https://www.commonwealthfund.org/blog/2019/health-care-2019-year-review

Health care was front and center for policymakers and the American public in 2019. An appeals court delivered a decision on the Affordable Care Act’s (ACA’s) individual mandate. In the Democratic primaries, almost all the presidential candidates talked about health reform — some seeking to build on the ACA, others proposing to radically transform the health system. While the ACA remains the law of the land, the current administration continues to take executive actions that erode coverage and other gains. In Congress, we witnessed much legislative activity around surprise bills and drug costs. Meanwhile, far from Washington, D.C., the tech giants in Silicon Valley are crashing the health care party with promised digital transformations. If you missed any of these big developments, here’s a short overview.
1. A decision from appeals court on the future of the ACA: On December 18, an appeals court struck down the ACA’s individual mandate in Texas v. United States, a suit brought by Texas and 17 other states. The court did not rule on the constitutionality of the ACA in its entirety, but sent it back to a lower court. Last December, that court ruled the ACA unconstitutional based on Congress repealing the financial penalty associated with the mandate. The case will be appealed to the U.S. Supreme Court, but the timing of the SCOTUS ruling is uncertain, leaving the future of the ACA hanging in the balance once again.
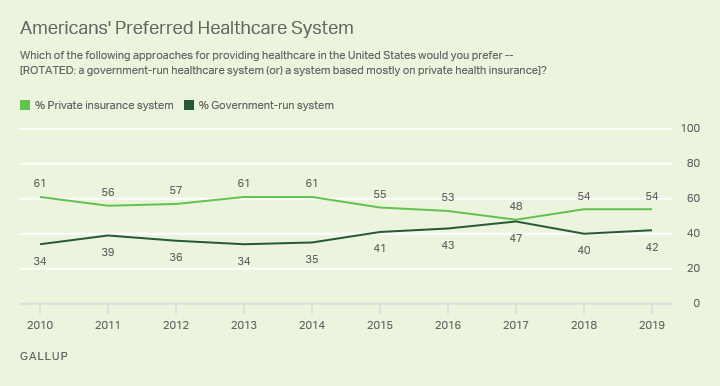
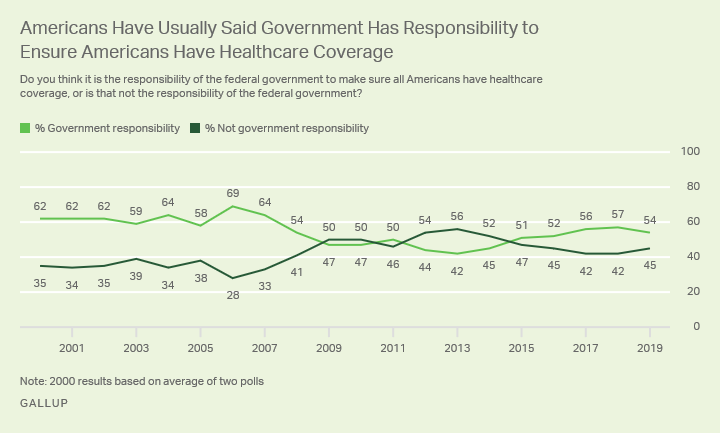
2. Democratic candidates propose health reform options: From a set of incremental improvements to the ACA to a single-payer plan like Medicare for All, every Democratic candidate who is serious about running for president has something to say about health care. Although these plans vary widely, they all expand the number of Americans with health insurance, and some manage to reduce health spending at the same time.
3. Rise in uninsured: Gains in coverage under the ACA appear to be stalling. In 2018, an estimated 30.4 million people were uninsured, up from a low of 28.6 million in 2016, according to a recent Commonwealth Fund survey. Nearly half of uninsured adults may have been eligible for subsidized insurance through ACA marketplaces or their state’s expanded Medicaid programs.
4. Changes to Medicaid: States continue to look for ways to alter their Medicaid programs, some seeking to impose requirements for people to work or participate in other qualifying activities to receive coverage. In Arkansas, the only state to implement work requirements, more than 17,000 people lost their Medicaid coverage in just three months. A federal judge has halted the program in Arkansas. Other states are still applying for waivers; none are currently implementing work requirements.
5. Public charge rule: The administration’s public charge rule, which deems legal immigrants who are not yet citizens as “public charges” if they receive government assistance, is discouraging some legal immigrants from using public services like Medicaid. The rule impacts not only immigrants, but their children or other family members who may be citizens. DHS estimated that 77,000 could lose Medicaid or choose not to enroll. The public charge rule may be contributing to a dramatic recent increase in the number of uninsured children in the U.S.
6. Open enrollment numbers: As of the seventh week of open enrollment, 8.3 million people bought health insurance for 2020 on HealthCare.gov, the federal marketplace. Taking into account that Nevada transitioned to a state-based exchange, and Maine and Virginia expanded Medicaid, this is roughly equivalent to 2019 enrollment. In spite of the Trump administration’s support of alternative health plans, like short-term plans with limited coverage, more new people signed up for coverage in 2020 than in the previous year. As we await final numbers — which will be released in March — it is also worth noting that enrollment was extended until December 18 because consumers experienced issues on the website. In addition, state-based marketplaces have not yet reported; many have longer enrollment periods than the federal marketplace.
7. Outrage over surprise bills: Public outrage swelled this year over unexpected medical bills, which may occur when a patient is treated by an out-of-network provider at an in-network facility. These bills can run into tens of thousands of dollars, causing crippling financial problems. Congress is searching for a bipartisan solution but negotiations have been complicated by fierce lobbying from stakeholders, including private equity companies. These firms have bought up undersupplied specialty physician practices and come to rely on surprise bills to swell their revenues.
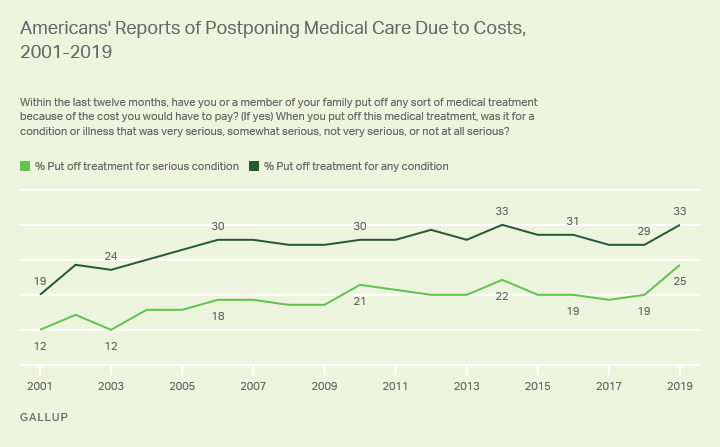
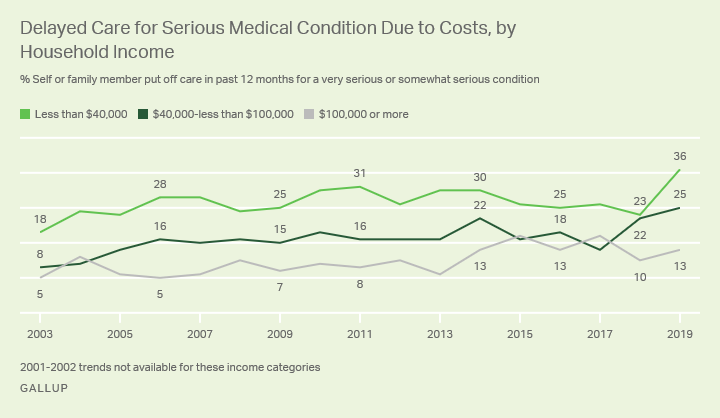
8. Employer health care coverage becomes more expensive: Roughly half the U.S. population gets health coverage through their employers. While employers and employees share the cost of this coverage, the average annual growth in the combined cost of employees’ contributions to premiums and their deductibles outpaced growth in U.S. median income between 2008 and 2018 in every state. This is because employers are passing along a larger proportion to employees, which means that people are incurring higher out-of-pocket expenses. Sluggish wage growth has also exacerbated the problem.
9. Tech companies continue inroads into health care: We are at the dawn of a new era in which technology companies may become critical players in the health care system. The management and use of health data to add value to common health care services is a prime example. Recently, Ascension, a huge national health system, reached an agreement with Google to store clinical data on 50 million patients in the tech giant’s cloud. But the devil is in the details, and tech companies and their provider clients are finding themselves enmeshed in a fierce debate over privacy, ownership, and control of health data.
10. House passes drug-cost legislation: For the first time, the U.S. House of Representatives passed comprehensive drug-cost-control legislation, H.R. 3. Reflecting the public’s distress over high drug prices, the legislation would require that the government negotiate the price of up to 250 prescription drugs in Medicare, limit drug manufacturers’ ability to annually hike prices in Medicare, and place the first-ever cap on out-of-pocket drug costs for Medicare beneficiaries. This development is historic but unlikely to result in immediate change. Its prospects in the Republican–controlled Senate are dim.