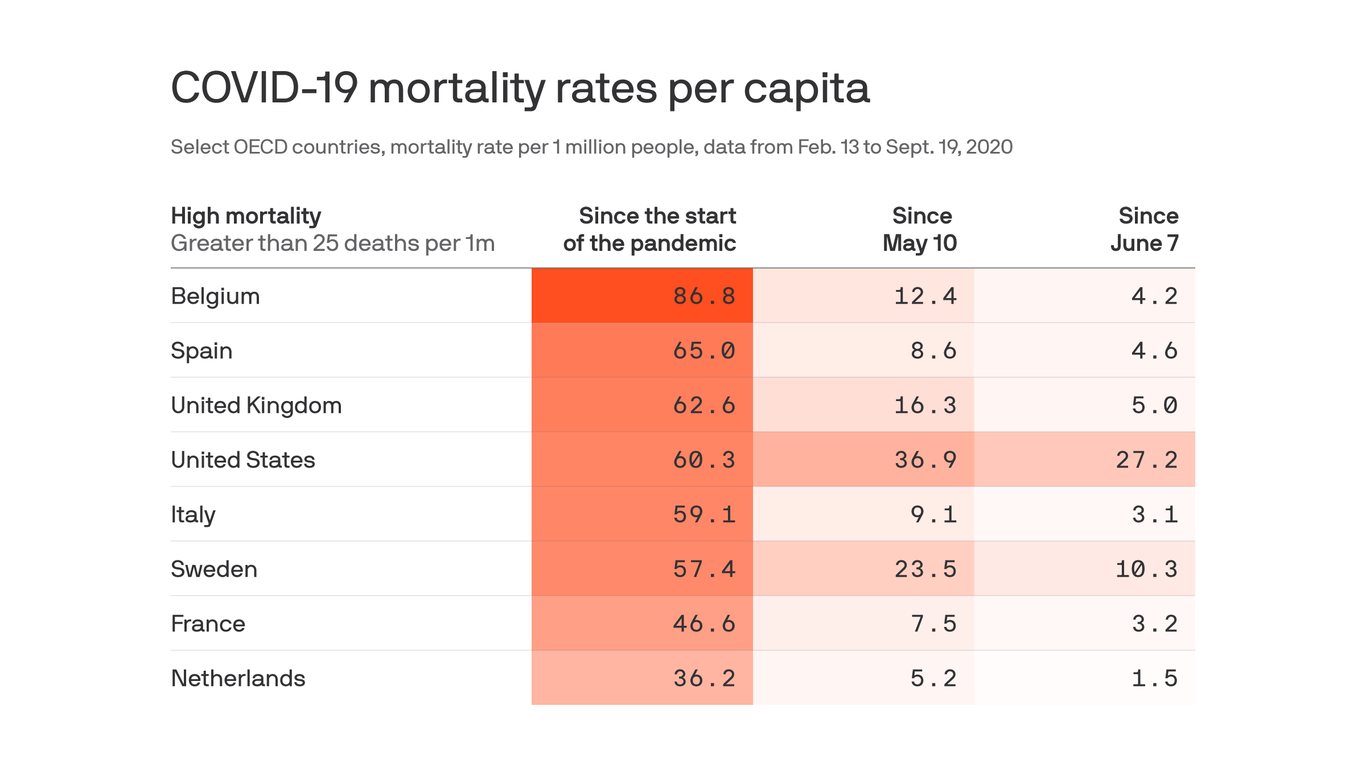
Although other wealthy countries have higher overall coronavirus mortality rates than the United States, the U.S. death rate since May is unrivaled among its peers, according to a new study published in JAMA.
Between the lines:After the first brutal wave of outbreaks, other countries did much better than the U.S. at learning from their mistakes and preventing more of their population from dying.
Why it matters:“If the U.S. had comparable death rates with most high-mortality countries beginning May 10, it would have had 44,210 to 104,177 fewer deaths,” the authors conclude.
Excess deaths have followed a similar pattern: The hardest-hit European countries had similar or higher rates of excess deaths of all causes to the U.S. early on, but these fell much lower than the America did after the first wave.
Yes, but: Death rates are not static, as this study proves, and outbreaks in several European countries have taken a turn for the worse lately.
The head of the World Health Organization said Monday that allowing the novel coronavirus to spread in an attempt to reach herd immunity was “simply unethical.”
The remark was a sharp rebuke of the approach amid mounting new infections around the world. Recent days have seen the most rapid rise in cases since the pandemic began in March.
“Never in the history of public health has herd immunity been used as a strategy for responding to an outbreak, let alone a pandemic,” WHO Director-General Tedros Adhanom Ghebreyesus said at a Monday media briefing. “It is scientifically and ethically problematic.”
In a public health context, herd immunity typically describes a scenario in which a large enough share of the population is vaccinated against a disease to prevent it from spreading widely, thereby providing default protection to a minority of people who have not been vaccinated.
But as there is still no vaccine for the coronavirus, achieving herd immunity in the current environment would require a large number of people to contract the virus, survive covid-19, and then produce sufficient antibodies to provide long-term protection.
While the scientific community has roundly rejected herd immunity the approach, public interest in it has waxed and waned amid pressure to reopen schools and economies.
Last month, President Trump appeared to praise the idea during a town hall in Pennsylvania.
“You’ll develop herd — like a herd mentality,” he said. “It’s going to be — it’s going to be herd developed — and that’s going to happen.”
British Prime Minister Boris Johnson’s government initially expressed interest in the theory before backtracking amid public outcry over the dangers of letting the virus spread. Johnson himself was hospitalized with a severe case of covid-19, which he said could have killed him.
Tedros, noting that there had been “some discussion” about the concept recently, told reporters Monday that allowing people to be exposed to a deadly virus whose effects are still not fully known was “not an option.”
“Most people who are infected with the virus that causes covid-19 develop an immune response within the first few weeks, but we don’t know how strong or lasting that immune response is, or how it differs for different people,” he said.
Though rare, there are multiple documented instances of people being infected for a second time after recovering from covid-19. An 89-year-old woman in the Netherlands died after being infected with the coronavirus for a second time, Dutch news reported Monday.
Antibody studies suggest that less than 10 percent of people in most countries have contracted covid-19, Tedros said, which is nowhere near the majority that would be needed for herd immunity.
With the “vast majority” of the world’s population susceptible, letting the virus spread “means allowing unnecessary infections, suffering and death,” he said.
Just in the last four days, Tedros said Monday, the global coronavirus count has continued to break its daily record for the number of new confirmed infections.
“Many cities and countries are also reporting an increase in hospitalizations and intensive care bed occupancy,” he added.
Tedros has urged governments to pursue comprehensive plans that include widespread testing, social distancing, and other preventive measures, such as face-mask wearing, alongside a global push to develop a vaccine. The WHO is spearheading an effort to distribute coronavirus vaccines equitably once they are available, which Trump declined to join.
What is the probability of testing positive for Covid-19 before you get symptoms? Scientists really don’t know.
Vice President Mike Pence has not tested positive for SARS-CoV-2, the virus that causes Covid-19. But he’s been in close contact, in recent days, with people with confirmed Covid-19 infections. And he debated Sen. Kamala Harris last night. Was this a good idea?
In a word: No. Per the Centers for Disease Control and Prevention’s own guidelines, Pence should have been quarantining, not debating, even if he’s testing negative. (That said, CDC director Robert Redfield had cleared Pence to debate.)
Since the Trump administration’s actions over the last 11 days have muddied the message from public health experts, let’s be clear: A negative test is not an all-clear for doing risky activities during the pandemic.
Scientists don’t yet understand exactly when a person who is infected with the coronavirus will start testing positive for the virus. There are situations when a person could test negative, actually be infected, and also be contagious. It’s also possible — since this virus multiplies itself exponentially in the body very, very quickly — that someone could test negative in the morning (and not be contagious), but by the afternoon test positive (and be very contagious).
Confusing? Yes, it is. But the bottom line is that Covid-19 diagnostic tests (both the slower, more common, viral genetic test — called RT-PCR— and the more rapid viral protein test, called an antigen test) are most useful, and most accurate, when used on people experiencing symptoms.
“One of the huge gaps now in the data is: What is the probability of testing positive before you get symptoms?” Benny Borremans, a disease ecologist at UCLA, says. Right now, scientists just don’t know for sure.
Why testing is less accurate before symptoms begin
There are several reasons scientists are unsure about when in an infection people will start testing positive for SARS-CoV-2. To understand why, and to make this less confusing, it’s helpful to think through all the things that have to happen for a Covid-19 test to come back positive.
First, the virus needs to take its time to establish itself in a person’s body. This is called the incubation period, and it can take upward of two weeks. On average, this happens in about five or six days. During the incubation period, a person might not test positive for the virus because there’s not enough virus in their body to detect in a test.
“The virus particles, day by day, will multiply,” Muge Cevik, a virologist and physician at the University of St. Andrews, says. “The virus needs to reach a threshold for the PCR [i.e. viral genetic] tests to pick it up.” PCR is the more common Covid-19 diagnostic test because it requires a lower threshold of the virus to test positive; rapid antigen tests would require a higher level of virus to register a positive test.
Testing positive should coincide with being contagious. But not always.
Generally, a person can start being infectious for the virus around two days before they start to show symptoms, in what’s known as the presymptomatic phase.
And, generally — but not always — scientists would expect that if a person is contagious, they’d test positive. After all, if they’re spewing enough virus out to get another person sick, they’re probably spewing enough virus out for a diagnostic test to pick up on.
But there are a few wrinkles here: When exactly a person makes the jump from testing negative and being non-infectious to testing positive and being infectious is hard to predict.
“If everything works as it should, the test should be positive if you are infectious at the very moment of the test, as there must be virus present then,” Justin Lessler, an epidemiologist at Johns Hopkins University, says. “However, you could easily test negative then become infectious a day, or even hours, after the test.” Unless you’re testing every hour, it’s impossible to get a fine-grained view on when the infectious period truly begins. (Also possible, but probably rarer: A person tests positive before they start to be contagious.)
Even if a person is contagious, they may not test positive. It could come down to where the sample for testing was taken from.
In general, “we consider the gold standard to be the nasopharyngeal swab,” Bobbi Pritt, the director of clinical microbiology at the Mayo Clinic, says. “That’s the deep nasal swab that goes all the way back into the back of your nose. Whereas other specimens — like a throat swab or just the very outer edge of your nose, like right inside your nostril — that’s not going to contain as much virus.”
Early on in the infection, a person who is incubating the virus is expected to test negative. Over the summer, Johns Hopkins researchers — including Lessler — published a paper estimating the likelihood of a false negative test in the first few days after being exposed to the virus. On the first day, they found the chance of a false negative is near 100 percent. No test is going to find the virus so early. Through the first four days, that rate drops to 67 percent on day four, on average, but with a very large range of error. On the day people first reported symptoms, there’s still a significant false negative rate, at 38 percent.
What does this all add up to? “What we’re saying is don’t test anyone in less than four days after exposure,” Cevik says. It’s not going to tell you much about the person’s status. Or if a person is tested in that time, they ought to be retested a few days later.
“In general, five to eight days after exposure is the best time to test,” Cevik says. “Or day three after symptom onset.” That’s when the genetic RT-PCR tests are most likely to reveal a true positive.
Because nothing about Covid-19 can be simple, here’s another thing to consider: The antigen tests that produce quick results have a shorter window in which you’d expect a person would test positive.
They are also slightly less accurate. But if used correctly, they can be very useful: They’ll test positive in the window when a person is most likely to be contagious. With repeated use, scientists hope these quick tests could help stop outbreaks from growing out of control.
The White House, on the other hand, has been using another rapid test, Abbott’s ID Now, to screen asymptomatic people. We just don’t know how good these tests — or any tests, for that matter — are at screening asymptomatic, or presymptomatic, people. “The FDA would be the first ones to tell you that they don’t know how the test is going to perform in that population,” Pritt says.
A negative test without symptoms might not mean much. Keep your mask on.
Here’s the bottom line: “We don’t know when one will test positive pre-symptom onset for PCR or antigen tests,” epidemiologist A. Marm Kilpatrick writes in an email. If you have symptoms, you’re likely to test positive the day you start feeling ill, but not guaranteed. The first few days after starting to feel sick, you have a very high probability of testing positive.
We could learn more in the months ahead about testing asymptomatic and presymptomatic people with studies following people after they have been exposed to the virus, and testing them repeatedly over a few weeks to determine the likelihood of testing positive before symptoms begin. “We have a lot of data from symptom onset onwards, but we don’t have data in terms of pre-symptoms,” Cevik says.
This is why testing is no replacement for other Covid-19 mitigation measures, like quarantining people exposed to the virus, mask-wearing, and social distancing.
“Testing negative is not like a passport for people to go out and do whatever they want to do,” Cevik says. If you might have been exposed to the coronavirus, like Vice President Pence was, you should quarantine for two weeks, regardless of what your test says.
A new wave of Covid-19 cases is building across the United States, a harbinger of difficult winter months ahead.
America is now averaging nearly 48,000 new confirmed cases every day, the highest numbers since mid-August, according to the Covid Tracking Project. More than 34,500 Americans are currently hospitalized with Covid-19 in the US, up from less than 30,000 a week ago. Nearly 700 new deaths are being reported on average every day, too — and while that is down from August, when there were often more than 1,000 deaths a day, deaths are going to eventually start increasing if cases and hospitalizations continue to rise. It’s a pattern we have seen before.
Public health experts have been warning for months that fall and winter could lead to a spike in Covid-19 cases. Why? Because the best way to slow down the coronavirus’s spread is to keep your distance from other people and, if you are going to be around others, to be outside as much as possible — and both become harder when the weather gets cold.
We may now be seeing those predictions start to come true. The US already has more than 7.7 million confirmed cases and 214,000 deaths. Both numbers will continue to climb.
Eight months into the pandemic, America’s failures to contain Covid-19, and states’ eagerness to reopen even if they haven’t gotten their outbreaks under control, is once again leading to a surge in cases and hospitalizations.
Covid-19 cases are rising everywhere across the country
Earlier in the year, there was limited value to discussing “waves” because some states would have a decline in cases while other states were experiencing surges. What distinguishes this autumn wave is that it seems to be happening everywhere.
Case numbers are up in the Northeast, the Midwest, and the West. The South appears to be, at best, plateauing at a level even higher than that which the Northeast endured during the worst of New York’s outbreak.
What’s so worrisome is that no one state or region can be blamed for this new wave. Just 13 states have seen their number of new Covid-19 cases drop over the last two weeks, according to Covid Exit Strategy. Cases are up in all the others.
Raw case numbers can, of course, obscure important differences in population; 100 new cases means something different for California than it does for Wyoming. Experts will use another metric — new cases per million people — to gauge how saturated a given state is with Covid-19.
The goal would be to have fewer than 40 new cases per million people. But just three states — Maine, Vermont, and New Hampshire — meet that threshold. Meanwhile, North Dakota (627 cases per million), South Dakota (596), Montana (474), and Wisconsin (434) are some of the states seeing very high levels of new infections.
As Vox’s German Lopez reported this week, just one state — Maine — meets all of the benchmarks established by experts for a state to consider its Covid-19 outbreak contained. And yet, most states have reopened many of the businesses that were closed in the spring: 40 or so states have reopened restaurants, bars, gyms, movie theaters, and nonessential retail.
“Part of the problem is America never really suppressed its Covid-19 cases to begin with,” Lopez wrote, explaining why experts were anticipating a new surge in cases. “Think of a disease epidemic like a forest fire: It’s going to be really difficult to contain the virus when there are still flames raging in parts of the forest and small embers practically everywhere. The country always risks a full blaze with each step toward reopening and with each failure to take precautions seriously.”
Too many Covid-19 tests are coming back positive right now
Another closely watched indicator for renewed Covid-19 spread is the percentage of coronavirus tests that come back positive. The number of tests being conducted doesn’t actually tell you all that much; if a high percentage of them are positive, that suggests that many others aren’t being caught at all and the virus could continue to spread unchecked.
So while the US is now averaging nearly 1 million tests every day, that is not quite the triumph it might sound like (or President Donald Trump would like to believe it is). The country’s positive test rate is 5 percent, right at the threshold experts say would reflect adequate testing. Ideally, it would be even lower, 2 percent or less.
But even with that passable national positivity rate, most states are still not conducting nearly enough testing. Here are the 10 states with the highest positive test rates, according to Covid Exit Strategy:
Idaho (25 percent)
South Dakota (20.6 percent)
Wisconsin (19.5 percent)
Iowa (17.1 percent)
Kansas (16.1 percent)
Wyoming (15.5 percent)
Utah (14.7 percent)
Nevada (14.4 percent)
Indiana (13.6 percent)
Alabama (13.3 percent)
It’s really only a handful of better-performing states — namely, New York, with more than 115,000 tests conducted per day and a 1.2 percent positivity rate — that’s keeping the US’s overall positive test rate from looking a lot worse.
America has never had a cohesive Covid-19 testing strategy. Since February, there have been regular supply shortages delaying test results. States have been fighting each other for precious testing resources. Contact tracing has not been a priority for the federal government, and most states have still not hired nearly enough people to perform that work.
Wealthy countries like Germany and South Korea have used effective test-trace-isolate programs to keep their Covid-19 outbreaks in check. The US, meanwhile, is still struggling to perform enough tests or scale up its contact tracing capabilities. Just 11 states, plus the District of Columbia, could realistically expect to perform adequate contact tracing, according to Covid Exit Strategy, considering their positivity rate.
Without improvement in both of those areas, it will continue to be difficult for the US to contain the coronavirus before a vaccine becomes available.
More Americans are being hospitalized with Covid-19 too
Both case numbers and the positive test rate can be a little deceptive, depending on how many tests are being performed. They suggest what’s happening on the ground — in this case, Covid-19 is spreading — but they do have their limitations. There is some truth to the president’s claim that more tests will mean more cases, though that is not a reason to stop testing.
Hospitalizations, on the other hand, are more concrete. If more people are developing symptoms severe enough to warrant being hospitalized, that is a strong indicator that the real number of people being infected with Covid-19 is growing, regardless of whether they are getting tested.
And after a dip in September, the number of Americans currently in the hospital with Covid-19 is higher than it’s been in a month. That trend has been seen across the country.
The worry becomes that if hospitals take in too many patients, they’ll have to turn other people away, or that overwhelmed staff and facilities could lead to some patients receiving substandard care. According to Covid Exit Strategy, 20 states currently have reduced ICU capacity that puts them in a danger zone; 21 states have an elevated occupancy rate in their regular hospital beds.
Wisconsin,where the number of hospitalized Covid-19 patients has risen over the last month from about 300 to 876 today, recently established a new field hospital on its state park fairgrounds over fears that the state’s hospitals wouldn’t have enough beds given the recent surge in cases.
Fortunately, hospitals have gotten much better at treating Covid-19. They have proven treatments, like remdesivir and dexamethasone, that reduce the length of hospital stays and reduce mortality in patients with severe symptoms. They have learned techniques like putting patients on their stomach to improve breathing. Hospitals that have endured multiple spikes of Covid-19 cases report patients in the later waves are spending less time in the hospital and dying less frequently.
Nevertheless, more people developing severe symptoms, as we are starting to see, will inevitably lead to more deaths. Over the summer, people wondered why deaths were falling while cases and hospitalizations rose — until deaths did start to increase. There is a long lag between cases rising and deaths rising, because it can take a month or more between when a person first contracts Covid-19 and, if they die, when their death is reported.
That’s why these new Covid-19 trends in the US are so worrisome. Cases are rising, as are hospitalizations. It could be only a matter of time before deaths start to spike as well.
An otherwise healthy 25-year-old Nevada man is the first American confirmed to have caught COVID-19 twice, with the second infection worse than the first.
He has recovered, but his case raises questions about how long people are protected after being infected with the coronavirus that causes the disease, and potentially how protective a vaccine might be.
“It’s a yellow caution light,” said Dr. William Schaffner, an infectious disease expert at the Vanderbilt University School of Medicine in Nashville, Tennessee, who was not involved in the research.
Respiratory infections like COVID-19 don’t provide lifelong immunity like a measles infection. So, Dr. Paul Offit, an infectious disease expert at Children’s Hospital of Philadelphia, said he’s not at all surprised people could get infected twice with the coronavirus, SARS-CoV-2.
It’s too soon to know whether the man from Washoe County, Nevada, who had no known health problems other than his double infection, was highly unusual or if many people could easily get infected more than once with SARS-CoV-2, Schaffner said.
“There’s hardly an infectious disease doctor in the country who hasn’t encountered a patient who thinks they’ve had a second infection,” he said. “Whether that’s true or not, we don’t know. There are lots of respiratory infections out there.”
How rare is he?
There have been at least 22 documented cases of reinfection worldwide since the start of the pandemic, but it’s unclear how many cases there have actually been, and how common it may be among people who don’t even know they’re infected.
“It could be a one in a million event, we don’t know,” said Akiko Iwasaki, an immunologist at Yale University and an investigator with the Howard Hughes Medical Institute, who wrote a commentary with the study.
With millions of people infected, it’s hard to know if case studies like the new one represent very rare events or the tip of an iceberg, she said. “It’s possible that the vast majority of people are completely protected from reinfection, but we’re not measuring them, because they’re not coming to the hospital.”
Also, many people don’t know they are infected the first time, so it’s hard to say whether they’re getting re-infected.
In one of the recent cases, a Hong Kong man only knew he was reinfected because it was caught during a routine screening when he returned from outside the country, months after he had cleared an infection and tested negative.
One reason there may not be more documented cases of reinfection: It’s tough to prove, said Mark Pandori, a pathologist at the University of Nevada, Reno School of Medicine, and senior author on the new study.
His team coordinated early in the pandemic with members of the Washoe County Health District to look for repeat infections. They had the benefit of sequencing equipment on campus, as well as microbiologists, he said. And they got lucky finding someone who had been tested both times he was infected and cleared in between.
Why his infection was worse the second time remains unclear, said Pandori, director of the Nevada State Public Health Laboratory. “I can’t tell you if it tells us anything in particular about the biology of this virus.”
The man caught a slightly different version of the virus the second time, according a genetic analysis of the man’s infections. It’s possible the second version was more dangerous, though there is no evidence of that, or that it was just different enough that his body didn’t recognize it, the paper said.
Implications for vaccination
Iwasaki said the study raises questions about how long immunity lasts after a natural infection. Protection with a vaccine is likely to be quite different, she said.
“Vaccines can be designed to induce much higher levels of antibody and much longer lasting immunity,” she said. Just because the natural infection doesn’t give you protection doesn’t mean the vaccines cannot. It’s a separate issue.”
Offit, also a vaccine expert at the Perelman School of Medicine at the University of Pennsylvania, said he expects protection from vaccines will likely last at least a year or two.
The protection provided by infection or vaccination isn’t 100% perfect until the day it disappears completely, he said. Instead, protection fades gradually, so someone exposed to a huge dose of the virus might get re-infected within months, while others could be protected for years, Offit said.
It’s also possible the Nevada man has an undiagnosed problem with his immune system. “He probably should be seen by an immunologist,” Offit said.
The length of time an infection will be protective remains one of the key open questions about the virus.
Infected twice, two months apart
The Nevada man, considered an essential worker, started feeling ill in late March, with a sore throat, cough, headache, nausea and diarrhea. His workplace had been hit with an outbreak early in the pandemic, before safety measures like masks could be put in place, said Heather Kerwin, senior epidemiologist at the Washoe County Health District and a co-author on the paper.
He went for testing on April 18 and his infection with the coronavirus was confirmed.
On April 27, he reported his symptoms had all resolved and he felt fine, but at the time, employees were required to test negative for COVID-19 twice before they would be allowed back to work, Kerwin said. So he remained isolated at home.
A month later, he began feeling poorly again. At the same time, there was an outbreak where one of his parent’s, also an essential worker, was employed, Kerwin said.
On May 31, he went to an urgent care center, reporting fever, headache, dizziness, cough, nausea and diarrhea. On June 5, he went to see a doctor who found his oxygen levels dangerously low and had him hospitalized. Again, the man tested positive for the virus, even though he still had antibodies to the virus in his bloodstream, Kerwin said.
Genetic differences between the viruses responsible for each of his infections suggested he was infected two separate times. The virus doesn’t mutate quickly enough within a single person to explain the differences between the two infections, the researchers found.
A parent living with the man also caught COVID-19 and was diagnosed on June 5.
Mark Pandori, pathologist
The paper reports it’s possible the man was reinfected because he was exposed to a higher dose of the virus the second time, perhaps from the family member.
His cough lingered and he suffered from shortness of breath and mental fog, and was on oxygen for six weeks after the second infection, Kerwin said. He has now fully recovered.
Reinfections imply so-called herd immunity cannot be obtained just through natural infection. If natural infection protects for only a few months, then it will be impossible for enough people to be protected simultaneously to reach herd immunity.
The moral of the case study, said co-author Pandori, is even people who already have been sick with COVID-19 need to protect themselves by wearing a mask, avoiding large gatherings, washing hands frequently and maintaining social distance.
“You’re not invulnerable to this,” Pandori said. “In fact, you could get it worse the second time.”
For its first 208 years, the New England Journal of Medicine has never endorsed a political candidate. But this week the journal published an editorial outlining its political position in the upcoming Presidential election, signed unanimously by all editors who are US citizens.
The editors did not explicitly endorse former Vice President Biden, but rather offered a scathing condemnation of the current administration’s performance during the COVID pandemic:“Reasonable people will certainly disagree about the many political positions taken by candidates.
But truth is neither liberal nor conservative. When it comes to the response to the largest public health crisis of our time, our current political leaders have demonstrated that they are dangerously incompetent. We should not abet them and enable the deaths of thousands more Americans by allowing them to keep their jobs.” (Formally endorsing Biden last month, Scientific American also made the first political endorsement in its 175-year history.)
Much of the media coverage of the NEJM statement has centered on the question of whether medicine should involve itself in politics, or “live above it”.
Medicine has been drawn into political disputes before, but now the nature of the involvement has changed. In the past, debates largely centered around regulation, payment or policy—but now the science itself has become a fundamentally political issue.
The very nature of the coronavirus has become a matter of political belief, not just an indisputable scientific fact.
Public trust in both scientific institutions and the government, and their ability to work together, has been damaged. We fear this will lead to poorer health outcomes regardless of who wins the upcoming election.
The COVID-19 pandemic is rife with scientific and medical uncertainty, including debates about the ethics of using experimental treatments.
The big picture: As the global pandemic continues, the tension between providing the best available care for patients and performing trials to determine whether that care is effective risks complicating the medical response.
The big question: Is it unethical to withhold a possible treatment from someone who instead receives a placebo, or to continue to administer that treatment without having collected data on whether it works?
Driving the news: President Trump received an experimental monoclonal antibody cocktail via expanded access or “compassionate use,” which allows someone to access a treatment outside of a clinical trial before it is approved, provided their doctor, the drug company and the FDA agree.
Experts say his subsequent claims of the treatment being a cure risks reducing enrollment in clinical trials, flooding companies with requests for access to a limited number of doses andcreating false hope for patients.
“It’s important that we not say the president got access to a beneficial experimental intervention because we don’t know if it is beneficial or if there are adverse events associated with it,“ says Alex John London, director of the Center for Ethics and Policy at Carnegie Mellon University.
He and other ethicists say the president’s treatment highlights a broader question about the ethical obligation doctors have to the science needed to determine if those treatments are effective.
Between the lines: Offering patients experimental COVID-19 drugs via emergency use authorizations, expanded access programs and compassionate use can slow needed clinical trials.
Researchers have struggled to enroll people in clinical trials in which they may receive a placebo if patients can access a drug directly.
One example: “There’s been some hiccups with the expanded access use for convalescent plasma, because it was something that precluded people from enrolling in a randomized control trial, so it took longer, and we still don’t quite know how well convalescent plasma works,” says Amesh Adalja, an infectious disease physician and senior scholar at the Johns Hopkins Center for Health Security.
More than 100,000 COVID-19 patients at almost 2,800 U.S. hospitals received convalescent plasma from people who survived the virus and developed antibodies to it.
“It’s easy for people to say you enrolled 100,000 people, there should have been a trial. But a small number of those 2,800 hospitals would have been capable of doing those trials,” says the Mayo Clinic’s Michael Joyner, who leads the program.
There are now smaller trials taking place to answer questions about the effectiveness of plasma in treating the disease in different stages.
But if this happens again, Joyner says programs at academic medical centers should be peeled off earlier to form clinical trials run in parallel.
The gold standard for determining whether a treatment works is through randomized controlled trials in which people are randomly assigned to receive a treatment or to be in a control group.
In the uncertainty and urgency of a pandemic, some physicians argue randomizing people to receive a placebo goes against physicians’ ethics and that it is better to do something to help patients than do nothing.
“That’s a false dichotomy because the question is, what should we do?” says London.
From a doctor’s perspective, it’s important to weigh the collective value of theearly drug data and the individual needs of the patient, Adalja says.
“I do think you have to be extra careful when you’re thinking about drugs that you don’t have strong randomized control trial data for, or the data is incomplete or inconclusive,” he adds.
“What people have to ask themselves is what constitutes evidence or proof and where do you want to make the bets in a pandemic?” says Joyner.
“There is a moral, legal and public health obligation to do those trials before people use those products,” says Alison Bateman-House, a professor of medical ethics at NYU’s Grossman School of Medicine who co-chairs an international working group on pre-approval access to treatments.
She says she understands the emotional pull on doctors to help patients whose health is quickly deteriorating, “but it is not evidence-based medicine.”
“There is no ethical obligation to give anyone an unproven substance.”
— Alison Bateman-House, NYU Grossman School of Medicine
In a forthcoming paper, London argues that when medical professionals don’t have the knowledge they need to treat patients, it is their responsibility “to band together and run studies to get evidence to discharge [their] very ancient medical obligation.”
Medical ethics should be updated to include a responsibility to learn in the face of uncertainty, says London, who was part of a committee that called for research to be incorporated into the response to the Ebola outbreak in West Africa in 2014.
The U.K.’s large randomized RECOVERY trial is based in part on the Ebola experience, says London. “Because of it, we know dexamethasone is effective and hydroxychloroquine is not.”
What to watch: How the FDA’s handling of treatments during the pandemic influences other drugs and diseases once the pandemic ends.
The bottom line: “Medicine doesn’t have a good handle on uncertainty, and that is a problem,” says London.
The United States needs to “own up to the fact that we didn’t do a good job” up until this point of the Covid-19 pandemic, billionaire and philanthropist Bill Gates said during a Fox News Sunday interview, adding that the slow turnaround for testing results remains “outrageous.”
KEY FACTS
“Unfortunately we did a very poor job and you can just see that in the numbers,” Gates said.
Despite having around 4% of the world’s population, the U.S. has around 22% of all cases with 6,782,083 and about 21% of all reported deaths with 199,411.
The inability to create a testing structure as seen in countries like South Korea “led to us having not just a bad spring, we’ve had a pretty tough summer and sadly because of the seasonality, until we get these new tools, the fall is looking to shape up as pretty tough as well,” Gates said.
“Part of the reluctance I think to fix the testing system now is that nobody wants to admit that it’s still outrageous,” Gates said, adding, “The U.S. has more of these machines, more capacity than other countries by a huge amount, and so partly the reimbursement system is creating perverse incentive.”
After remaining fairly stagnant through the end of summer into September, the U.S. performed a record 1,061,106 Covid-19 tests on Saturday, according to Johns Hopkins University, but labs are still dealing with supply shortages and delays in results.
“We’ll have time to look at those mistakes, which in February and March were really super unfortunate, but we can’t pretend like we get a good grade even today,” Gates said.
CRUCIAL QUOTE
“Even today, people don’t get their results in 24 hours, which it’s outrageous that we still have that,” Gates said.
BIG NUMBER
4.7%. That’s the average positivity percentage in the past week, according to Johns Hopkins.
TANGENT
President Trump has excused the world-leading cases of the coronavirus as a result of the number of tests performed in the country, even saying that he instructed officials to slow testing down. The Centers for Disease Control and Prevention sparked outrage in August when it published new guidelines on testing, recommending people exposed to the virus but not showing symptoms should not get tested. Reports indicate that the guidance was dictated by the Health and Human Services and Trump administration as opposed to CDC scientists. The guidelines were changed again on Friday.


:format(webp):no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/21952241/1R_Reg_Positive__1_.png)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/21952308/5R_Reg_Hospitalized.png)