
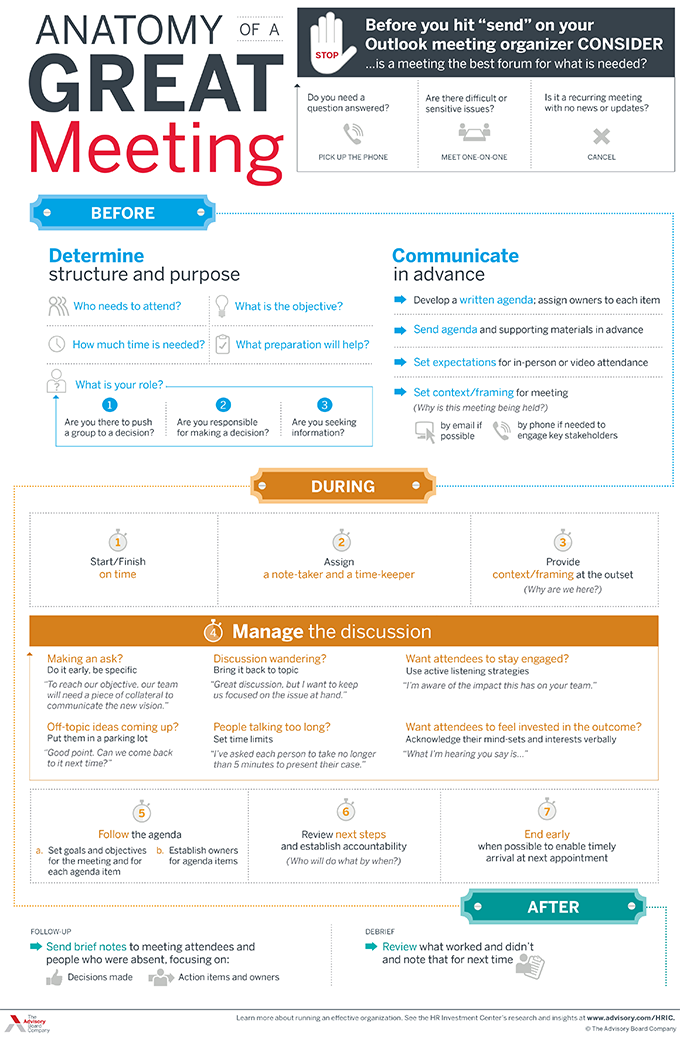
Anatomy of a Great Meeting

With input from stakeholders across the industry, Modern Healthcare outlines six challenges health care is likely to face in 2023—and what leaders can do about them.
In 2023, health systems will likely continue to face financial difficulties due to ongoing staffing problems, reduced patient volumes, and rising inflation.
According to Tina Wheeler, U.S. health care leader at Deloitte, hospitals can expect wage growth to continue to increase even as they try to contain labor costs. They can also expect expenses, including for supplies and pharmaceuticals, to remain elevated.
Health systems are also no longer able to rely on federal Covid-19 relief funding to offset some of these rising costs. Cuts to Medicare reimbursement rates could also negatively impact revenue.
“You’re going to have all these forces that are counterproductive that you’re going to have to navigate,” Wheeler said.
In addition, Erik Swanson, SVP of data and analytics at Kaufman Hall, said the continued shift to outpatient care will likely affect hospitals’ profit margins.
“The reality is … those sites of care in many cases tend to be lower-cost ways of delivering care, so ultimately it could be beneficial to health systems as a whole, but only for those systems that are able to offer those services and have that footprint,” he said.
Although hospital transactions have slowed in the last few years, market watchers say mergers are expected to rebound as health systems aim to spread their growing expenses over larger organizations and increase their bargaining leverage with insurers.
“There is going to be some organizational soul-searching for some health systems that might force them to affiliate, even though they prefer not to,” said Patrick Cross, a partner at Faegre Drinker Biddle & Reath. “Health systems are soliciting partners, not because they are on the verge of bankruptcy, but because they are looking at their crystal ball and not seeing an easy road ahead.”
Financial challenges may also lead more physician practices to join health systems, private-equity groups, larger practices, or insurance companies.
“Many independent physicians are really struggling with their ability to maintain their independence,” said Joshua Kaye, chair of U.S. health care practice at DLA Piper. “There will be a fair amount of deal activity. The question will be more about the size and specialty of the practices that will be part of the next consolidation wave.”
According to data from Fitch Ratings, health care job openings reached an all-time high of 9.2% in September 2022—more than double the average rate of 4.2% between 2010 and 2019. With this trend likely to continue, organizations will need to find effective ways to recruit and retain workers.
Currently, some organizations are upgrading their processes and technology to hire people more quickly. They are also creating service-level agreements between recruiting and hiring teams to ensure interviews are scheduled within 48 hours or decisions are made within 24 hours.
Eric Burch, executive principal of operations and workforce services at Vizient, also predicted that there will be a continued need for contract labors, so health systems will need to consider travel nurses in their staffing plans.
“It’s really important to approach contract labor vendors as a strategic partner,” Burch said. “So when you need the staff, it’s a partnership and they’re able to help you get to your goals, versus suddenly reaching out to them and they don’t know your needs when you’re in crisis.”
When it comes to retention, Tochi Iroku-Malize, president of the American Academy of Family Physicians (AAFP), said health systems are adequately compensated for their work and have enough staff to alleviate potential burnout.
AAFP also supports legislation to streamline prior authorization in the Medicare Advantage program and avoid additional cuts to Medicare payments, which will help physicians provide care to patients with less stress.
A potential recession, along with the ensuing job cuts that typically follow, would limit insurers’ commercial business, which is their most profitable product line. Instead, many people who lose their jobs will likely sign up for Medicaid plans, which is much less profitable.
Because of increased labor, supply, and infrastructure costs, Brad Ellis, senior director at Fitch Ratings, said providers could pressure insurers into increasing the amount they pay for services. This will lead insurers to passing these increased costs onto members’ premiums.
Currently, Ellis said insurers are keeping an eye on how legislators finalize rules to implement the No Surprise Act’s independent resolution process. Regulators will also begin issuing fines for payers who are not in compliance with the law’s price transparency requirement.
Much like 2022, investment in digital health is likely to remain strong but subdued in 2023.
“You’ll continue to see layoffs, and startup funding is going to be hard to come by,” said Russell Glass, CEO of Headspace Health.
However, investors and health care leaders say they expect a strong market for digital health technology, such as tools for revenue cycle management and hospital-at-home programs.
According to Julian Pham, founding and managing partner at Third Culture Capital, he expects corporations such as CVS Health to continue to invest in health tech companies and for there to be more digital health mergers and acquisitions overall.
In addition, he predicted that investors, pharmaceutical companies, and insurers will show more interest in digital therapeutics, which are software applications prescribed by clinicians.
“As a physician, I’ve always dreamed of a future where I could prescribe an app,” Pham said. “Is it the right time? Time will tell. A lot needs to happen in digital therapeutics and it’s going to be hard.”
This year, CMS will continue rolling out new health equity initiatives and quality measurements for providers and insurers who serve marketplace, Medicare, and Medicaid beneficiaries. Some new quality measures include maternal health, opioid related adverse events, and social need/risk factor screenings.
CMS, the Joint Commission, and the National Committee for Quality Assurance are also partnering together to establish standards for health equity and data collection.
In addition, HHS is slated to restore a rule under the Affordable Care Act that prohibits discrimination based on a person’s gender identity or sexual orientation. According to experts, this rule may conflict with recently passed state laws that ban gender-affirming care for minors.
“It’s something that’s going to bear out in the courts and will likely lack clarity. We’ll see differences in what different courts decide,” said Lindsey Dawson, associate director of HIV policy and director of LGBTQ health policy at the Kaiser Family Foundation. “The Supreme Court acknowledged that there was this tension. So it’s an important place to watch and understand better moving forward.”

Segundo, Calif.-based Pipeline Health, now a five-hospital system, exited bankruptcy Feb. 7
Former CFO Robert Allen has replaced Andrei Soran as CEO. Mr. Allen previously served as group CEO for CHA Hollywood Presbyterian Medical Center in Los Angeles. He also held CFO positions at San Francisco-based Dignity Health and Keck Medical Center of USC, Valley Presbyterian Hospital and Sherman Oaks Hospital and Health Center, all in Los Angeles.
Four other leaders have also been appointed to executive positions:
Pipeline filed for Chapter 11 bankruptcy Oct. 2, and its plan to emerge was confirmed Jan. 13. Over the last few months, the system has worked through a restructuring process that included selling two Chicago hospitals, evaluating vendor contracts, creating a business plan with realistic financial goals and securing financial agreements with key stakeholders. It now owns four hospitals in the Los Anegeles area and one in Dallas.
In a memo sent Feb. 7 to employees and affiliated physicians, Mr. Allen wrote, “Hospitals across the country face similar financial challenges. You should take great pride in knowing that our company stands on solid footing now with a clear path forward. And I am proud — and grateful — that our employees and physicians have stayed with us, keeping their focus on delivering quality patient care throughout this period of uncertainty.”
Pipeline’s path forward includes a renewed commitment to quality care and an improved workforce strategy, according to Mr. Allen.
“That means providing the right care in the right place at the right time to every patient who comes to us and ensuring timely patient discharges,” he said in a Feb. 7 news release. “We also will focus on enhanced workforce management to care for the patients we serve and to enhance our critical relationships with our employees.”

There is no shortage of challenges to confront in healthcare today, from workforce shortages and burnout to innovation and health equity (and so much more). We’re committed to giving industry leaders a platform for sharing best practices and exchanging ideas that can improve care, operations and patient outcomes.
Check out this podcast interview with Ketul J. Patel, CEO at Virginia Mason Franciscan Health and division president, Pacific Northwest at CommonSpirit Health, for his insights on where healthcare is headed in the future.
In this episode, we are joined by Ketul J. Patel, Division President, Pacific Northwest; Chief Executive Officer, CommonSpirit Health; Virginia Mason Franciscan Health, to discuss his background & what led him to executive healthcare leadership, challenges surrounding workforce shortages, the importance of having a strong workplace culture, and more.

Payers, pharmacy benefit managers and drug manufacturers are no strangers to heavy criticism from the public and providers alike. Now another sector of the healthcare system has found itself increasingly caught in the crosshairs of constituents looking to point a finger for the rising cost of care: hospitals.
As sharp words against the industry bubble up more often and encompass a wider variety of issues, it marks an important turn in the ethos of American healthcare. Most policymakers have historically wanted hospitals on their side, and health systems are often the largest employer within their communities and in many states.
“In my career, I’ve never seen things more aligned to the detriment of hospitals than it is now,” Paul Keckley, PhD, said. Dr. Keckley is a widely known industry analyst and editor of The Keckley Report, a weekly newsletter discussing healthcare policy and current trends.
Confidence in the medical system as a whole fell from 51 percent in 2020 to a record low of 38 percent in 2022. Though the healthcare system is among all major U.S. institutions facing record-low public confidence, are hospitals ready for an era of widespread distrust?
“We’re going into hospital purgatory. It’s a period in which old rules may not work in the future,” Dr. Keckley said. “The only thing we know for sure is that it’s not going to get easier.”
State-versus-hospital fights have popped up throughout the U.S. over the past year. Most recently, in Colorado, a back and forth unfolded between Gov. Jared Polis and the state’s hospital association over who is ultimately responsible for high care costs. In a speech Jan. 17, the Democratic governor accused Colorado’s hospitals of overcharging patients and sitting on significant cash reserves.
“It’s time that we hold them accountable,” he said.
The Colorado Hospital Association says the data supporting those claims does not reflect the several ongoing industry challenges, among them labor shortages, regulatory burdens and inflationary pressures.
“Unfortunately, we continue to hear rhetoric against the hospitals and health systems that have worked diligently on healthcare quality, access and affordability,” CHA said in a statement to Becker’s. “Colorado’s hospitals and health systems have been working with the administration on many of these programs, including reinsurance, hospital discounted care, price transparency, out-of-network patient protections, and more.”
Some 1,500 miles eastward, another incident of hospital-community conflict grew. In January, Pennsylvania lawmakers promoted a nonpartisan report that accuses UPMC of building a monopoly in the state through consolidation over the last decade — the Pittsburgh-based system refuted the claims, saying they were based on “flawed data.”
To the south, North Carolina officials accused the state’s seven largest health systems in June of using pandemic aid to enrich themselves. Hospitals said the accusations were based on “cherry-picked data” spun in a way that does not reflect their ongoing challenges.
As state- and market-level fights against hospitals intensify and grab national attention, hospitals and health systems may find themselves less familiar in steadying public perception than their payer and pharmaceutical counterparts, who are no strangers to vocal opponents.
“With public opinion shifting a bit amid COVID, and with some anecdotal evidence that hospitals are doing some bad things, state policymakers feel that they are enjoying the political will to make these gestures,” Ge Bai, PhD, said. “It’s also a key issue for voters. Even if they don’t do anything in reality, the gesture will probably get political capital.”
Dr. Bai is a professor of accounting and health policy at Baltimore-based Johns Hopkins University. She believes a key underlying factor driving hospital critiques as of late is the reduced public confidence in medicine by way of the pandemic.
“The hospital industry has moved away from its traditional charitable mission and toward a business orientation that is undeniable,” she said. “With the [pandemic] dust settling, I think a lot of people realize the clinicians are the heroes, but hospitals are maybe not as altruistic as they once thought.”
In 2021, over 70 percent of Americans said they trusted physicians and nurses, but only 22 percent said the same about hospital executives, according to a study from the University of Chicago and The Associated Press-NORC Center for Public Affairs Research.
“It’s a tough job and a complicated business to run, and everybody in the community has an opinion about it based on anecdotal evidence,” Dr. Keckley said. “I think much of the blame too for hospitals taking a lot of hits has been boards that are not prepared to govern.”
For both Drs. Keckley and Bai, there are other major issues they each point to as contributing factors to the growing wariness around hospital operations:
“The center of gravity in healthcare has shifted from hospitals that muscled their way into scaling,” Dr. Keckley said. “The reality is that providing hospital services in non-hospital settings that are safe, effective and less costly is where the market, and insurers, are going.”
Despite the uptick in states and Americans that have gone into fault-finding mode against hospitals and those running them, operating a financially successful hospital or health system in 2023 is a monumental task, perhaps even close to impossible for many. Last year, approximately half of U.S. hospitals finished the year with a negative margin, making it “the worst financial year” for the industry since the start of the pandemic, according to Kaufman Hall’s latest “National Flash Hospital Report.”
“Hospitals aren’t going into this with a huge amount of goodwill at their backs, and I think that’s what they need to be prepared for,” Dr. Keckley said. “You can’t just go in and tell the story of ‘look at what we do for the community’ or ‘look at all the people we employ’ — that is not going to work anymore.”


Running a health system recently has proven to be a very hard job. Mounting losses in the face of higher operating expenses, softer than expected volumes, deferred capex, and strained C-suite succession planning are just a few of the immediate issues with which CEOs and boards must deal.
But frankly, none of those are the biggest strategic issue facing health systems. The biggest
strategic issue is the reorganization of the American healthcare landscape into an ambulatory care
business that emphasizes competing for covered lives at scale in lower cost and convenient settings
of care. This shift in business model has significant ramifications, if you own and operate acute care
hospitals.
Village MD and Optum are two of the organizations driving the business model shift. They are
owned by large publicly traded companies (Walgreens and UnitedHealth Group, respectively). Both
Optum and Village MD have had a string of announced major patient care acquisitions over the past
few years, none of which is in the acute care space.
The future of American healthcare will likely be dominated by large well-organized and well-run
multi-specialty physician groups with a very strong primary care component. These physician
service companies will be payer agnostic and focused on value-based care, though will still be
prepared to operate in markets where fee-for-service dominates. They will deliver highly
coordinated care in lower cost settings than hospital outpatient departments. And these companies
will be armed with tools and analytics that permit them to manage the care for populations of
patients, in order to deliver both better health outcomes and lower costs.
At the same time this is happening, we are experiencing steady growth in Medicare Advantage.
And along with it, a stream of primary care groups who operate purpose-built clinics to take full risk
on Medicare Advantage populations. These companies include ChenMed, Cano Health and Oak
Street, among others. These organizations use strong culture, training, and analytics to better
manage care, significantly reduce utilization, and produce better health outcomes and lower costs.
Public and private equity capital are pouring into the non-acute care sectors, fueling this growth. As
of the start of 2022, nearly three quarters of all physicians in the US were employed by either
corporate entities (such as private equity, insurance companies, and pharmacy companies), or
employed by health systems. And this employment trend has accelerated since the start of the
pandemic. The corporate entities, rather than health systems, are driving this increasing trend.
Corporate purchases of physician practices increased by 86% from 2019 to 2021.
What can health systems do? To succeed in the future, you must be the nexus of care for the
covered lives in your community. But that does not mean the health system must own all the
healthcare assets or employ all of the physicians. The health system can be the platform to convene these assets and services in the community. In some respects, it is similar to an Apple iPhone. They are the platform that convenes the apps. Some of those apps are developed and owned by Apple. But many more apps are developed by people outside of Apple, and the iPhone is simply the platform to provide access.
Creating this platform requires a change in mindset. And it requires capital. There are many opportunities for health systems to partner with outside capital providers, such as private equity, to position for the future – from both a capital and a mindset point of view.
The change in mindset, and the access to flexible capital, is necessary as the future becomes more and more about reorganizing into an ambulatory care business that emphasizes competing for covered lives at scale in lower cost and convenient settings of care.
