Here are seven health systems with strong operational metrics and solid financial positions, according to recent reports from Moody’s Investors Service, Fitch Ratings and S&P Global Ratings.
Note: This is not an exhaustive list. Hospital and health system names were compiled from recent credit rating reports and are listed in alphabetical order.
1. St. Louis-based BJC Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has good margins and a favorable market position, according to Moody’s.
2. Hollywood, Fla.-based Memorial Healthcare System has an “Aa3” rating and stable outlook with Moody’s. The health system has a dominant market position in the southern portion of South Broward County and above average balance sheet liquidity, according to Moody’s.
3. Broomfield, Colo.-based SCL Health has an “Aa3” rating and stable outlook with Moody’s and an “AA-” rating and stable outlook with S&P. The health system has strong operating performance and solid balance sheet measures, according to Moody’s. The credit rating agency expects the health system’s cash flow to continue to grow.
4. Seattle Children’s Healthcare System has an “Aa2” rating and stable outlook with Moody’s. The health system has consistently strong operating performance, solid liquidity measures, and a favorable reputation within a broad service area, according to Moody’s.
5 Norfolk, Va.-based Sentara Healthcare has an “Aa2” rating and stable outlook with Moody’s. The health system has a leading market position in its service area, robust balance sheet metrics and solid margins, according to Moody’s.
6. St. Louis-based SSM Health has an “AA-” rating and stable outlook with Fitch. The health system has a strong financial profile and a growing health plan, according to Fitch. The credit rating agency expects SSM to continue to grow unrestricted liquidity and sustain improved operating performance.
7. Arlington-based Texas Health Resources has an “Aa2” rating and stable outlook with Moody’s. The health system has solid financial performance, a leading market position, good coverage of moderate debt levels, and a strong cash position, according to Moody’s.
The owner of telemedicine company Video Doctor Network on Friday pleaded guilty for his role in what the Justice Department is calling one of the largest healthcare fraud schemes prosecuted to date in the U.S.
Lester Stockett, 52, a resident of Colombia, agreed to pay $200 million in restitution to the U.S. as part of his plea agreement.
The Justice Department in April brought charges against 24 defendants including Stockett for their role in a $424 million conspiracy to defraud Medicare and receive illegal kickbacks. Stockett’s company allegedly received kickbacks from brace suppliers in exchange for arranging for physicians to order medically unnecessary medical equipment, such as back, knee and shoulder braces.
Stockett, owner of the Video Doctor Network and CEO of one of its subsidiaries, AffordADoc, on Friday pleaded guilty to one count of conspiracy to defraud the U.S. and pay and receive healthcare kickbacks, as well as one count of conspiracy to commit money laundering. His sentencing is set for Dec. 16 in New Jersey.
As part of his guilty plea, Stockett said he and others had solicited and received illegal kickbacks and bribes from patient recruiters, pharmacies and brace suppliers. In exchange, he said he and other Video Doctor Network employees bribed healthcare providers to order medically unnecessary orthotic braces for Medicare beneficiaries.
These Medicare beneficiaries were contacted through an international telemarketing network, which identified hundreds of thousands of elderly and disabled patients.
“This CEO and his co-conspirators lined their own pockets with hundreds of millions of dollars by exploiting telemedicine technology meant to help elderly and disabled patients in need of healthcare,” Assistant Attorney General Brian A. Benczkowski of the Justice Department’s Criminal Division said in a statement.
Brace suppliers, which were co-conspirators in the scheme, submitted more than $424 million in false and fraudulent claims to Medicare for these orders, Stockett said.
Medicare paid brace suppliers more than $200 million for these claims, according to the Justice Department.
Stockett said he and others hid illegal kickbacks and bribes by having them paid indirectly through nominee companies and bank accounts, both in the U.S. and in other countries.
Between March 2016 and April 2019, Stockett said he and other Video Doctor Network executives transferred more than $10 million in illegal kickback payments to a bank account in the Dominican Republic. They then transferred more than $9.8 million from that bank account in the Dominican Republic to bank accounts of AffordADoc in the U.S.
Stockett and other Video Doctor Network executives had also defrauded investors by claiming the company was a legitimate telemedicine enterprise that made $10 million in revenue annually, while revenue was obtained through illegal kickbacks and bribes, according to the plea agreement.
It’s been reported that up to 15% of Goldman Sachs partners are preparing to leave by year’s end. Truth is, firms across Wall Street are having a crummy year and lots of personnel are going to be purged soon.
Investment-banking revenues had their worst first half since 2006, according to a report last week by Coalition, a London-based research firm. The weakest performance is in bond, currency and commodity trading, which accounts for 42% of revenue, down from almost two-thirds before the financial crisis. When bankers complain about regulation tying them down, this is what they mean. Shed a tear?
Because revenues have fallen faster than expenses, the industry’s return on capital has dropped to 6.7%. Its cost of capital, however, is in the 10% to 12% neighborhood.
For Goldman, Morgan Stanley and the like, the encouraging news is they remain highly profitable and have fewer problems than Deutsche Bank or UBS and their never-ending restructuring. The grimmer news is shares of Goldman and Morgan Stanleyare 21% and 27% lower, respectively, than 18 month ago. President Donald Trump’s trade wars and sluggish economic conditions overseas are taking a toll.
What could turn things around? If recession fears abated there could be a jump in corporate mergers, which produce a ton of fees. It would also help if WeWork went public at a hefty price, but right now WeWork isn’t working well as a possible initial public offering. Help could come from a Trump administration eager to ease the banks’ regulatory burden by reducing the amount of capital they must hold.
Still, making money in the markets figures to get harder in the years ahead. Late last month the $210 billion New York state pension fund dropped the long-term assumed rate of return on its investments to 6.8% from 7%. It was the third time the pension fund has cut its expected return since 2010, when it was 8%.
“The long-term outlook for investors is changing and requires a more conservative approach,” state Comptroller Thomas DiNapoli said in a statement.
If big buyers of investments are dialing down expectations, their dealers will have little choice but to follow.
A business I know well—journalism—has been permanently altered by the same technological upheaval attacking the livelihoods of traders, dealmakers and number-crunchers. Staffers at BuzzFeed and other news organizations have responded by unionizing so their owners will collectively bargain with them. It would be odd indeed for the Wall Street crowd to spend some of their bonus money casting their lot with organized labor. But given how precarious their jobs look, maybe they should.
This new study, being released ahead of print, used data from the National Survey of Gun Policy from the years 2013, 2015, 2017, and 2019. The surveys were administered by the Johns Hopkins Center for Gun Policy and Research, which sampled adult gun owners and non–gun owners alike. The findings show that large majorities of both owners and nonowners strongly support a range of measures to strengthen US gun laws. Read More >>
This study will also appear in the October issue of Health Affairs, a theme issue with studies focusing on violence and health.
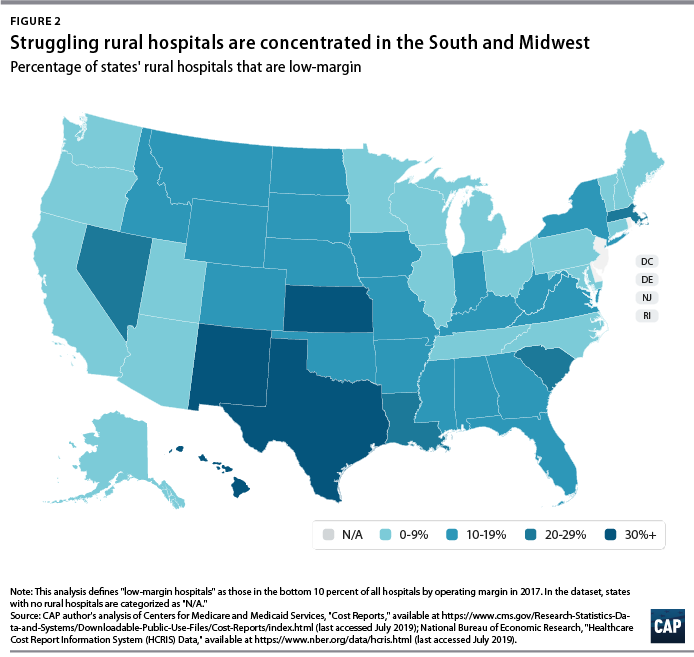
The number of rural hospital closures in the United States has increased over the past decade.1 Since 2010, 113 rural hospitals,2 predominantly in Southern states, have closed. This is a concerning trend, since hospital closures reduce rural communities’ access to inpatient services and emergency care.3 In addition, hospitals that are at risk financially are more likely to serve rural communities with higher proportions of vulnerable populations.4
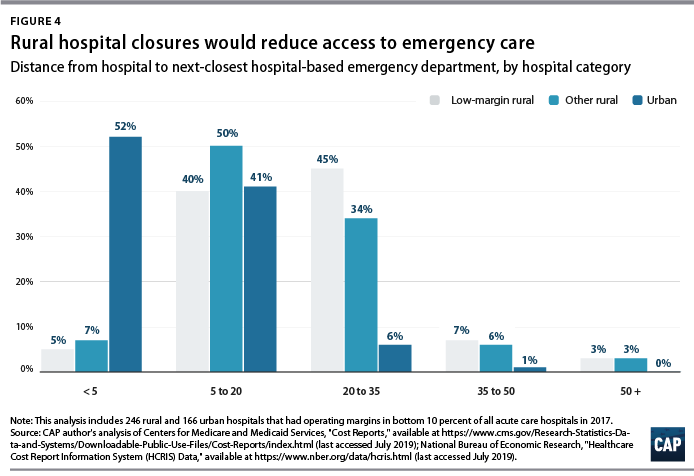
Understanding the financial pressures facing rural hospitals is imperative to ensuring that America’s 60 million rural residents have access to emergency care.5 Rural hospitals are generally less profitable than urban ones, and those with the lowest operating margins maintain fewer beds and have lower occupancy rates. Low-margin rural hospitals are also more likely to be in states that have not expanded Medicaid under the Affordable Care Act (ACA). According to new analysis by the Center for American Progress, future hospital closures would reduce rural Americans’ proximity to emergency treatment. Among low-margin, rural hospitals—those most likely to close—the majority of those with emergency departments are at least 20 miles away from the next-closest emergency department.
This report first discusses the role that hospitals and emergency care play in rural health care as well as trends in hospital closures. It then uses federal data to examine differences in the financial viability of rural and urban hospitals and the availability of hospital-based emergency care in rural areas. The final section of this report offers policy recommendations to improve health care access and emergency care for rural residents.
Rural hospitals have been closing at an unprecedented rate
From 2013 to 2017, rural hospitals closed at a rate nearly double that of the previous five years.6 (See Figure 1) According to the Government Accountability Office (GAO), recent rural hospital closures have disproportionately occurred among for-profit and Southern hospitals. Southern states accounted for 77 percent of rural hospital closures over that time period but only 38 percent of all rural hospitals in 20137
Hospital closures may deepen existing disparities in access to emergency care. Closures are more likely to affect communities that are rural, low income, and home to more racial/ethnic minority residents.8 Although about half of acute care hospitals are located in rural communities and the other half are located in urban areas,9 rural residents live 10.5 miles from the nearest acute care hospital on average, compared with 4.4 miles for those in urban areas.10 According to a poll by the Pew Research Center, about one-quarter (23 percent) of rural residents said that “access to good doctors and hospitals” is a problem in their community, while only 18 percent of urban residents and 9 percent of suburban residents said it was a problem.11
A variety of factors influence hospitals’ sustainability. Thanks to medical and technological advances, conditions that once required hospitalization can now be treated in an ambulatory care center or a physician’s office. University of Pennsylvania professor and CAP nonresident senior fellow Ezekiel Emanuel has argued that one reason hospitals are closing is that “more complex care can safely and effectively be provided elsewhere, and that’s good news.”12 As a whole, the hospital industry remains highly profitable, and hospital margins are at their highest in decades.13
Evidence on the relationship between hospital closures and health outcomes is mixed. A 2015 study of nearly 200 hospital closures in Health Affairs found no significant changes in hospitalization rates or mortality in the affected communities, whether rural or urban.14 More recent studies have found an association between rural hospital closures and increased mortality. Harvard researcher Caitlin Carroll showed that rural hospital closures led to an overall increase in mortality rates for time-sensitive health conditions,15 and Kritee Gujral and Anirban Basu of the University of Washington found that rural hospital closures in California were followed by increases in mortality for inpatient stays.16
In rural areas, hospitals face additional challenges to their viability, including lower patient volumes; higher rates of uncompensated care; and physician shortages.17 In addition, rural patients tend to be older and lower income.18 Rural hospitals tend to be smaller, serve a higher share of Medicare patients, and have lower occupancy rates than urban hospitals.19 Rural hospitals commonly offer obstetrics, imaging and diagnostic services, emergency departments, as well as hospice and home care,20 but patients needing more complicated treatment are often referred to tertiary or specialized hospitals. In fact, rural patients are more likely to be transferred to another hospital than patients at urban hospitals.21
Most urban hospitals are reimbursed under the prospective payment systems (PPS) for Parts A and B of Medicare. Through both the inpatient and outpatient PPS, the Centers for Medicare and Medicaid Services (CMS) reimburse hospitals at a predetermined amount based on diagnoses, with adjustments—including those for local input costs and patient characteristics.22However, rural hospitals often face higher costs due to lower occupancy rates and provide care to a higher percentage of patients covered by Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). Such hospitals may be eligible to receive higher payments from Medicare if they qualify as a Sole Community Hospital (SCH) or Medicare-Dependent Hospital (MDH).23
Another form of financial relief for rural hospitals is obtaining designation as a Critical Access Hospital (CAH), which Medicare reimburses based on cost rather than on the PPS.24 To qualify as a CAH, a hospital must provide 24/7 emergency services; maintain no more than 25 beds; and serve a rural area that is 35 miles from another hospital.25 Medicare reimburses CAHs at 101 percent of reasonable costs, rather than through the inpatient and outpatient PPS structures.26 As of 2018, there were 1,380 CAHs nationwide,27 accounting for about two-thirds of all rural hospitals.28
Even with cost-based reimbursement, however, some CAHs are unable to sustain the costs required to maintain inpatient beds.29 The 25-bed limit for CAHs prevent participating hospitals from eliminating inpatient services and restrict their ability to expand in response to fluctuations in community populations or care volumes. Other challenges facing rural hospitals include lacking sufficient patient volume to maintain high-quality performance for certain procedures and pressure to drop high-value but poorly reimbursed services such as obstetrics while maintaining low-volume, high profit services such as joint replacement procedures. 30
A key way that states can support struggling rural hospitals is by expanding Medicaid under the ACA. Expanding Medicaid increases coverage among low-income adults, 31 which in turn reduces uncompensated care costs for hospitals32 and allows financially vulnerable hospitals to improve their viability.33 Consistent with other recent studies,34 the GAO concluded in a 2018 report on rural hospitals that those “located in states that increased Medicaid eligibility and enrollment experienced fewer closures.”35
Rural hospitals are cutting back on services
Rural hospitals in different states have responded to financial pressures in a variety of ways, trying to balance community needs with financial viability. For many hospitals this has meant cutting inpatient obstetric services, leaving more than half of rural counties without hospital obstetric services.36 For instance, in Wisconsin, falling birth rates led to 12 hospitals in the state closing their obstetric services in the past decade.37 In Grantsburg, Wisconsin, lower birth rates and an older community population led Burnett Medical Center to shut down its obstetrics services.38 In order to offer these services, Burnett Medical Center would have needed to keep a general surgeon on call to perform caesarean sections, and with just 40 deliveries in 2017, the hospital could not justify the expense.39 While the hospital will continue providing prenatal and postnatal care, it will refer patients to a facility in Minnesota for deliveries—a facility is almost 40 minutes away.40
In other communities, hospitals have been replaced by other types of health care facilities. For example, Appalachian Regional Healthcare System closed Blowing Rock Hospital in North Carolina in 2013. Three years later, it opened a 112-bed post-acute care center in Blowing Rock in response to demand for rehabilitation services and the aging population in the surrounding area.41
Financial data shows that rural hospitals are more likely to struggle
To compare the financial situations of rural and urban hospitals and examine how future rural hospital closures could affect the availability of emergency care, CAP analyzed data from the CMS Healthcare Cost Report Information System (HCRIS). The CMS requires all Medicare-certified hospitals to report their financial information annually. CAP used the HCRIS to examine the financial margins and other characteristics of 4,147 acute care hospitals for fiscal year 2017. Of these, 1,954 hospitals (47 percent) were in rural areas, while the remaining were in urban areas. Hospitals self-report their status in the HCRIS as either urban or rural, which the CMS defines as either inside or outside of a metropolitan statistical area, respectively.42 Further information about CAP’s hospital sample can be found in the Methodological appendix.
Hospital operating margins, which measure excess patient-related revenues relative to patient-related expenses, are often used as an indicator of financial health.43 A 2011 study by Harvard researchers Dan Ly, Ashish Jha, and Arnold Epstein found that the lowest 10 percent of hospitals by operating margin were 9.5 times more likely to close within two years compared to all others. 44 The same study concluded that hospitals with low operating margins were also more likely to be acquired or merge.45
In CAP’s hospital sample, the median operating margin was negative 2.6 percent among all hospitals, negative 0.1 percent for urban hospitals, and negative 4.9 percent for rural hospitals.46 Public hospitals and MDHs in the sample were more likely to have negative operating margins, consistent with what other studies have found.47 To analyze hospitals’ relative financial health across geographic areas, CAP ranked hospitals in the HCRIS sample based on operating margin, splitting them into three groups: the lowest 10 percent, the middle 80 percent, and the highest 10 percent. The range of operating margins for each group is shown in Table 1.
Rural hospitals are less likely to be financially healthy than urban hospitals. In 2017, rural hospitals comprised only 27.9 percent of the hospitals with operating margins in the highest decile but comprised 59.7 percent of the hospitals in the lowest decile. Southern and Midwestern states had the greatest proportion of rural hospitals with low operating margins, mimicking the geographic patterns in hospital closures that the GAO report identified. CAP finds that from 2015 through 2017, rural hospitals were consistently more likely than urban hospitals to fall in the bottom 10 percent of operating margins. CAP’s analysis also confirms that rural hospitals in states that expanded Medicaid had a higher median operating margin (negative 3.4 percent) than those in states that have not expanded Medicaid (negative 5.7 percent).
To examine commonalities among the hospitals most vulnerable to closure, CAP analyzed characteristics of the hospitals with low margins, defined as having an operating margin in the lowest 10 percent among all hospitals. Smaller, low-occupancy rural hospitals were most likely to struggle financially: nearly 1 in 6 (15 percent) of hospitals with 25 or fewer beds had low margins, and nearly one-fifth (17 percent) of hospitals with low-occupancy rates had low margins. (See Figure 3)
Emergency departments are on the front lines for rural health
In some emergency situations, hospital closures can be life-threatening, increasing the time and distance patients travel to receive care. Studies show that the probability of dying from a heart attack increases with distance from emergency care,48 and traumatic injuries are more likely to be fatal for rural residents than for urban ones.49
Rural residents are more likely than urban residents to visit the emergency department.50 A shortage of primary care providers; lack of public transportation infrastructure; shortages in preventive care; higher rates of smoking and obesity; and greater prevalence of chronic disease in rural areas all contribute to the greater utilization of emergency room care.51 As a result, emergency departments often stand in as the main source of care for vulnerable and low-income populations, especially for communities that face a shortage of primary care. 52 Among the dozens of rural hospitals that have closed in recent years, some served as the only emergency department in a community, according to MedPAC53
While freestanding emergency departments have proliferated,54 they are not filling the gap for rural emergency care. MedPAC found that, as of 2016, nearly all the country’s 566 stand-alone emergency departments were in urban areas and tended to be located in more affluent communities.55 Researchers at the North Carolina Rural Health Research Program found that the freestanding emergency department model was generally not viable in rural areas of the state due to low patient volumes, high rates of uninsured patients, and provider shortages.56 One limit on the growth of independent freestanding emergency centers is that they are not recognized in Medicare law and are therefore unable to bill the program, unlike hospital-affiliated off-campus emergency departments. 57
Future rural hospital closures would increase the distances that patients travel for emergencies
To better understand how future rural hospital closures could affect access to emergency care, CAP calculated hospitals’ distance to the next-closest hospital-based emergency department. CAP restricted its 2017 HCRIS data sample to the 3,616 acute care hospitals that provide 24-hour emergency services.58 Using addresses or coordinates provided in the HCRIS, CAP mapped each low-margin rural hospital to the next-closest hospital emergency department. Mapping strategies are detailed in the Methodological appendix.
Among the 222 low-margin rural hospitals, more than half (55 percent) were more than 20 miles away from the next-closest hospital-based emergency department, and one-tenth were more than 35 miles away. (See Figure 4). The average distance to the next-closest emergency department was 22 miles.
The disappearance of rural, low-margin hospitals would greatly increase patients’ travel distances for emergency care. Without other resources to fill the gap, some patients might forgo care they need and others would be forced to undertake an even longer journey to receive medical attention.
Policies to improve rural emergency and nonemergency care
As rural hospitals continue to close, it is crucial to preserve access to emergency care for rural Americans. The following section details a series of policy recommendations to support adequate emergency care and address care shortages in rural communities.
Expand Medicaid
Experience to date suggests that rural hospitals in those states that have not yet expanded their Medicaid programs under the ACA would benefit from Medicaid expansion through lower levels of uncompensated care and increased financial sustainability. Medicaid expansion is associated with improvements in health and a wide variety of other outcomes, including lower mortality, less uncompensated care, and lower rates of medical debt.59 According to the Kaiser Family Foundation, about 4.4 million adults would gain Medicaid eligibility if the remaining 14 nonexpansion states expanded their programs.60
Policymakers can also support rural communities and their hospitals by opposing efforts to repeal the ACA. If the Trump administration-backed lawsuit against the ACA were to succeed, 20 million Americans would lose health insurance coverage, and uncompensated care would rise by $50 billion, according to the Urban Institute.61
Create a greater number of rural emergency centers
To preserve access to emergency care, Congress could allow rural hospitals like CAHs to downsize to an emergency department and eliminate inpatient beds without giving up special Medicare reimbursement arrangements. Qualifying hospitals could transfer patients requiring inpatient admission to other hospitals, while continuing to offer some diagnostic imaging and other outpatient services.
One such proposal is the Rural Emergency Acute Care Hospital Act (REACH Act), bipartisan legislation proposed by Sen. Amy Klobuchar (D-MN) and Sen. Chuck Grassley (R-IA) that would create rural emergency centers.62 This designation would allow hospitals to provide only emergency care in rural communities and receive Medicare reimbursement at 110 percent of operating costs. Separately, MedPAC has recommended that rural hospitals located more than 35 miles from the nearest emergency department be allowed to convert to freestanding emergency departments while still being reimbursed at hospital rates.63
Institute global budgeting for rural hospitals
Under global budgeting, hospitals are paid a fixed amount rather than having their reimbursements based on the volume and types of services they provide.64 Global budgeting can reduce small, rural hospitals’ financial risk by providing them with a more predictable stream of revenue. In addition, payment reforms that include both hospital and nonhospital care can encourage communities to invest in services that are typically less generously reimbursed, such as preventive care.65
For example, in 2014, Maryland transitioned its acute hospitals from fee-for-service payments to a global budget.66 An evaluation of the global budget program showed that it reduced hospital expenditures relative to trend without transferring costs to other parts of the health care system.67 Future global budgets should emphasize improvements in population health and primary care,68 including ensuring that patients receive care in appropriate settings and reducing the number of avoidable hospital visits.
The Pennsylvania Rural Health Model is the first Medicare demonstration project to test the financial viability and community effects of a global budget for strictly rural hospitals.69 This six-year program aims to smooth out cash flow for 30 rural Pennsylvania hospitals on a monthly basis with the goal of enabling hospitals to meet community needs, especially for substance-use disorder and mental health services.70 With global budgets based on the previous year’s revenues, participating hospitals will have a more predicable stream of revenue. Importantly, the program allows hospitals to share in the savings that result from avoidable utilization.71
Improve transportation for rural residents
The lack of transportation infrastructure can lead rural residents to rely on ambulances and emergency rooms for nonemergency care. In nonemergency situations, patients often cite the lack of affordable transportation as a major barrier to care access.72 In order to fill the gap, payers and policymakers should consider efforts to utilize existing community transit resources for medical transportation or reimburse patients who use ride-sharing services in areas that lack public transit or taxi services. 73 Another option would be to formalize volunteer services for medical transit. Oregon offers a tax credit for volunteer rural emergency medical services (EMS) providers, who provide medical and transportation services analogous to those of volunteer firefighter programs.74 The CMS should also consider policies to better reimburse and expand the use of telehealth in remote areas to reduce patients’ burden of transportation.75Finally, the CMS should stop approving states’ requests to waive coverage of nonemergency medical transportation (NEMT) requirements under Medicaid.76 NEMT is vital to eligible beneficiaries’ access to care, including appointments for preventive care, chronic disease management, and substance-use disorder treatment.
Strengthen the rural health care workforce
Rural health care provider shortages contribute to poorer access to care and poorer quality of care in rural communities. While 20 percent of the U.S. population lives in rural areas, only 9 percent of primary care physicians practice in rural areas.77 Greater access to primary care providers in rural areas would improve quality of care and health outcomes while also reducing unnecessary emergency department visits.78
One way to assist rural areas would be to encourage health professionals to train and work in underserved communities. Federal funding for physician training should include reimbursements for community-based sites so that medical residents can rotate through nonhospital settings.79 Expanding the National Health Service Corps—which provides scholarships and student loan repayment for professionals who work in federally designated health professional shortage areas—could also help bolster the rural workforce. In addition, changes to immigration policy—such as expanding the Conrad 30 program that funnels immigrant doctors into rural and underserved communities, reforming H-1B visas to benefit high-need communities—could help alleviate rural areas’ shortage of medical professionals.80
Conclusion
Mounting closures of rural hospitals across the country are exacerbating the disparity in health care access between rural and urban areas. The financial vulnerability of the remaining rural hospitals suggests that the trend may continue, leaving shortages in emergency care and other hospital services.
Policymakers should support initiatives that allow remaining rural hospitals the flexibility to tailor their services to meet community needs and improve access to care for rural Americans.
The U.S. trade war with China threatens to hit hospitals and health systems as well as consumers in the form of higher prices and product shortages, the president of medical supply distributor DealMed told Yahoo Finance.
On Sept. 1, President Donald Trump imposed a 10 percent tariff on $300 billion in Chinese imports, tacking more medical supplies on the list. And the administration is threatening to hike the current 25 percent tariff on $250 billion in Chinese imports to a 30 percent tariff on Oct. 1.
The products affected by the tariffs are used daily in physician offices, hospitals, pharmacies and by consumers at home, according to DealMed President Michael Einhorn.
“Think of products like gauze that are in Band-Aids. Think of other products like medical gloves,” Mr. Einhorn told Yahoo Finance. “Those products will be somewhat affected, somewhere between 10 percent and 25 percent.
“When you throw tariffs into the mix, we’re talking about potential shortages, we’re talking about potential price increases — not only to hospitals and big healthcare systems, but also to the consumer at home,” Mr. Einhorn said.
For a small group of vascular surgery centers in metropolitan Washington, D.C., it was local churches that turned out to be surprisingly lucrative.
It was at health screening fairs hosted by these houses of worship where Marty Makary, M.D., found surgeons drumming up business for pricey—and often unnecessary—leg stents. It’s among the collection of systemic and human examples Makary examines in his new book “The Price We Pay: What Broke American Health Care—and How to Fix It” as driving forces behind rising U.S. health costs.
Makary, a surgeon at Johns Hopkins and New York Times best-selling author, hits every segment of the market, from a health system in New Mexico that has sued 1 in 5 residents in town to a health insurance conference where brokers described over drinks why they usually aren’t helping employers get the best deal.
“Healthcare has adopted a business model that uses middlemen, price gouging and sometimes delivers care that can be inappropriate, and this bloated economy has a tremendous amount of waste,” Makary said. “So our research really asks the question: ‘What is the experience of the everyday American interfacing with our healthcare system?’”
I caught up with Makary recently to discuss some of the problems he highlights in his new book, which is being released Sept. 10, and some of his ideas on how we solve them.
FierceHealthcare: Why did you write this book?
Marty Makary: Hospitals are amazing places and there is a tremendous amount of public trust in hospitals. But I’ve been seriously concerned about the erosion of public trust by the price gouging and predatory billing practices that patients are describing all over America. Our research team found bills are marked up as much as 23 times higher than what hospitals will accept from Medicare. We kept hearing over and over again that, ‘No one is expected to pay these bills. Hospital CEOs assured me when I showed them inflated bills that nobody is expected to pay the sticker price.’ But that didn’t seem to match the stories we were hearing on the ground.
FH: One of the hospitals you highlight in this book in Carlsbad, New Mexico, had a practice of hiking prices and suing patients who were unable to pay. What did you find there?
MM:We decided to shift our research into the question: “Are Americans asked to pay the sticker price and if so, what happens when they can’t afford it?”
A woman sent me a message where not only was the bill inflated, but the care was—in her opinion, unnecessary—and the hospital had sued her. When I reached out, she said, “They’ve sued all my friends as well and garnished our paychecks.” I couldn’t believe this, and so I flew out to Carlsbad. The driver of the Chamber of Commerce taxi service that picked us up from the airport, the receptionist at the hotel, the waitress at the breakfast place, the clerk’s office staff, families in the courthouse: You couldn’t believe it. Everywhere you turned, people had been terrorized financially by this local community hospital. I thought: “Where is the spirit of medicine? Do these executives even know the consequences on the ground of these billing practices?”
FH: In the book, you mention many hospital executives don’t even know they’re suing patients.
MM:Oftentimes, there’s detachment. And when we’re detached from the consequences or problems, that’s when horrible things happen in societies historically. I found sometimes hospital executives, board members and certainly our research supports doctors not knowing about this practice. And when they find out, the clinicians are outraged. By and large, board members want it to stop … I think if you look at any major issue in the United States, whether it be race, poverty or healthcare, if we are not proximate to the problem, we tend to rationalize financial systems that enable the problem. In healthcare, what I’ve noticed is, when I would share these stories at conferences, other healthcare experts argued it was not a problem that was diabolical, they just weren’t proximate to the issue.
FH: You also document that many hospitals are doing the right thing.
MM: Most hospitals try to do the right thing. But I think it tells us a lot about the practice of suing patients and that it’s unnecessary. When all the revenue generated from suing patients amounts to less than the amount of the CEO pay increase in one year, which is something we’ve seen, the argument that it’s essential to sue patients in order for the hospital to be sustainable melts away.
FH: But obviously, the problem is not just about hospitals, right?
MM: A lot of people are getting rich in healthcare. We’ve created tens of thousands of millionaires that are not patient-facing. If you look at the earnings on Wall Street of some of these healthcare companies, for example, UnitedHealth Group reported a 25% increase in earnings in a recent earnings report. How do earnings go up 25% in an actuarial insurance business? They said on their call it was in part due to their pharmacy benefit manager (PBM), a well-known middleman that profits from spread pricing and money games. Hospitals are on target this year for their highest margin in history—5.1% based on early 2019 data. At the same time rural hospitals are closing, large hospitals are making barrels of money. Although they are claiming razor-thin margins, the cost shift accounting is so sophisticated, that they can use their profit to buy new buildings, pay down debt, buy more real estate, increase executive pay. What we have right now is an arms race of profiteering in healthcare where all the stakeholders are making a lot of money except for one, and that’s the patient.
FH: In the book, you talk about efforts to address practice outliers like those vascular surgeons through the use of big data, which led to the creation of the “Improving Wisely” initiative. What did you do?
MM: Most doctors do the right thing or always try to. But the fraction that are responding to the consumerist culture or the perverse incentives or are just not practicing state of the art care can cost the system a lot more money than those who aren’t … Instead of hammering doctors that do the right thing with reporting burdens and other hassles, we can shunt those resources to address outliers identified in the data using metrics endorsed by the experts in each specialty, and gold card the good doctors so they don’t have to deal with reporting hassles and the expense of the reporting hassles.
In studying the issue of inappropriate care and delivering measures of the appropriateness of care, we’ve been meeting with individual specialists around the country and many of these doctors are telling us about the practice pattern that a fraction of specialists in their field are doing that represents overuse. Our work called “Improving Wisely” partners with associations to send outlier physicians their data around a specialty-endorsed measure of overuse. What we’ve seen is, among doctors, among outlier physicians who see their data with a confidential dear doctor letter, that 83% reduce their pattern of overuse. The initial project two years ago that cost $150,000 has resulted in $27 million worth of savings. This is an example of a high consensus approach that results in real savings that you just don’t see in other areas. By and large, politicians are talking about different ways to fund the broken healthcare system and not ways to fix it. We need to talk about how to fix it.
FH: In the book, you really seem to try to take on everyone: doctors, hospitals, air ambulances, workplace wellness companies, PBMs.
MM:Almost all the voices in healthcare are beholden to some special interest or stakeholder. We desperately need a global critique of how this system has gone awry and there’s a lot of finger-pointing going on right now, especially at the insurance companies and pharma. But the reality is, we all have a piece of this pie. I don’t think there’s really any one villain in the healthcare system. I don’t even think there’s much deliberate malfeasance that goes on. I think we have a system that’s largely run by people doing what they are told to do and they are doing it in a place where they may not be proximate to the hardship the system creates.
FH: So the big question: How do we fix the problems?
MM: For every problem I described, I tried to describe one of the most exciting disrupters in this space. With the pricing failure problem, I highlight the Free Market Medical Association and the individuals who are saying they are going to make all prices transparent and fair regardless of who’s paying whether it’s a patient or an insurance company. There’s one fair price. Keith Smith of the Surgery Center of Oklahoma is offering one fair true price. Not a sticker price but a true price, regardless of who’s paying. You look at MDsave and Clear Health Costs. They are offering ways for people to shop. If the government does nothing on healthcare, I’m still optimistic we are moving in the right direction because businesses in American are realizing that they’re getting ripped off on their healthcare and pharmacy plans. They’re increasingly doing direct contracting and looking closely at their health insurance benefits and pharmacy design and realizing there is a lot of money wasted.
One of the root issues in healthcare is the way we physicians are educated. It uses a model that’s highly flawed, relying highly on rote memorization of things that are easily available on the Internet today and omits training in effective communication, public policy and healthcare literacy. It turns out that many doctors feel paralyzed in fixing this broken system even as they’re suspicious of the waste in it. One of the goals of writing the book was creating healthcare literacy because we in the field are taught medical literacy but we’re never taught healthcare literacy. One of the exciting disrupters I had the privilege of spending time was the Sidney Kimmel Medical College (in Philadelphia). They have an academic standard in the admissions process. Once people meet that academic standard, everybody is considered based on their empathy, self-awareness and communication skills. It’s revolutionary as simple as it sounds. But they’re focusing on what matters.
Hospitals recorded profit improvements in July after posting significant year-over-year decreases in June, according to a report from financial advisory firm Kaufman Hall.
The firm found hospitals’ EBITDA margin rose 77.5 basis points month over month. Hospitals also saw their operating margins climb 105 basis points. Both measures marked the sixth month of improved hospital profitability out of the past seven months.
“While these trends generally are good news for the industry, the improvements do not necessarily mean that hospitals are achieving sufficient margins,” according to Kaufman Hall. “Also, margins of individual hospitals do not necessarily reflect those of overall health systems.”
Kaufman Hall noted that hospitals did see their volumes increase in July compared to June, which saw declines in patient volumes.