Providence, a 51-hospital system headquartered in Renton, Wash., ended the first nine months of 2022 with an operating loss of $1.1 billion, according to financial documents released Nov. 14.
The system said in a Nov. 11 news release that its third quarter financial results showed the “ongoing impact of inflation, the national healthcare labor shortage, delayed reimbursement from payers, global supply chain disruptions and financial market weakness.”
For the nine months ended Sept. 30, Providence’s operating revenues were $19.6 billion on a pro forma basis, up from $18.8 billion during the same period last year, according to the report. The pro forma results exclude the operations of Newport Beach, Calif.-based Hoag Hospital. Providence and Hoag ended their affiliation in January.
Operating expenses over the first nine months of the year were $20.7 billion, a 7 percent increase over the same period in 2021 on a pro forma basis. This includes a 9 percent increase in salary and benefits due to the cost of agency staff, overtime and wage increases, according to the release. It also includes a 6 percent increase in supply costs, driven by an 8 percent increase in pharmaceutical spending.
Providence said financial market weakness and volatility drove investment losses of $1.4 billion for the first nine months of 2022, bringing the system’s unrestricted cash and investments to $9.1 billion.
“Healthcare delivery systems across the country face unprecedented challenges, and Providence has not been immune,” Providence President and CEO Rod Hochman, MD, said in the release. “However, just as we have for more than 165 years, we will continue to be here to meet the health care needs of our communities. While we still have a journey ahead of us, we are moving in the right direction and are beginning to see signs of renewal this quarter. My deepest gratitude to the caregivers of Providence for continuing to focus on the Mission and serving those in need, especially those who are most vulnerable, with excellence and compassion.”
South Dakota-based Sanford Health and Minnesota-based Fairview Health Services unveiled plans Tuesday to merge and form a 58-hospital juggernaut serving rural and urban patients across the Midwest.
The nonprofits have signed a nonbinding letter of intent as they proceed with due diligence and regulatory antitrust reviews, they said in a press release. Each would maintain their own regional presence, leadership and regional boards but operate as a single integrated system under Sanford Health’s banner.
The organizations said they anticipate closing their deal sometime next year.
“Our organizations are united by a shared commitment to advance the health and well-being of our communities,” Sanford Health President and CEO Bill Gassen said in the release. “As a combined system, we can do more to expand access to complex and highly specialized care, utilize innovative technology and provide a broader range of virtual services, unlock greater research capabilities and transform the care delivery experience to ensure every patient receives the best care no matter where they live.”
Gassen is teed up to serve as the president and CEO of the new entity should the merger go through, while Fairview CEO James Hereford would serve as co-CEO for one year following the deal’s close.
Headquarted in Sioux Falls, Sanford Health describes itself as the country’s largest rural health system with nearly 48,000 employees, 47 medical centers, 224 clinics and hundreds of other facilities. It serves over 1 million patients and 220,000 health plan members, according to its website, and each year logs 5.2 million outpatient or clinic visits, nearly 83,000 admissions, about 128,000 surgeries and procedures and roughly 195,000 emergency department visits.
Minneapolis-based Fairview Health Services employs 31,000 people across 11 hospitals as well as dozens of clinics, pharmacies and other facilities. It boasts a network of over 5,000 doctors after merging a few years back with fellow Twin Cities system HealthEast and due to partnerships with University of Minnesota Health specialists.
The two systems said their planned merger will improve care quality, outcomes, patient experience and health equity across their patient populations. New efficiencies will also help the systems offer more affordable care, they noted, while their workforces will benefit from stronger recruitment and advancement opportunities.
“With Sanford Health, Fairview Health Services has found a partner that shares our Midwestern values and our commitment to affordable, accessible and equitable care delivery,” Hereford said in the release. “Our complementary capabilities mean that together, we are uniquely positioned to improve clinical outcomes, develop new care delivery models, expand opportunities for employees and clinicians across our broader operational footprint, and apply our combined resources to positively impact the well-being of our patients and communities today and for decades to come.”
Sanford and Fairview’s news lands about six months after Advocate Aurora Health and Atrium Health announced their own nonprofit megamerger. That deal continues to move through the necessary regulatory hurdles and, if closed, would yield a 67-hospital with strong presences in the nearby Chicago and Milwaukee markets.
There’s an old trope among human resources leaders that people don’t quit companies, they quit managers. There’s certainly truth to it. If an employee has a difficult or inattentive boss, they are at much greater risk of leaving for another opportunity. But a “bad” manager is not always someone lacking in the skills necessary to engage employees; sometimes the problem is that their own roles are structured in ways that make it nearly impossible to succeed.
We’ve recently heard stories from leaders at several health systems describing the untenable management scope for many of their mid-level nursing leaders. It’s common to hear that nurse managers have dozens of direct reports, and a few systems reported that some of their managers have well over a hundred individuals reporting to them. With that scope, it’s impossible to develop relationships with everyone on the team, much less be able to customize roles, or provide tailored feedback and support.
For younger workers, the manager relationship is critical for engagement, skill development, and building loyalty.
Given today’s intense margin pressures, it’s tempting to cut clinical managers and increase the span of control for those who remain—but underinvestment here is short-sighted, and will surely exacerbate challenges maintaining critical capacity in the near-term, as well as building the foundation for future growth.
Here are 10 health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings and Moody’s Investors Service.
1. Advocate Aurora Health has an “AA” rating and a stable outlook with Fitch. The health system, dually headquartered in Milwaukee and Downers Grove, Ill., has a strong financial profile and a leading market position over a broad service area in Illinois and Wisconsin, Fitch said. The health system’s fundamental operating platform is strong, the credit rating agency said.
2. Allina Health System has an “AA-” rating and a stable outlook with Fitch. The Minneapolis-based system is the inpatient market share leader in a highly competitive market and has a strong relation with payers in the market, Fitch said. Alliana’s financial profile is strong, the ratings agency said.
3. Banner Health has an “AA-” rating and stable outlook with Fitch. The Phoenix-based health system’s core hospital delivery system and growth of its insurance division combine to make it a successful, highly integrated delivery system, Fitch said. The credit rating agency said it expects Banner to maintain operating EBITDA margins of about 8 percent on an annual basis, reflecting the growing revenues from the system’s insurance division and large employed physician base.
4. Bon Secours Mercy Health has an “AA-” rating and stable outlook with Fitch. The Cincinnati-based health system has a broad geographic footprint as one of the five largest Catholic health systems in the U.S., a good payer mix and a leading or near-leading market share in eight of its eleven markets in the U.S., Fitch said.
5. Bryan Health has an “AA-” rating and stable outlook with Fitch. The Lincoln, Neb.-based health system has a leading and growing market position, very strong cash flow and a strong financial position, Fitch said. The credit rating agency said Bryan Health has been resilient through the COVID-19 pandemic and is well-positioned to accommodate additional strategic investments.
6. Deaconess Health System has an “AA” rating and stable outlook with Fitch. The Evansville, Ind.-based system has a leading market position in its primary service area and a favorable payer mix, Fitch said. The ratings agency said it expects Deaconess’ operating EBITDA margins to improve and stabilize around 10 percent by 2023, reflecting strong volumes and focus on operating efficiencies.
7. Gundersen Health System has an “AA-” rating and stable outlook with Fitch. The La Crosse, Wis.-based health system has strong balance sheet metrics, a leading market position and an expanding operating platform in its service area, Fitch said. The credit rating agency expects the health system to return to strong operating performance as it emerges from disruption related to the COVID-19 pandemic.
8. Hackensack Meridian Health has an “AA-” rating and stable outlook with Fitch. The Edison, N.J.-based health system has shown consistent year-over-year increases in market share and has a solid liquidity position, Fitch said.
9. Intermountain Healthcare has an “Aa1” rating and stable outlook with Moody’s. The Salt Lake City-based health system has exceptional credit quality, which will continue to benefit from its leading market position in Utah, Moody’s said. The credit rating agency said the health system’s merger with Broomfield, Colo.-based SCL Health will also give Intermountain greater geographic reach.
10. Yale New Haven (Conn.) Health has an “AA-” rating and stable outlook with Fitch. The health system’s turnaround efforts, brand recognition and market presence will help it return to strong operating results, Fitch said.
Allentown, Pa.-based Lehigh Valley Health Network, which operates 13 hospitals and numerous care sites in Eastern Pennsylvania, will largely stop accepting Aetna insurance in 2023, Morning Call reported Nov. 10.
The move will be effective from March 13, LVHN said in a letter to employees. It comes after years of Aetna refusing to pay for care or delaying care for patients, the health group claimed.
LVHN, which has contracted with Aetna for 20 years, has been in dispute with the insurance company before, the report said. Back in 2000, the hospital group threatened to cut ties with Aetna over a dispute over care reimbursements.
Some Aetna coverage will remain for emergency care or for serious treatments such as cancer care, according to the letter.
LVHN declined to comment to Morning Call, and Aetna could not be reached, the report said.
More details on the story, which comes at a time when people are enrolling in new healthcare plans, can be found here.
Many hospitals and health systems aim to recruit and retain permanent staff to replace contract labor positions, which have seen wages skyrocket because of staff shortages during the COVID-19 pandemic.
Hospitals across the country have relied on contract labor and temporary staffing agencies to support their clinical teams when many burned-out providers are exiting healthcare. An October survey conducted by Bain & Company found that 25 percent of physicians, advanced practice providers and nurses are considering changing careers. Eight-nine percent of the providers thinking about leaving the profession cited burnout as the driving force.
Staffing shortages are driving labor costs to an unsustainable level for hospitals operating on razor-thin margins and reducing temporary staffing costs is top of the agenda for many financial executives looking to reduce expenses in the coming quarters.
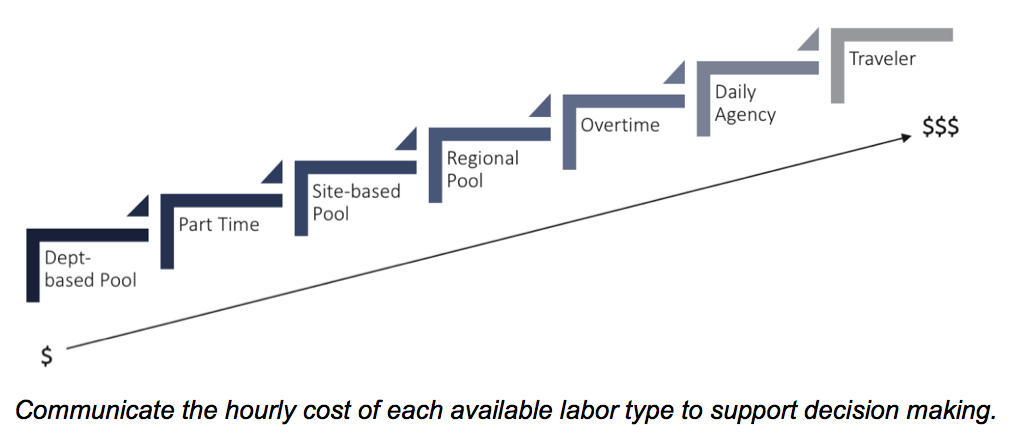
Here are 22 numbers that demonstrate the cost of contact labor for hospitals, according to reports from Kaufman Hall, Definitive Healthcare, Vaya Workforce and big hospital operators:
1. The demand for contract labor increased500 percent in fall 2021 compared with 2019, according to healthcare staffing services company Vaya Workforce. While demand has since decreased, it is still nearly triple pre-pandemic levels and is projected to remain as high as 20 percent above the 2019 baseline.
2. In 2020, the average amount hospitals spent on contract labor was $4.6 million, more than double the average expense of $2.2 million in 2011, according to a report from Definitive Healthcare, a data and analytics company.
3. Rochester, Minn.-based Mayo Clinic Hospital, Saint Mary’s Campus spent $286.8 million on contract labor in 2020, the most of any hospital in the country that year, according to Definitive Healthcare’s analysis of about 3,100 U.S. hospitals
4. From 2019 to 2022, the hourly wage rate for contract nurses increased106 percent, according to Kaufman Hall. Contract nurses are earning an average of $132an hour in 2022 versus $64an hour in 2019. At the height of the pandemic, some travel nurses earned up to $300 an hour, with rates as high as these placing immense pressure on hospital balance sheets.
5. The rise in contract labor from 2019 through March of 2022 led to a 37 percent increase in labor expenses per patient, equating to between $4,009 and $5,494 per adjusted discharge.
6. Hospitals with 25 beds or fewer spent about $460,000 on contract labor in 2020 compared to hospitals with more than 250 beds that spent almost $11 million on average, according to Definitive Healthcare.
7. Hospitals in the western U.S. have the highest contract labor expenses, with an average of $9.6 million reported in 2020. Large cities, high cost of living and high salary rates in the region contribute to this high average.
8. Labor costs were one of the core reasons Franklin, Tenn.-based Community Health Systems reported a net loss of $42 million in the third quarter, but CFO Kevin Hammons said he expects to see a 40 percent to 50 percent reduction in contract labor costs next year compared with 2022.
9. Nashville, Tenn.-based HCA Healthcare reported a 19 percent decrease in contract labor costs in the third quarter compared to the second quarter, allowing the system to absorb much of the market-based wage adjustment costs for its employee workforce, CFO Bill Rutherford said during an Oct. 21 earnings call.
10. According to Kaufman Hall’s “2022 State of Healthcare Performance Improvement” report, published Oct. 18, 46 percent of hospital and health system leaders identify labor costs as the greatest opportunity for cost reductions. This was significantly up from the 17 percent of respondents who noted labor costs as their greatest opportunity to cut costs last year.
11. There are some hopeful signs that the use of contract labor has stabilized and is steadily falling, according to Kaufman Hall: 44 percent of hospitals in its survey reported that their utilization of contract labor is declining while 29 percent said that it is holding steady.
Oakland, Calif.-based Kaiser Foundation Health Plan, Kaiser Foundation Hospitals and their subsidiaries reported a net loss of $1.5 billion for the quarter ending Sept. 30, according to a Nov. 4 financial report.
The company posted total operating revenues of $24.3 billion and total operating expenses of $24.3 billion for the quarter. Total operating revenues of $23.2 billion and total operating expenses of $23.1 billion for the same period in 2021.
Additionally, there was an operating loss of $75 million in the third quarter compared to an operating income of $38 million in the third quarter of 2021, according to a Nov. 4 news release.
“I am proud of our ability to navigate the challenges of the past few years, including a global economic crisis, the high cost of goods and services, supply chain issues, labor shortages, and the pandemic while serving our 12.6 million members,” said Greg Adams, chair and CEO of Kaiser Permanente.
The net loss of $1.5 billion in the third quarter of 2022 compares to a $1.6 billion net income in the third quarter of 2021. Capital spending totaled $2.5 billion year-to-date.
“We are grateful to our extraordinary people whose commitment and compassion allow us to continue to fulfill our mission of providing high-quality and affordable care and improving the health of our communities,” said Tom Meier, corporate treasurer of Kaiser Permanente.
Physicians are set to see a 4.5 percent decrease in Medicare payment next year, in part due to the expiration of a temporary payment boost that was passed by Congress in December 2021 to avert scheduled sequester cuts. Physician groups are expected to lobby lawmakers heavily in the final months of the year, hoping to secure a reprieve, especially as inflation and labor costs continue to rise.
Other changes in the 2023 rules include advance payments to new participants in the Medicare Shared Savings Program, intended to boost participation of providers in rural and underserved areas. Some pandemic-era telehealth flexibilities that are set to expire with the end of the federal COVID public health emergency were also extended.
The Gist: We do not expect the full Medicare physician reimbursement cut to physicians to go into effect, as a bipartisan group of Senators has already asked leadership to address it in the upcoming lame-duck session. However, the cut serves the important purpose ofrebasing negotiations between physician lobbies and Congress, such that keeping rates flat or obtaining a small boost would feel like a win for both groups—even if it falls far short of the rate increases needed to meet the rising cost of running a practice.
If Congress continues to intervene to push off or mitigate Medicare’s sequestration payment reductions, we could find ourselves back in a Sustainable Growth Rate (SGR)-type situation where a payment cut constantly looms, physicians continually lobby for yet another reprieve, and the delayed cuts balloon in size.
I began to wonder if this trip to a pediatric urgent care with my son was even necessary.
Sure, he had been diagnosed with pneumonia a week ago and didn’t seem to be getting better. His cough sounded uglier. But here Ethan was in classic two-and-a-half-year-old mode: running in big circles around the waiting room chairs and causing the kind of ruckus only a toddler can.
He’d stuff some Pirate’s Booty I had hastily thrown into my purse in his mouth, before returning to his wild banshee ways and dashing around in circles again.
Our pediatrician said their office was too swamped with sick kids to see us, and referred us to this place. We had been told the wait to see a doctor would be a minimum of an hour. We struggled to find a seat in the packed waiting room as far as possible from other coughing kids.
We finally graduated from the waiting room to the doctor’s office, only for Ethan to continue his marathon by scooting a rolling chair back and forth, roaring with laughter every time it hit the examining table. When the physician walked in, I felt like I needed to defend wasting her time with this visit with my seemingly A-OK, albeit destructive, son.
But Ethan wasn’t OK.
The doctor listened to his chest with her stethoscope and didn’t like what she heard: wheezing, some crackling.
She showed me how Ethan’s Pirate’s Booty-stuffed stomach moved heavily each time he inhaled and exhaled.
They had Ethan complete a nebulizer treatment in the office, which meant slipping a device on his face that resembled an oxygen mask, while medicated air meant to open up his lungs flowed through a frightfully loud machine. I held him in my lap while the nebulizer was on, scrambling to find 100 different versions of “Wheels on the Bus” videos on YouTube to try to distract him from the vacuum-like whirring of the machine.
The doctor listened to his lungs again. His breathing still didn’t sound great, but she said the hospitals were too inundated right now.
I knew all too well what she meant. A few days before our urgent care visit, I had flagged a report for editors at The Hill that said children’s hospitals in the Washington area were at capacity, flooded with young kids suffering from RSV, a potentially life-threatening respiratory illness that has no vaccine.
After a three-hour visit, she gave Ethan a steroid and told us to follow up with his pediatrician the next day.
By the time we got to the pediatrician’s office the following morning, my happy-go-lucky, playful little guy was anything but. He curled up in my lap, as we went through a similar routine that the urgent care doctor had done just the night before. His oxygen levels were too low, and our pediatrician had him do another nebulizer treatment.
“Our goal is to keep you from going to the hospital,” our pediatrician told us.
It seemed like an unusual “goal” from a doctor, but I understood her reasoning. But after Ethan’s oxygen levels dipped lower still after the nebulizer, she said we should rush him straight to the hospital after all.
My “Blue’s Clues” and vehicle-obsessed son, usually the epitome of toddler “I can do it myself!” independence, wouldn’t let me put him down for even a moment as we waited in the emergency room lobby. Surprisingly, a separate waiting area in the ER just for children wasn’t completely full, and I wondered if maybe news reports of endless waits were overblown.
Not so.
“He’s so cute,” a young mother in the waiting room told me, as she motioned to Ethan’s head of curls. She cradled her two-month-old in her arms, patiently rocking the baby after telling me she had waited three hours so far.
I held Ethan as my husband rushed from work to the hospital, meeting us there and with us as we were brought to an ER triage area. They ran more oxygen tests on Ethan, got some of his history, and then sent us back to the waiting room.
Finally, they called Ethan’s name and we were in the ER. My vibrant, otherwise-healthy kid was lethargic, laying on me with a glazed look in his eyes. We struggled to fit the two of us on an exam table meant for a single adult. They draped a lead apron over me and Ethan as they took X-rays of his tiny lungs. The nurse placed a cannula in Ethan’s nose for supplemental oxygen and put an IV in his arm to give him fluids, before wrapping it with a diaper so he wouldn’t try to take out the tube.
My husband and I, loopy from what was happening, laughed at the sight of a diaper being used MacGyver-style. “Hey, it works!” the nurse said, explaining that he’d done the maneuver with kid after kid in recent weeks.
The ER doctor finally came in our room and delivered a crash course in what might be to come. “Everywhere is full. The entire Eastern seaboard,” he said of hospitals.
“We’ve been airlifting kids to Pittsburgh, sometimes to Richmond,” he added. This hospital had a pediatric unit, but not an intensive care geared towards kids. So if Ethan’s condition became even more dire, they wouldn’t be able to treat him there. Our only hope was that the pediatric unit, which had just a few remaining beds, accepted him.
It was a gut punch. As the doctor left, my husband looked at Ethan, who had fallen asleep with a mask on as the nebulizer loudly buzzed away for another treatment.
“He’s just a baby. He’s not supposed to be here,” my husband said, defeated.
The pediatric unit doctor finally came into our room. She examined Ethan, and briefed us on how they’ve been dealing with case after case of the same thing: RSV.
But she offered us hope: he could head to the pediatric unit at the hospital. We wouldn’t need to travel for his care, as long as he didn’t worsen. Ten hours after we first entered the hospital, we had a bed for Ethan.
We’re among the lucky ones. We were told beyond airlifting, plenty of families had been spending multiple nights in the ER because there were no beds.
In Maryland, Gov. Larry Hogan (R) announced last week that that hospitals would receive $25 million in additional funding from the state to prioritize pediatric intensive care unit staffing. Children from birth to age two comprised 57 percent of hospitalizations last week, according to Hogan’s office.
Next to the ghost decorations for Halloween adorning the doors of the pediatric unit, room after room had the same notice taped up: isolation guidelines. The rooms were all filled with kids facing the exact same thing as Ethan. RSV was everywhere.
There’s no cure for RSV. Every two hours on the dot, the nurses would give Ethan the nebulizer treatment.
A monitor affixed to his foot would alert nurses if his oxygen dipped dangerously low, which it did several times throughout the first night. I thought at one point to ask what happens if Ethan stopped responding to the treatments, but then didn’t ask because I didn’t want to know the answer.
The goal was to get him going without the need for additional oxygen, and breathing well for at least four hours between treatments, two times in a row.
That seemingly simple goal proved elusive for two full days. I originally thought it would be a nightmare trying to get a two-year-old to stay in a hospital bed for more than five minutes, but Ethan was in such bad shape that he barely made a fuss. Then, after midnight on our second night in the hospital, Ethan suddenly perked up.
He sat up and rolled over in the hospital bed. Then, he rolled onto my head, spreading his arms and legs out as far as he could stretch, and giggled.
“Should I sleep here?” he said, cracking himself up.
It was like someone hit the power button on my kid, and suddenly he snapped back to himself. I didn’t care that it was midnight and we needed to get some extremely interrupted sleep before the next nebulizer treatment. My son was back.
A nurse later told me that she enjoyed working with kids because for as quickly as their health can deteriorate, they can just as speedily bounce back.
After that, the doctor advised us to try stretching out his time between treatments. Finally, we were told he was stable enough to go home. I somehow hadn’t shed a tear the entire time we were at the hospital, but when the doctor signed off on us leaving, I bawled.
As nightmarish an experience as it was, I realize how incredibly fortunate my family is.
My husband and I have jobs that allowed us to drop everything when our son needed help, we have health insurance policies, and resources to get through spending days at the hospital.
Perhaps most importantly, we had access to an incredible team of doctors and nurses and the sheer fortune of being able to get a bed for our son during an unprecedented and unthinkable time for hospitals.
At the risk of repeating one of those parenting cliches that I would’ve rolled my eyes at a week ago, I’m thankful that I trusted my gut. Even when Ethan was being a wild child at urgent care, I knew something just wasn’t right. What I didn’t know was how much he had been struggling to breathe.
At the hospital after being discharged, Ethan and I waited in the lobby as my husband went to get our car from the parking lot to pick us up. Ethan spotted some empty wheelchairs in the corner of the lobby, and immediately ran over to them. He giggled as he tried to roll one of the chairs into the automatic opening and closing doors. As I looked on as he laughed and laughed at the pint-sized commotion he created, I breathed a sigh of relief.
The third quarter brought little relief to hospitals in what is shaping up to be one of their worst financial years.
Kaufman Hall’s October National Hospital Flash Report— based on data from more than 900 hospitals — found slightly lower hospital expenses in September did not outweigh lower revenue across the board, with decreases in discharges, inpatient minutes and operating minutes.
The median year-to-date operating margin index for hospitals was -0.1 percent in September, marking a ninth straight month of negative operating margins and a dimmer outlook for their climb back into the black by year’s end.
Kaufman Hall noted that expense pressures and volume and revenue declines could force hospitals to make “difficult decisions” about service reductions and cuts.
“Health systems are starting to get a clear picture of what service lines have a positive effect on their margins and which ones are weighing them down,” said Matthew Bates, managing director and Physician Enterprise service line lead with Kaufman Hall. “Without a positive margin there is no mission. Health systems must think carefully and strategically about what areas of care they invest in for the future.”