The Federal Trade Commission has closed its investigation of the merger between Atrium Health Navicent and Houston Healthcare System following news the two have abandoned their plans for a deal.
FTC staff had recommended commissioners challenge the merger on grounds that it would have led to “significant harm” for area residents and businesses in the form of higher healthcare costs, the FTC alleged.
The tie-up between two of the largest systems in central Georgia would also hamper investment in facilities, technologies and expanded access to services, according to a statement released Wednesday.
Dive Insight:
FTC Acting Chairwoman Rebecca Kelly Slaughter said in the statement, “This is great news for patients in central Georgia.”
When the deal was originally announced, Atrium Health Navicent promised to spend $150 million on Houston over a decade, earmarking the money for routine capital expenditures and strategic growth initiatives, according to a previous review of the transaction by the state attorney general’s office.
After engaging with consultants at Kaufman Hall in 2017, leaders at Houston, an independent system, decided they needed to find a strategic partner to weather long-term challenges and ultimately picked Navicent.
Navicent recently merged with North Carolina-based Atrium Health, formerly known as Carolinas HealthCare System. At the time, the deal gave Atrium a foothold in the state of Georgia.
Healthcare consolidation has continued at a steady clip despite the pandemic, and the FTC will be closely investigating any deal involving close competitors. The agency is seeking to expand its arsenal to block future mergers by researching new theories of harm.
The FTC attempted to block a hospital deal in Philadelphia last year but has since abandoned its challenge after a series of setbacks in court. The judge was not swayed that the consolidation of providers would lead to an increase in prices given the plethora of healthcare options in the area.
Mercy Hospital & Medical Center in Chicago has secured a nonbinding purchase agreement with Insight Chicago just months before it is slated to close its doors, according to the Chicago Tribune.
Under terms of the deal, still being negotiated, Insight Chicago would operate Mercy Hospital as a full-service, acute care facility. Insight Chicago is a nonprofit affiliated with a Flint, Mich.-based biomedical technology company.
The deal is subject to regulatory approval, but if it goes through, it would keep the 170-year-old safety-net hospital open.
Securing a potential buyer is the latest in a series of events related to the Chicago hospital.
On Feb. 10, Mercy filed for bankruptcy protection, citing mounting financial losses and losses of staff that challenged its ability to provide safe patient care.
The bankruptcy filing came just a few weeks after the Illinois Health Facilities and Services Review Board rejected a plan from Mercy’s owner, Trinity Health, to build an outpatient center in the neighborhood where it planned to close Mercy. The same board unanimously rejected Livonia, Mich.-based Trinity’s plan to close the hospital in December.
The December vote from the review board came after months of protests from physicians, healthcare advocates and community organizers, who said that closing the hospital would create a healthcare desert on Chicago’s South Side.
Mercy said that until the pending deal with Insight Chicago is signed and approved by regulators, it still plans to close the facility. If the agreement is reached before the May 31 closure, Mercy will help transition services to Insight Chicago, according to theChicago Sun-Times.
Insight Chicago told local NPR affiliateWBEZthat it has a difficult task ahead to build community trust and address the financial issues that have plagued the Chicago hospital.
“I think the big main point we want to understand between now and then is the community needs to build trust with the community, and I think to build trust we have to tell the truth and be sincere,” Atif Bawahab, chief strategy officer at Insight, told WBEZ. “And there’s a reality of the situation as to why [the hospital] is going bankrupt and why several safety net hospitals are struggling.”
In its bankruptcy filing, Mercy said its losses have averaged about $5 million per month and reached $30.2 million for the first six months of fiscal year 2021. The hospital also said it has accumulated debt of more than $303.2 million over the last seven years, and the hospital needs more than $100 million in upgrades and modernizations.
West Reading, Pa.-based Tower Health is looking for a partner to buy the entire system, which comprises six hospitals, according to the Reading Eagle.
“We are compelled to pursue every possible avenue available to protect and preserve the future of care at all of our hospitals and facilities,” Tower said in a statement to The Philadelphia Inquirer on Feb. 26. “As part of this process, we will examine potential partnerships for the entire Tower Health system with like-minded health systems that share our same values and passion for clinical excellence.”
The health system had previously said it was looking for buyers for its hospitals, with the exception of its flagship facility, Reading Hospital in West Reading, according to the Inquirer.
On March 1, Tower Health was hit with a three-notch credit downgrade by Fitch Ratings. The credit rating agency said its long-term “B+” rating and negative outlook for the system reflect significant ongoing financial losses from the COVID-19 pandemic and operational challenges following the 2017 acquisition of five hospitals.
S&P lowered its rating on Tower Health by two notches, to “BB-” from “BB+,” on March 2.
Tower Health had operating losses of more than $415 million in fiscal year 2020, and it expects an operating loss of about $160 million in fiscal 2021, according to Fitch.
Even though signs point to a post-COVID spike in health system mergers, retailers, insurers, and other healthcare industry players already far exceed health system scale. Even the largest of the “mega health systems” pale in comparison to other healthcare companies up and down the value chain, as shown in the graphic above. And with the exception of pharma, these other industry players have seen revenues surge during the pandemic, while health system growth has stagnated.
According to a recent report from Kaufman Hall, hospitals saw a three percent reduction in annual total gross revenue in 2020.The majority of the decrease stemmed from a six percent decline in outpatient revenue, as volumes plummeted during the pandemic.
The largest companies listed here, including Walmart, Amazon, CVS, and UnitedHealth Group, continue to double down on vertical integration strategies, configuring an array of healthcare assets into platform businesses focused on delivering value to consumers.
To remain relevant, health systems will need to increase their focus on this strategy as well, assembling the right capabilities for a marketplace driven by value, at a scale that enables rapid innovation and sustainability.
After filing a lawsuit in May to end its affiliation with Renton, Wash.-based Providence, Hoag Memorial Hospital in Newport Beach, Calif., is alleging it is now the target of retaliation, according to theLos Angeles Times.
Hoag Memorial said that Providence removed Hoag Memorial’s three facilities from its website of Southern California locations and terminated Hoag Memorial’s specialists from St. Joseph Heritage Healthcare, a network of medical providers for managed care plans in Southern California. Additionally, Hoag Memorial said that Providence informed Heritage members they would lose access to Hoag’s 13 urgent care centers by Dec. 31.
According to the report, Providence’s notice to patients that Hoag facilities and physicians would be dropped from its network all came in the fall of 2020, amid the COVID-19 pandemic.
“It was the most inappropriate, inexplicable and harsh thing to do to a lot of patients,” Hoag President and CEO Robert Braithwaite told the Los Angeles Times. “Finding a new physician or new specialist is particularly hard on seniors and any patient who has a chronic condition and has established a long-term relationship with an endocrinologist or rheumatologist or cancer doctor.”
Providence told the Los Angeles Times it disagrees that patients have been disadvantaged.
“We are committed to the well-being of our communities and to serving patients with high quality and compassionate care,” a Providence spokesperson told the Los Angeles Times.
Hoag Memorial has been affiliated with Providence, a Catholic health system, since 2016.
Hoag Memorial said the changes all came after the hospital sought to end its affiliation with Providence by filing a lawsuit. Hoag Memorial said in its lawsuit it is seeking to end the affiliation because Providence is undermining local decision-making and Catholic Church restrictions are expanding.
Providence has fought Hoag’s lawsuit to end the affiliation. The health system claims Hoag doesn’t have the right to unilaterally dissolve the affiliation, and its board members don’t have the authority to file the lawsuit. An Orange County Superior Court judge rejected Providence’s argument Feb. 1 and scheduled another court hearing for March.
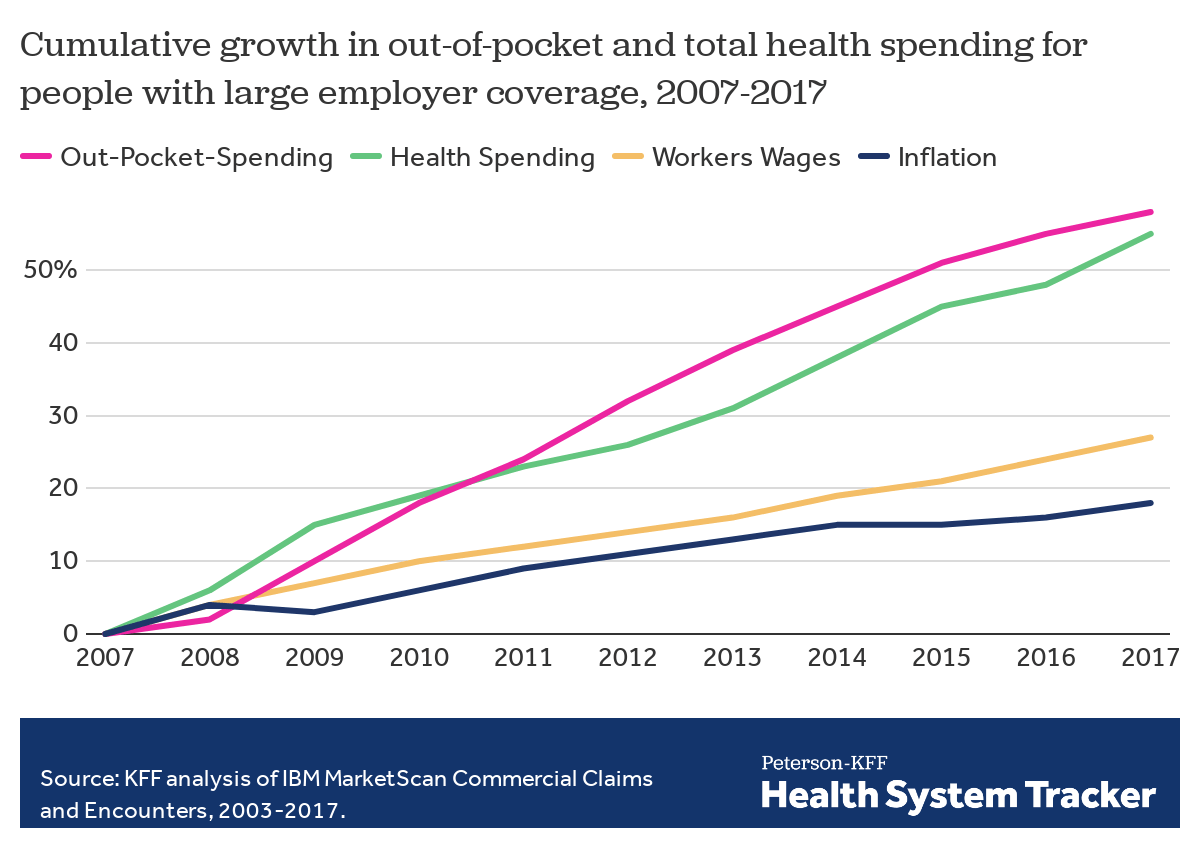
Employers — including companies, state governments and universities — purchase health care on behalf of roughly 150 million Americans. The cost of that care has continued to climb for both businesses and their workers.
For many years, employers saw wasteful care as the primary driver of their rising costs. They made benefits changes like adding wellness programs and raising deductibles to reduce unnecessary care, but costs continued to rise. Now, driven by a combination of new research and changing market forces — especially hospital consolidation — more employers see prices as their primary problem.
By amassing and analyzing employers’ claims data in innovative ways, academics and researchers at organizations like the Health Care Cost Institute (HCCI) and RAND have helped illuminate for employers two key truths about the hospital-based health care they purchase:
1) PRICES VARY WIDELY FOR THE SAME SERVICES
Data show that providers charge private payers very different prices for the exact same services — even within the same geographic area.
For example, HCCI found the price of a C-section delivery in the San Francisco Bay Area varies between hospitals by as much as:$24,107
Data show that hospitals charge employers and private insurers, on average, roughly twice what they charge Medicare for the exact same services. A recent RAND study analyzed more than 3,000 hospitals’ prices and found the most expensive facility in the country charged employers:4.1xMedicare
Hospitals claim this price difference is necessary because public payers like Medicare do not pay enough. However, there is a wide gap between the amount hospitals lose on Medicare (around -9% for inpatient care) and the amount more they charge employers compared to Medicare (200% or more).
Employer Efforts
A small but growing group of companies, public employers (like state governments and universities) and unions is using new data and tactics to tackle these high prices. (Learn more about who’s leading this work, how and why by listening to our full podcast episode in the player above.)
Note that the employers leading this charge tend to be large and self-funded, meaning they shoulder the risk for the insurance they provide employees, giving them extra flexibility and motivation to purchase health care differently. The approaches they are taking include:
Steering Employees
Some employers are implementing so-called tiered networks, where employees pay more if they want to continue seeing certain, more expensive providers. Others are trying to strongly steer employees to particular hospitals, sometimes know as centers of excellence, where employers have made special deals for particular services.
Purdue University, for example, covers travel and lodging and offers a $500 stipend to employees that get hip or knee replacements done at one Indiana hospital.
Negotiating New Deals
There is a movement among some employers to renegotiate hospital deals using Medicare rates as the baseline — since they are transparent and account for hospitals’ unique attributes like location and patient mix — as opposed to negotiating down from charges set by hospitals, which are seen by many as opaque and arbitrary. Other employers are pressuring their insurance carriers to renegotiate the contracts they have with hospitals.
In 2016, the Montana state employee health plan, led by Marilyn Bartlett, got all of the state’s hospitals to agree to a payment rate based on a multiple of Medicare. They saved more than $30 million in just three years. Bartlett is now advising other states trying to follow her playbook.
In 2020, several large Indiana employers urged insurance carrier Anthem to renegotiate their contract with Parkview Health, a hospital system RAND researchers identified as one of the most expensive in the country. After months of tense back-and-forth, the pair reached a five-year deal expected to save Anthem customers $700 million.
Legislating, Regulating, Litigating
Some employer coalitions are advocating for more intervention by policymakers to cap health care prices or at least make them more transparent. States like Colorado and Indiana have passed price transparency legislation, and new federal rules now require more hospital price transparency on a national level. Advocates expect strong industry opposition to stiffer measures, like price caps, which recently failed in the Montana legislature.
Other advocates are calling for more scrutiny by state and federal officials of hospital mergers and other anticompetitive practices. Some employers and unions have even resorted to suing hospitals like Sutter Health in California.
Employer Challenges
Employers face a few key barriers to purchasing health care in different and more efficient ways:
Provider Power
Hospitals tend to have much more market power than individual employers, and that power has grown in recent years, enabling them to raise prices. Even very large employers have geographically dispersed workforces, making it hard to exert much leverage over any given hospital. Some employers have tried forming purchasing coalitions to pool their buying power, but they face tricky organizational dynamics and laws that prohibit collusion.
Sophistication
Employers can attempt to lower prices by renegotiating contracts with hospitals or tailoring provider networks, but the work is complicated and rife with tradeoffs. Few employers are sophisticated enough, for example, to assess a provider’s quality or to structure hospital payments in new ways.Employers looking for insurers to help them have limited options, as that industry has also become highly consolidated.
Employee Blowback
Employers say they primarily provide benefits to recruit and retain happy and healthy employees. Many are reluctant to risk upsetting employees by cutting out expensive providers or redesigning benefits in other ways. A recent KFF survey found just 4% of employers had dropped a hospital in order to cut costs.
The Tradeoffs
Employers play a unique role in the United States health care system, and in the lives of the 150 million Americans who get insurance through work. For years, critics have questioned the wisdom of an employer-based health care system, and massive job losses created by the pandemic have reinforced those doubts for many.
Assuming employers do continue to purchase insurance on behalf of millions of Americans, though, focusing on lowering the prices they pay is one promising path to lowering total costs. However, as noted above, hospitals have expressed concern over the financial pressures they may face under these new deals. Complex benefit design strategies, like narrow or tiered networks, also run the risk of harming employees, who may make suboptimal choices or experience cost surprises. Finally, these strategies do not necessarily address other drivers of high costs including drug prices and wasteful care.
The federal government has penalized 774 hospitals for having the highest rates of patient infections or other potentially avoidable medical complications.Those hospitals, which include some of the nation’s marquee medical centers, will lose 1% of their Medicare payments over 12 months.
The penalties, based on patients who stayed in the hospitals anytime between mid-2017 and 2019, before the pandemic, are not related to covid-19. They were levied under a program created by the Affordable Care Act that uses the threat of losing Medicare money to motivate hospitals to protect patients from harm.
On any given day, one in every 31 hospital patients has an infection that was contracted during their stay, according to the Centers for Disease Control and Prevention. Infections and other complications can prolong hospital stays, complicate treatments and, in the worst instances, kill patients.
“Although significant progress has been made in preventing some healthcare-associated infection types, there is much more work to be done,” the CDC says.
Now in its seventh year, the Hospital-Acquired Condition Reduction Program has been greeted with disapproval and resignation by hospitals, which argue that penalties are meted out arbitrarily. Under the law, Medicare each year must punish the quarter of general care hospitals with the highest rates of patient safety issues. The government assesses the rates of infections, blood clots, sepsis cases, bedsores, hip fractures and other complications that occur in hospitals and might have been prevented. The total penalty amount is based on how much Medicare pays each hospital during the federal fiscal year — from last October through September.
Hospitals can be punished even if they have improved over past years — and some have. At times, the difference in infection and complication rates between the hospitals that get punished and those that escape punishment is negligible, but the requirement to penalize one-quarter of hospitals is unbending under the law. Akin Demehin, director of policy at the American Hospital Association, said the penalties were “a game of chance” based on “badly flawed” measures.
Some hospitals insist they received penalties because they were more thorough than others in finding and reporting infections and other complications to the federal Centers for Medicare & Medicaid Services and the CDC.
“The all-or-none penalty is unlike any other in Medicare’s programs,” said Dr. Karl Bilimoria, vice president for quality at Northwestern Medicine, whose flagship Northwestern Memorial Hospital in Chicago was penalized this year. He said Northwestern takes the penalty seriously because of the amount of money at stake, “but, at the same time, we know that we will have some trouble with some of the measures because we do a really good job identifying” complications.
Other renowned hospitals penalized this year include Ronald Reagan UCLA Medical Center and Cedars-Sinai Medical Center in Los Angeles; UCSF Medical Center in San Francisco; Beth Israel Deaconess Medical Center and Tufts Medical Center in Boston; NewYork-Presbyterian Hospital in New York; UPMC Presbyterian Shadyside in Pittsburgh; and Vanderbilt University Medical Center in Nashville, Tennessee.
There were 2,430 hospitals not penalized because their patient complication rates were not among the top quarter. An additional 2,057 hospitals were automatically excluded from the program, either because they solely served children, veterans or psychiatric patients, or because they have special status as a “critical access hospital” for lack of nearby alternatives for people needing inpatient care.
The penalties were not distributed evenly across states, according to a KHN analysis of Medicare data that included all categories of hospitals. Half of Rhode Island’s hospitals were penalized, as were 30% of Nevada’s.
All of Delaware’s hospitals escaped punishment.Medicare excludes all Maryland hospitals from the program because it pays them through a different arrangement than in other states.
Over the course of the program, 1,978 hospitals have been penalized at least once, KHN’s analysis found. Of those, 1,360 hospitals have been punished multiple times and 77 hospitals have been penalized in all seven years, including UPMC Presbyterian Shadyside.
The Medicare Payment Advisory Commission, which reports to Congress, said in a 2019 report that “it is important to drive quality improvement by tying infection rates to payment.” But the commission criticized the program’s use of a “tournament” model comparing hospitals to one another. Instead, it recommended fixed targets that let hospitals know what is expected of them and that don’t artificially limit how many hospitals can succeed.
Although federal officials have altered other ACA-created penalty programs in response to hospital complaints and independent critiques — such as one focused on patient readmissions — they have not made substantial changes to this program because the key elements are embedded in the statute and would require a change by Congress.
Boston’s Beth Israel Deaconess said in a statement that “we employ a broad range of patient care quality efforts and use reports such as those from the Centers for Medicare & Medicaid Services to identify and address opportunities for improvement.”
UCSF Health said its hospital has made “significant improvements” since the period Medicare measured in assessing the penalty.
“UCSF Health believes that many of the measures listed in the report are meaningful to patients, and are also valid standards for health systems to improve upon,” the hospital-health system said in a statement to KHN. “Some of the categories, however, are not risk-adjusted, which results in misleading and inaccurate comparisons.”
Cedars-Sinai said the penalty program disproportionally punishes academic medical centers due to the “high acuity and complexity” of their patients, details that aren’t captured in the Medicare billing data.
“These claims data were not designed for this purpose and are typically not specific enough to reflect the nuances of complex clinical care,” the hospital said. “Cedars-Sinai continually tracks and monitors rates of complications and infections, and updates processes to improve the care we deliver to our patients.”
As COVID-19 cases surged last fall, non-COVID-19 hospital admissions fell substantially, particularly in the Midwest and West, according to a new analysis by the Kaiser Family Foundation of 2020 inpatient admission data from electronic medical records through Dec. 5.
The analysis also highlights admission trends by age and sex, and found that patients 65 and over — those most at risk of complications from the novel coronavirus — delayed care at greater rates than those under 65 again in the fall. Still, the discrepancy between visits based on age was more pronounced in the spring.
On average, males and females had almost identical admission patterns throughout the entire year. Though looking at the raw numbers, women’s total admissions trended above their male counterparts, which researchers attributed to childbirth.
Dive Insight:
The latest analysis from the think tank provides a fuller picture of how the COVID-19 pandemic influenced admission trends throughout 2020.
Overall, total admissions bottomed out in April and March but have remained near normal, or above 90% of expected admissions since June, according to electronic medical record data from the Epic Health Research Network, which pools information from 20 million patients across 97 hospitals in the U.S.
However, while total admissions — which includes those sick with COVID-19 — remained near normal, the pattern differed when zeroing in on non-COVID-19 admissions, or those admitted who did not have the virus.
Non-COVID-19 admissions started to fall againin November and by Dec. 5 they fell to 80% of expected volume, which is likely to put financial pressure on hospitals, particularly those with smaller reserves of cash on hand, Kaiser noted.
The decline was steepest in the Midwest and West, dropping to about 76% of expected volume between early November and December.
Researchers fear the drop in non-COVD-19 admissions may have long-term consequences.
“The levels of non-COVID-19 admissions seen in the fall of 2020 suggest that people may be delaying care in ways that could be harmful to their long-term health,” according to the study.
Insurers observed similar patterns of depressed volume in the fourth quarter.
Humana, which largely covers seniors in Medicare plans, noted non-COVID-19 volume dropped the last two months of the quarter after previously returning to near normal. It led Humana to report a loss in the fourth quarter as COVID-19 testing and treatment accelerated. Centene, which reported a Q4 loss, echoed a similar pattern.

/the-us-federal-trade-commission--ftc--bu-71968930-e5e36febe53543aaa53329c6c17fc982.jpg)