Since the Affordable Care Act (ACA) was signed into law a little more than a decade ago, it has fundamentally reshaped the American healthcare system. As the graphic below highlights, the far-reaching law expanded insurance coverage, increased consumer protections, led to new payment models, established minimum coverage standards, reformed the Indian Health Service—and even gave us calorie counts on menus, among myriad other things.
The fate of the ACA is once again in the Supreme Court’s hands—and the nine Justices, now including Amy Coney Barrett, are scheduled to hear arguments starting November 10th. Eighteen states with Republican leadership are asking the court to determine whether the individual mandate is constitutional without a financial penalty, and whether the mandate is severable from the rest of the law.
The process of unwinding a law that touches nearly every facet of the US healthcare system would mean a confusing and financially detrimental road ahead for many.Although we believe it’s unlikely that the entire law will be ruled unconstitutional, if it is—and no replacement legislation is passed—the effects could be devastating.
An estimated 21 million people would be at serious risk of losing their health insurance. This risk is magnified for Hispanic and Black Americans, who are also hardest hit by COVID-19. As many as 133M people with pre-existing conditions could face insurance disqualification or significantly higher premiums.
The lost coverage would result in a significant revenue hit for doctors and hospitals. While the impact would vary by state depending on Medicaid expansion terms, an Urban Institute report projects that total uncompensated care would grow an average of 78 percent for hospitals and 68 percent for physician services if the ACA is struck down. Although the Court is not expected to rule on the fate of the law until mid-2021, the direction and pace of future health reform legislation will be set by the ruling, under either a Trump or Biden administration.
The upcoming election has huge implications for healthcare, far beyond how COVID is managed, ranging from how care is covered to how it’s delivered. The graphic above shows a continuum of potential policy outcomes of the November 3rd vote.
If President Trump wins a second termand Republicans control at least one house of Congress, there will likely be more attempts to dismantle the ACA, as well as continued privatization of Medicare coverage.
If Democrats win the presidency and sweep Congress, actions to expand the Affordable Care Act (ACA), or even create a national public option, are on the table—although major healthcare reform seems unlikely to occur until the second half of a Biden term.
In the short term, we’d expect to see more policy activity in areas of bipartisan agreement, like improving price transparency, ending surprise billing and lowering the cost of prescription drugs, regardless of who lands in the White House.
While healthcare emerged as the most important issue for voters in the 2018 midterm elections, the COVID pandemic has overshadowed the broader healthcare reform platforms of both Presidential candidates heading into the election. As shown in the gray box, many Americans view the election as a referendum on the Trump administration’s COVID response. Managing the pandemic is one of the most important issues for voters, especially Democrats, who now rank the issue above reducing the cost of healthcare or lowering the cost of drugs.
In many aspects, the COVID policies of Biden and Trump are almost diametrically opposed, especially concerning the role of the federal government in organizing the nation’s pandemic response.
The next administration’s actions to prevent future COVID-19 surges, ensure safe a return to work and school, accelerate therapies, and coordinate vaccine delivery will remain the most important aspect of healthcare policy well into 2021.
This week Nebraska became the latest state to receive waiver authority from the Trump administration to implement work requirements as part of its Medicaid expansion program.
The program, called “Heritage Health Adult”, will be a two-tiered system, with expansion-eligible adults choosing between “Basic” and “Prime” coverage levels. The lower tier will provide coverage for physical and behavioral health services, with a prescription drug benefit, and is open to adults not eligible for traditional Medicaid with incomes under 138 percent of the federal poverty line.
“Prime” enrollees will get additional dental, vision, and over-the-counter drug benefits, in exchange for agreeing to 80 hours per month of work, volunteering, or active job seeking, which must be reported to the state.
Nebraska voters approved the Medicaid expansion two years ago, although enrollment only began this August, and the work-linked demonstration project is slated to start next year. An estimated 90,000 additional Nebraskans are expected to enroll in Medicaid under the expanded program.
The approval of Nebraska’s Medicaid work requirement comes a week after the Trump administration approved a partial expansion of Medicaid in Georgia, called “Pathways to Coverage”, which is also tied to a requirement to seek or engage in employment or education activities.
The Georgia program also requires premium payments by eligible adults who make between 50 and 100 percent of the federal poverty line. Court challenges will inevitably ensue for both the Nebraska and Georgia programs—only Utah has successfully implemented Medicaid work requirements, with 16 other state programs either pending approval, held up in court, or awaiting implementation. We continue to be deeply skeptical of Medicaid work requirements, and believe they only serve to deter those who would otherwise qualify for coverage from enrolling, and that the expense of their implementation and ongoing operation often outweighs any savings to the state.
The argument that “work encourages health”, often advanced by proponents of work requirements, gets it exactly backwards—rather, health security encourages work, a reality that has become ever more urgent as the COVID pandemic has drawn on.
As the economy continues to falter, Medicaid’s importance as a safety net program grows ever greater, and work requirements create an unhelpful obstacle to basic healthcare access.
President Trump repeated baseless claims at the final presidential debate that the coronavirus “will go away” and that the U.S. is “rounding the turn,” while Joe Biden argued that any president that has allowed 220,000 Americans to die on his watch should not be re-elected.
Why it matters: The U.S. is now averaging about 59,000 new coronavirus infections a day, and added another 73,000 cases on Thursday, according to the Covid Tracking Project. The country recorded 1,038 deaths due to the virus Thursday, the highest since late September.
What they’re saying: “More and more people are getting better,” Trump said. We have a problem that’s a worldwide problem. This is a worldwide problem. But I’ve been congratulated by the heads of many countries on what we’ve been able to do … It will go away and as I say, we’re rounding the turn. We’re rounding the corner. It’s going away.”
Trump later disputed warnings by public health officials in his administration that the virus would see a resurgence in the winter, claiming: “We’re not going to have a dark winter at all. We’re opening up our country.”
Biden responded: “Anyone responsible for that many deaths should not remain as president of the United States of America.”
“What I would do is make sure we have everyone encouraged to wear a mask all the time. I would make sure we move in the direction of rapid testing, investing in rapid testing.”
“I would make sure that we set up national standards as to how to open up schools and open up businesses so they can be safe and give them the wherewithal, the financial resources, to be able to do that.”
The bottom line:Biden and Trump are living in two different pandemic realities, but Biden’s is the only one supported by health experts.
As the presidential election draws near, we reflect on the meaningful differences in health policy priorities and platforms between the two candidates, which we’ve described more fully in our recent blog series.
While similarities exist in some areas — most notably prescription drug pricing and proposals to control health care costs — the most striking differences between the positions taken by President Donald Trump and those of former Vice President Joe Biden are on safeguarding access to affordable health care coverage, advancing health equity for those who have been historically disadvantaged by the current system, and managing the novel coronavirus pandemic.
The importance of maintaining or expanding access to affordable health care in the midst of a pandemic cannot be understated. Going into the crisis, 30 million Americans lacked health coverage, with many more potentially at risk as a result of the current economic downturn. And even for many with coverage, costs are a barrier to receiving care. Moreover, despite efforts by Congress and the Trump administration to ease the financial burden of COVID-19 testing and treatment, many people remain concerned about costs; examples of charges for COVID-related medical expenses are not uncommon.
In this context, President Trump’s efforts to repeal the Affordable Care Act (ACA) is the most important signal of his position on health care. The administration’s legal challenge of the law will be considered by the Supreme Court this fall. With no Trump proposal for a replacement to the ACA, if the Court strikes the law in its entirety or in part, many voters cannot be certain that their health coverage will be secure. By undermining the ACA — the vast law that protects Americans with preexisting health conditions and makes health coverage more affordable through a system of premium subsidies and cost-sharing assistance — the president has put coverage for millions at risk.
Trump issued an executive order to preserve preexisting condition protections. If the ACA remains intact, the order is redundant. But if the ACA is repealed by the Court, the order is meaningless because it lacks the legal underpinning and legislative framework to take effect.
In contrast, Vice President Biden has proposed expanding coverage through the ACA by adding a public option, enhancing subsidies to make health care more affordable, filling the gap for low-income families living in states that did not expand Medicaid, and giving people with employer health plans the option to enroll in marketplace coverage and take advantage of premium subsidies. For sure, if Biden is elected, many policy details must be ironed out; passing legislation in a deeply divided Congress is never easy. Despite these challenges, Biden proposes expanding health coverage rather than revoking it.
Just as COVID-19 has exposed gaps in health coverage and affordability, it also has highlighted the poor health outcomes stemming from racial and ethnic inequities in the U.S. health system. Communities of color — Black, Hispanic, and American Indian and Alaska Native people — have higher rates of COVID cases, hospitalizations, and deaths compared to white people. These disparities are a result of myriad factors, many of which are deeply rooted in structural racism. The candidates’ plans to address health disparities and advance health equity set them apart.
The ACA has played a critical role in reducing disparities in access to health care and narrowed the uninsured rate among Black and Hispanic people compared to white people. Medicaid expansion has been key to improving racial equity. Repealing the ACA, as President Trump has sought to do, would reverse these gains. Even beyond repealing the ACA, this administration has pursued policies intended to limit Medicaid eligibility — for example, by permitting states to impose work requirements and other restrictions that would lead to fewer people covered. These measures and others are already having an impact; coverage gains achieved through the ACA have eroded since 2016. Health care for legal immigrants also has declined as a result of policies like the recently finalized “public charge” rule, which seems also to have caused an increase in uninsurance among children. The administration has further revoked ACA antidiscrimination and civil rights protections for LGBTQ people.
In addition to restoring and expanding coverage under the ACA, Vice President Biden has pledged to address health disparities and reinstate antidiscrimination protections. He has a proposal to advance racial equity not just in health care but across the economy. If successful, his plan could address underlying factors contributing to higher rates of COVID-19 cases and deaths among people of color, as well as their higher rates of heart disease, diabetes, and other health conditions tied to social determinants of health.
Finally, the candidates differ deeply in their approaches to the coronavirus pandemic. President Trump has failed to orchestrate a national strategy for combating coronavirus and has routinely undermined accepted public health advice with respect to mask-wearing and social distancing. He has delegated to the states responsibility for controlling the pandemic when it is clear that the virus travels freely across the country, regardless of state borders. Lax states can negate the efforts of those states sacrificing to bring the pandemic under control. Vice President Biden has strongly signaled, though his personal conduct and rhetoric, that he intends more aggressive federal leadership in fighting the virus.
In a recent Commonwealth Fund survey of likely voters, control of the pandemic and covering preexisting conditions were very important factors in choosing a president. In seven battleground states, protections for preexisting conditions outweighed COVID-19 and health costs as the leading health care issue voters are considering. In all 10 battleground states included in the survey, Vice President Biden was viewed as the more likely candidate to address these critical health care issues.
Perhaps since the Civil War, the United States has never faced starker choices in a presidential election. In health and other areas, there are profound differences in the positions of President Trump and former Vice President Biden. Voting this November is literally a matter of life and death for the American people.
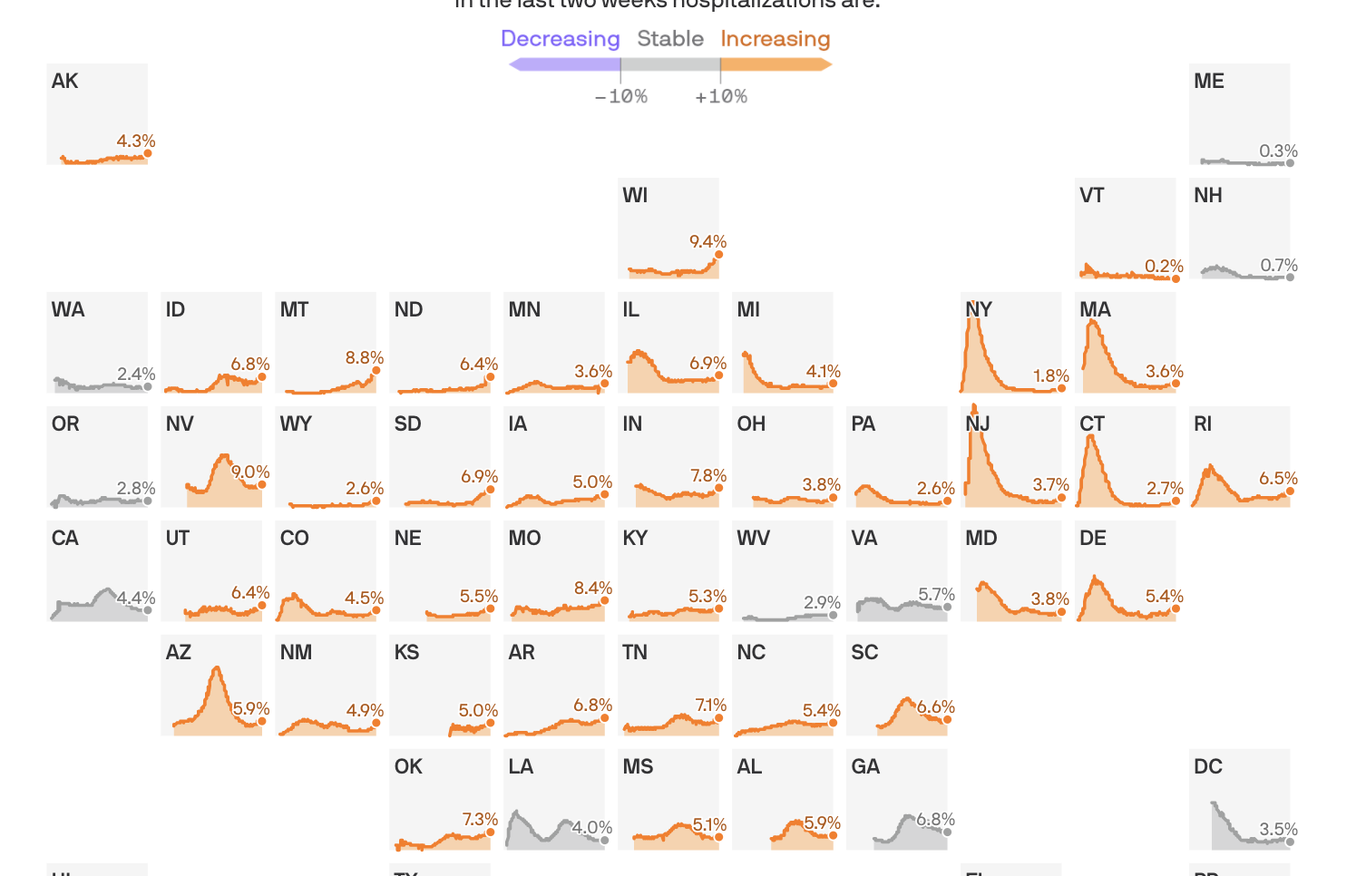
Share of hospital beds occupied by COVID-19 hospitalizations
States shown from first date of reported data, from March 17 to Oct. 17, 2020
In the last two weeks hospitalizations are:
Coronavirus hospitalizations are increasing in 39 states, and are at or near their all-time peak in 16.
The big picture: No state is anywhere near the worst-case situation of not having enough capacity to handle its COVID-19 outbreak. But rising hospitalization rates are a sign that things are getting worse, at a dangerous time, and a reminder that this virus can do serious harm.
By the numbers: 39 states saw an increase over the past two weeks in the percentage of available hospital beds occupied by coronavirus patients.
Wisconsin is faring the worst, with 9.4% of the state’s beds occupied by COVID patients.
Sixteen states are at or near the highest hospitalization rates they’ve seen at any point in the pandemic.
Yes, but: The all-time peak of coronavirus hospitalizations happened in the spring, when 40% of New Jersey’s beds were occupied by COVID patients. Thankfully, even the the worst-performing states today are still a far cry from that.
Between the lines:These numbers, combined with the nationwide surge in new infections, confirm that the pandemic in the U.S. is getting worse — just as cold weather begins to set in in some parts of the country, which experts have long seen as a potentially dangerous inflection point.
They also suggest that most parts of the country won’t need to pause or scale back non-coronavirus treatments, as hospitals did in the spring when no one was quite sure how bad things could get.
In rural areas, however, even a modestly sized outbreak can strain local hospital capacity.