

Cartoon – Value Based Care
https://mailchi.mp/31b9e4f5100d/the-weekly-gist-june-03-2022?e=d1e747d2d8

This week we heard from three healthcare executives that they’ve seen a recent uptick in emergency department (ED) volumes. As we’ve discussed before, ED visits plummeted at the beginning of the pandemic, and were the slowest class of care volume to rebound. Over the past year, many systems reported that ED volume had remained persistently stuck at 10 to 15 percent lower than pre-COVID levels, leading us to question whether there had been a secular shift in patient demand, with consumers choosing alternative options like telemedicine or urgent care as a first stop for minor acute care needs.
An uptick in ED volume would be welcome news to many hospital executives, as the emergency department is the source of half or more of inpatient admissions for many hospitals. But according to what we’re hearing, the recent rise in emergency department patient volume has not resulted in an expected bump in inpatient volume.
“We’ve dug into it, and it seems like the jump in ED visits is a function of COVID,” one leader shared. “There’s just so much COVID out there now…even though the disease is milder, there are still a lot of patients coming to the ED. But unlike last year, most aren’t sick enough to be admitted.”
And ED visits for other causes have not rebounded in the same way: “We’re hoping patients aren’t still staying away because they’re afraid of catching the virus.” We’ll be watching closely across the summer to see how volumes trend as the pandemic waxes and wanes across the country—we’d still bet that many consumers have changed their thinking on where and how they will seek care when the need arises.
https://mailchi.mp/31b9e4f5100d/the-weekly-gist-june-03-2022?e=d1e747d2d8

When Congress passed the “No Surprises Act” in 2021, credit rating agencies like Moody’s warned that the bill would hurt physician staffing firms, especially those that provide emergency department (ED) services, which result in a surprise bill in roughly one in five visits. A piece from investigative outlet The Lever highlights how one private equity-backed physician staffing firm, Nashville-based American Physician Partners, is responding to the resultant cash flow challenges by cutting ED physician pay, after already reducing staffing levels. As the article describes, this is possible in an otherwise tight labor market because, unlike many other specialties, there’s an oversupply of ED physicians, due to the rapid growth in emergency medicine residency programs over the last decade.
The Gist: With two-thirds of hospitals outsourcing at least some ED physician labor, the potential insolvency of large physician staffing firms could bring a crisis in access and coverage.
In addition to revenue cuts tied to the surprise billing ban, rising interest rates also mean that PE firms may soon find it more difficult to fund their aggressive growth strategies.
Health systems should proactively evaluate their partnerships with PE-backed physician staffing groups, with an eye toward anticipating potential staffing problems and service quality shortfalls.
https://mailchi.mp/31b9e4f5100d/the-weekly-gist-june-03-2022?e=d1e747d2d8

The for-profit, 39-hospital Steward system manages 171K lives across the Medicare Advantage, Medicare shared savings, and Medicare direct contracting programs. This deal will allow Miami-based CareMax, a publicly-traded, value-based care company with 42 senior centers (mostly in Florida) and 34K lives under management, to expand across Steward’s footprint, which includes Texas and Arizona, states with rapidly growing Medicare populations.
The Gist: This deal is an example of the rise of venture-funded MSO (medical services organization) services that aim to subsume and scale value-based care functions from hospitals and medical groups. Steward wagers it can find greater success in managing risk in partnership with CareMax, moving a greater share of its Medicare population into risk, and outsourcing care management and patient engagement functions.
Many health systems have spent substantial resources building out accountable care organizations and risk-based Medicare businesses over the last decade. While selling these assets to a company like CareMax may be one way to generate a return, particularly for those frustrated by lower-than-anticipated gains from moving to value-based care, it also requires relinquishing control of functions likely central to the future health system business model.
https://mailchi.mp/31b9e4f5100d/the-weekly-gist-june-03-2022?e=d1e747d2d8

On Wednesday afternoon, an aggrieved patient shot and killed four people, including his orthopedic surgeon and another doctor, at a Saint Francis Hospital outpatient clinic, before killing himself. The gunman, who blamed his surgeon for ongoing pain after a recent back surgery, reportedly purchased his AR-15-style rifle only hours before the mass shooting, which also injured 10 others. The same day as this horrific attack, an inmate receiving care at Miami Valley Hospital in Dayton, OH shot and killed a security guard, and then himself.
The Gist: On the heels of the horrendous mass shootings in Buffalo and Uvalde, we find ourselves grappling with yet more senseless gun violence. Last week, we called on health system leaders to play a greater role in calling for gun law reforms. This week’s events show they must also ensure that their providers, team members, and patients are safe.
Of course, that’s a tall order, as hospital campuses are open for public access, and strive to be convenient and welcoming to patients. Most health systems already staff armed security guards or police officers, have a limited number of unlocked entrances, and provide active shooter training for staff.
This week’s events remind us that our healthcare workers are not just on the front lines of dealing with the horrific outcomes of gun violence, but may find themselves in the crosshairs—adding to already rising levels of workplace violence sparked by the pandemic.
Something must change.
https://www.axios.com/2022/06/02/health-care-workers-unions-covid-fatigue

Health care workers nationwide are organizing and pushing for workplace changes like better pay or more favorable staffing ratios after waves of pandemic-fueled burnout and frustration.
Why it matters: COVID-19 and its aftereffects triggered an exodus of health care workers. Those who stayed are demanding more from health systems that claim to be reaching their own breaking points.
Driving the news: About 1,400 resident physicians in public Los Angeles County hospitals have authorized a strike if their demands for pay parity with other local facilities aren’t met in contract negotiations this week.
Less than half of the of nearly 12,000 nurses polled by the American Nurses Association last year believe their employer cares about their concerns, and 52% of those surveyed said they intend to leave their jobs or are considering doing so.
The other side: Hospital operators generally oppose unionization efforts, as well as mandated staffing ratios.
Go deeper: The pandemic drove up labor costs significantly for hospitals that were forced to pay travel nurses to fill workforce gaps during COVID surges.
And yet, some big hospital chains like Tenet reported strong earnings in the first quarter.
Between the lines: California is the only state to have set staffing ratios for nurses, but hospital unions in other states have fought for similar requirements in their contracts.
What we’re watching: While many legislative proposals failed this year, unions representing health care workers say their message is getting across.
The bottom line: The labor tension is a sobering coda to a health crisis that’s stretched health systems and workers alike in unprecedented ways.
“What you’re seeing is nurses finally saying enough is enough and this system is broken and we need it to be fixed,” said Denelle Korin, a nurse alliance coordinator with Nurses of Pennsylvania.

Cleveland Clinic ended the first three months of this year with higher revenue, but rising expenses offset those gains, according to financial documents released May 26.
The health system’s revenue climbed to $3.03 billion in the first quarter of this year, which ended March 31, up from $2.81 billion in the same period of 2021. The system’s net patient service revenue increased from $2.53 billion in the first quarter of 2021 to $2.73 billion in the same period this year.
“Operating revenues in the first quarter of 2022 were impacted by lower patients served, partially due to the postponement of nonessential surgeries and procedures during the month of January,” the system said in an earnings release.
In the first quarter of this year, Cleveland Clinic facilities had 57,864 inpatient admissions and 61,103 surgical cases. In the same period a year earlier, the system reported 60,338 inpatient admissions and 63,051 surgical cases.
Cleveland Clinic reported expenses of $2.96 billion in the first quarter of this year, up from $2.56 billion in the same quarter of 2021. The system saw expenses rise across all categories, including supplies and salaries, wages and benefits.
The hospital system ended the first quarter of 2022 with an operating loss of $104.5 million, compared to operating income of $61.7 million in the same period of 2021.
Cleveland Clinic posted a net loss of $282.46 million in the first quarter of this year, compared to net income of $350.26 million in the same period a year earlier.

The bill is coming due for federal loans given to hospitals early in the COVID-19 pandemic, adding to their financial woes, Oregon Public Broadcasting reported May 28.
The Medicare Accelerated and Advance Payment program offered hospitals short-term interest- free loans, according to the report. These loans are coming due as hospitals’ costs are rising quickly and revenue from patient stays and surgeries is growing more slowly.
The idea behind the program was that hospitals would be able to pay back the advance once the pandemic passed and operations returned to normal, according to the report. Hospitals are still dealing with the effects of the pandemic, but the federal government wants to recoup the money to keep Medicare funded.
In March 2021, HHS began recovering those cash advances by paying hospitals 25 percent less for Medicare reimbursement claims, according to the report. Earlier this year, HHS began paying hospitals 50 percent less for reimbursement claims.
Hospitals lobbied for the loans to be forgiven, but were unsuccessful, according to the report.

Here are 11 health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings, Moody’s Investors Service and S&P Global Ratings.
1. Morristown, N.J.-based Atlantic Health System has an “Aa3” rating and stable outlook with Moody’s. The health system has strong operating performance and liquidity metrics, Moody’s said. The credit rating agency expects Atlantic Health System to sustain strong performance to support capital spending.
2. Greensboro, N.C.-based Cone Health has an “AA” rating and stable outlook with Fitch. The health system has a leading market share and a favorable payer mix, Fitch said. The health system’s broad operating platform and strategic capital investments should enable it to return to stronger operating results, the credit rating agency said.
3. Falls Church, Va.-based Inova Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has a consistently strong operating cash flow margin and ample balance sheet resources, Moody’s said. Inova’s financial excellence will remain undergirded by its favorable regulatory and economic environment, the credit rating agency said.
4. Vineland, N.J.-based Inspira Health Network has an “AA-” rating and stable outlook with Fitch. The health system has strong operating performance, a leading market position in a stable service area and a growing residency program, Fitch said. The credit rating agency expects the system’s growing outpatient footprint and an increase in patient volumes to support its operating stability.
5. Oakland, Calif.-based Kaiser Permanente has an “AA-” rating and stable outlook with Fitch. The health system has a strong financial profile, and the system’s operating platform is “arguably the most emulated model” for nonprofit healthcare delivery in the U.S., Fitch said. By revenue base, Kaiser is the largest nonprofit health system in the U.S., and it is the most fully integrated healthcare delivery system in the country, according to the credit rating agency.
6. Mass General Brigham has an “Aa3” rating and stable outlook with Moody’s and an “AA-” rating and stable outlook with S&P. The Boston-based health system has an excellent clinical reputation, good financial performance and strong balance sheet metrics, Moody’s said. The credit rating agency said it expects Mass General Brigham to maintain a strong market position and stable financial performance.
7. Rochester, Minn.-based Mayo Clinic has an “Aa2” rating and stable outlook with Moody’s. The credit rating agency said Mayo Clinic’s strong market position and patient demand will drive favorable financial results. The health system “will continue to leverage its excellent reputation and patient demand to continue generating favorable operating performance while maintaining strong balance sheet ratios,” Moody’s said.
8. Methodist Health System has an “Aa3” rating and stable outlook with Moody’s. The Dallas-based system has strong operating performance, and investments in facilities have allowed it to continue to capture more market share in the fast-growing Dallas-Fort Worth, Texas, area, Moody’s said. The credit rating agency said it expects Methodist Health System’s strong operating performance and favorable liquidity to continue.
9. Traverse City, Mich.-based Munson Healthcare has an “AA” rating and stable outlook with Fitch. The health system has a strong market position, a good payer mix and robust cash-to-adjusted debt levels, Fitch said. The credit rating agency expects the system to weather an expected period of weakened operating cash flow margins.
10. Albuquerque, N.M.-based Presbyterian Healthcare Services has an “Aa3” rating and stable outlook with Moody’s and an “AA” rating and stable outlook with Fitch. Presbyterian Healthcare Services is the largest health system in New Mexico, and it has strong revenue growth and a healthy balance sheet, Moody’s said. The credit rating agency said it expects the health system’s balance sheet and debt metrics to remain strong.
11. University of Iowa Hospitals and Clinics has an “Aa2” rating and stable outlook with Moody’s. The Iowa City-based health system, the only academic medical center in Iowa, has strong patient demand and excellent financial management, Moody’s said. The credit rating agency said it expects the health system to continue to manage the pandemic with improved operating cash flow margins.
https://mailchi.mp/d73a73774303/the-weekly-gist-may-27-2022?e=d1e747d2d8
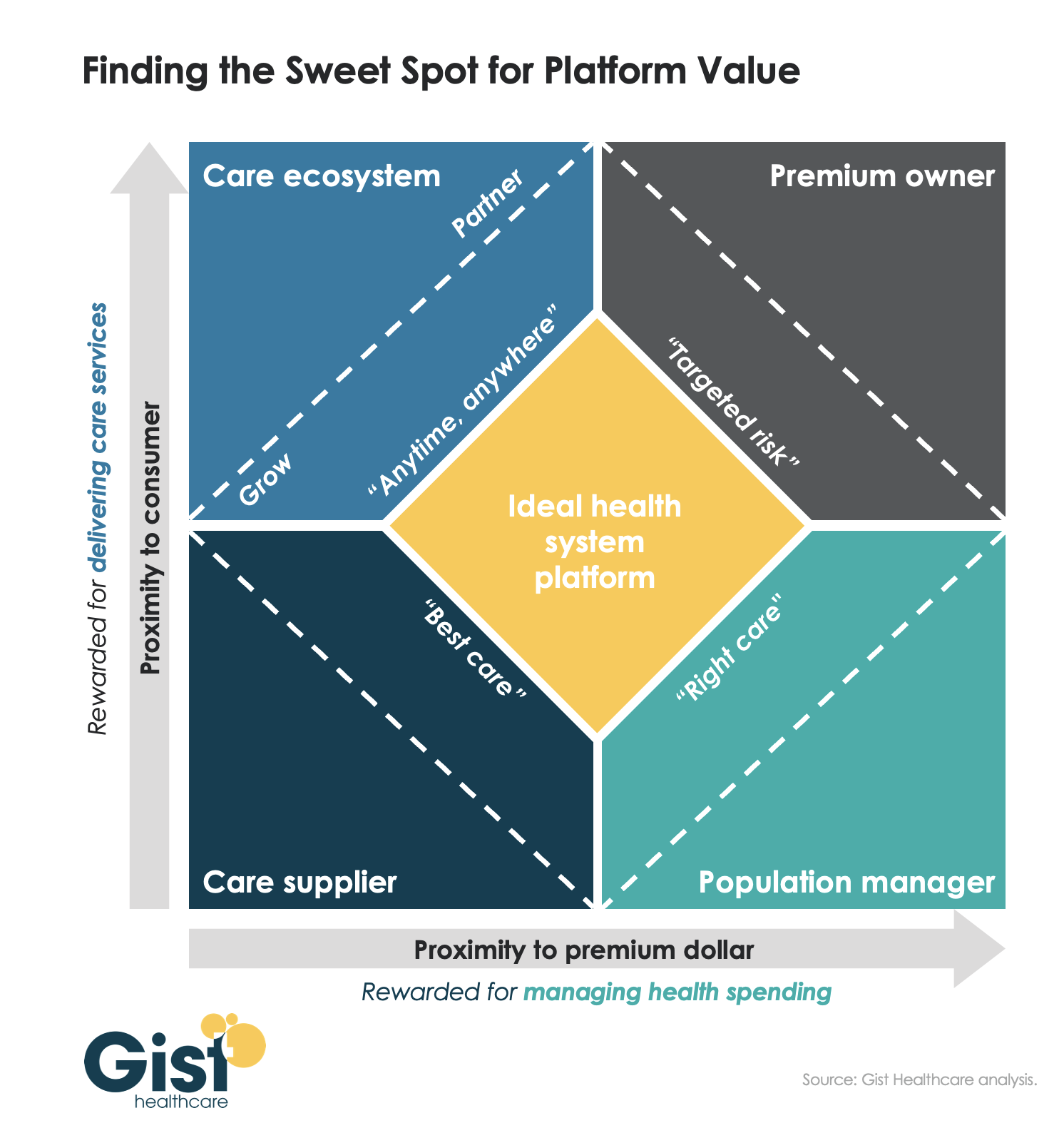
As we’ve been discussing over the past few years, several environmental forces—shifting consumer behavior, evolving demographics, new technology, and a flood of new market entrants—are pushing health systems to adopt a more consumer-centric business model. Systems must develop the capabilities needed to create an omnichannel consumer loyalty and population management platform. This platform will be the foundation for connecting consumers, curating providers, and coordinating care.
To achieve this vision, health systems must deliver value across two dimensions: increasing their proximity to the consumer (our y-axis) and their proximity to the premium dollar (our x-axis), as shown in the graphic above. Traditionally, health systems have operated primarily in the lower-left quadrant, as “care suppliers.” Some have spent considerable time and resources across the last decade, pushing closer to the premium dollar, to become “population managers.” But, importantly, managing population health is neither patient-facing, nor something consumers demand and seek.
To build deeper consumer loyalty, health systems must also move up the y-axis, creating a “care ecosystem” that provides “anywhere, anytime” care through multiple channels, including virtual and home-based solutions. And for certain populations, like Medicare Advantage, it will make sense for many systems to also explore becoming the “premium owner”, owning the full care budget and ensuring the incentives to design a consumer-centric offering.
The ideal health system platform should combine all four of these identities, tailored to the local market situation.
