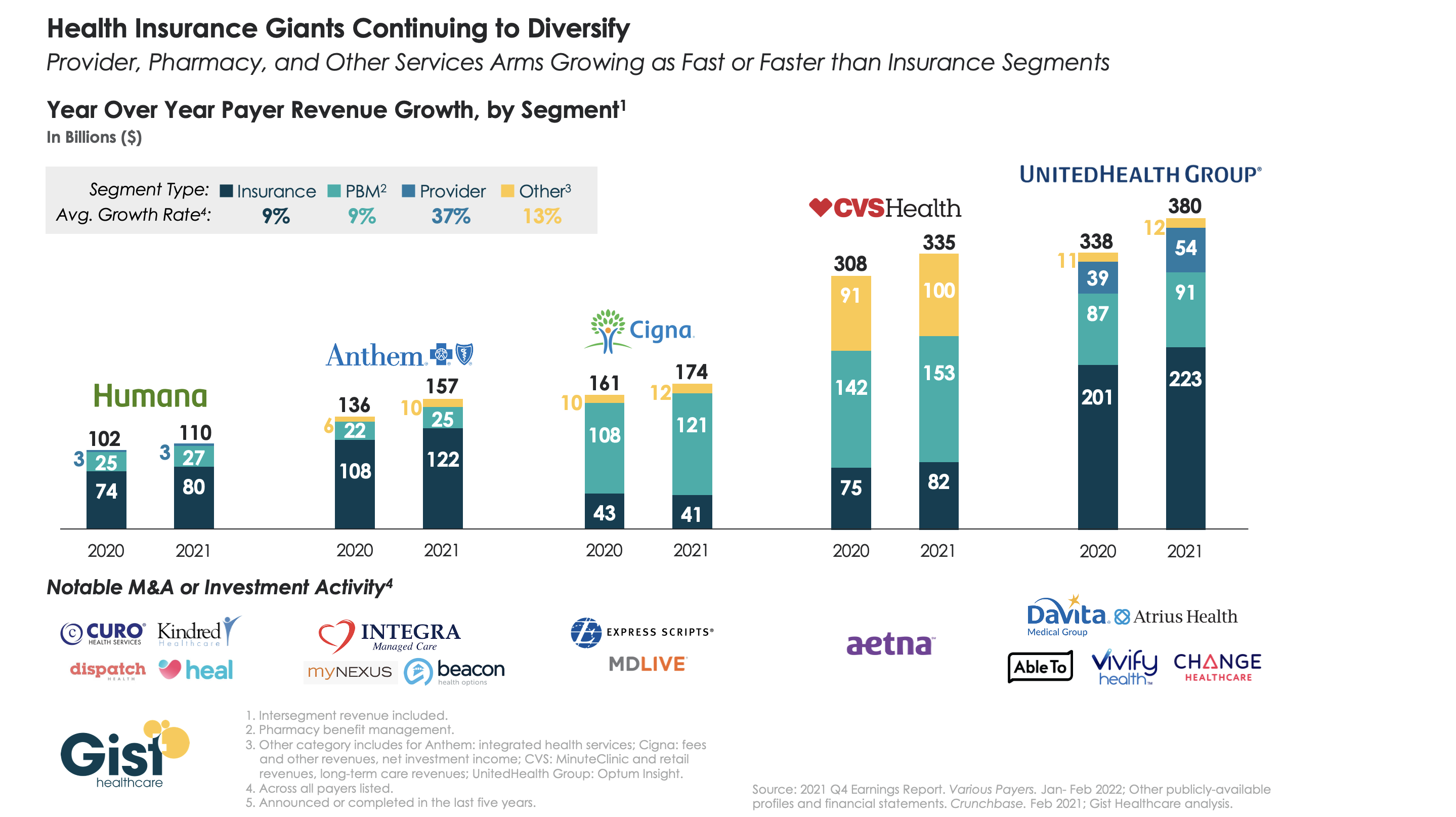
The largest health insurers are quickly becoming vertically integrated healthcare organizations that span the care and coverage continuum. While 2021 was a mixed year for these companies as healthcare volumes bounced back, their diversified portfolios helped cushion losses from higher claims.
The graphic above analyzes revenue growth by segment for the five largest insurers across the last two years. On averagethe insurance and pharmacy benefit management components of the companies grew at nine percent, while care delivery and integrated health services grew at much higher rates. UnitedHealth Group (UHG) and Anthem boasted the highest year-over-year revenue growth, driven by UHG’s Optum subsidiary and Anthem’s integrated health services.
Cigna and CVS Health each earned less than a quarter of their total revenue from their insurance arms lastyear. While Humana lags the others in topline revenue, it has assembled a robust portfolio of care delivery investments and partnerships, surpassed only by UHG.
As antitrust scrutiny on vertical integration increases (case in point: the DOJ is now challenging UHG’s acquisition of Change Healthcare), insurers will face the hard task of integrating their portfolio of service—and demonstrating that they deliver value to consumers and patients.
A recent New Yorker article details the history of the American Medical Association’s (AMA) opposition to single-payer healthcare, and the grassroots movement that nearly changed its position in 2019.
Since its founding in the 1840s, the largest association of the nation’s doctors has wielded significant influence over healthcare policy, and has been the most effective opponent of several waves of progressive healthcare reform proposals across the last century. More recent changes in the demographic makeup of its physician constituents have begun to mirror the US population. A quarter of today’s practicing physicians graduated from foreign medical schools, and gender and racial gaps in medical schools have been reduced. Today, half of medical students are female, and half are people of color.
The Gist: The perspectives, needs, and politics of the physician community are changing. Younger physicians tend to be more left-leaning, and more are employees, rather than entrepreneurial business owners. While physician pocketbook issues historically dominated the AMA’s policy positions, today’s younger physicians are increasingly motivated by social justice concerns, leading to advocacy positions that would have been unimaginable a few decades ago.
Physician societies continue to move closer to endorsing more extensive healthcare reform policies, over trying to ensure economic protection for the profession—and in the long run, this shift in physician support could prove a key driver in increasing public approval of “Medicare for All” and other coverage reforms.
The February 14th deadline for healthcare workers to receive their first dose of the COVID vaccine does not appear to have significantly worsened the hospital staffing crisis, even in rural hospitals. But the mandate hasn’t necessarily meant that all healthcare workers are now vaccinated, as some hospitals reported approving a flurry of medical and religious exemptions to avoid staff departures.
The Gist: Just as when states and early-adopter health systems enforced healthcare worker vaccine mandates last year, COVID vaccine uptake jumped just ahead of the federal deadline.
After months of challenges, we may finally be moving beyond debates over healthcare worker vaccine requirements. And as hospitalizations from the Omicron wave continue to decline, most states and health systems are not planning to implement booster requirements.
DOJ alleges that allowing UHG’s Optum subsidiary to acquire Change, a direct competitor used by most large commercial insurers for healthcare claims solutions, would give UHG 75 percent of the healthcare claims processing and management market. This would significantly reduce competition, the DOJ claims, while simultaneously giving UHG access to its competitors’ sensitive plan design and pricing information. UHG called the DOJ’s position ‘deeply flawed’ and promised to fight the case.
The Gist: This is the second big move by antitrust regulators in a week to put the brakes on consolidation in healthcare: shortly after the DOJ sued to block Rhode Island’s two largest health systems, Care New England and Lifespan, from merging, those systems abandoned plans to combine.
We are seeing the first real signs that the Biden administration is following through on plans to more closely scrutinize healthcare deals, including payer-led vertical integration. For both payers and providers, increased scrutiny will place a premium on the consumer value proposition of any combination—and force merging companies to deliver on the benefits of scale.
On Thursday CMS announced it will replace all versions of its Global and Professional Direct Contracting (GPDC) model, which allowed primary care providers to take full or partial risk on managing cost of care for traditional Medicare beneficiaries, after progressive Democrats raised concerns about whether a growing presence of Medicare Advantage insurers and private equity-backed groups in the model might compromise patient care and access in the traditional Medicare program. GPDC will be replaced with a new three-year demonstration called Accountable Care Organization Realizing Equity, Access and Community Health (ACO REACH), to start enrollment in 2023. The 51 current participants in the GPDC model can move into ACO REACH as long as they meet new requirements, which include developing plans to identify and address health disparities, and ensuring providers control three quarters of governing boards (as compared to a quarter in the GPDC model). Private equity and insurer applicants can still apply, but must demonstrate a track record of direct patient care, delivering quality outcomes, and serving vulnerable populations.
The Gist: ACO REACH is largely a “re-skinning” of the Direct Contracting program, rather than a significant overhaul. Physician, health system, and ACO groups, who were concerned that the program would be canceled altogether, were pleased with the announced changes to the model, although debate continues on whether the new guardrails will effectively address concerns around for-profit insurer and investor participation.
Like Direct Contracting before it, ACO REACH will be an important vehicle for risk-ready providers to move more extensively into full-risk contracting, without launching a plan or partnering directly with a MA insurer.
Healthcare professionals in Oklahoma who have cared for COVID-19 patients throughout the pandemic are now facing a facility lockdown due to threats made against them.
Mercy Hospital Oklahoma City upped its security and locked down its intensive care unit following online threats against the facility and its staff, mostly revolving around COVID treatments and conspiracy theories, Becker’s Hospital Review reported.
Claims made during a recent protest outside the facility and online included that the hospital had a “Fauci protocol,” and that it received government vouchers for using certain medications or treatments for COVID patients, which Mercy Hospital denied, according to Becker’s.
Hospital officials released a statement to staff on Friday, which they shared with MedPage Today. “There is truly nothing more important to us than your safety. We have a team monitoring these online attacks in real time. Every level of our ministry is deeply concerned and committed to doing whatever it takes to protect our co-workers against these baseless attacks,” they said.
“We are proud to serve with you,” they added. “We know you are tired and weary, but please try your best to put these baseless claims out of your mind. Remember, you are called to serve our patients and each other. We are praying for peace and protection over each of you, as well as the protection of all our patients and visitors, while we take action on your behalf.”
Late last week, the hospital filed a restraining order against the founder and director of an Oklahoma church group that has been protesting outside the facility and making threats against its staff online, Oklahoma’s KFOR reported.
In a recent press release, the church group, known as Ekklesia Oklahoma, called Mercy Hospital an “evil Marxist controlled death camp.”
Court documents stated that the founder of the group called one of the hospital’s doctors a “murderer,” noting that members even posted the doctor’s home address online, according to KFOR.
Hospital officials told KFOR that they are thankful for local police departments that are providing extra security for staff and patients.
Other hospitals across the U.S. have also received threats to the safety of healthcare workers in recent days.
Last week, the Massachusetts Medical Society said it was “angered” over the recent neo-Nazi protest outside Brigham and Women’s Hospital in Boston that targeted two doctors whose work focuses on health equity.
Carole Allen, MD, MBA, president of the society, told MedPage Today that the protest outside Brigham and Women’s was a threat to healthcare workers who were just trying to do their jobs, as well as to patients, and was so disruptive that it “could endanger healthcare in general.”
The website for the group Physicians for Informed Consent (PIC) reads like an apolitical, educational resource that provides information on vaccines and why they shouldn’t be government-mandated. Its mission is “that doctors and the public are able to evaluate the data on infectious diseases and vaccines objectively, and voluntarily engage in informed decision-making about vaccination.”
The group’s accompanying social media accounts, however, tell a different story. On PIC’s Facebook, Twitter, Instagram, and LinkedIn feeds, you’ll find post after post about reasons to be scared of vaccines – especially for children – often highlighting selective portions of scientific research that contain vaccination risks.
Who’s Behind PIC?
The group was founded in 2015 after California passed a law that prohibited the use of personal belief exemptions from vaccinations required for children to attend any public or private school in the state.
Three years later, the number of waivers issued by doctors to parents seeking medical exemptions for their children tripled. As a result, another law was passed in 2019, cracking down on the inappropriate use of medical exemptions.
The group’s founder, Shira Miller, MD, is a concierge integrative medicine doctor based in Los Angeles, specializing in menopausal care. On her own Twitter profile, she describes herself as “Facebook’s Most Popular Menopause Doctor.”
Miller earned her medical degree in 2002 from Technion-Israel Institute of Technology in Haifa, Israel, and has reportedly been working as a concierge physician since 2010.
PIC’s leadership team also includes 20 physicians from a wide range of specialties, most of whom, like Miller, don’t specialize in infectious diseases.
Among its leaders is Paul Thomas, MD, an Oregon-based pediatrician. Thomas, who is listed as one of PIC’s founding directors, was issued an emergency suspension order of his medical license in 2021 by the state medical board, in which they cited at least eight cases of alleged patient harm. In line with PIC’s philosophy, Thomas maintains that he isn’t “anti-vax” – he’s pro-informed-consent.
Also on the team is Jane Orient, MD, internist and executive director of the Association of American Physicians and Surgeons (AAPS), a group that also opposes vaccine mandates. Orient received her medical degree from Columbia University and currently practices in Arizona. In 2020, the AAPS sued the federal government for withholding its stockpile of hydroxychloroquine from COVID patients, despite research showing that the drug is ineffective. The complaint was dismissed in September 2021.
Doug Mackenzie, MD, a plastic surgeon who graduated from Johns Hopkins University of Medicine, is PIC’s treasurer. He has previously identified himself as an “ex-vaxxer” rather than an anti-vaxxer when speaking on a panel in 2019.
The only RN on the team is Tawny Buettner. After California mandated vaccinations for healthcare workers, Buettner organized a protest outside of her place of work, Rady Children’s Hospital in San Diego; she later sued the hospital after she was dismissed from her job. According to the complaint, Buettner and the 36 other plaintiffs alleged that their requests for religious exemptions from the COVID-19 vaccine were all denied.
Kenneth Stoller, MD, also listed on the leadership team, graduated from the American University of the Caribbean School of Medicine and completed pediatric residency training at the University of California Los Angeles. Stoller was disciplined in 2019 for doling out medical exemptions to children without adequate evidence. According to state records, his license in California has since been revoked; he currently holds a medical license in New Mexico.
What’s PIC?
The most notable physician groups accused of spreading COVID-19 misinformation since the vaccine rollout have been affiliated with right-wing media, if not overtly proclaiming conservative, anti-vaccination beliefs.
For example,America’s Frontline Doctors, a group notorious for its support of hydroxychloroquine as a treatment for COVID-19, has made its values well-known. The group’s founder, Simone Gold, MD, JD, was arrested for participating in the Jan. 6 capitol riot and has openly opposed mask-wearing. Similarly, physician leaders of theFront Line COVID-19 Critical Care Alliance, known for promoting the use of ivermectin to treat COVID-19, tout their appearances on the ultra-conservative Newsmax on the website’s homepage.
PIC wants to be different. The group’s focus, according to its general counsel Greg Glaser, JD, of Copperopolis, California, is on the “authoritative citations that show, or calculate, the risks [of vaccines] to the public,” he told MedPage Today.
“We are pro-informed consent, pro-ethics, pro-health. PIC is not anti-vaccine, and PIC is not pro-vaccine – PIC is neutral,” Glaser said on behalf of the group.
In August 2021, Glaser submitted an amicus brief to the Supreme Court PIC’s behalf, arguing against the implementation of vaccine mandates. The document claims that “government statements confirm there is no evidence that COVID-19 vaccines prevent the spread of SARS-CoV-2 or COVID-19,” ignoring the breadth of existing literature that says otherwise.
Two nurses and a licensed physical therapist (PT) originally from the Philippines have filed a proposed class action lawsuit against an Ohio staffing firm, claiming its contracts and practices amount to trafficking and fraud, among other allegations.
The lawsuit claims that Cincinnati-based Health Carousel, which recruits and hires healthcare workers primarily from the Philippines to work in the U.S., employs its workers in “essentially indentured servitude.”
“Health Carousel mandates that its workers not leave the company for years unless they pay the company tens of thousands of dollars,” a complaint filed on behalf of Novie Carmen, RN, Kersteen Flores, RN, and licensed PT Jerlin Amistoso states. “And the company follows through on its threats by suing workers who dare to leave anyway.”
Earlier this month, a Bloomberg investigation first shed light on the case and Carmen, the original nurse behind it.
“I was basically trapped,” Carmen told Bloomberg. “Duped.”
According to the Bloomberg report, Carmen borrowed money from her boyfriend to help pay the $20,000 “quitting fee” and break ties with Health Carousel.
Carmen, Flores, and Amistoso now claim in their lawsuit that Health Carousel knows its workers must partake in lengthy orientation sessions and work overtime, but that the company doesn’t count those hours toward their required commitment period. The lawsuit adds that, “to make these workers feel even more vulnerable,” Health Carousel isolates them and prohibits them from discussing their pay and working conditions with others.
According to the complaint, Health Carousel maintains its scheme through defrauding the federal government, which approves its visa petitions without knowing it routinely fails to pay workers the wage it promises, and defrauding the workers themselves — who are unexpectedly subject to harsh employment terms, difficult workplace conditions, long work requirements, and stringent rules.
The complaint adds that Health Carousel continues to profit from its alleged scheme because healthcare facilities at which workers are placed pay the company more than what it pays its workers, and the company recoups even more money from workers who leave before the company determines they have completed their commitment period.
The lawsuit seeks to end what it claims are Health Carousel’s illegal practices and to compensate victims through forced labor claims under federal and state law, claims under the Racketeer Influenced and Corrupt Organizations Act and Ohio’s Corrupt Practices Act, and claims under the Fair Labor Standards Act.
Ultimately, Carmen, Flores, and Amistoso allege their circumstances aren’t unique. The Cincinnati Enquirer reported that at least 20 nurses in Pennsylvania alone, where Carmen was placed at a hospital by Health Carousel in 2018, have paid high financial penalties in recent years, according to the lawsuit.
Of Health Carousel, the Enquirer reported that the staffing firm has made the Deloitte Cincinnati 100 list of the region’s largest privately held companies for the past 5 years. “In the latest ranking, the company dropped from 39 to 45 on the list, reporting a revenue of $288 million in 2020,” the Enquirer wrote. “It hauled in $301 million in 2019.”
Legal counsel for Carmen, Flores, and Amistoso did not immediately provide additional comment on the case.
A spokesperson for Health Carousel, which has denied the allegations against it in court documents, told MedPage Today in an email that, “Unfortunately, we cannot comment on the specifics of ongoing litigation, but we are confident we will be successful in this matter.”
The spokesperson also pointed to a statement posted on the company’s website that includes the following: “For our part, ensuring the health, safety and well-being of every one of our nurses is the core of our business. To imply otherwise, based on activists intent on exploiting and twisting the experiences of a few, is disheartening and damaging. But more than that, it is simply inaccurate and a grave insult to the millions of people worldwide who continue to be victimized by traffickers.”
The company also posted a list of answers to frequently asked questions, one of which includes information on why nurses have to reimburse expenses when they break a contract. To that end, Health Carousel states in part that, “Requiring repayment of invested expenses and other damages if an employee does not fulfill a service obligation is not a ‘quitting fee’ or a penalty. Rather, it is a customary, reasonable and fair practice that many employers use in a range of industries and occupations to recoup investment in tuition reimbursement, relocation expenses, signing bonuses and more.”
Health Carousel added that the expenses it expects healthcare professionals to reimburse should they not complete their contracts “approximates or underestimates” its upfront investment on their behalf. “For example, when healthcare professionals do not complete the commitment period in the contract, the nurse retains his or her permanent resident visa to work in the United States, but Health Carousel suffers a financial loss because it cannot earn back the money it had advanced for their recruitment, credentialing, sponsorship, relocation and resettlement, and employment,” the company stated.
The cost of an ambulance ride has soared over the past five years, according to a report from FAIR Health, shared first with Axios.
Why it matters: Patients typically have little ability to choose their ambulance provider, and often find themselves on the hook for hundreds, if not thousands of dollars.
The details: Most ambulance trips billed insurers for “advanced life support,” according to FAIR Health’s analysis.
Private insurers’ average payment for those rides jumped by 56% between 2017 and 2020 — from $486 to $758.
Ambulance operators’ sticker prices, before accounting for discounts negotiated with insurers, have risen 22% over the same period, and are now over $1,200.
Medicare, however, kept its payments in check: Its average reimbursement for advanced life support ambulance rides increased by just 5%, from $441 to $463.
Between the lines: Ambulances aren’t covered by the new law that bans most surprise medical bills, meaning patients are still on the hook in payment disputes between insurers and ambulance operators.
State of play: Ground ambulances are operated by local fire departments, private companies, hospitals and other providers and paid for in a variety of ways, which makes this a tricky issue to address, according to the Commonwealth Fund.
Some states — such as Colorado, Delaware, Florida, Illinois, Maine, Maryland, New York, Ohio, Vermont and West Virginia — have protections against surprise ground ambulance billing, a columnist in the Deseret News pointed out earlier this year.
But in California, Florida, Colorado, Texas, Illinois, Washington state and Wisconsin, more than two-thirds of emergency ambulance rides included an out-of-network charge for ambulance-related services that posed a surprise bill risk in 2018, according to a Peterson-KFF Health System Tracker brief.
The bottom line: Costs for ground ambulance care are on the rise and, with few balance billing protections, that means patients could still be hit with some big surprises if they wind up needing a ride in an ambulance.