

Importance of Good Discussions



One hesitates to elevate obviously bad arguments, even to point out how bad they are. This is a conundrum that comes up a lot these days, as members of the media measure the utility of reporting on bad faith, disingenuous or simply bizarre claims.
If someone were to insist, for example, that they were not going to get the coronavirus vaccine solely to spite the political left, should that claim be elevated? Can we simply point out how deranged it is to refuse a vaccine that will almost certainly end an international pandemic simply because people with whom you disagree think that maybe this is a good route to end that pandemic? If someone were to write such a thing at some attention-thirsty website, we certainly wouldn’t want to link to it, leaving our own readers having to figure out where it might be found should they choose to do so.
In this case, it’s worth elevating this argument (which, to be clear, is actually floating out there) to point out one of the myriad ways in which the effort to vaccinate as many adults as possible has become interlaced with partisan politics. As the weeks pass and demand for the vaccine has tapered off, the gap between Democratic and Republican interest in being vaccinated seems to be widening — meaning that the end to the pandemic is likely to move that much further into the future.
Consider, for example, the rate of completed vaccinations by county, according to data compiled by CovidActNow. You can see a slight correlation between how a county voted in 2020 — the horizontal axis — and the density of completed vaccinations, shown on the vertical. There’s a greater density of completed vaccinations on the left side of the graph than on the right.
If we shift to the percentage of the population that’s received even one dose of the vaccine, the effect is much more obvious.
This is a relatively recent development. At the beginning of the month, the density of the population that had received only one dose resulted in a graph that looked much like the current density of completed doses.
If we animate those two graphs, the effect is obvious. In the past few weeks, the density of first doses has increased much faster in more-Democratic counties.

If we group the results of the 2020 presidential contest into 20-point buckets, the pattern is again obvious.

It’s not a new observation that Republicans are less willing to get the vaccine; we’ve reported on it repeatedly. What’s relatively new is how that hesitance is showing up in the actual vaccination data.
A Post-ABC News poll released on Monday showed that this response to the vaccine holds even when considering age groups. We’ve known for a while that older Americans, who are more at risk from the virus, have been more likely to seek the vaccine. But even among seniors, Republicans are significantly more hesitant to receive the vaccine than are Democrats.
This is a particularly dangerous example of partisanship. People 65 or older have made up 14 percent of coronavirus infections, according to federal data, but 81 percent of deaths. That’s among those for whom ages are known, a subset (though a large majority) of overall cases. While about 1.8 percent of that overall group has died, the figure for those aged 65 and over is above 10 percent.
As vaccines have been rolled out across the country, you can see how more-heavily-blue counties have a higher density of vaccinations in many states.
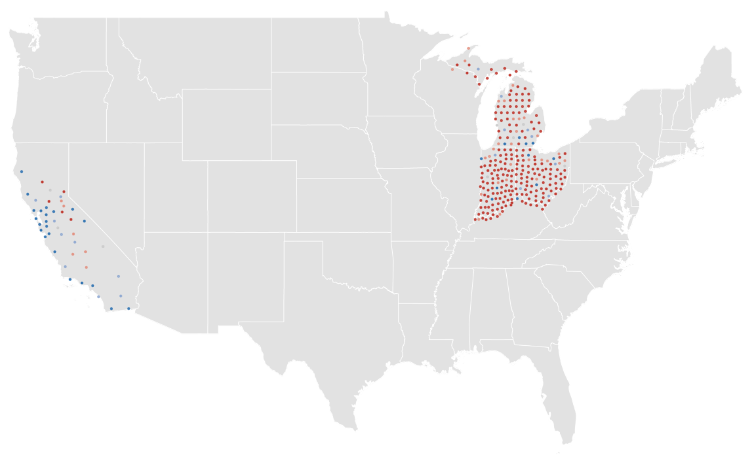
This is not a universal truth, of course. Some heavily Republican counties have above-average vaccination rates. (About 40 percent of counties that preferred former president Donald Trump last year are above the average in the CovidActNow data. The rate among Democratic counties is closer to 80 percent.) But it is the case that there is a correlation between how a county voted and how many of its residents have been vaccinated. It is also the case that the gap between red and blue counties is widening.
Given all of that, it probably makes sense to point out that an argument against vaccines based on nothing more than “lol libs will hate this” is an embarrassing argument to make.

The pandemic won’t end for anyone until it ends for everyone. That sentiment has been repeated so many times, by so many people, it’s easy to forget it’s not just a cliche—particularly if you live in one of the wealthy countries, like the U.S. and Israel, that has made significant moves toward what feels like an end to the COVID-19 era.
Israel, for example, has fully vaccinated more than half of its population and about 90% of its adults 50 and older are now immune to the virus—enough that the country is “busting loose” and “partying like it’s 2019,” as the Washington Post put it last week. The U.S. is a bit further behind, with nearly 30% of its population fully vaccinated, but the possibility of a post-pandemic reality is already coming into focus. While daily case counts remain high, they are far lower than they were even a few months ago—about 32,000 diagnoses were reported on April 25, compared to daily tallies well above 250,000 in January. Deaths have also trended downward for most of 2021. The U.S. Centers for Disease Control and Prevention has relaxed its guidance on travel and indoor gatherings, and some states have repealed mask mandates and other disease precautions.
But while people in certain affluent countries celebrate a return to vacations and parties, COVID-19 remains a dire threat in many nations around the world—nowhere more so than India. For five days in a row, the country has set and reset the global record for new cases in a single day, tallying about 353,000 on April 26.
By official counts, about 2,000 people in India are dying from COVID-19 every day as hospitals grow overtaxed and oxygen supplies run short. Experts say the true toll is likely even higher than that. People are dying as they desperately seek treatment, and crematoriums nationwide are overwhelmed.
It can be difficult to grapple with that devastating reality when people in countries like the U.S. are reuniting with loved ones and cautiously emerging from lockdown. How can both scenarios be happening at once? The answer, as it often has during the pandemic, lies in disparity. As of April 26, 83% of vaccinations worldwide had been given in high- and upper-middle-income countries, according to a New York Times data analysis. In the developing world, many countries are preparing for the reality that it could take until 2022 or even 2023 to reach vaccination levels already achieved by richer countries today. Even in India, one of the world’s leading vaccine manufacturers, fewer than 10% of people have gotten a vaccine—a cruel irony, as people in India die in the streets while those thousands of miles away celebrate receiving their second doses.
To truly defeat COVID-19, we must reckon with that cognitive dissonance, says Dr. Rahel Nardos, who is originally from Ethiopia and now works in the University of Minnesota’s Center for Global Health and Social Responsibility. As an immigrant and global health physician who lives in the U.S., Nardos says she inhabits two worlds: one in which the U.S. may feasibly vaccinate at least 70% of its population this year, and another in which many countries struggle to inoculate even 20% of their residents in the same time frame.
“It’s a huge disparity,” Nardos says. “We need to get out of our silos and start talking to each other and hearing each other.”
That’s imperative, first and foremost because it could save lives. More than 13,000 people around the world died from COVID-19 on April 24. Remaining vigilant about disease prevention and monitoring, and working to distribute vaccines in countries that desperately need them to fight back COVID-19 surges, could help prevent more deaths in the future. That’s especially critical for developing countries, many of which are so overwhelmed by COVID-19 that nearly all other aspects of health care have suffered. “We may be looking at five, 10 years before they can get back to their baseline, which wasn’t that great to begin with,” Nardos says.
There’s also a global health argument for distributing vaccines more equitably. Infectious diseases do not respect borders. If even one country remains vulnerable to COVID-19, that could allow the virus to keep spreading and mutating, potentially evolving to such a point that it could infect people who are vaccinated against original strains of the disease. Already, vaccine makers are exploring the possibility of booster shots to add extra protection against the more transmissible variants currently circulating in various parts of the world.
We aren’t at that point yet; currently authorized vaccines appear to hold up well against these variants. But if the virus keeps spreading for years in some areas, there’s no telling what will happen, says Jonna Mazet, an epidemiologist and emerging infectious disease expert at the University of California, Davis.
“Evolution of those new strains could go into multiple directions. They may evolve to cause more severe or less severe disease. Some of the variants [could be] more concerning for young people,” Mazet says. “The whole dynamics of the disease change.”
And if the virus is mutating somewhere, chances are good it will eventually keep spreading in multiple areas, Mazet says. “Unless or until we have a major shift, we are still going to have large parts of every country that have a susceptible population,” she says. “The virus is going to find a way.”
The only way to stop a virus from mutating is to stop giving it new hosts, and vaccines help provide that protection. COVAX—a joint initiative of the World Health Organization; Gavi, the Vaccine Alliance; the Coalition for Epidemic Preparedness Innovations; and UNICEF—was meant to ensure that people in low-income countries could get vaccinated at the same time as people in wealthier ones. COVAX is providing free vaccines to middle- and low-income countries, using funds gained through purchase agreements and donations from richer countries. But supply and funding shortages have made it difficult for the initiative to distribute vaccines as quickly as it intended to. Many of the doses it planned to disseminate were supposed to have come from the Serum Institute of India, which delayed exporting doses in March and April as India focused on domestic vaccine rollout to combat its COVID-19 surge at home.
In the meanwhile, many poorer countries have been unable to vaccinate anywhere close to as many people as would be required to reach herd immunity. That will almost surely improve as new vaccines are authorized for use by regulators around the world, and as manufacturers scale up production, but those moves may be months away.
COVAX is also developing a mechanism through which developed countries could donate vaccine doses they don’t need. Some wealthy countries, including the U.S. and Canada, have contracts to purchase more than enough doses to vaccinate their entire populations, and have signaled their intent to eventually donate unneeded supplies—but timing is everything. That is, these countries will likely only donate once they are sure their own populations have been vaccinated at a level that ensures herd immunity.
On April 25, the Biden Administration said the U.S. would provide India with raw supplies for making AstraZeneca’s vaccine, as well as COVID-19 tests and treatments, ventilators, personal protective equipment, and funding. That’s a significant shift, since the export of raw vaccine materials was previously banned, but it still doesn’t provide India with ready-to-go vaccines. That step may be next, though. The U.S. will export as many as 60 million doses of AstraZeneca’s vaccine once the shot clears federal safety reviews, the Associated Press reports.
Gian Gandhi, UNICEF’s COVAX coordinator for supply, says he fears many wealthy countries’ vaccine donations may not come until late in 2021, just when global supply is expected to ramp up. That may cause a bottleneck effect: all doses may come in at once, rather than at a slow-but-steady pace that allows countries with smaller health care networks to distribute them. “We need doses now, when we’re not able to access them via other means,” Gandhi says.
The global situation is also critical now. Worldwide, more than 5.2 million cases and 83,000 deaths were reported during the week leading up to April 18. Indian hospitals are so overrun, crowds have formed outside their doors and desperate families are trying to source their own oxygen. Hospitals in Brazil are reportedly running out of sedatives. Iran last week broke daily case count records three days in a row. Countries across Europe remain under various forms of lockdown. Vaccines won’t change those realities immediately—but without them, the global community stands little chance of containing COVID-19 worldwide.

Just as other industries are rolling back some consumer-friendly changes made early in the pandemic — think empty middle seats on airplanes — so, too, are health insurers.
Many voluntarily waived all deductibles, copayments and other costs for insured patients who fell ill with covid-19 and needed hospital care, doctor visits, medications or other treatment.
Setting aside those fees was a good move from a public relations standpoint. The industry got credit for helping customers during tough times. And it had political and financial benefits for insurers, too.
But nothing lasts forever.
Starting at the end of last year — and continuing into the spring — a growing number of insurers are quietly ending those fee waivers for covid treatment on some or all policies.
“When it comes to treatment, more and more consumers will find that the normal course of deductibles, copayments and coinsurance will apply,” said Sabrina Corlette, research professor and co-director of the Center on Health Insurance Reforms at Georgetown University.
Even so, “the good news is that vaccinations and most covid tests should still be free,” added Corlette.
That’s because federal law requires insurers to waive costs for covid testing and vaccination.
Guidance issued early in President Joe Biden’s term reinforced that Trump administration rule about waiving cost sharing for testing and said it applies even in situations in which an asymptomatic person wants a test before, say, visiting a relative.
But treatment is different.
Insurers voluntarily waived those costs, so they can decide when to reinstate them.
Indeed, the initial step not to charge treatment fees may have preempted any effort by the federal government to mandate it, said Cynthia Cox, a vice president at KFF and director for its program on the Affordable Care Act.
In a study released in November, researchers found about 88% of people covered by insurance plans — those bought by individuals and some group plans offered by employers — had policies that waived such payments at some point during the pandemic, said Cox, a co-author. But many of those waivers were expected to expire by the end of the year or early this year.
Some did.
Anthem, for example, stopped them at the end of January. UnitedHealth, another of the nation’s largest insurers, began rolling back waivers in the fall, finishing up by the end of March. Deductible-free inpatient treatment for covid through Aetna expired Feb. 28.
A few insurers continue to forgo patient cost sharing in some types of policies. Humana, for example, has left the cost-sharing waiver in place for Medicare Advantage members, but dropped it Jan. 1 for those in job-based group plans.
Not all are making the changes.
For example, Premera Blue Cross in Washington and Sharp Health Plan in California have extended treatment cost waivers through June. Kaiser Permanente said it is keeping its program in place for members diagnosed with covid and has not set an end date. Meanwhile, UPMC in Pittsburgh planned to continue to waive all copayments and deductibles for in-network treatment through April 20.
What It All Means
Waivers may result in little savings for people with mild cases of covid that are treated at home. But the savings for patients who fall seriously ill and wind up in the hospital could be substantial.
Emergency room visits and hospitalization are expensive, and many insured patients must pay a portion of those costs through annual deductibles before full coverage kicks in.
Deductibles have been on the rise for years. Single-coverage deductibles for people who work for large employers average $1,418, while those for employees of small firms average $2,295, according to a survey of employers by KFF. (KHN is an editorially independent program of KFF.)
Annual deductibles for Affordable Care Act plans are generally higher, depending on the plan type.
Both kinds of coverage also include copayments, which are flat-dollar amounts, and often coinsurance, which is a percentage of the cost of office visits, hospital stays and prescription drugs.
Ending the waivers for treatment “is a big deal if you get sick,” said Robert Laszewski, an insurance industry consultant in Maryland. “And then you find out you have to pay $5,000 out-of-pocket that your cousin didn’t two months ago.”
Costs and Benefits
Still, those patient fees represent only a slice of the overall cost of caring for a hospitalized patient with covid.
While it helped patients’ cash flow, insurers saw other kinds of benefits.
For one thing, insurers recognized early on that patients — facing stay-at-home orders and other restrictions — were avoiding medical care in droves, driving down what insurers had to fork out for care.
“I think they were realizing they would be reporting extraordinarily good profits because they could see utilization dropping like a rock,” said Laszewski. “Doctors, hospitals, restaurants and everyone else were in big trouble. So, it was good politics to waive copays and deductibles.”
Besides generating goodwill, insurers may benefit in another way.
Under the ACA, insurers are required to spend at least 80% of their premium revenue on direct health care, rather than on marketing and administration. (Large group plans must spend 85%.)
By waiving those fees, insurers’ own spending went up a bit, potentially helping offset some share of what are expected to be hefty rebates this summer. That’s because insurers whose spending on direct medical care falls short of the ACA’s threshold must issue rebates by Aug. 1 to the individuals or employers who purchased the plans.
A record $2.5 billion was rebated for policies in effect in 2019, with the average rebate per person coming in at about $219.
Knowing their spending was falling during the pandemic helped fuel decisions to waive patient copayments for treatment, since insurers knew “they would have to give this money back in one form or another because of the rebates,” Cox said.
It’s a mixed bag for consumers.
“If they completely offset the rebates through waiving cost sharing, then it strictly benefits only those with covid who needed significant treatment,” noted Cox. “But, if they issue rebates, there’s more broad distribution.”
Even with that, insurers can expect to send a lot back in rebates this fall.
In a report out this week, KFF estimated that insurers may owe $2.1 billion in rebates for last year’s policies, the second-highest amount issued under the ACA. Under the law, rebate amounts are based on three years of financial data and profits. Final numbers aren’t expected until later in the year.
The rebates “are likely driven in part by suppressed health care utilization during the COVID-19 pandemic,” the report says.
Still, economist Joe Antos at the American Enterprise Institute says waiving the copays and deductibles may boost goodwill in the public eye more than rebates. “It’s a community benefit they could get some credit for,” said Antos, whereas many policyholders who get a small rebate check may just cash it and “it doesn’t have an impact on how they think about anything.”

Europe seems poised to set the global standard for vaccine passports, now that European Commission President Ursula von der Leyen has signaled that vaccinated Americans will be allowed to travel to the continent this summer.
Why it matters: Opening up travel to vaccinated Americans will bring new urgency to creating some kind of trusted means for people to prove they’ve been vaccinated, Axios’ Felix Salmon reports.
The big picture: There will probably never be a single credential that most people use to prove they’ve been vaccinated, for every purpose.
Details: Informal mechanisms like simply asking someone whether they’re had a shot can suffice in many situations. A system for international travel will likely be far more stringent. And there’s a wide middle, too.
The bottom line: The world of vaccine passports is almost certainly going to end up as a mishmash of different credentials for different activities, rather than a single credential used by everybody for everything.

Several hospitals are looking to split from the health system they belong to, regain independence or partner with a different healthcare organization.
Below are five instances reported since Jan. 1, beginning with the most recent:
1. 2 hospitals to part ways with U of Kansas Health System
HaysMed, a single-hospital system in Hays, Kan., and Pawnee Valley Community Hospital in Larned, Kan., will depart from the University of Kansas Health System in Kansas City. University of Kansas Health System and the two hospitals said they decided that working independently “best supports the long-term health and wellness of our communities.”
2. North Carolina system to sever ties with Atrium
Carolinas HealthCare System Blue Ridge, a two-campus system in Morganton, N.C., plans to cut ties with Charlotte, N.C.-based Atrium Health. The hospital system said its board of directors approved a nonbinding letter of intent to instead become part of the Chapel Hill, N.C.-based UNC Health network through a management services agreement.
3. California hospital seeks split from Providence: 6 things to know
Hoag Memorial Hospital Presbyterian in Newport Beach, Calif., is seeking to end its affiliation with Providence, a Catholic health system based in Renton, Wash. Hoag filed a lawsuit last year to split from the 51-hospital system.
4. Boone Hospital Center splits from BJC HealthCare April 1
Columbia, Mo.-based Boone Hospital Center became independent April 1, separating from St. Louis-based BJC HealthCare.
5. Washington hospital splits from Virginia Mason
Virginia Mason Memorial in Yakima, Wash., has transitioned back to an independent hospital and reverted to its old name. The board of Virginia Mason Memorial voted in late October to end its affiliation with Seattle-based Virginia Mason Health System. The hospital said it split from Virginia Mason because of the system’s merger with Tacoma, Wash.-based CHI Franciscan.
