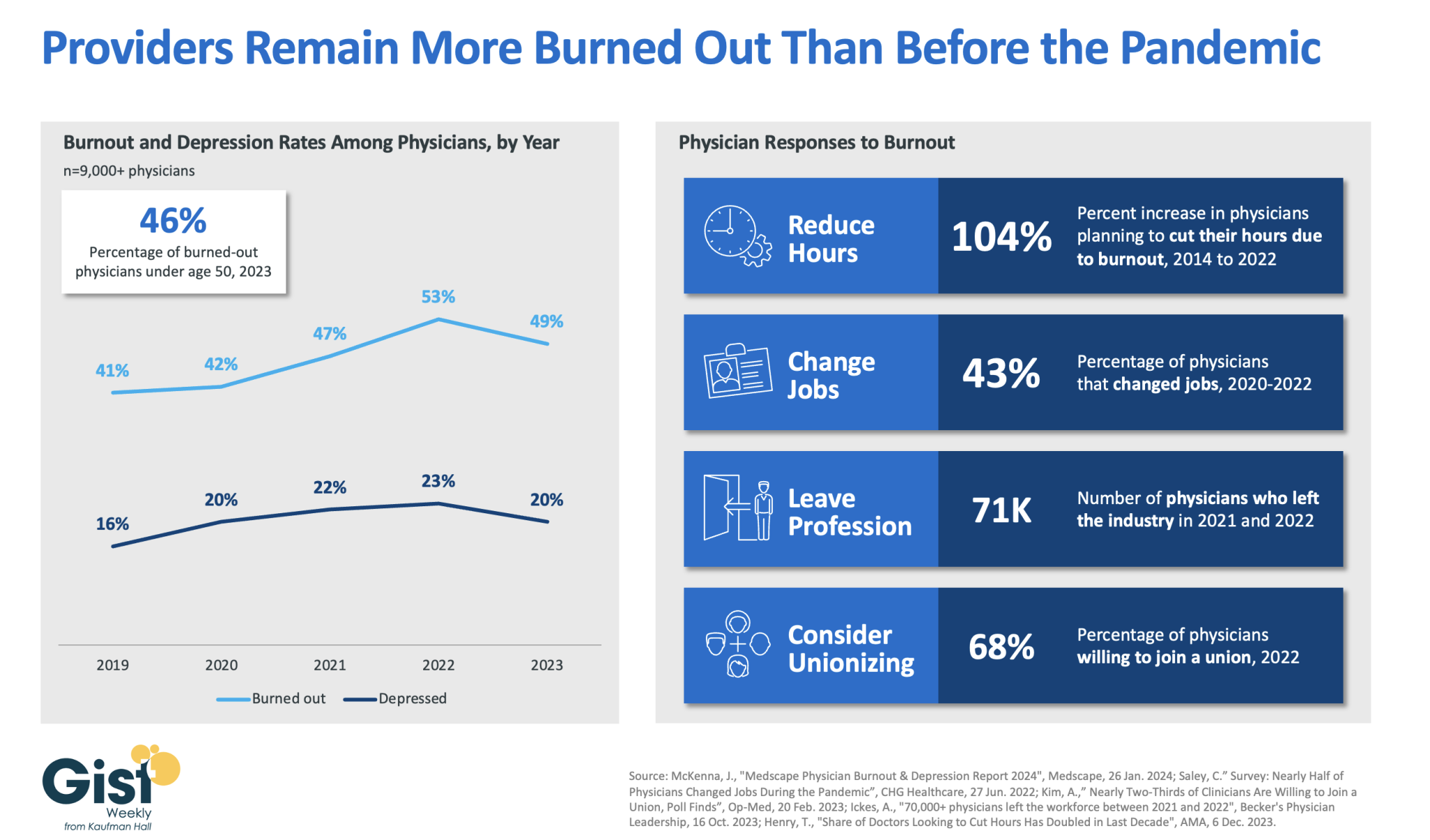
In 2023, nearly half of physicians reported feeling burned out, and a fifth reported feeling depressed. Although this does represent a drop from 2022’s peak, physicians remain more distressed than they were before the pandemic.
These numbers reveal some of the toll that the continued labor shortages, financial challenges, and payment changes of the past few years have taken on providers. In response to feeling burned out, an increased number of physicians say they are planning to cut their hours and over a third say they actually have changed jobs. Many have left the industry all together and the majority now say they are willing to join a union.
Health systems have long prioritized addressing provider burnout, but tighter operating margins have heightened both the challenge and the importance of helping to relieve it.
Continuing to find solutions to reduce administrative tasks, enhance team-based care models, and empower providers in decision-making processes are as important as ever for provider organizations today.
“I know that I have less to live than I have lived.
I feel like a child who was given a box of chocolates. He enjoys eating it, and when he sees that there is not much left, he starts to eat them with a special taste.
I have no time for endless lectures on public laws – nothing will change. And there is no desire to argue with fools who do not act according to their age. And there’s no time to battle the gray. I don’t attend meetings where egos are inflated and I can’t stand manipulators.
I am disturbed by envious people who try to vilify the most capable to grab their positions, talents and achievements.
I have too little time to discuss headlines – my soul is in a hurry.
Too few candies left in the box.
I’m interested in human people. People who laugh at their mistakes are those who are successful, who understand their calling and don’t hide from responsibility. Who defends human dignity and wants to be on the side of truth, justice, righteousness. This is what living is for.
I want to surround myself with people who know how to touch the hearts of others. Who, through the blows of fate, was able to rise and maintain the softness of the soul.
Yes, I hustle, I hustle to live with the intensity that only maturity can give. I’ll eat all the candy I have left – they’ll taste better than the ones I already ate.
My goal is to reach the end in harmony with myself, my loved ones and my conscience.
I thought I had two lives, but it turned out to be only one, and it needs to be lived with dignity.”
Brilliant Anthony Hopkins
and free interpretation of Mario de Andrade’s poem
At a recent dinner with my good friend and colleague Dave Blom, the former President and CEO of Ohio Health, he and I discussed the difficulties of leading and managing complex healthcare organizations in the post-Covid era.
We agreed that the leadership issues that matter most right now center around the ability of executives to possess and demonstrate an authentic emotional IQ.
Taking care of patients—in fact, taking care of communities—is not only managerially complicated but also emotionally testing.
Success cannot be achieved by technical and clinical excellence alone; rather, it must be built on a platform of an emotional IQ that is supported, valued, and shared by the entire organization.
The below list is what Dave and I settled on as the most important elements of emotional IQ for healthcare leaders today, and we think that leadership teams thatfully embrace these behaviors unlock a higher level of organizational trust, as well as corporate and managerial integrity.
–Empathy.
A leader needs to understand and share the feelings of his or her entire organization, as well as understand the difference between sympathy and empathy: sympathy is a passive emotion while empathy is an active emotion. A leader with empathy not only notes the problem but immediately moves to be of help at either the personal or organizational level, whichever is required.
–Vulnerability.
Historically, executive leadership, especially in corporate situations, has been trained and encouraged not to show emotion or weakness. But organizations are changing, and the composition of the today’s workforce is different. The patient care process is emotional in and of itself, and daily operational interactions demand a different kind of leadership—a leadership that is comfortable with both emotion and weakness.
–Humility.
Executives who show humility are willing to ask for help, and don’t insist on everything being done their way; they are quick to forgive and are known for their patience. Humility supports a collaborative and cooperative leadership model, which has at its core a heavy dose of decentralization and delegation.
On Tuesday, the Centers for Medicare and Medicaid Services (CMS) published a final rule redefining how disproportionate share hospital (DSH) payments are determined.
Hospitals used to calculate their Medicaid shortfalls based on the costs and payments associated with all of their Medicaid-eligible patients, even if some of those patients used a different primary payer. Prompted by Congress to address this issue in 2021, CMS is now limiting the scope of Medicaid shortfall to only patients for whom Medicaid is their primary payer. The rule exempts safety-net hospitals providing care to the highest percentages of low-income patients, defined as those in the 97th percentile of inpatient days treating Medicare SSI (Social Security Income) recipients.
This change is expected to amount to an $8B annual reduction in DSH payments over the next four years. Congress has repeatedly delayed the implementation of these cuts, which are now set to go in effect on March 8, 2024.
The Gist: Though the formula for calculating appropriate DSH payments has always been complex, the point of the program is to provide additional support to hospitals caring for underserved, low-income populations.
This $8B cut may be targeted at hospitals with slightly better payer mixes, but it will be felt heavily by many safety-net providers reliant on the payments, especially in today’s challenging financial operating environment where over 40 percent of hospitals are still losing money on operations.