“We have a collaborative culture; it’s one of our system’s core values. But it takes us far too long to make decisions.” A health system CEO made this comment at a recent meeting, giving voice to a dilemma many system executives are no doubt facing. Of course, leaders want their teams to collaborate—in any important decision, we want to hear different voices, consider diverse points of view, and incorporate various areas of expertise.
On the other hand, collaboration takes time, which we don’t have right now.It also can add complexity, be the enemy of clear direction, and muddy accountability. This CEO went on to make an essential connection: “My concern is that this protracted decision making isn’t just a process problem, but that it’s showing up in our results.
Take performance improvement—we all quickly agreed we need to cut costs, but it’s taking far too long for us to act, and I fear we’ll have trouble holding the new line over time.” She further mused
“I wonder if this problem is, at least in part, due to how we make decisions. We don’t make them quickly enough, they aren’t clear enough, and we don’t have the most effective system of accountability.”
On one hand, traditional hospital culture is rightly grounded in the safety, hierarchy, and tradition of a do-no-harm world. But on the other hand, today’s economic, technological, and competitive environments require an approach to operations, revenue, and growth that has the aggressiveness of a Fortune 50 company. This should not be an either-or situation. Health systems can uphold a culture of safety while also fostering nontraditional values that will drive the organization assertively toward the future – all while committing to change.
Nearly 50% of U.S. adults report struggling to keep up with the cost of healthcare, with four in ten ringing in the new year with medical debt. Medical debt is a major burden that often forces people to delay–and sometimes forgo–access to care. Not only do outstanding medical bills undermine health, but they also represent the most common type of collections, with estimates ranging anywhere from $81 to $140 billion.
With problematic hospital practices gaining national media attention – including rejecting appointments for patients with outstanding medical bills and going so far as to sue such patients – the issue of medical debt is front and center for many Americans.
A glimpse into the state of hospital billing practices
Hospital watchdogs have started collecting valuable data on hospital billing practices to inform patients about these practices and potentially put pressure on hospitals to improve.
In an effort to capture the varied nature of hospital billing and collection practices, the Lown Institute is building a database of financial assistance policies and billing and collection practices across 2,500 hospitals with the support of Arnold Ventures. Initial results are expected to be available in mid-2024 with a full report issued in 2025.
Also interested in evaluating the current state of hospital’s financial practices, in 2021, the Leapfrog Group added questions to their hospital survey around billing and collections. Researchers from the Leapfrog Group, Northwestern University Feinberg School of Medicine, and Johns Hopkins University School of Medicine published a recent analysis of this data in JAMAwhere they found that many hospitals are still falling short when it comes to billing ethics. Although the data set of 2,270 hospitals was not nationally representative, it provides an interesting glimpse into the billing practices of some U.S. hospitals.
Here are the key takeaways:
754 hospitals (33.2%) reported that they “take legal action against patients for late payment or insufficient payment of a medical bill.” Rural hospitals were 38% more likely than urban hospitals to take legal action against patients.
1,020 (44.9%) hospitals did not routinely send patients itemized bills within 30 days of final claims adjudication or date of service for patients without insurance.
125 (5.5%) hospitals did not provide access to billing representatives capable of investigating billing errors, offering price adjustment, and establishing payment plans.
Ultimately, only 38% of surveyed hospitals reported meeting all three proposed billing quality standards. Interestingly, hospitals with worse Leapfrog safety grades were less likely to meet all three billing standards compared to hospitals with better grades. It’s not clear what’s behind this pattern, but it could be an issue of capacity (hospitals with more resources and staff have an easier time abiding by safety protocol and billing standards), or potentially profiteering (hospitals more concerned with making money may be both understaffing hospitals and suing patients).
So, how can we encourage better billing practices and reduce harm caused by medical debt?
The JAMA study authors recommend standardizing measurement and reporting of hospital billing practices to “increase accountability, reduce variation in billing practices, and reduce barriers in access to care in the US.”
Some states are taking these recommendations to the policy-level, working to make healthcare more affordable for patients. To date, eight states limit medical debt interest and two states restrict credit reporting of medical debt. Current policy proposals on the docket include New York’s Senate Bill S5909B, which seeks to ban hospitals from suing patients making less than 400% of the federal poverty level (FPL).
This research is important to not only provide further insight into how hospitals financially support, or undermine, their patients, but also inform policy efforts to improve healthcare affordability and hospital accountability moving forward.
A jury found former Vanderbilt Health nurse RaDonda Vaught guilty of negligent homicide and gross neglect of an impaired adult after she committed a fatal drug error in 2017. Vaught, who gave a patient a lethal dose of the paralytic agent vecuronium rather than the sedative Versed, overlooking several warning alerts, now faces up to six years in prison.
The Gist: Criminal charges for unintentional medical errors like this one are very unusual; discipline is normally the purview of licensing boards and civil courts. While Vaught certainly made an egregious mistake that directly led to a patient’s death, there’s a delicate line between holding caregivers accountable and making them criminally liable for unintentional errors.
The American Nurses Association warns this verdict could set a dangerous precedent, and have a chilling effect on providers’ reporting errors. Health systems have worked diligently over decades to promote a culture of quality improvement and transparency—central to that is an environment that encourages providers to report all medical errors in order to improve patient safety. Many providers are now concerned that this conviction could reverse that progress.
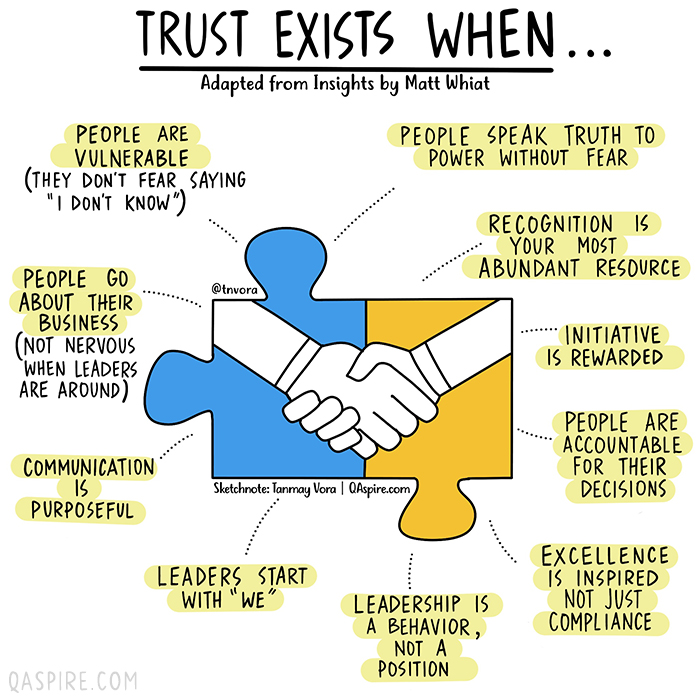
In the era of great awakening, leaders have to step up and be conscious about building trust with people they work with.
The old rules and hierarchies, that were already becoming obsolete, have now been thrown out of the window. People look for integration of work and well-being knowing that work is what you do, not a place you go to.
Opportunities are abound and excellent people have ample choices (they always had). It is high time that organizations and leaders think this through carefully to first align their own mindset to this new reality and then take conscious actions to build teams, practices and processes that are not just high-performing but also have a strong fabric of trust woven in.
Employees, after all, are volunteers who exercise their choice of working with you. Effective leadership is about making it worth for them.
Building high-trust environment means putting the human back at the center of how a business functions and building everything – purpose, culture, processes, structures, rituals, systems, tools and mindsets – around it.
How would we know if we are working in an environment where we can trust others and that we are trusted? We can always answer this based on our intrinsic feeling but if you are a leader who is working hard to build trust, here are a few vital signs that you need to look for.
President Trump on Monday moved to lift restrictions imposed on travelers to the U.S. from much of Europe and Brazil that were implemented last year to slow the spread of the novel coronavirus, though the action is expected to be stopped by the incoming Biden administration.
Trump issued an executive order terminating the travel restrictions on the United Kingdom, Ireland, Brazil and the countries in Europe that compose the Schengen Area effective Jan. 26. The order came two days before Trump leaves office. President-elect Joe Biden’s team immediately signaled they would move to reverse the order.
“With the pandemic worsening, and more contagious variants emerging around the world, this is not the time to be lifting restrictions on international travel,” tweeted incoming White House press secretary Jen Psaki.
“On the advice of our medical team, the Administration does not intend to lift these restrictions on 1/26. In fact, we plan to strengthen public health measures around international travel in order to further mitigate the spread of COVID-19,” Psaki continued.
The order states that Trump’s action came at the recommendation of outgoing Health and Human Services Secretary Alex Azar.The memo cites the new order from the Centers for Disease Control and Prevention (CDC) that requires passengers traveling by air to the U.S. to receive a negative COVID-19 test within three days before their flight departs, saying it will help prevent travelers from spreading the virus.
The Trump administration’s travel restrictions on China and Iran will remain in place, however, because, the order states, the countries “repeatedly have failed to cooperate with the United States public health authorities and to share timely, accurate information about the spread of the virus” and therefore cannot be trusted to implement the CDC’s order.
“Accordingly, the Secretary has advised me to remove the restrictions applicable to the Schengen Area, the United Kingdom, the Republic of Ireland, and the Federative Republic of Brazil, while leaving in place the restrictions applicable to the People’s Republic of China and the Islamic Republic of Iran,” Trump’s order states. “I agree with the Secretary that this action is the best way to continue protecting Americans from COVID-19 while enabling travel to resume safely.”
Though Trump signed the order on Monday, the action does not take effect until six days after he leaves office and Biden is inaugurated.
The order comes as coronavirus cases and deaths continue to hit worrisome, record-high levels on a daily basis. Nearly 400,000 people in the U.S. and more than 2 million people globally have died from COVID-19. While two vaccines have been approved for emergency use in the U.S., the Trump administration has fallen far short of early targets in distributing and administering the vaccine.
The order will be one of the final actions that Trump takes with respect to the pandemic, after being widely criticized for regularly minimizing the threat posed by the virus.
Trump announced in mid-March of last year that he would impose travel restrictions on individuals entering the United States from the 26 countries that compose the Schengen Area, weeks after the first case was reported in the U.S. The move initially attracted scrutiny because it did not include the U.K. or Ireland, and the Trump administration later moved to restrict travel from those countries as well.
Trump later placed travel restrictions on Brazil at the end of May.
The executive order lifting the travel restrictions was one of several released by the White House on Monday as the final hours of Trump’s presidency wind down. Trump is also expected to grant a final slew of pardons before he leaves office on Wednesday.