Hospitals and health systems across the country are telling some Medicare and Medicaid patients that they can’t schedule telehealth appointments due to the federal government’s shutdown, now heading into its second week. That’s because Medicare reimbursement for telehealth expired on September 30, leaving health systems with the choice of pausing such visits or keeping them going in hopes of retroactive reimbursement after the shutdown ends.
Reimbursement for the Hospital at Home program, which allows patients to receive care without being admitted to a hospital, also lapsed with the shutdown. That led to providers scrambling to discharge patients under the program or admit them to a hospital. Mayo Clinic, for example, had to move around 30 patients from their homes in Arizona, Florida and Wisconsin to its facilities.
At issue in the government shutdown is healthcare, specifically tax credits for middle- and lower-income Americans that enable them to afford health insurance on the federal exchanges set up by the Affordable Care Act. Democrats want to extend those tax credits, which are set to expire at the end of the year, while Republicans want to reopen the government first and then negotiate about the tax credits in a final budget.
The impasse has prevented the Senate from overcoming a filibuster, despite a Republican majority. Around 24 million Americans get their health insurance through the ACA, and the loss of tax credits will cause their premiums to rise an average of 75%–and as high as 90% in rural areas–and likely cause at least 4 million people to lose coverage entirely.
The government’s closure has reverberated through its operations in healthcare. The Department of Health and Human Services has furloughed some 41% of its staff, making it harder to run oversight operations. CDC’s lack of staff will hinder surveillance of public health threats. And FDA won’t accept any new drug applications until funding is restored.
When the government might reopen remains unclear. Most shutdowns are relatively brief, but the longest one, which lasted 35 days, came during Donald Trump’s first term. Senate majority leader John Thune, R-S.D., and Speaker of the House Mike Johnson, R-La., have both said they won’t negotiate with Democrats, and the House won’t meet again until October 14.Bettors on Polymarket currently expect it to last until at least October 15. Pressure on Congress will increase after that date because there won’t be funds available to pay active military members.
The Supreme Court on Friday upheld a key Affordable Care Act requirement that insurance companies cover certain preventative measures recommended by an expert panel.
Justices upheld the constitutionality of the provision in a 6-3 decision and protected access to preventative care for about 150 million Americans.
The justices found that the secretary of the Department of Health and Human Services has the power to appoint and fire members of the U.S. Preventative Services Task Force (USPSTF).
The cases started when a small business in Texas and some individuals filed a lawsuit against the panel’s recommendation that pre-exposure prophylaxis (PreP) for HIV be included as a preventative care service.
They argued that covering PreP went against their religious beliefs and would “encourage homosexual behavior, intravenous drug use, and sexual activity outside of marriage between one man and one woman.”
The plaintiffs further argued that the USPSTF mandates are unconstitutional because panel members are “inferior officers” who are not appointed by the president or confirmed by the Senate.
While the panel is independent, they said that since their decisions impact millions of people members should be confirmed.
A U.S. district judge in 2023 ruled that all preventative-care coverage imposed since the ACA was signed into law areinvalid and a federal appeals court judge ruled in agreement last year.
The Biden administration appealed the rulings to the Supreme Court, and the Trump administration chose to defend the law despite its long history of disparaging Obamacare.
Though public health groups celebrated the ruling Friday, some noted another potential outcome.
“While this is a foundational victory for patients, patients have reason to be concerned that the decision reaffirms the ability of the HHS secretary, including our current one, to control the membership and recommendations of the US Preventive Services Task Force that determines which preventive services are covered,” Anthony Wright, executive director of Families USA, said in a statement.
“We must be vigilant to ensure Secretary Kennedy does not undo coverage of preventive services by taking actions such as his recent firing of qualified health experts from the CDC’s independent vaccine advisory committee and replacing them with his personal allies.”
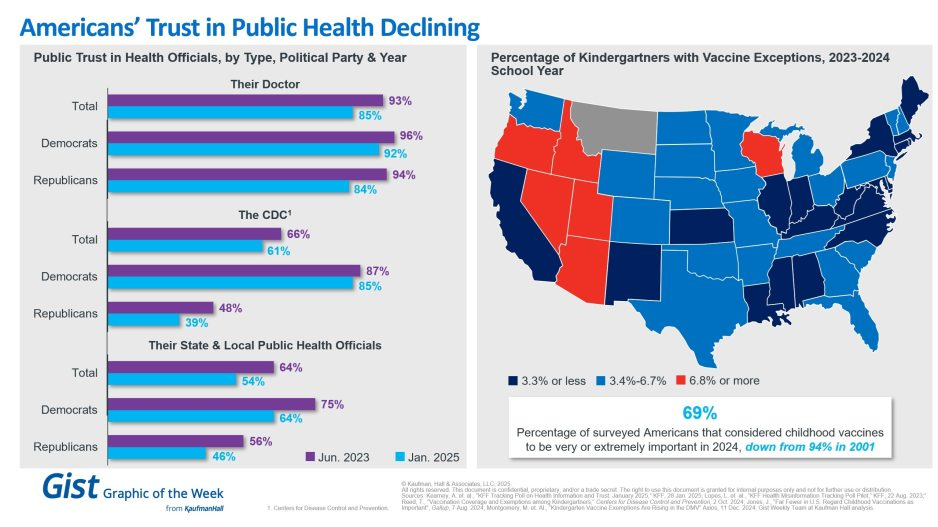
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
As seasonal virus activity surges across the United States, experts stress the importance of preventive measures – such as masking and vaccination – and the value of treatment for those who do get sick.
Tens of thousands of people have been admitted to hospitals for respiratory illness each week this season. During the week ending December 23, there were more than 29,000 patients admitted with Covid-19, about 15,000 admitted with the flu and thousands more with respiratory syncytial virus, or RSV, according to data from the US Centers for Disease Control and Prevention.
Nationally, Covid-19 levels in wastewater, a leading measure of viral transmission, are very high – higher than they were at this time last year in every region, CDC data shows. Weekly emergency department visits rose 12%, and hospitalizations jumped about 17% in the most recent week.
And while Covid-19 remains the leading driver of respiratory virus hospitalizations, flu activity is rising rapidly. The CDC estimates that there have been more than 7 million illnesses, 73,000 hospitalizations and 4,500 deaths related to the flu this season, and multiple indicators are high and rising.
RSV activity is showing signs of slowing in some parts of the US, but many measures, including hospitalization rates, remain elevated. Overall, young children and older adults are most affected.
“It’s a wave of winter respiratory pathogens, especially respiratory viruses. So it’s Covid, it’s flu, and we can’t diminish the importance of RSV,” said Dr. Peter Hotez, dean of the National School of Tropical Medicine at the Baylor College of Medicine. “So it’s a triple threat, and arguably a fourth threat because we also have pneumococcal pneumonia, which complicates a lot of these virus infections.”
Respiratory virus activity has been on the rise for weeks. Now, flu-like activity is high or very high in two-thirds of the United States, including California, New York City and Washington, as well as throughout the South and Northeast, according to the CDC.
“Remember, all of these numbers are before people got together for the holidays,” Hotez said. “So don’t be disappointed or surprised that we even see a bigger bump as we head into January.”
Vaccines can help prevent severe illness and death, but uptake remains low this season – despite a historic first, with vaccines available to protect against each of the three major viruses. Just 19% of adults and 8% of children have gotten the latest Covid-19 vaccine, and 17% of adults 60 and older have gotten the new RSV vaccine, CDC data shows. Less than half of adults and children have gotten the flu vaccine this season.
“We have, as a population, underutilized both influenza and the updated Covid vaccines, unfortunately,” said Dr. William Schaffner, an infectious disease expert at Vanderbilt University. “But it’s not too late to get vaccinated, because these viruses are going to be around for a while yet.”
According to the CDC, hospital bed capacity remains “stable” nationally, including within intensive care units. But with high levels of respiratory viruses, hospitals in at least five states are returning to requiring masks.
Mass General Brigham spokesman Timothy Sullivan said it will require masking for health-care staff who interact directly with patients starting Tuesday, and patients and visitors will be “strongly encouraged to wear a facility-issued mask.”
In Wisconsin, UW Health and UnityPoint Health – Meriter have expanded mask policies to cover more people. UW requires all staff, patients and visitors to wear a mask for patient interactions in clinic settings, including waiting areas and exam rooms.
UnityPoint Health – Meriter says masks continue to be required for team members and visitors in patient rooms.
Bellevue, a public hospital in New York City, said on social media last week that it had reinstated its mandatory masking policy due to an uptick in respiratory illnesses.
In Pennsylvania, the University of Pittsburgh Medical Center has required everyone to wear a mask when entering or inside since December 20. The systemwide masking policies were adjusted to “address the increase of respiratory virus cases” but may change when there is a “marked decrease in respiratory health cases,” according to the health care system.
An order posted last week by the Los Angeles County Health Officer requires all health-care personnel and visitors to mask while in contact with patients or in patient-care areas, based on the CDC’s categorization of Covid-19 hospital admission levels.
During the week ending December 23, more than 230 US counties were considered to have “high” levels of Covid-19 hospital admissions, defined by the CDC by at least 20 new hospital admissions for every 100,000 people. Nearly a thousand other counties, about a third of the country, have “medium” Covid-19 hospital admission levels, with at least 10 admissions for every 100,000 people.
Vaccines and masks can help reduce the risk of severe illness before getting sick, but treatments are also available to help prevent people from getting very sick if they do become infected.
Antiviral treatments for Covid-19, such as Paxlovid, and flu, such as Tamiflu, can be especially helpful for people who are more likely to get very sick, including people who are 50 or older and those with certain underlying conditions, such as a weakened immune system, heart disease, obesity, diabetes or chronic lung disease.
“If more people at higher risk for severe illness get treatment in a timely manner, we will save lives,” the CDC said in a recent blog post. But “not enough people are taking them.”
Seasonal respiratory virus activity can be hard to predict, but CDC forecasts suggest that hospitalization rates will continue at elevated levels for weeks and that this season, overall, will probably result in a similar number of hospitalizations as last season.
“One of the ways to help us all go into a happy new year is for us to be as protected as we can against these viruses,” Schaffner said.
“Of course, I continue to recommend vaccination, prudent use of the mask by high-risk people and, should you become sick, do not go to work and spread the virus further. Call your health care provider, because you may have some treatment available that will get you healthier sooner.”
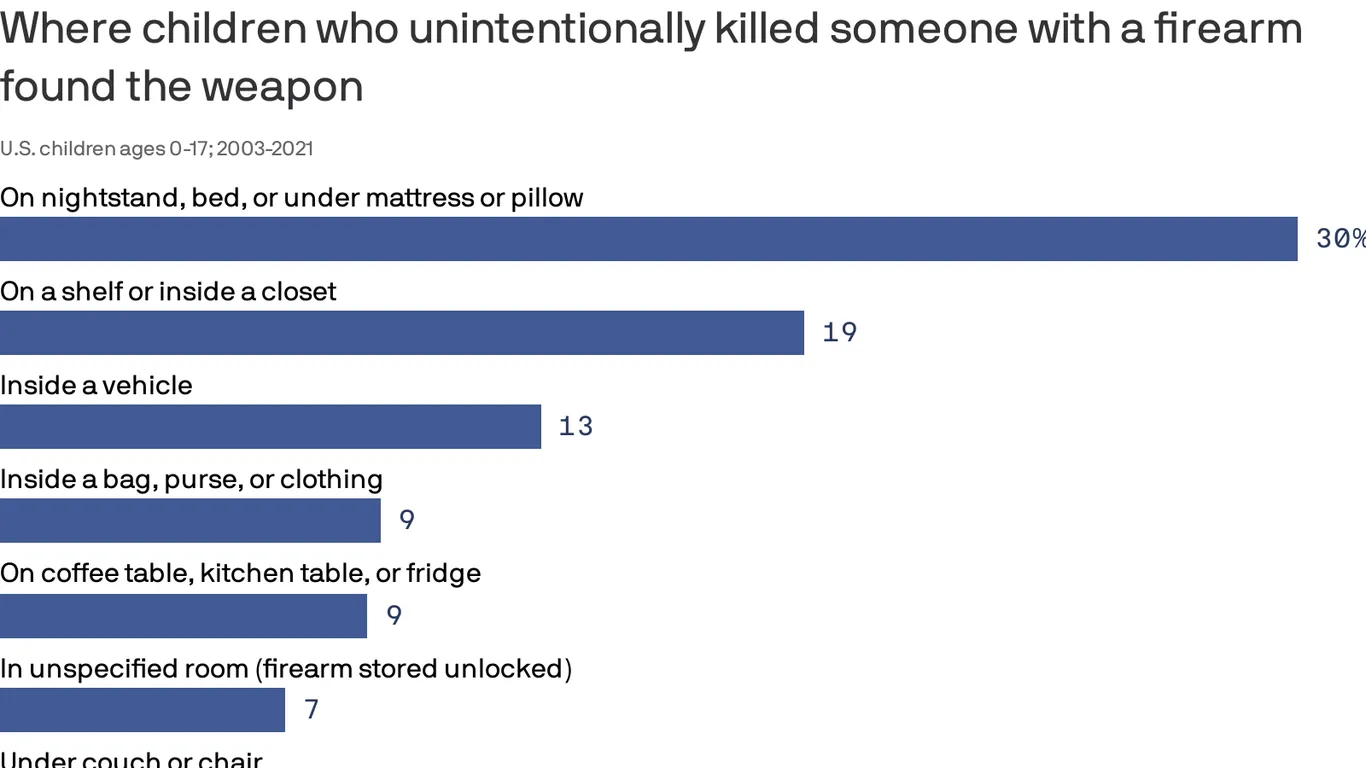
Children and teens involved in unintentional fatal shootings most commonly found the gun inside or on top of a nightstand, under a mattress or pillow, or on top of a bed, according to a new federal study.
Why it matters:
The data from the Centers for Disease Control and Prevention, which covers nearly 20 years of deadly firearm accidents among America’s youth, demonstrates why putting a gun out of sight or out of reach is not “safe storage,” federal researchers said.
It underscores the need for policymakers, health experts and parents to promote safe gun storage, they said.
Using data recorded between 2003 and 2021 by the National Violent Death Reporting System, researchers identified more than 1,250 unintentional gun deaths among kids.
The vast majority involved guns that were unlocked (76%), and most of those unlocked firearms were also loaded (91%).
Two-thirds (67%) of unintentional gun injury deaths among kids occurred when the shooter was playing with the gun or showing it to others.
In 30% of deaths, guns were found around nightstands and other sleeping areas.
Guns were also most commonly found on top of a shelf or inside a closet (18.6%) or inside a vehicle (12.5%).
On Monday, the Food and Drug Administration authorized new COVID vaccines from Moderna and Pfizer-BioNTech, and the Centers for Disease Control and Prevention followed Tuesday by recommending the shots be given as a single dose for most people five years of age and older. Children older than six months but younger than five, as well as completely unvaccinated people of any age, may be eligible for multiple doses.
These vaccines were formulated to target the XBB.1.5. variant,
which was the dominant strain in January but has since receded, although initial results suggest they remain effective against all currently circulating variants. Pharmacies and healthcare providers are expected to have the updated vaccines available by early next week.
The Gist: Due to the end of the COVID public health emergency in May, this COVID vaccination campaign will be the first not directly bankrolled by the federal government.
While insurers are still required to cover vaccinations without cost-sharing, the uninsured may find free shots, which the Biden administration says it will still provide at certain locations, harder to access.
Unlike past COVID boosters, reframing this shot as an annual vaccine that patients receive along with their flu shots should help with the rollout, as around 50 percent of Americans got a flu shot in 2022 while only 17 percent received the bivalent COVID booster.
With COVID cases and hospitalizations currently rising, promoting widespread uptake is critical to dampening a likely winter COVID spike.
However, public health officials will have to overcome many Americans’ wearied indifference toward COVID to motivate them to get vaccinated.
Influential conservative policy groups are sketching out health care plans for a potential Republican administration over a year before the election.
Why it matters:
Republicans have moved on from the “repeal and replace” — the Affordable Care Act didn’t even get a mention in the first GOP presidential debate last week — but still haven’t settled on new health care agenda.
Republican-aligned groups are stepping in to build out ideas for a party platform that may not be as ambitious as an ACA replacement but could still shift health care policy in a conservative direction on everything from Medicaid to abortion to public health.
Context:
The early push to define the next GOP health agenda partly stems from Republicans’ inability to agree on an ACA alternative after former President Trump was elected, despite years of promises to overhaul the 2010 health care law. The GOP policy experts also said they want to avoid repeating the Trump administration’s failure to plan health care executive actions and key staffing decisions before taking office.
“A large part of it comes from the experience of 2017. There wasn’t a clear agenda that was ready to go,” said Brian Blase, a former Trump administration health official who’s now president of the right-leaning Paragon Health Institute.
Details:
Conservative think tanks are looking to advance some long-held conservative goals like transforming Medicaid’s open-ended entitlement into block grants, but there’s also a new generation of Trump alumni who hope to revive some of his administration’s policies.
These include initiatives like encouraging businesses to form association health plans, and pushing even further on price transparency and curbing higher payments to hospitals’ outpatient departments.
Some are also drawing up plans for limiting the CDC’s power over public health policy in reaction to what they view as the agency’s failed response to the COVID-19 pandemic.
Zoom in:
Paragon Health, as well as the Heritage Foundation and America First Policy Institute, are the primary conservative think tanks now drafting health regulations, policy plans and recruiting personnel who could serve in a Republican administration.
A roadmap from Paragon envisions a burst of rulemaking at the beginning of a new administration, mostly through the Department of Health and Human Services.
Meanwhile, the America First Policy Institute, founded by Trump administration alumni in 2021, has put forward a 12-part health policy agenda it describes as “radical incrementalism.”
That’s an acknowledgement that they’re not planning a major health care overhaul, but a belief that significant changes are possible in the current structure, said former Louisiana Gov. Bobby Jindal, who chairs the group’s health policy division.
“We are advocating specific policies that try to reform our health care system in a very specific direction that empowers patients … that makes health care more affordable, accessible, that improves outcomes by giving control back to individual patients working with their providers, not government agencies and programs. But, we’re not trying to write the next 3,000-page bill,” Jindal said.
Some of those incremental ideas they hope could get bipartisan support, such as broadening health savings accounts for those with chronic conditions, expanding telehealth flexibilities for providers across state lines, implementing transparency for pharmacy benefit managers and speeding up deployment of biosimilars.
The Heritage Foundation has also detailed policy proposals and recently joined more than 70 other conservative groups to launch an initiative called Project 2025 to develop a governing agenda.
One of those Heritage policy proposals laid out earlier this year illustrates how a future GOP president could overhaul HHS.
Heritage’s plan contains the most detailed ideas for how the next GOP president — who would be the first since the demise of Roe v. Wade — could implement anti-abortion policies, cut off Medicaid funding to Planned Parenthood, and roll back Biden administration initiatives aimed at increasing access to abortion.
The group also envisions splitting CDC into two agencies — one for research and data collection and another for making public health recommendations with “severely confined ability” to influence policy.
What we’re watching: The GOP presidential candidates themselves have said relatively little so far about their plans for the health care system. That could eventually change, given Americans’ concern over health care costs.
In just 2020, deaths from gun violence cost the U.S. healthcare system $290 million, or about $6,400 per patient, according to a report from the Commonwealth Fund. These costs are mostly covered by Medicaid and other government insurance programs.
The U.S. healthcare system sees about 30,000 inpatient hospital stays and 50,000 emergency room visits due to gun violence each year, leading to more than $1 billion in initial medical costs, according to a new analysis.
The Commonwealth Fund published these results last week and relied on three data sources for its analysis: the 2019 Global Burden of Disease study, the Small Arms Survey and the U.S. Government Accountability Office.
Even after leaving the hospital, patients are faced with challenges. A year after a gun injury, medical spending rises about $2,495 per person per month. In addition, those who suffer firearm injuries are more likely to form mental health challenges and substance use disorders.
“The impact of gun violence reaches far beyond the hospital room,” the analysis states.
Firearm-related deaths are increasing, according to the Centers for Disease Control and Prevention. In 2021, almost 49,000 Americans died from firearms, compared to 45,000 in 2020.
Additional findings from the report include:
In 2019, the U.S. had a higher rate of firearm deaths than any other country. Its rate of firearm deaths was almost five times as much as France, the second-highest country.
Eight times more people in the U.S. died from firearm violence in 2019 compared to Canada, the second-highest country.
More people died from self-harm by firearm in the U.S. than any other country in 2019, more than three times higher than France and Switzerland.
More women were killed by guns in the U.S. than any other country in 2019.
In the U.S., there are 67 million more firearms than people. That difference is higher than the population of the United Kingdom, which has 66.2 million people.
In the U.S., 52% of people who are admitted to hospitals for firearm injuries are Black, 29% are White, 14% are Hispanic and 5% are another race or ethnicity. Black Americans account for 50% of firearm injury hospital costs, while White Americans account for 27%, Hispanic Americans account for 17% and other races or ethnicities account for 6%.
About 48% of firearm-related inpatient hospital stays are in the American South, while 20% are in the Midwest, 20% are in the West and 12% are in the Northeast. The South accounts for 44% of firearm injury hospital costs, while the West accounts for 26%, the Midwest accounts for 18% and the Northeast accounts for 11%.
China is in the middle of what may be the world’s largest covid-19 outbreak after authorities abruptly loosened almost three years of strict pandemic restrictions in December following nationwide protests against the measures.
The sudden dismantling of China’s “zero covid” regime — enforced through mass lockdowns, testing and contact tracing — has left the country’s health system unprepared and overwhelmed. It has alarmed international health experts concerned about Beijing’s transparency and caused diplomatic friction as countries enforce travel restrictions on arrivals from China.
How many people have been infected?
So far, there are no reliable national figures for the number of people among China’s 1.4 billion population who have been infected in the current outbreak. After admitting the difficulty of tracking infections, China’s National Health Commission stopped reporting daily tallies in December.
The data is still maintained by the Chinese Center for Disease Control and Prevention, based on counts from hospitals and local health commissions. But because mandatory mass testing has been dropped, the official figure is believed to massively underestimate the rate of infection. As of Jan. 8, there have been a little more than 500,000 confirmed covid cases since the pandemic began, according to the CDC.
Statements from local governments indicate that the true number of infections is exponentially higher. Officials in Henan province estimated this week that 89 percent of the province’s 99 million residents have been infected. In Zhejiang province, officials said the province was seeing over a million new infections a day in late December. As of Jan. 8, all 31 provinces, municipalities and regions had reported covid infections, according to the CDC.
How serious is the outbreak?
The number of deaths remains unknown, even as evidence is mounting that the true death count is much higher than what has been reported — a little more than 5,200 deaths since the pandemic began and fewer than 40 since zero-covid restrictions were lifted on Dec. 7.
As of Dec. 25, the takeup of intensive care beds in secondary and tertiary hospitals across the country was about 54 percent, but that figure has since increased to 80 percent, Jiao Yahui, director of the Department of Medical Affairs of the National Health Commission, said in an interview with state broadcaster CCTV on Sunday.
Officials reassured the public by noting that the fatality rate of the coronavirus’s omicron variant is 0.1 percent. The current outbreak has mostly consisted of the omicron subvariants BA.5.2 and BF.7, the State Council Information Office said in a news conference Monday.
The lack of testing combined with the narrow definition of what counts as a covid death — positive patients who die of respiratory failure — continue to skew the statistics. Officials have said they will investigate fatalities and release the results in the future.
What is the government saying?
Authorities say the worst of the outbreak is over for Chinese cities where infections spread quickly in December. Now, they are preparing for a new surge in rural areas around the upcoming Lunar New Year holiday that begins Jan. 21.
State media has reported that cases in most major cities have started to decline. Yin Yong, acting mayor of Beijing, told CCTV on Monday that the city had reached its peak and that authorities were turning their focus to monitoring potential new coronavirus variants or subvariants of omicron, and to mitigating the impact of covid on the elderly and other vulnerable groups.
Officials also said the peak had been reached in the province of Jiangsu in late December, while in Zhejiang, authorities said, “the first wave of infections has passed smoothly,” according to Health Times, a publication managed by People’s Daily. The state-run Farmers’ Daily said that visits to 51 villages across 31 provinces showed that most residents had been infected and had recovered.
Data released by Baidu, the main search engine in China, showed that the number of searches related to covid symptoms and medical supplies had dropped since peaking in mid-December.
Yet in Henan, officials said hospitals remain overcrowded because of a rise in critical cases in the past week. Researchers at the Institute of Public Health at Nankai University in Tianjin, using data from fever clinics, project that the nationwide peak will be between Dec. 20 and Jan. 15, with two smaller peaks in the first half of this year.
Officials have predicted a second wave over the Lunar New Year holiday, when the total number of passenger trips by residents is expected to reach 2.1 billion as pent-up demand for travel is unleashed. At this point, more contagion could spread to rural areas, where severe shortages of anti-fever drugs and medical staff have been reported.
How did zero covid affect the outbreak?
China’s pursuit of zero covid, eliminating the spread of the virus through lockdowns, mandatory quarantines, travel restrictions and mass testing, has proved to be a double-edged sword. While the approach kept infections and death rates low throughout most of the pandemic, it left the Chinese population with little natural immunity to the virus.
Many elderly residents — already skeptical of vaccines, which have had a troubled past in China — did not get vaccinated, feeling that they would be protected by the zero-covid strategy. Only 40 percent of residents above the age of 80 have had booster shots.
Under China’s covid policy, the population was immunized with domestically made vaccines that are not as effective against the omicron variant as mRNA vaccines. China has yet to approve foreign mRNA vaccines, and a domestically made one is still under production.
What does this mean for the rest of the world?
Concerns about the possibility of a new variant emerging in China have prompted countries including the United States, Japan and South Korea, and many European countries, to require extra screening for arrivals from China.
Wu Zunyou, the chief epidemiologist at the CDC, told CCTV in a report published Sunday that no new variants have emerged and that new strains are being collected every day to monitor changes.
“All the strains we found so far have already been shared with international sharing platforms,” he said. “They are the ones either reported abroad, or have been introduced to China after spreading overseas. So far, no newly emerged mutated strains have been found in China.”
The World Health Organization has called on China to share more real-time data on the outbreak. Michael Ryan, the health emergencies director, said at a news conference in Geneva on Wednesday that the WHO “still believes that deaths are heavily underreported from China.” He added: “We still do not have adequate information to make a full comprehensive risk assessment.”
Beijing has criticized travel restrictions on people arriving from China imposed by other countries as “ridiculous” and politically motivated. It has threatened countermeasures and this week suspended short-term visas for Japanese and South Korean citizens.
Hospitals across the country are being hit with a spike in respiratory syncytial virus (RSV) and influenza cases, while still dealing with a steady flow of COVID admissions, in what’s been dubbed a “tripledemic”. The graphic above uses hospitalization data from the Centers for Disease Control and Prevention (CDC) to show that each disease has been sending similar shares of the population to hospitals across late fall, with flu hospitalizations having just overtaken COVID admissions after Thanksgiving.
These numbers reflect that we’re experiencing the worst RSV season in at least five years, and we’re set to endure the worst flu season since 2009-10.As RSV is most severe in very young children, its recent surge has revealed another capacity shortage in our nation’s hospitals: pediatric beds. From 2008 to 2018, pediatric inpatient bed counts fell by 19 percent, as hospitals shifted resources to higher revenue services.
This strategy has now come to a head in many parts of the country, as RSV has driven pediatric bed usage rates to a recent high. (The Department of Health and Human Services’ pediatric capacity data only dates back to August 2020.) With three straight weeks of declining RSV hospitalizations, there is reason to hope that pediatric care units will soon feel a reprieve. However, flu season has yet to reach its peak, prompting calls for a return to widespread mask-wearing and a renewed emphasis on flu shots, given that more than half of Americans have not yet gotten vaccinated this season.