Of all the pandemic’s impacts still felt today, disruptions to the healthcare workforce and rising labor costs may be most impactful to current health system operations.
Over the next three editions of the Weekly Gist, we’ll be exploring the lingering effects of this workforce crisis, with a focus on nurse staffing and recruitment.
While wage increases helped reduce hospital registered nurse (RN) turnover rates from 27 percent in 2021 to 23 percent in 2022, nurses—along with hospital employees in general—are still changing jobs at higher rates than before the pandemic.
Over half of all hospitals still face nurse vacancy rates above 15 percent, a slight improvement from 2022 but still far more than before the pandemic.
While the worst of nursing turnover appears to have passed, the “rebasing” of wages (for nursing, 27 percent higher compared to 2019) will provide ongoing pressure to strained hospital margins.
Peter Drucker, the hall of fame management guru, once famously said that the hardest business organization to run in America was a hospital. If that comment was true so many years ago, imagine what Drucker would have to say about the difficulty of hospital management right now.
Hospital financial performance suffered significantly in 2022 and recovery during 2023 has been quite slow. This trend suggests the question,
“What steps are hospital C-suites taking to recover pre-Covid financial stability?”
Erik Swanson manages all analyses for our monthly Kaufman Hall Flash Report and he and I speculated that an industry-wide hospital recovery could not be achieved without reductions in force across the hospital ecosystem. Some research on our part determined that no official organization tracks hospital layoffs over time but we wondered if we could use our Flash Report data, which is provided to us by Syntellis Performance Solutions, to reach an informed conclusion.
What we were able to do was prepare three types of charts, as follows:
The first chart measures net employee percentage change by month. This chart shows whether overall hospital employment is increasing or decreasing over time and by how much.
The second chart attempts to establish the median turnover for hospitals over an annual period and then measure the deviation from that turnover rate. A greater deviation from what might be termed “normal turnover” suggests that an increasing number of hospitals are using reductions in force to more quickly reduce the cost of doing business.
The third chart shows average FTEs per occupied bed on a comparative basis looking at month-to-month and year-to-year statistics.
The first chart, Net Employee Percentage Change by Month, begins at January 1, 2018, and continues to March 1, 2023 (Figure 1). Overall additions to hospital employment remained generally positive through January 1, 2020. Overall hospital employment then went generally negative from March 2020 (the onset of Covid restrictions) to March 2022. The reductions in hospital employees during this period were likely the result of the “great resignation” during the worst of the Covid pandemic. But then, from July 2022 to March 2023, overall hospital employees demonstrated by the Flash Report dropped dramatically with an overall 2% decrease at the March 2023 date. This statistic suggests more than simply increased hospital turnover, but rather a formal layoff process initiated across many hospital organizations, along with aggressive management of contract labor.
Figure 1: Net Employee Percentage Change by Month
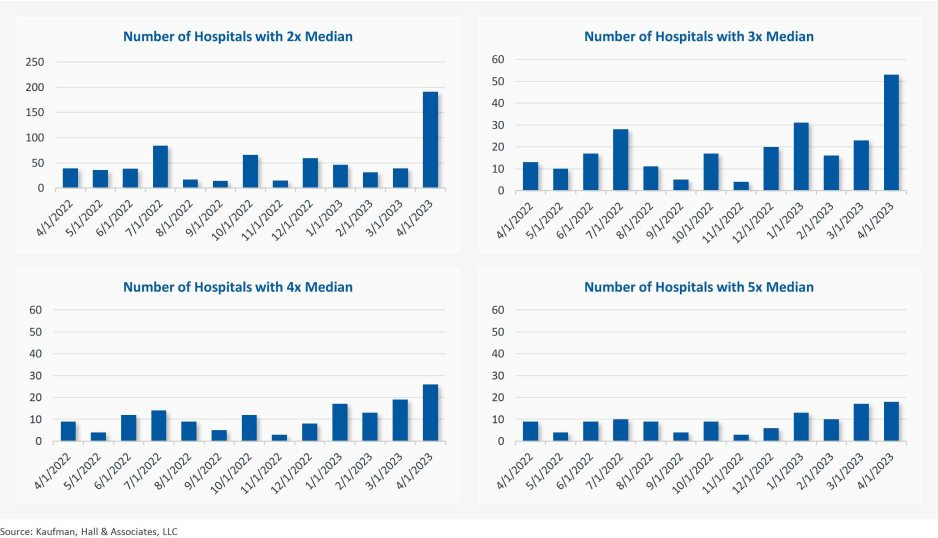
The second chart demonstrates the deviation from expected turnover at levels of 2x, 3x, 4x, and 5x by number of hospitals (Figure 2). No matter which measure you examine, the deviation of employees from expected turnover spiked significantly in April 2023 and even more so in May 2023. This again suggests the aggressive management of labor costs that likely could not occur without the intentional reduction of actual positions and/or the cost of these positions.
Figure 2: Number of Hospitals with Deviations from Expected Turnover at 2x, 3x, 4x, and 5x the Median
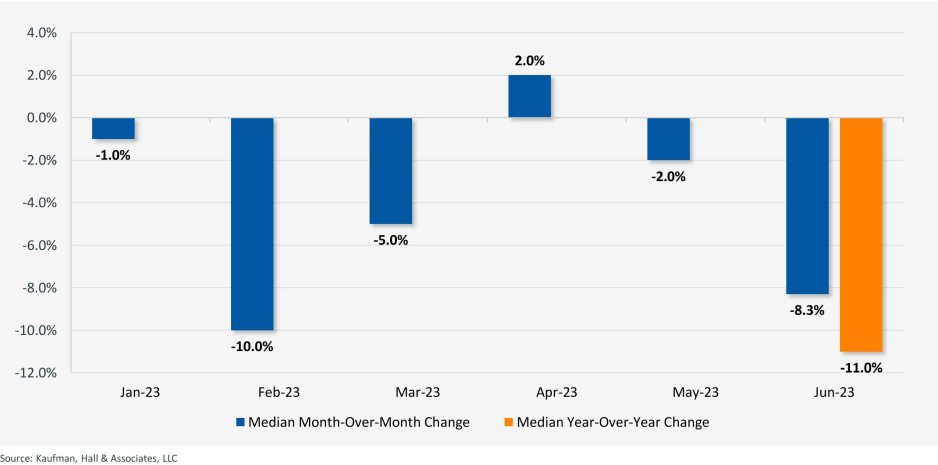
The last chart provides a remarkable set of observations (Figure 3). FTEs per adjusted occupied bed (AOB) declined by 8.3% between June 2023 and July 2023. The year-over-year variation for July 2023 was a decline of 11.01%. Our data further reveals that the FTE per AOB statistic has declined in five of the past six months on a month-over-month basis.
Figure 3: Median Change in FTEs per Adjusted Occupied Bed by Month
The conclusion here is that the return of the hospital industry to pre-Covid financial results has been no walk in the park. 2022 was, of course, a dismal financial year for the hospital industry. And while 2023 has shown improvement, the usual management steps to recovery have been only moderately effective. The data and analysis above demonstrate that C-suites across America are moving to stronger measures to assure the financial survivability and competitiveness of their organizations.
There is no revenue solve here, or at least not in the current environment: costs must come down and they must come down materially. From the sense and the trend of the data it would seem that hospital executive teams get the joke.
From time to time the blogging process stimulates a conversation between the author and the audience. This type of conversation occurred after the publication of my recent blog, “The Hospital Makeover—Part 2.” This blog focused entirely on the current problems, financial and otherwise, of the hospital physician employment model. I received responses from CEOs and other C-suite executives and those responses are very much worth adding to the physician employment conversation. Hospital executives have obviously given the physician employment strategy considerable thought.
One CEO noted that, looking back from a business perspective, physician employment was not actually a doctor retention strategy but, in the long run, more of a customer acquisition and customer loyalty strategy.
The tactic was to employ the physician and draw his or her patients into the hospital ecosystem. And by extension, if the patient was loyal to the doctor, then the patient would also be loyal to the hospital. Perhaps this approach was once legitimate but new access models, consumerism, and the healthcare preferences of at least two generations of patients have challenged the strategic validity of this tactic.
The struggle now—and the financial numbers validate that struggle—is that the physician employment model has become extraordinarily expensive and, from observation, does not scale.
Therefore, the relevant business question becomes what are the most efficient and durable customer acquisition and loyalty models now available to hospitals and health systems?
A few more physician employment observations worth sharing:
Primary Care. The physician employment model has generally created a one-size-fits all view of primary care. Consumers, however, want choice. They want 32 flavors, not just vanilla. Alternative primary care models need to match up to fast-changing consumer preferences.
Where Physician Employment Works. In general, the employment model has worked where doctor “shift work” is involved. This includes facility-based specialists such as emergency physicians, anesthesiologists, and hospitalists.
Chronic Care Management. Traditional physician employment models that drive toward doctor-led physical clinics have generally not led to the improved monitoring and treatment of chronic care patient problems. As a result, the chronic care space will likely see significant disruption from virtual and in-home tools.
All in all, the four very smart observations detailed above continue the hospital physician employment conversation. Please feel free to add your thoughts on this or on other topics of hospital management which may be of interest to you. Thanks for reading.
Mountain View, Calif.-based El Camino Health ended the first quarter with an impressive operating margin of 10.2 percent when many health systems saw their margins hover above zero or fall into the red. The system’s revenue for the quarter totaled $131,290.
For the nine months ended March 31, the two-hospital system posted an operating gain of $141.4 million on revenue of just over $1 billion.
However, like most health systems, El Camino’s expenses are substantially higher than the same period last year, increasing 10.6 percent year over year for the nine months ending March 31, 2023, to $881.9 million.
The system is making a conscious effort to march down labor costs while also placing a significant emphasis on retention. In June, El Camino agreed a deal to increase pay for nurses by 16 percent over three years.
“Like nearly all hospitals, our nursing staff comprises the largest part of our workforce. With the recruitment of a single nurse estimated to be nearly $60,000, our primary strategy to reduce labor costs is to focus on decreasing turnover,” El Camino CEO Dan Woods told Becker’s.
“Our turnover rate for nurses is just about 8 percent while the turnover rate nationally is still running at 22 percent.”
In March, the system also received a credit rating upgrade from Moody’s, which noted the system’s “superlative cash metrics and operating performance.” Fitch Ratings also revised El Camino’s outlook to positive in February, noting that the system has a history of generating double-digit operating EBITDA margins, driven by a solid market position that features strong demographics and a very healthy payer mix.
Labor costs have spun out of control in the last few years as inflation set in and hospitals relied on contracted travel nurses to combat nationwide workforce shortages.
The secret to lowering labor costs now, hospital CEOs say, is putting a modern spin on a tried-and-true strategy: retention.
Dan Woods, CEO of El Camino Health in Mountain View, Calif., estimates the cost of recruiting a single nurse as being nearly $60,000, which drove his team’s decision to focus on reducing labor costs by decreasing turnover. The nurse turnover rate is around 22 percent nationally, but El Camino has achieved just 8 percent nurse turnover rate through a variety of retention efforts.
“We continue to chip away at our turnover rate by fostering a positive practice environment for our nurses,” said Mr. Woods. “We achieve this by creating structures and enabling processes so our staff are engaged in assisting with making changes within their practice environments. Also, our staffing and scheduling processes promote efficiency while meeting the needs of our staff, which is essential for retention.”
El Camino does have guardrails to ensure nurses don’t self-schedule overtime or other premium pay. Mr. Woods also mentioned positive labor relations as a retention tool.
“We just completed a new three-year agreement with our nursing union prior to the existing contract expiring and without strikes or the acrimony often associated with labor relations,” he said.
David Callendar, MD, president and CEO of Memorial Hermann Health System in Houston also recently told Becker’s the system is relying less on contract labor and increasing retention through its Well Together employee experience model, which allows employees to personalize programs and benefits to meet their individual needs.
“At Memorial Hermann, we believe that investing in our workforce is the most effective approach to managing labor costs,” said Dr. Callendar. “We accomplish this in three ways: one, creating a workplace where all feel valued and welcomed, and diversity is celebrated; two, investing in employee health and wellness programs; and three, providing professional development and career growth opportunities.”
Rochester (N.Y.) Regional Health is transforming its operating model and workforce strategy to offer more flexibility and build a culture valuing team members for retention.
“We’ve created a new in-house agency to significantly reduce our reliance on third-party contracts and improve staff integration within the health system to foster a more robust culture of collaboration, interdependency, alignment and system-ness,” said Richard Davis, PhD, CEO Of Rochester Regional.
Jeffrey P. Gold, chancellor of the University of Nebraska Medical Center in Omaha, said the academic medical center is focused on reducing the cost per unit of labor and lowering the number of units. The hospital is considering several tactics including additional training and mentorship, evaluating its benefits program and productivity across the organization.
The University of Nebraska Medical Center is also evaluating fixed labor cost departments and roles, and slowing or eliminating full-time employee growth to force innovation, organizational redesign, use of technology and productivity gains with staff retained.
Many hospitals are seeing wages increase within their markets, and increasing pay for existing team members is often less expensive than recruiting and onboarding new ones.
“Obviously, compensation is a key element of staffing, and we are working diligently to ensure that we are competitive within our market,” said R. Kyle Cramer, CEO of Day Kimball Health in Putnam, Conn. “Concurrently, we are evaluating how we staff our clinical areas and the mix of professionals we utilize to create a stronger level of team support and patient engagement. Ultimately we see stabilizing our workforce and reducing turnover through retaining strong members of our clinical and operational team as the key to effectively managing labor costs in this new era.”
Paula Ellis, DNP, interim CEO of F.W. Huston Medical Center in Winchester, Kan., said the critical access hospital has salaries in line with competitors but found benefits lagging. The hospital increased 401K match, provided better health insurance rates, improved tuition assistance and added competitive scholarships to keep employees engaged. The hospital also combined four positions into two.
“Staff were willing and able to take on new duties in exchange for a better schedule,” said Dr. Ellis. “We believe the best method to manage labor costs is to retain staff.”
At least 17 health systems announced changes to executive ranks and administration teams in 2023.
The changes come as hospitals continue to grapple with financial challenges, leading some organizations to cut jobs and implement other operational adjustments.
The following changes were announced within the last two months and are summarized below, with links to more comprehensive coverage of the changes.
1. Middletown, N.Y.-based Garnet Healthlaid off 49 employees, including 25 leaders, to offset recent operating losses. The reductions represent 1.13 percent of the organization’s total workforce and $13 million in salaries and benefits.
2. Greensburg, Pa.-based Independence Health Systemlaid off 53 employees and has cut 226 positions — including resignations, retirements and elimination of vacant positions — since January, The Butler Eagle reported June 28. The 226 reductions began at the executive level, with 13 manager positions terminated in March.
3. Coral Gables-based Baptist Health South Florida is offering its executives at the director level and above a “one-time opportunity” to apply for voluntary separation, according to a June 29 Miami Herald report. Decisions on buyout applications will be made during the summer.
4. MultiCare Health System, a 12-hospital organization based in Tacoma, Wash., will lay off 229 employees, or about 1 percent of its 23,000 staff members, including about two dozen leaders, as part of cost-cutting efforts, the health system said June 29. The layoffs primarily affect support departments, such as marketing, IT and finance.
5. Seattle Children’s is eliminating 135 leader roles, citing financial challenges. The management restructuring and reduction affects 1.5 percent of employees across the organization.
6. Bonnie Panlasigui was tapped as the first president of Summa Health System Hospitals.This new role was first announced in October as the Akron, Ohio-based system made 10 changes to its executive team: reshuffling three leaders’ roles, adding three positions and eliminating four.
7. Allentown, Pa.-based Lehigh Valley Health Network named two new regional and hospital presidents. Bob Begliomini, PharmD, was appointed president of Lehigh Valley Hospital-Cedar Crest campus in Allentown, according to a news release shared with Becker’s. He will also lead the health system’s Lehigh region, which includes four hospital campuses. Jim Miller, CRNA, was selected to replace Mr. Begliomini as president of the Muhlenberg hospital. He was also named president of the health system’s Northampton region, which includes three hospitals, Muhlenberg being one of them.
8. McLaren St. Luke’s Hospital in Maumee, Ohio, will lay off 743 workers, including 239 registered nurses, when it permanently closes this spring. Other affected roles include physical therapists, radiology technicians, respiratory therapists, pharmacists and pharmacy support staff, and nursing assistants. The hospital’s COO is also affected, and a spokesperson for McLaren Health Care told Becker’s other senior leadership roles are also affected.
9. Habersham Medical Center in Demorest, Ga., laid off four executives. The layoffs were part of cost-cutting measures before the hospital joined Gainesville-based Northeast Georgia Health System.
10. Grand Forks, N.D.-based Altru Health announced it would trim its executive team as its new hospital project moves forward. The health system is trimming its executive team from nine to six and incentivizing 34 other employees to take early retirement.
11. Scripps Healtheliminated 70 administrative roles, according to WARN documents filed by the San Diego-based health system in March. The layoffs took effect May 8 and affect corporate positions in San Diego and La Jolla, Calif.
12. Columbia-based University of Missouri Health Care announced it would eliminate five hospital leadership positions across the organization. According to MU Health Care, the move is a result of restructuring “to better support patients and the future healthcare needs of Missourians.”
13. Winston-Salem, N.C.-based Novant Healthlaid off about 50 workers, including C-level executives, the health system confirmed to Becker’s March 29. The layoffs affected Jesse Cureton, the health system’s executive vice president and chief consumer officer since 2013; Angela Yochem, its executive vice president and chief transformation and digital officer since 2020; and Paula Dean Kranz, vice president of innovation enablement and executive director of the Novant Health Innovation Labs.
14. Philadelphia-based Penn Medicine announced that it would eliminate administrative positions. The change is part of a reorganization plan to save the health system $40 million annually, the Philadelphia Business Journal reported March 13. Kevin Mahoney, CEO of the University of Pennsylvania Health System, told Penn Medicine’s 49,000 employees changes include the elimination of a “small number of administrative positions which no longer align with our key objectives,” according to the publication.
15. Sovah Health, part of Brentwood, Tenn.-based Lifepoint Health, eliminated the COO positions at its Danville and Martinsville, Va., campuses. The responsibilities of both COO roles are now spread across members of the existing administrative team.
16. Valley Health, a six-hospital health system based in Winchester, Va., eliminated 31 administrative positions. The job cuts are part of the consolidation of the organization’s leadership team and administrative roles. They were announced internally on Feb. 28.
17. Roseville, Calif.-based Adventist Healthannounced it would transition from seven networks of care to five systemwide to reduce costs and strengthen operations. Under the reorganization, the health system will have separate networks for Northern California, Central California, Southern California, Oregon and Hawaii. The reorganization will result in job cuts, including reducing administration by more than $100 million.
That’s the amount you arrive at if you multiply the number of physicians employed by hospitals and health systems (approximately 341,200 as of January 2022, according to data from the Physicians Advocacy Institute and Avalere) by the median $306,362 subsidy—or loss—reported in our Q1 2023 Physician Flash Report.
Subsidizing physician employment has been around for a long time and such subsidies were historically justified as a loss leader for improved clinical services, the potential for increased market share, and the strengthening of traditionally profitable services.
But I am pretty sure the industry did not have $104 billion in losses in mind when the physician employment model first became a key strategic element in the hospital operating model. However, the upward reset in expenses brought on by the pandemic and post-pandemic inflation has made many downstream hospital services that historically operated at a profit now operate at breakeven or even at a loss. The loss leader physician employment model obviously no longer works when it mostly leads to more losses.
This model is clearly broken and in demand of a near-term fix. Perhaps the critical question then is how to begin? How to reconsider physician employment within the hospital operating plan?
Out of the box, rethink the physician productivity model. Our most recent Physician Flash Report data shows that for surgical specialties, there was a median $77 net patient revenue per provider wRVU. For the same specialties, there was a median $80 provider paid compensation per provider wRVU. In other words, before any other expenses are factored in, these specialties are losing $3 per wRVU on paid compensation alone. Getting providers to produce more wRVUs only makes the loss bigger.
It’s the classic business school 101 problem.
If a factory is losing $5 on every widget it produces, the answer is not to produce more widgets. Rather, expenses need to come down, whether that is through a readjustment of compensation, new compensation models that reward efficiency, or the more effective use of advanced practice providers.
Second, a number of hospital CEOs have suggested to me that the current employed physician model is quite past its prime. That model was built for a system of care that included generally higher revenues, more inpatient care, and a greater proportion of surgical vs. medical admissions. But overall, these trends were changing and then were accelerated by the Covid pandemic. Inpatient revenue has been flat to down. More clinical work continues to shift to the outpatient setting and, at least for the time being, medical admissions have been more prominent than before the pandemic.
Taking all this into account suggests that in many places the employed physician organizational and operating model is entirely out of balance. One would offer the calculated guess that there are too many coaches on the team and not enough players on the field. This administrative overhead was seemingly justified in a different loss leader environment but now it is a major contributor to that $104 billion industry-wide loss previously calculated.
Finally, perhaps the very idea of physician employment needs to be rethought.
My colleagues Matthew Bates and John Anderson have commented that the “owner” model is more appealing to physicians who remain independent then the “renter” model. The current employment model offers physicians stability of practice and income but appears to come at the cost of both a loss of enthusiasm and lost entrepreneurship. The massive losses currently experienced strongly suggest that new models are essential to reclaim physician interest and establish physician incentives that result in lower practice expenses, higher practice revenues, and steadily reduced overall subsidies.
Please see this blog as an extension of my last blog, “America’s Hospitals Need a Makeover.”It should be obvious that by analogy we are not talking about a coat of paint here or even new appliances in the kitchen.
The financial performance of America’s hospitals has exposed real structural flaws in the healthcare house. A makeover of this magnitude is going to require a few prerequisites:
Don’t start designing the renovation unless you know specifically where profitability has changed within your service lines and by explicitly how much. Right now is the time to know how big the problem is, where those problems are located, and what is the total magnitude of the fix.
The Board must be brought into the discussion of the nature of the physician employment problem and the depth of its proposed solutions. Physicians are not just “any employees.” They are often the engine that runs the hospital and must be afforded a level of communication that is equal to the size of the financial problem. All of this will demand the Board’s knowledge and participation as solutions to the physician employment dilemma are proposed, considered, and eventually acted upon.
The basic rule of home renovation applies here as well: the longer the fix to this problem is delayed the harder and more expensive the project becomes. The losses set out here certainly suggest that physician employment is a significant contributing factor to hospitals’ current financial problems overall. It would be an understatement to say that the time to get after all of this is right now.
A number of hospitals and health systems are trimming their workforces or jobs due to financial and operational challenges.
Below are workforce reduction efforts or job eliminations that were announced within the past year and/or take effect later in 2023.
Editor’s Note: This webpage was updated June 30 and will continue to be updated.
1. Coral Gables-based Baptist Health South Florida is offering its executives at the director level and above a “one-time opportunity” to apply for voluntary separation, according to a June 29 Miami Herald report. Decisions on buyout applications will be made during the summer.
2. MultiCare Health System, a 12-hospital organization based in Tacoma, Wash., will lay off 229 employees, or about 1 percent of its 23,000 staff members, including about two dozen leaders, as part of cost-cutting efforts, the health system said June 29. The layoffs primarily affect support departments, such as marketing, IT and finance.
3. Greensburg, Pa.-based Independence Health System laid off 53 employees and has cut 226 positions — including resignations, retirements and elimination of vacant positions — since January, The Butler Eagle reported June 28. The 226 reductions began at the executive level, with 13 manager positions terminated in March.
4. Billings (Mont.) Clinic will lay off workers as part of a restructuring plan to address financial and operational headwinds in today’s healthcare environment, the organization confirmed. The layoffs are expected to affect approximately 27 or fewer positions.
5. Melbourne, Fla.-based Health First is eliminating some positions and leaving open ones vacant, Florida Today reported June 21. Seventeen jobs will be cut and 36 will be left unfilled, according to Paula Just, the health system’s chief experience officer.
6. Pittsburgh-based Highmark Health laid off 118 employees on June 21, including two from Allegheny Health Network, a spokesperson for the health system told Becker’s. The layoffs follow the health system’s cutbacks in March and April, according to the Pittsburgh Business Times. Highmark laid off 141 workers earlier this year.
7. Vibra Hospital of Western Massachusetts, a long-term-acute care hospital in Springfield, will lay off 87 employees by Aug. 15 ahead of the facility’s planned closure. About 30 patients will be relocated to Baystate Health’s Valley Springs Behavioral Health Hospital in Holyoke, Mass., which will open in August.
8. Cortez, Colo.-based Southwest Memorial Hospital laid off nine people to help ensure the hospital is staffed appropriately, and create financial stability for the future, a spokesperson confirmed to Becker’s. The spokesperson, Chuck Krupa, said the layoffs occurred June 14 and included administrative workers. No bedside care positions were affected.
9. Henry Mayo Newhall Hospital in Valencia, Calif., is making “a little over 100” layoffs amid financial challenges, spokesperson Patrick Moody confirmed to Becker’s. Mr. Moody said the layoffs affect workers “in a wide range of hospital departments.” This includes some management-level employees. The hospital, which has about 1,800 employees total, is not providing specific numbers for specific job titles or departments.
10. Dartmouth Health is laying off 75 workers and eliminating 100 job vacancies. The layoffs came after the Lebanon, N.H.-based health system implemented a performance improvement plan in November.
11. Seattle Children’s is eliminating 135 leader roles, citing financial challenges. The management restructuring and reduction affects 1.5 percent of employees across the organization.
12. White Rock (Texas) Medical Center laid off 30 workers across 28 departments. The layoffs include clinical and administrative roles.
13. Jackson, Miss.-based St. Dominic Health Services is laying off 157 workers and ending behavioral health services. The reduction represents 5.5 percent of the hospital’s workforce.
14. Danville, Pa.-based Geisinger laid off 47 employees from its IT department. The reduction is part of a restructuring plan to offset high labor and supply costs.
15. Cascade Behavioral Health Hospital in Tukwila, Wash., is winding down operations and laying off 288 employees. The 137-bed psychiatric facility is slated to close by July 31.
16. Cambridge (Mass.) Health Alliance is laying off 69 employees, reducing the hours of 15 others and eliminating 170 open positions, according to The Boston Globe. The reductions are primarily in management, administrative and support areas, a health system spokesperson told Becker’s.
17. Wenatchee, Wash.-based Confluence Health has eliminated its chief operating officer amid restructuring efforts and financial pressures, the health system confirmed to Becker’s May 16.
18. Conemaugh Memorial Medical Center, a Duke LifePoint hospital in Johnstown, Pa., has laid off less than 1 percent of its workforce, the hospital confirmed to Becker’s May 15.
19. Community Health Network, a nonprofit health system based in Indianapolis, plans to cut an unspecified number of jobs as it restructures its workforce and makes organizational changes. The health system confirmed the job cuts in a statement shared with Becker’s on May 11. It did not say how many jobs would be cut or which positions would be affected.
20. New Orleans-based Ochsner Health eliminated 770 positions, or about 2 percent of its workforce, on May 11. This is the largest layoff to date for the health system.
21. Cedars-Sinai Medical Center eliminated the positions of 131 employees and cut about two dozen other jobs at related Cedars-Sinai facilities, a spokesperson confirmed via a statement shared with Becker’s May 7. The Los Angeles-based organization said reductions represent less than 1 percent of the workforce and apply to management and non-management roles primarily in non-patient care jobs.
22. Rochester (N.Y.) Regional Health is eliminating about 60 positions. A statement from RRH said the changes affect less than one-half percent of the system population, mostly in nonclinical and management positions.
23. Memorial Health System laid off fewer than 90 people, or less than 2 percent of its workforce.The Gulfport, Miss.-based health system said May 2 that most of the affected positions are nonclinical or management roles, and the majority do not involve direct patient care.
24. Monument Health laid off at least 80 employees, or about 2 percent of its workforce. The Rapid City, S.D.-based system said positions are primarily corporate service roles and will not affect patient services. Unfilled corporate service positions were also eliminated.
25. Habersham Medical Center in Demorest, Ga., laid off four executives. The layoffs are part of cost-cutting measures before the hospital joins Gainesville-based Northeast Georgia Health System in July, nowhaberbasham.com reported April 27.
26. Scripps Health is eliminating 70 administrative roles, according to WARN documents filed by the San Diego-based health system in March. The layoffs take effect May 8 and affect corporate positions in San Diego and La Jolla, Calif.
27. Trinity Health Mid-Atlantic, part of Livonia, Mich.-based Trinity Health, eliminated fewer than 40 positions, a spokesperson confirmed to Becker’s April 24. The layoffs represent 0.5 percent of the health system’s approximately 7,000-person workforce.
28. PeaceHealth eliminated 251 caregiver roles across multiple locations. The Vancouver, Wash.-based health system said affected roles include 121 from Shared Services, which supports its 16,000 caregivers in Washington, Oregon and Alaska.
29. Toledo, Ohio-based ProMedica plans to lay off 26 skilled nursing support staff. The layoffs, effective in June, affect 20 employees who work remotely across the U.S, and six who work at the ProMedica Summit Center in Toledo, according to a Worker Adjustment and Retraining Notification filed April 18. Most affected positions support sales, marketing and administrative functions for the skilled nursing facilities, Promecia told Becker’s.
30. Northern Inyo Healthcare District, which operates a 25-bed critical access hospital in Bishop, Calif., anticipates eliminating about 15 positions, or less than 4 percent of its 460-member workforce, by April 21, a spokesperson confirmed to Becker’s. The layoffs include nonclinical roles within support and administration, according to a news release. No further details were provided about specific positions affected.
31. West Reading, Pa.-based Tower Health is eliminating 100 full-time equivalent positions. The move will affect 45 individuals, according to an April 13 news release the health system shared with Becker’s. The other 55 positions are either recently vacated or involve individuals who plan to retire in the coming weeks and months.
32. Grand Forks, N.D.-based Altru Health is trimming its executive team as its new hospital project moves forward. The health system is trimming its executive team from nine to six and incentivizing 34 other employees to take early retirement.
33. Tacoma, Wash.-based Virginia Mason Franciscan Health laid off nearly 400 employees, most of whom are in non-patient-facing roles. The job cuts affected less than 2 percent of the health system’s 19,000-plus workforce.
34. Katherine Shaw Bethea Hospital in Dixon, Ill., will lay off 20 employees, citing financial headwinds affecting health organizations across the U.S. It will also leave other positions unfilled to reduce expenses amid rising labor and supply costs and reductions in payments by insurance plans. Affected employees largely work in administrative support areas and not direct patient care.
35. Danbury, Conn.-based Nuvance Health will close a 100-bed rehabilitation facility in Rhinebeck, N.Y., resulting in 102 layoffs. The layoffs are effective April 12, according to the Daily Freeman.
36. Charleston, S.C.-based MUSC Health University Medical Center laid off an unspecified number of employees from its Midlands hospitals in the Columbia, S.C. area. Division President Terry Gunn also resigned after the facilities missed budget expectations by $40 million in the first six months of the fiscal year, The Post and Courier reported March 30.
37. Winston-Salem, N.C.-based Novant Health laid off about 50 workers, including C-level executives, the health system confirmed to Becker’s March 29. The layoffs affected Jesse Cureton, the health system’s executive vice president and chief consumer officer since 2013; Angela Yochem, its executive vice president and chief transformation and digital officer since 2020; and Paula Dean Kranz, vice president of innovation enablement and executive director of the Novant Health Innovation Labs.
38. Penn Medicine Lancaster (Pa.) General Health eliminated fewer than 65 jobs, or less than 1 percent of its workforce of about 9,700, the health system confirmed to Becker’s March 30. The layoffs include support, administrative and executive roles, and COVID-19-related support staff, spokesperson John Lines said, according to lancasteronline.com. Mr. Lines did not provide a specific number of affected workers.
39. McLaren St. Luke’s Hospital in Maumee, Ohio, will lay off 743 workers, including 239 registered nurses, when it permanently closes this spring. Other affected roles include physical therapists, radiology technicians, respiratory therapists, pharmacists and pharmacy support staff, and nursing assistants. The hospital’s COO is also affected, and a spokesperson for McLaren Health Care told Becker’s other senior leadership roles are also affected.
40. Bellevue, Wash.-based Overlake Medical Center and Clinics laid off administrative staff, the health system confirmed to the Puget Sound Business Journal. The layoffs, which occurred earlier this year, included 30 workers across Overlake’s human resources, information technology and finance departments, a spokesperson said, according to the publication. This represents about 6 percent of the organization’s administrative workforce. Overlake’s website says it employs more than 3,000 people total.
41. Columbia-based University of Missouri Health Care is eliminating five hospital leadership positions across the organization, spokesperson Eric Maze confirmed to Becker’s March 20. Mr. Maze did not specify which roles are being eliminated saying that the organization won’t address individual personnel actions. According to MU Health Care, the move is a result of restructuring “to better support patients and the future healthcare needs of Missourians.”
42. Greensboro, N.C.-based Cone Health eliminated 68 senior-level jobs. The job eliminations occurred Feb. 21, Cone Health COO Mandy Eaton told The Alamance News. Of the 68 positions eliminated, 21 were filled. Affected employees were offered severance packages.
43. The newly merged Greensburg, Pa.-based organization made up of Excela Health and Butler Health System eliminated 13 filled managerial jobs. The affected employees and positions are from across both sides of the new organization, Tom Chakurda, spokesperson for the Excela-Butler enterprise, confirmed to Becker’s. The positions were in various support functions unrelated to direct patient care.
44. Crozer Health, a four-hospital system based in Upland, Pa., is laying off roughly 215 employees amid financial challenges. The system announced the layoffs March 15 as part of its “operational restructuring plan” that “focuses on removing duplication in administrative oversight and discontinuing underutilized services.” Affected employees represent about 4 percent of the organization’s workforce.
45. Philadelphia-based Penn Medicine is eliminating administrative positions. The change is part of a reorganization plan to save the health system $40 million annually, the Philadelphia Business Journal reported March 13. Kevin Mahoney, CEO of the University of Pennsylvania Health System, told Penn Medicine’s 49,000 employees last week that changes include the elimination of a “small number of administrative positions which no longer align with our key objectives,” according to the publication. The memo did not indicate the exact number of positions that were eliminated.
46. Sovah Health, part of Brentwood, Tenn.-based Lifepoint Health, eliminated the COO positions at its Danville and Martinsville, Va., campuses. The responsibilities of both COO roles will now be spread across members of the existing administrative team.
47. Valley Health, a six-hospital health system based in Winchester, Va., eliminated 31 administrative positions. The job cuts are part of the consolidation of the organization’s leadership team and administrative roles.
48. Marshfield (Wis.) Clinic Health System said it would lay off 346 employees, representing less than 3 percent of its employee base.
50. Roseville, Calif.-based Adventist Health plans to go from seven networks of care to five systemwide to reduce costs and strengthen operations. The reorganization will result in job cuts, including reducing administration by more than $100 million.
51. Arcata, Calif.-based Mad River Community Hospital is cutting 27 jobs as it suspends home health services.
52. Hutchinson (Kan.) Regional Medical Center laid off 85 employees, a move tied to challenges in today’s healthcare environment.
53. Oklahoma City-based OU Health eliminated about 100 positions as part of an organizational redesign to complete the integration from its 2021 merger.
54. Memorial Sloan Kettering Cancer Center announced it would lay off to reduce costs amid widespread hospital financial challenges. The layoffs are spread across 14 sites in New York City, and equate to about 1.8 percent of Memorial Sloan’s 22,500 workforce.
55. St. Louis-based Ascension completed layoffs in Texas, the health system confirmed in January. A statement shared with Becker’s says the layoffs primarily affected nonclinical support roles. The health system declined to specify to Becker’s the number of employees or positions affected.
57. Chillicothe, Ohio-based Adena Health System announced it would eliminate 69 positions — 1.6 percent of its workforce — and send 340 revenue cycle department employees to Ensemble Health Partners’ payroll in a move aimed to help the health system’s financial stability.
58. Ascension St. Vincent’s Riverside in Jacksonville, Fla., will end maternity care at the hospital, affecting 68 jobs, according to a Workforce Adjustment and Retraining Notification filed with the state Jan. 17. The move will affect 62 registered nurses as well as six other positions.
59. Visalia, Calif.-based Kaweah Health said it aimed to eliminate 94 positions as part of a new strategy to reduce labor costs. The job cuts come in addition to previously announced workforce reductions; the health system already eliminated 90 unfilled positions and lowered its workforce by 106 employees.
60. Oklahoma City-based Integris Health said it would eliminate 200 jobs to curb expenses. The eliminations include 140 caregiver roles and 60 vacant jobs.
61. Toledo, Ohio-based ProMedica announced plans to lay off 262 employees, a move tied to its exit from a skilled-nursing facility joint venture late last year. The layoffs will take effect between March 10 and April 1.
62. Employees at Las Vegas-based Desert Springs Hospital Medical Center were notified of layoffs coming to the facility, which will transition to a freestanding emergency department. There are 970 employees affected. Desert Springs is part of the Valley Health System, a system owned and operated by King of Prussia, Pa.-based Universal Health Services.
63. Philadelphia-based Jefferson Health plans to go from five divisions to three in an effort to flatten management and become more efficient. The reorganization will result in an unspecified number of job cuts, primarily among executives.
64. Pikeville (Ky.) Medical Center said it would lay off 112 employees as it outsources its environmental services department. The 112 layoffs were effective Jan. 1, 2023.
65. Southern Illinois Healthcare, a four-hospital system based in Carbondale, announced it would eliminate or restructure 76 jobs in management and leadership. The 76 positions fall under senior leadership, management and corporate services. Included in that figure are 33 vacant positions, which will not be filled. No positions in patient care are affected.
66. Citing a need to further reduce overhead expenses and support additional investments in patient care and wages, Traverse City, Mich.-based Munson Health said it would eliminate 31 positions and leave another 20 jobs unfilled. All affected positions are in corporate services or management. The layoffs represent less than 1 percent of the health system’s workforce of nearly 8,000.
67. West Reading, Pa.-based Tower Health on Nov. 16 laid off 52 corporate employees as the health system shrinks from six hospitals to four. The layoffs, which are expected to save $15 million a year, account for 13 percent of Tower Health’s corporate management staff.
68. Sioux Falls, S.D.-based Sanford Health announced layoffs affecting an undisclosed number of staff in October, a decision its CEO said was made “to streamline leadership structure and simplify operations” in certain areas. The layoffs primarily affect nonclinical areas.
69. St. Vincent Charity Medical Center in Cleveland closed its inpatient and emergency room care Nov. 11, four days before originally planned — and laid off 978 workers in doing so. After the transition, the Sisters of Charity Health System will offer outpatient behavioral health, urgent care and primary care.
More than a year after launching an in-house travel staffing agency, UPMC is adding a new regional approach to the effort.
Maribeth McLaughlin, MPM, BSN, RN, chief nursing executive for the Pittsburgh-based health system, told Becker’s the approach provides a new option for nurses and surgical technologists who desire to travel.
“Our overall travel program, when you travel for us, you travel across our hospitals in New York, Maryland and Pennsylvania,” she said. “And now we are launching a regional travel strategy where some staff can choose to travel only within certain regions.”
UPMC initially announced in December 2021 that it had created UPMC Travel Staffing, a new in-house travel staffing agency to address a nursing shortage and to attract and retain workers.
Through the agency, nurses and surgical technologists earn $85 an hour and $63 an hour, respectively, in addition to a $2,880 stipend at the beginning of each six-week assignment.
Ms. McLaughlin said the rate is lower — about $60 an hour — for those who opt for the regional approach.
As of June 1, UPMC has hired more than 700 staff into the in-house travel staffing agency, with 60 percent of those workers being external hires, according to Ms. McLaughlin. And there have been fewer workers leaving UPMC to go to other travel agencies.
“One of my goals since I’ve taken this role is to really look at building in as many flexible programs as I could for staff,” said Ms. McLaughlin, who has served in her current role since August 2022. “I think as we came out of the pandemic, it’s clear to me that work-life harmony means something different to staff today than it maybe meant when I was a young staff nurse years ago, and that we need to have as much flexibility and as many different programs as we can.”
She said UPMC Travel Staffing has delivered this flexibility and allowed the health system to cancel about 90 contracts with external travel agencies. Additionally, some external travelers have now moved into UPMC’s in-house agency. Ms. McLaughlin expects more to join the in-house agency now that UPMC has launched the regional approach.
“We’re launching a win-back program where we’re going out and trying to see some of the people who we know we lost and see if they’re interested in coming back closer to home and traveling closer to home,” she explained.
Still, she acknowledged some of the challenges along the way.
“Our IT department built us an app to be able to manage all of this because, as you can imagine, we have external travel, internal travelers, core staff and at times it could get a little confusing,” said Ms. McLaughlin. “So we’ve been able to build that to be able to figure out the best ways to assign the staff where the greatest needs are.”
Another challenge she noted is that shifts for workers from external travel agencies are often 12 weeks, while shifts with UPMC Travel Staffing are six weeks. She said this is a purposeful move because those in UPMC Travel Staffing receive benefits and are considered UPMC employees, rather than receiving an hourly rate.
“Overall, it’s been a really successful program for us because it’s allowed us to look at things in a different way,” said Ms. McLaughlin. “It’s a central function. It’s not something we did and farmed out to every hospital to administer themselves. We did it as a system and as a core, which I also think is important.”
Now, she said she’s excited about the new regional approach and the opportunities it presents for recruiting and retention.
“We’re growing our own students, we’re bringing in all these students, and we’re not saying, ‘You have to just work here.’ We’re saying, ‘You can work for us at UPMC, and here are all the options. You can even be a traveler with us,'” she said.
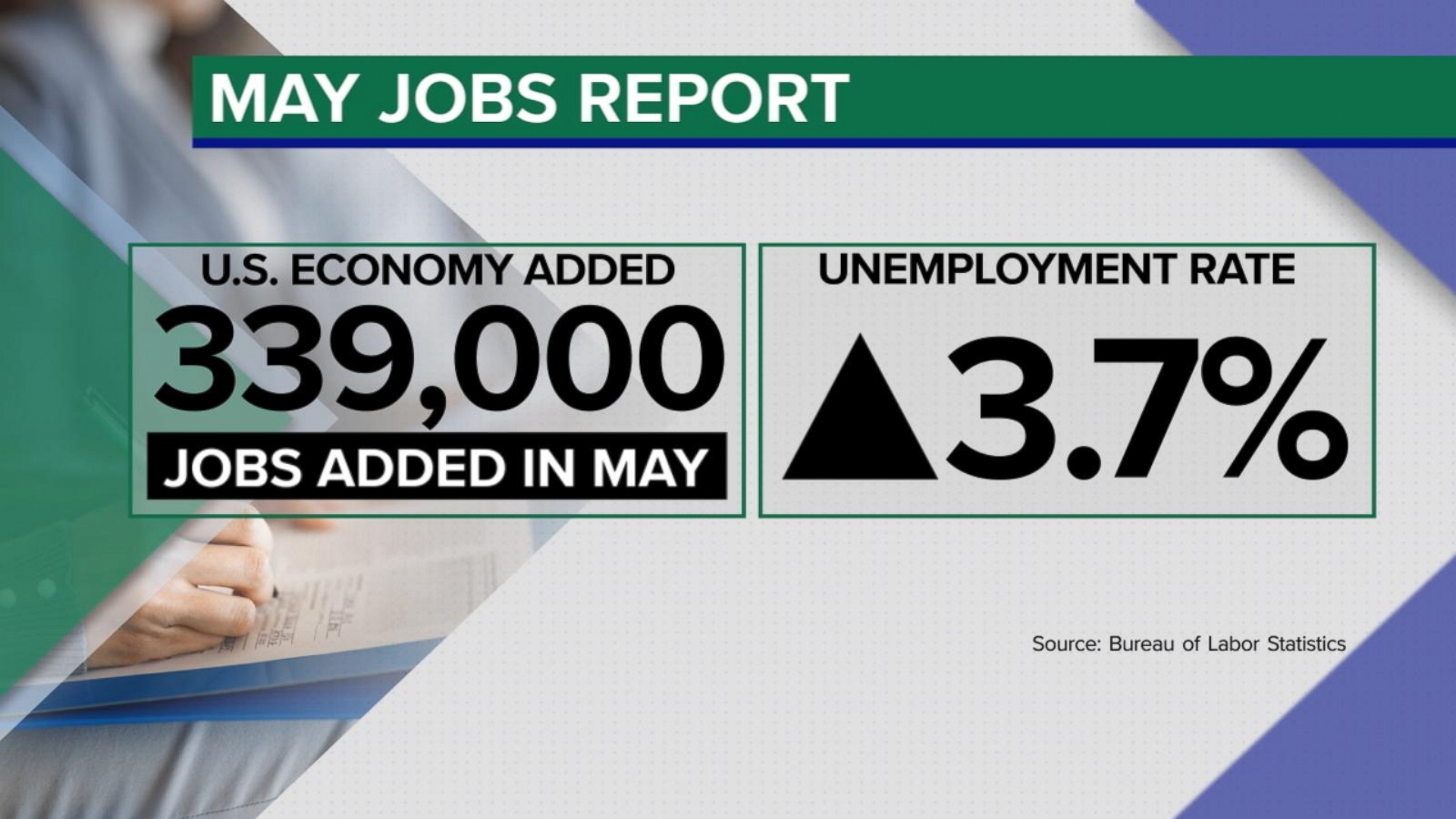
The U.S. economy added 339,000 jobs in May, while the unemployment rate jumped to 3.7% from 3.4%, the Labor Department said Friday.
Why it matters:
Job gains came in well above forecasters’ expectations — the latest sign that the economy is still underpinned by a hot labor market.
Economists expected a gain of 190,000 jobs last month. The May jobs figures are a pickup from the 294,000 added in April, which was revised up by 41,000. Job gains in March were revised up, too.
Details:
Economic policymakers have kept a close eye on other details from the payrolls report — whether more Americans are joining the workforce and how quickly pay is rising.
The labor force participation rate — the share of workers with a job or hunting for one — held at 62.6% in May.
Meanwhile, average hourly earnings, a measure of pay, rose by 0.3% in May. Compared to the same period a year ago, wages are up 4.3%.
What we’re watching:
The May jobs report is among the final data points Federal Reserve officials will consider before deciding whether to continue the interest rate hiking campaign that began more than a year ago.
Inflation remains too high, and there are concerns that rapid price gains are being fueled by the tight labor market and strong consumer demand.
Still, a top Fed official this week signaled the central bank may skip a rate hike at its meeting later this month.