Tomorrow, America’s Physician Groups (APG) will kick-off its Annual Spring Conference “Going the Distance” in San Diego with breakout sessions focused on wide ranging operational issues and 3 general sessions that address restoring trust in the profession, lessons from the pandemic and Medicare Advantage.
Next Thursday, the American Medical Association (AMA) will kick off its 5-day House of Delegates session in Chicago with a plethora of resolutions and votes on the docket and committee reports on issues like the ethical impact of private equity on physicians in private equity owned practices, health insurer payment integrity and much more.
These meetings are coincident with the expected resolution of the debt-ceiling dispute in Congress which essentially leaves current Medicare and Medicaid payments to physicians and others in tact through 2025. So, for at least the time being, surprises in insurer payments to physicians are not anticipated.
Nonetheless, it’s a critical time for APG and AMA as their members face unparalleled market pressures:
Trust in the profession has eroded. Media attention to its bad actors has expanded.
Settings have changed: the majority now work as employees of large groups owned by hospitals or private equity sponsors.
Consumer (patient) expectations about physician quality, access and service are more exacting.
Technologies that improve precision in diagnostics and therapies and integration of social determinants in care planning have altered where, how and by whom care is delivered.
Affordability and lack of price transparency are fundamental concerns for U.S. consumers (and voters), employers and Congress. While drug PBMs, hospitals and health insurers are a focus of attention, physicians are not far behind.
Private equity and retail giants are creatine formidable competition in primary and specialty care.
Media coverage of “bad actors” engaged in fraudulent activity (i.e. unnecessary care, medications, et al) has increased.
Operating losses in hospitals remain significant limiting hospital investments in their employed medical practices.
Both organizations remain steadfast in the belief that the future for U.S. healthcare is physician centric:
For APG, it’s anchored in a core belief that changing payer incentives from fee-for-service to value is the essential means toward the system’s long-term sustainability and effectiveness. (APG represents 335 physician organizations)
For AMA, “true north” is the profession’s designated role as caregivers and stewards of the public’s health and wellbeing. (AMA’s membership includes 22% of the nation’s 1.34 million practicing physicians, medical students and residents).
But market conditions have taken their toll on physician psyche even as CMS has altered its value agenda.
Physicians are highly paid professionals. Per Sullivan Cotter and Kaufman Hall, their finances took a hit during the pandemic and their finances in 2022-2023 has been stymied by inflationary pressures. Thus, most worry about their income and they’re hyper-sensitive to critics of their compensation.
Fueling their frustration, virtually all believe insurance companies are reimbursement bullies, hospitals spend too much on executive salaries (aka suits) and administration and not enough on patient care and patients are increasingly difficult and unreasonable. Most think the profession hasn’t done enough to protect them and 65% say they’re burned out. That’s where APG and AMA find themselves relative to their members.
My take:
The backdrop for the APG and AMA meetings in the next 2 weeks could not be more daunting. Inflationary pressures dog the health economy as each advances an advocacy agenda suitable to their member’s needs.
But something is missing: a comprehensive, coherent, visionary view of the health system’s future in the next 10-20 years wherein physicians will play a key role.
That view should include…
How value and affordability are defined and actualized in policies and practice.
How the caregiver workforce is developed, composed and evaluated based on shifting demand.
How incentives should be set and funding sourced and rationalized across all settings and circumstances of service.
How consumerism can be operationalized.
How prices and costs in every sector (including physician services) can become readily accessible.
How a seamless system of health can be built.
How physician training and performance can be modernized to participate effectively in the system’s future.
The U.S. health system’s future is not a repeat of its past. Recognizing this, physicians and the professional associations like APG and AMA that serve them have an obligation to define its future state NOW.
Some physicians are on the brink of despair; others are at the starting line ready to take on the challenge.
In just 2020, deaths from gun violence cost the U.S. healthcare system $290 million, or about $6,400 per patient, according to a report from the Commonwealth Fund. These costs are mostly covered by Medicaid and other government insurance programs.
The U.S. healthcare system sees about 30,000 inpatient hospital stays and 50,000 emergency room visits due to gun violence each year, leading to more than $1 billion in initial medical costs, according to a new analysis.
The Commonwealth Fund published these results last week and relied on three data sources for its analysis: the 2019 Global Burden of Disease study, the Small Arms Survey and the U.S. Government Accountability Office.
Even after leaving the hospital, patients are faced with challenges. A year after a gun injury, medical spending rises about $2,495 per person per month. In addition, those who suffer firearm injuries are more likely to form mental health challenges and substance use disorders.
“The impact of gun violence reaches far beyond the hospital room,” the analysis states.
Firearm-related deaths are increasing, according to the Centers for Disease Control and Prevention. In 2021, almost 49,000 Americans died from firearms, compared to 45,000 in 2020.
Additional findings from the report include:
In 2019, the U.S. had a higher rate of firearm deaths than any other country. Its rate of firearm deaths was almost five times as much as France, the second-highest country.
Eight times more people in the U.S. died from firearm violence in 2019 compared to Canada, the second-highest country.
More people died from self-harm by firearm in the U.S. than any other country in 2019, more than three times higher than France and Switzerland.
More women were killed by guns in the U.S. than any other country in 2019.
In the U.S., there are 67 million more firearms than people. That difference is higher than the population of the United Kingdom, which has 66.2 million people.
In the U.S., 52% of people who are admitted to hospitals for firearm injuries are Black, 29% are White, 14% are Hispanic and 5% are another race or ethnicity. Black Americans account for 50% of firearm injury hospital costs, while White Americans account for 27%, Hispanic Americans account for 17% and other races or ethnicities account for 6%.
About 48% of firearm-related inpatient hospital stays are in the American South, while 20% are in the Midwest, 20% are in the West and 12% are in the Northeast. The South accounts for 44% of firearm injury hospital costs, while the West accounts for 26%, the Midwest accounts for 18% and the Northeast accounts for 11%.
April 1st marked the start date of a one-year window for state Medicaid offices to reassess their beneficiary rolls, as Medicaid’s continuous enrollment policy sunsets. Since the early days of the pandemic, the federal government has boosted state Medicaid funding by 6.2 percent, in exchange for a requirement that current Medicaid beneficiaries maintain eligibility, regardless of changes to their income or other qualifiers. This policy helped grow national Medicaid enrollment to a record 90M, but a projected 15M may now lose coverage through the redetermination process.
The Gist: After the US uninsured rate recently hit a record low, millions of Americans will now lose insurance coverage, at least temporarily.Of those no longer eligible for Medicaid, an estimated 2.7M will qualify for subsidized exchange plans, while around 400K in non-expansion states will have incomes too high for Medicaid and too low for exchange subsidies. The impact will vary in each state, both in terms of how quickly and how many Medicaid beneficiaries are disenrolled.
But in over half of states,at least one-fifth of those who will lose Medicaid coverage are projected to remain uninsured—a significant step backward in the effort to ensure universal coverage.
Communication from Medicaid offices and exchange plan navigators will be key to preventing as many people as possible from becoming uninsured.
At a meeting with hospital system CEOs last Wednesday, one asked: “has healthcare reached the tipping point?” I replied ‘not yet but it’s getting close.’
I iterated factors that make these times uniquely difficult in every sector:
An uncertain economy that’s unlikely to fully recover until next year.
The growth of Medicaid and Medicare coverage that shifts their financial shortfall to employers and taxpayers who are fed up and pushing back.
A vicious political environment that rewards partisan brinksmanship and focus-group tested soundbites to manipulate voters on complex issues in healthcare.
The growing domination of Big Business in each sector that have used acquisitions + corporatization to their advantage.
The widening role of private equity in funding non-conventional solutions that disrupt the status quo (and the uncertain future for many of these).
The federal courts system that’s increasingly the arbiter over access, fairness, quality and freedoms in healthcare.
The lingering impact of the pandemic.
And growing public disgust and distrust as the system’s altruism and good will is undermined by pervasive concern for profit.
Unprecedented! But events like those last week prompt hitting the pause button: not everyone pays attention to healthcare like many of us. The slaughter of 6 innocents in Nashville hit close to home: it’s about guns, mental health and life and death. The appeal of tech-giants to press the pause button on Generative AI for at least 6 months was sobering. The ravage of tornados that left thousands insecure without food, housing or hope seemed unfair. Mounting tensions with Russia and complex negotiations with China that reminded us that the U.S. competes in a global economy. And President Trump’s court appearance tomorrow will stoke doubt about our justice system at a time when it’s role in healthcare and society is expanding.
I am a healthcare guy. I am prone to see the world through the lens of the U.S. health industry and keen to understand its trends, tipping points and future. There’s plenty to watch: this week will be no exception. The punch list is familiar:
Medicaid coverage: Many will be watching the fallout of from state redetermination requirements for Medicaid coverage starting as soon as this week with disenrollment in Arizona, Arkansas, Idaho, New Hampshire and South Dakota.
Medicare Advantage: Health insurers will be modifying their Medicare Advantage strategies to adapt to CMS’ risk adjustment and Value-based Insurance Design modifications announced last week.
Prescription drug prices: PBMs and drug companies will face growing skepticism as Senate and House committees continue investigations about price gauging and collusion. Hospitals will be making adjustments to higher operating losses as states cut their Medicaid rolls.
Technology: The 7500 VIVA attendees will be doing follow-up to secure entrées for their technologies and solutions among prospective buyers.
Physicians: And physicians will intensify campaigns against insurers and hospitals now seen as adversaries while lobbying Congress for more money and greater income opportunities i.e., physician-owned hospitals.
Hospitals: On the offense against site-neutral payments, physician owned hospitals, drug prices and inadequate reimbursement from health insurers.
All will soldier on but the food fights in healthcare and broader headwinds facing the industry suggest a tipping point might be near.
I am not a fatalist: the future for healthcare is brighter than its past, but not for everyone. Strategies predicated on protecting the past are obsolete. Strategies that consider consumers incapable of active participation in the delivery and financing of their care are archaic. Strategies that depend on unbridled consolidation and opaque pricing are naïve. And strategies that limit market access for non-traditional players are artifacts of the gilded age gone by when each sector protected its own against infidels outside.
These times call for two changes in every board room and C Suite in of every organization in healthcare:
Broader vision: Understanding healthcare’s future in the broader context of American society, democracy and capitalism: Beltway insiders and academics prognosticate based on lag indicators that are decreasingly valid for forecasting. Media pundits on healthcare fail to report context and underpinnings. Management teams are operating under short-term financial incentives lacking longer-term applicability. Consultants are telling C suites what they want to hear. And boards are being mis-educated about trends of consequence that matter. Understanding the future and building response scenarios is out of sight and out of mind to insiders more comfortable being victims than creators of the new normal.
Board leadership: Equipping boards to make tough decisions: Governance in healthcare is not taken seriously unless an organization’s investors are unhappy, margins are shrinking or disgruntled employees create a stir. Few have a systematic process for looking at healthcare 10 years out and beyond their business. Every Board must refresh its thinking about what tomorrow in healthcare will be and adjust. It’s easier for board to approve plans for the near-term than invest for the long-term: that’s why outsiders today will be tomorrow’s primary incumbents.
So, is U.S healthcare near its tipping point? I don’t know for sure, but it seems clear the tipping point is nearer than at any point in its history. It’s time for fresh thinking and new players.
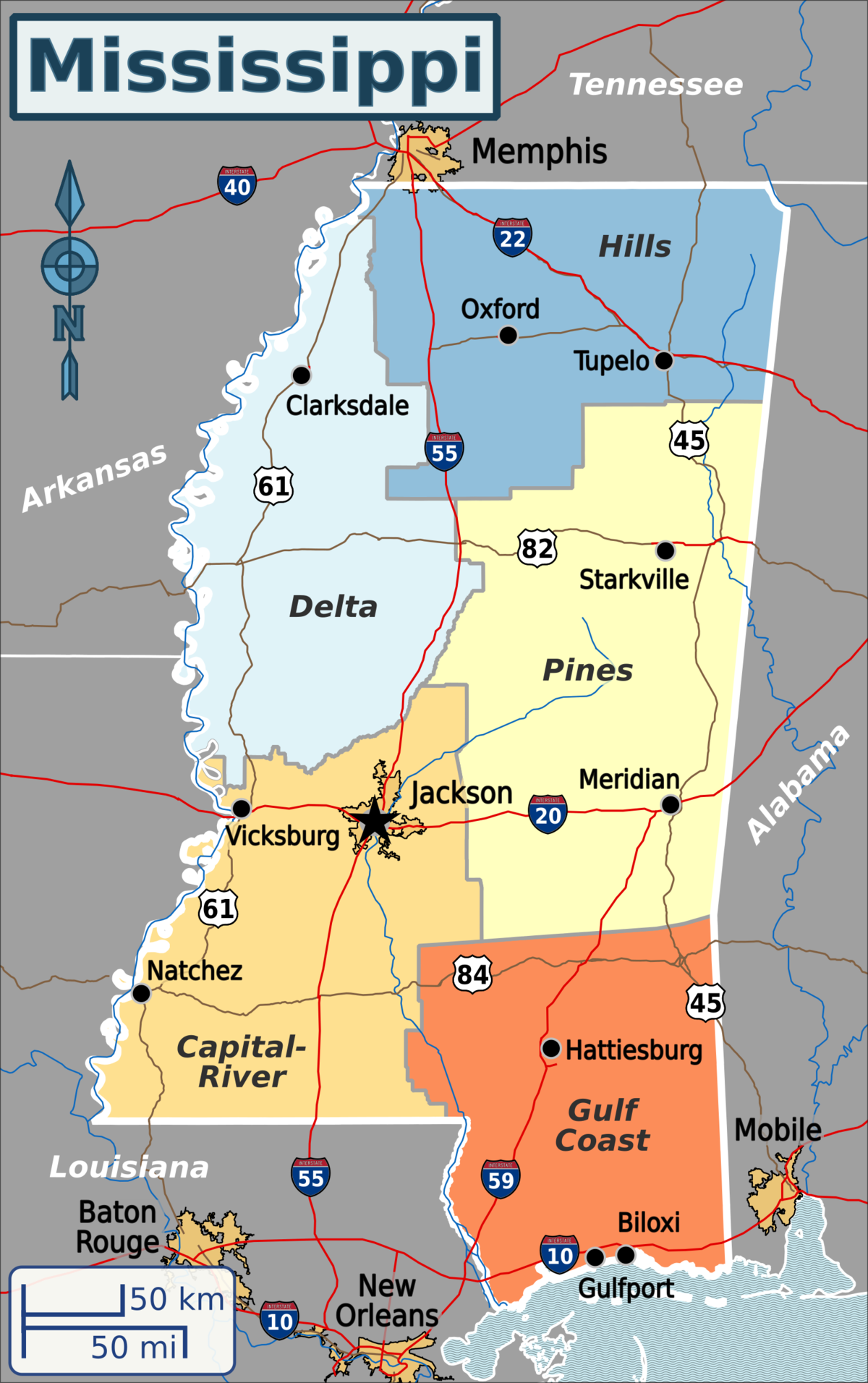
Published this week in the New York Times, this article describes the decaying state of Greenwood Leflore Hospital, a 117 year-old facility in the Mississippi Delta that may be within months of closure. While rural hospitals across the country are struggling, Mississippi’s firm opposition to Medicaid expansion has exacerbated the problem in that state, by depriving providers of an additional $1.4B per year in federal funds. Instead, only a few of the state’s 100-plus hospitals actually turn an annual profit, and uncompensated care costs are almost 10 percent of the average hospital’s operating costs.
Despite a dozen or more hospitals at imminent risk of closure, Mississippi officials would rather use the state’s $3.9B budget surplus to lower or eliminate the state income tax.
The Gist:Expanding Medicaid doesn’t just reduce rates of uncompensated care provided by hospitals, it changes the volume and type of care they provide.
Further, Medicaid expansion has been found to result in significant reductions in all-cause mortality.
Ensuring that low-income residents in Mississippi and other non-expansion states have access to Medicaid would allow providers to administer more preventive care and manage chronic diseases more effectively, before costly exacerbations require hospitalization.
Researchers estimate 15 million people will lose their Medicaid starting April 1 when states begin removing people from the low-income health insurance program for the first time in three years.
In March 2020, Congress banned states from removing people from Medicaid during the pandemic in exchange for more federal funding for state Medicaid programs. Medicaid enrollment is usually tied to people’s incomes, and individuals normally have to regularly prove they still qualify in what’s known as a redetermination. (In the 39 states and Washington, D.C., that have expanded Medicaid, a family of four has to make less than $40,000 to qualify. In non-expansion states, the cutoff is even lower.)
With redeterminations paused, Medicaid enrollment nationwide has grown from 71 million in February 2020 to an estimated 95 million in March 2023.Research shows Medicaid coverage is associated with better access to care, more financial security, better health and lower mortality. During the pandemic, beneficiaries have been able to enjoy these benefits without worrying about confirming their eligibility.
In December, Congress voted to let states restart the process of clearing their rolls on April 1, what’s sometimes referred to as “unwinding.”Lawmakers are giving states 14 months to redetermine millions of people’s eligibility — an unprecedented task made even more difficult by serious staffing and experience shortages in many Medicaid offices.
“It’s going to be a big lift,” said Sayeh Nikpay, a health policy researcher at the University of Minnesota and Tradeoffs Senior Research Advisor. “States have never had to do this many redeterminations this quickly before, and there’s a lot of uncertainty about what will happen.”
We asked Nikpay to pick out a few relevant studies to help us understand what is happening and how states and employers could keep more people insured. Here are three she identified as particularly helpful.
Two types of people will lose coverage
The Office of the Assistant Secretary for Planning and Evaluation, which provides research for the U.S. Department of Health and Human Services, released a report in August 2022 that estimated 15 million people will lose Medicaid coverage as a result of the unwinding. (The estimate is similar to another analysis by the independent Urban Institute.)
ASPE breaks those 15 million people into two groups. In the first group are people who make too much money to qualify for Medicaid. ASPE estimates there are about 8 million people in that category, and they should be able to get insurance through work or the Obamacare exchanges.
In the second group are roughly 7 million people ASPE estimates are still eligible but will lose coverage because of what’s called “administrative churn.”This can happen if the Medicaid office can’t get in touch with someone to confirm their eligibility because they’ve moved or changed their phone number or if they’re unable to make an in-person appointment because of work or child care responsibilities. (The Urban Institute projects about 4 million people will be in this group.)
These two groups represent a key tension to the unwinding process: States want to shed people who make too much money, but officials also know eligible people often lose coverage during redeterminations, and that danger is heightened given the scale and speed of this process.
Making the switch from Medicaid to private insurance
This next paper looks at the first group: the roughly 8 million people expected to move from Medicaid to private coverage, and specifically the roughly 4 million who are expected to get coverage through the Obamacare exchanges. Adrianna McIntyre, an assistant professor of health policy at Harvard, wrote in JAMA Health Forum in October 2022 about the most effective ways to move people from Medicaid onto private Obamacare plans.
There’s limited data on this, but based on the few studies available, McIntyre found that only 3 to 5 percent of people who leave Medicaid end up getting an Obamacare plan. Many policymakers are relying on the Obamacare exchanges to provide a life preserver to millions of people losing Medicaid coverage, but the research cited by McIntyre shows getting people into these plans is not guaranteed and will take focused effort by states.
McIntyre’s review cites several randomized controlled trials where states tested different ways of increasing enrollment in Obamacare plans. These studies found simple reminders from the state – like physical letters, emails and phone calls help – boost sign-ups anywhere from 7 to 16 percent.
But what really seems to make a difference is reminders plus connecting people to someone who can get them signed up while they are on the phone. In one of those trials published in 2022, people in California who got a reminder email and a call connecting them to enrollment assistance were almost 50% more likely to sign up for a plan. Such extra effort is obviously costly, and it may not be a priority or financially feasible for some states.
McIntyre’s review did not include any research on what employers can do to help their workers transition from Medicaid to work-based coverage, but based on the studies McIntyre cited, Nikpay said she thinks it’s a good idea for employers to make sure people know Medicaid could be going away and provide as much help as possible in getting new coverage.
Making it easier to stay on Medicaid can have other benefits
The final study looks at the second group of people expected to lose Medicaid coverage: the 7 million people who may lose coverage due to administrative churn even though they are still eligible.
Some states have tried to limit that churn, and researchers at the RAND Corporation evaluated New York’s effort. Starting in 2014, New York allowed people to stay on Medicaid without any redeterminations for 12 months once enrolled.
In addition to keeping more people on Medicaid for longer, researchers found that after this policy was in place, hospital admissions and monthly costs per beneficiary went down. The researchers can’t say whether the continuous enrollment policy directly caused these improved outcomes, but the findings suggest that avoiding administrative churn can help people stay covered without ballooning costs.
“It seems reasonable to me,” Nikpay said of the findings, “that making it easier to stay on Medicaid, even outside of a global pandemic, could benefit people’s health given what we know about how Medicaid affects people.”
Since its opening in a converted wood-frame mansion 117 years ago, Greenwood Leflore Hospital had become a medical hub for this part of Mississippi’s fertile but impoverished Delta, with 208 beds, an intensive-care unit, a string of walk-in clinics and a modern brick-and-glass building.
But on a recent weekday, it counted just 13 inpatients clustered in a single ward. The I.C.U. and maternity ward were closed for lack of staffing and the rest of the building was eerily silent, all signs of a hospital savaged by too many poor patients.
Greenwood Leflore lost $17 million last year alone and is down to a few million in cash reserves, said Gary Marchand, the hospital’s interim chief executive. “We’re going away,” he said. “It’s happening.”
Rural hospitals are struggling all over the nation because of population declines, soaring labor costs and a long-term shift toward outpatient care. But those problems have been magnified by a political choice in Mississippi and nine other states, all with Republican-controlled legislatures.
They have spurned the federal government’s offer to shoulder almost all the cost of expanding Medicaid coverage for the poor. And that has heaped added costs on hospitals because they cannot legally turn away patients, insured or not.
Opponents of expansion, who have prevailed in Texas, Florida and much of the Southeast, typically say they want to keep government spending in check. States are required to put up 10 percent of the cost in order for the federal government to release the other 90 percent.
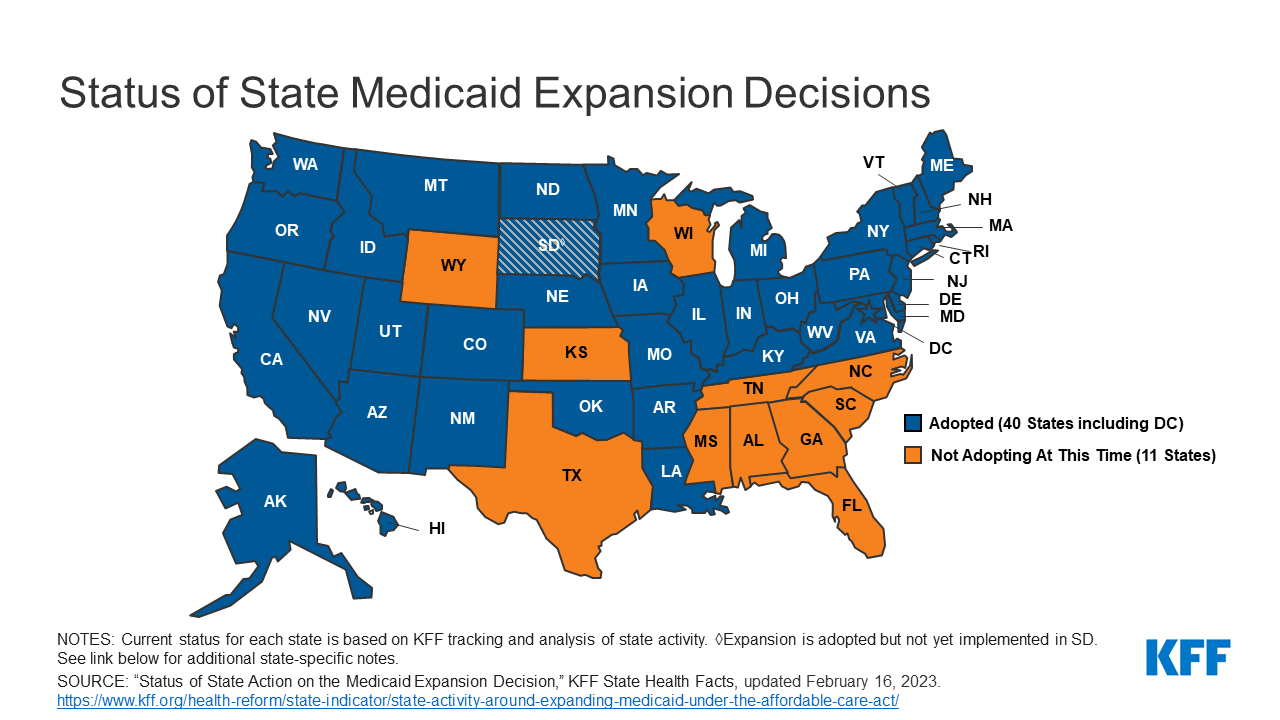
But the number of holdouts is dwindling. On Monday, North Carolina became the 40th state to expand Medicaidsince the option to cover all adults with incomes below 138 percent of the poverty line opened up in 2014 under the terms of the 2010 Affordable Care Act. The law, a major victory for President Barack Obama, has continued to defy Republican efforts to kill or limit it.
“This argument about rural hospital closures has been an incredibly compelling argument to voters,” said Kelly Hall, the executive director of the Fairness Project, a national nonprofit that has successfully pushed ballot measures to expand Medicaid in seven states.
In Mississippi, one of the nation’s poorest states, the missing federal health care dollars have helped drive what is now a full-blown hospital crisis. Statewide, experts say that no more than a few of Mississippi’s 100-plus hospitals are operating at a profit. Free care is costing them about $600 million a year, the equivalent of 8 percent to 10 percent of their operating costs — a higher share than almost anywhere else in the nation, according to the state hospital association.
Expanding Medicaid would uncork a spigot of about $1.35 billion a year in federal funds to hospitals and health care providers, according to a 2021 report by the office of the state economist.
And it would guarantee medical coverage to some 100,000 uninsured adults making less than $20,120 a year in a state whose death rates are at or near the nation’s highest for heart disease, stroke, diabetes, cancer, kidney disease and pneumonia. Infant mortality is also sky-high, and the Delta has the nation’s highest rate of foot and leg amputations because of diabetes or hypertension.
Health officials blame those numbers in part on the high rate of uninsured residents who miss out on preventive care.
“I can tell you I have a number of patients who are on dialysis with renal failure for the rest of their life because they couldn’t afford the medication for their blood pressure, and that caused their kidneys to go bad,” said Dr. John Lucas, a Greenwood Leflore surgeon.
Among Mississippi adults, only disabled people and parents with extremely low incomes, along with most pregnant women, are eligible for Medicaid. Many of the ineligible are also too poor to qualify for the tax credits for insurance under the Affordable Care Act, leaving them without affordable options.
The same is true for close to two million other Americans who live in the states that have not expanded Medicaid. Three in five are adults of color, according to a 2021 study by the Center on Budget and Policy Priorities, a nonprofit research group. In Mississippi, more than half are Black.
Gov. Tate Reeves, a Republican, and key G.O.P. state lawmakers argue that a bigger Mississippi program is not in taxpayers’ best interest. The governor says the state’s $3.9 billion surplus would be best used to help eliminate Mississippi’s income tax.
“Don’t simply cave under the pressure of Democrats and their allies in the media who are pushing for the expansion of Obamacare, welfare and socialized medicine,” Mr. Reeves said in his annual State of the State address in January.
Opponents also argue that the newly insured would become dependent on Medicaid and therefore be less likely to work. “I believe we should be working to get people off Medicaid as opposed to adding more people to it,” said Philip Gunn, the powerful Republican House speaker.
Yet in Mississippi’s Delta, a flat swath of fields of corn, soybeans and other crops nearly as big as Delaware, access to any kind of medical care is drying up for lack of money. More than 300,000 people live here, nearly 35 percent of them Black. About the same percentage live in poverty, a rate three times the national average.
Dr. Daniel P. Edney, the state’s top health officer, said he did not set Medicaid policy, and he has been careful not to take sides. But he predicted emerging health care deserts where women would have to travel long distances to deliver babies and more sick people would die because they could not gain access to care.
Of the state’s hospitals, “I have maybe heard of two that are generating any profit,” he said. When he asks hospital executives if Medicaid expansion would help their balance sheets, he said, “they say it’s a game changer.”
He predicted that five hospitals would soon downgrade into mere emergency rooms, where doctors work to stabilize patients, then transfer them to the nearest hospital.
If that happens, some of the sickest will not make it, said Dr. Jeff Moses, an emergency room physician at Greenwood Leflore.
“Where are they going? Davy Jones’s locker,” he said. “It is very dark, and I’m not exaggerating this. I just can’t imagine what will happen to this community if this hospital closes.”
Nine years after states began expanding Medicaid, evidence is growing that broader coverage saves lives. In a 2021 analysis, researchers for the National Bureau of Economic Research estimated that in one four-year period, 19,200 more adults aged 55 to 64 survived because of expanded coverage, and nearly 16,000 more would have lived if that coverage was nationwide.
Other studies suggest why: Making medical care more affordable led to increases in regular checkups, cancer screenings, diagnoses of chronic diseases and prescriptions for needed medicines.
Especially during the first six years of the Medicaid expansion, when the federal government picked up 95 to 100 percent of the cost, many states found that the program was a net fiscal gain. Some states have imposed taxes on hospitals or health care providers to cover their share of the expense, the same strategy used to help fund other Medicaid costs.
Now the federal government is offering a new incentive for the holdouts: As part of a 2021 pandemic relief measure, it agreed to temporarily pay a higher proportion of costs for some existing Medicaid patients if states broadened eligibility.
Mississippi’s office of the state economist has estimated that for at least the first decade, those savings and others would fully cover the roughly $200 million a year that Medicaid expansion would cost the state government.
Tim Moore, the president of the Mississippi Hospital Association, said expansion was “a no-brainer.” The state is so poor, he said, that for every dollar it spends on Medicaid, the federal government pumps four back in.
Polls, including by Mississippi Today and Siena College, appear to show Mississippians support Medicaid expansion, regardless of their political affiliation. Brandon Presley, the Democratic candidate for governor, is highlighting hospital closures as a reason to deny Mr. Reeves a second term in elections this November.
In a possible sign of political nervousness, the governor and the legislature recently agreed to extend Medicaid coverage to pregnant women for 12 months after they give birth, prolonging a federal pandemic-era policy.
The legislators are also trying to prop up the hospitals with a one-time infusion of $83 million or more. But that is a pittance compared with what the state has given up in Medicaid payments.
The state has lost four hospitals since 2008, according to the hospital association, and Dr. Edney, the state health officer, said that it would inevitably lose more. He said he worried most about health care access in the Delta, where he grew up, the child of working-class parents with no health insurance.
On Saturday, Representative Bennie Thompson, Democrat of Mississippi, said victims of a tornado that struck the Delta last week had to be ferried 50 miles away for medical treatment because the local hospital had no power. More Medicaid dollars, he said, would have equipped it with an emergency generator.
An hour due west from Greenwood Leflore, another major hospital, run by Delta Health System, is also in serious trouble. Licensed for more than 300 beds, the hospital one day last month held just 72 inpatients.
Thirty-two of them were kept in the emergency department, partly because of nursing cuts. One upshot is that patients seeking emergency care now wait an average of two hours, four times as long as they should, according to Amy Walker, the chief nursing officer. Some simply walk out.
The neonatal intensive care unit closed last July. Now babies in trouble must be ferried by ambulance or helicopter 125 miles south to Jackson.
Iris Stacker, the chief executive, said the hospital could remain open through the end of the year; after that, she makes no promises. She is hoping federal grants will help keep the doors open, despite the state’s failure to expand Medicaid.
But she said, “It’s very hard to ask the federal government for more money when you have this pot of money sitting here that we won’t touch.”
A top message on Greenwood Leflore’s website is now a request for donations. So far, the hospital has raised less than $12,000.
Mike Hardin, a 70-year-old retiree, was one of a handful of inpatients one recent day. He had come to the emergency room two days before with slurred speech. Doctors quickly diagnosed a stroke and now were sending him home with revised medications.
“They have to do something to keep this hospital open,” he said as he was wheeled out of his room. “The people around this area wouldn’t have any place else to go.”
The hospital’s outpatient clinics are largely still in business, and doctors there say their caseloads are full of impoverished patients who should have been treated earlier.
Dr. Abhash Thakur, a cardiologist, said he routinely saw patients in the late stages of congestive heart failure who had never seen a cardiologist or been prescribed heart medication. Some have as little as 10 percent of their heart function left.
“They are not the exception,” he said, before examining a 52-year-old man who uses a wheelchair because of his heart disease. “Every day, probably, I will see a few of them.”
Dr. Raymond Girnys, a general surgeon, had just treated a man in his late 50s. He said that a week earlier, the man had punctured his foot on a sharp stick while walking in his tennis shoes in a field.
The man did not seek medical attention until the foot became infected because he was poor and uninsured. Dr. Girnys pointed out the irony: If his patient lost his foot, he would become eligible for Medicaid because then he would be disabled.
“If they had insurance, they wouldn’t be afraid to seek care,” he said.
Experts say that no more than a few of Mississippi’s 100-plus hospitals are operating at a profit.
North Carolina is poised to become the 40th state to expand Medicaid.
Yesterday afternoon, Gov. Roy Cooper (D) signed legislation crafted by the state’s two Republican leaders, an unlikely deal that puts an end to an over-a-decade-long political battle.
But North Carolina may be the last of the Medicaid expansion holdout states to reverse course for a while. Supporters of extending the safety net coverage to hundreds of thousands more low-income adults have repeatedly run into Republican resistance in the 10 states that have long refused the Obamacare program — and another victory isn’t imminent.
“Now we’re down to some of the hardest states to get expansion through,” said Frederick Isasi, the executive director of Families USA, a left-leaning consumer health lobby, though he expressed confidence the remaining states would eventually budge.
Over the years, some steadfast GOP opposition to Medicaid expansion has softened, such as in North Carolina. The 2010 Affordable Care Act required states to extend the safety net program up to 138 percent of the federal poverty level, but the Supreme Court made doing so voluntary.
The ballot measures
Since 2017, advocates have put expanding Medicaid directly to voters in seven conservative-leaning states. They argued it would bring federal taxpayer dollars back to their state and help struggling rural hospitals — and the ballot measures passed in every instance.
But that strategy may be almost exhausted. Three of the holdout states have had citizen-led ballot measure processes — Florida, Wyoming and Mississippi — but at the moment, that path only appears viable in one state.
That’s Florida, where Medicaid advocates have their eye on fall 2026. Florida Decides Healthcare, a political committee supporting expansion, estimates it’ll cost roughly $10 million just to gather enough signatures to get the measure on the ballot, according to Jake Flaherty,the group’s campaign manager.
Even if that happens in a few years, there’s another hurdle. An amendment to the constitution must garner the support of 60 percent of voters. Only once — in Idaho — has that happened for Medicaid expansion.
The prospects are dim in the near future for the other two states. Wyoming advocates don’t believe they can use the ballot measure process to expand Medicaid, citing a mandate that an initiative not “make appropriations.” The next best chance is likely 2025, when the state legislature convenes again for a general session, according to Nate Martin, the executive director of Better Wyoming.
And in Mississippi, advocates filed paperwork to launch an expansion campaign in 2021. But it had to disband a month later when the state Supreme Court nullified the ballot measure process until state lawmakers fixed it, which the legislature failed to do this year, the Clarion Ledger reported.
Other states
North Carolina is the first state to expand Medicaid through the legislature since Virginia in 2018. And it’s still not finalized: The expansion is tied to the state passing a new budget, which is expected to occur over the summer.
Other states that haven’t expanded include Alabama, Georgia, Kansas, South Carolina, Tennessee, Texas and Wisconsin. Republicans opposing expansion have often cited fiscal concerns with the policy, which supporters push back against and have pointed to extra two-year incentives signed into law in 2021.
Several advocates said they’re watching Alabama closely, and that Gov. Kay Ivey (R) has the power to expand Medicaid without the GOP-led legislature’s sign-off. Last week, a House committee held an educational meeting on addressing the state’s coverage gap, the Alabama Reflector reported. In a statement to The Health 202, spokesperson Gina Maiola wrote that “the governor’s concern remains how the state would pay for it long-term.”
And in Kansas, Democratic Gov. Laura Kelly has been pushing the issue for years. But it’s an uphill battle to get it passed this year amid some Republican opposition, Will Lawrence,her chief of staff, acknowledged in an interview. Lawrence said he believes if a deal can be reached with the House speaker at some point, then the Senate may come along.
“We’ll continue to push those conversations,” Lawrence said. He added: “If it doesn’t happen this session, then we’ll be working over the summer and fall, like we did a few years ago, and we’ll come back with a strong push in January of next year.”
On Thursday, legislators in North Carolina’s Republican-led General Assembly passed a bill to expand Medicaid eligibility to more than 600K low-income residents. The bill is expected to be signed into law by Democratic Governor Roy Cooper, with expanded coverage beginning in 2024. The Tar Heel State is poised to become the 40th state to expand Medicaid through the Affordable Care Act, although it must still appropriate funding in upcoming budget negotiations. The North Carolina Healthcare Association, which represents the state’s health systems, helped get the deal over the line by supporting language that repeals state certificate of need (CON) review in certain instances, including ambulatory surgical centers (ASCs), behavioral health and substance treatment beds, and capital technology replacements costing below $3M.
The Gist: North Carolina legislators have been attempting to expand Medicaid since 2019. It’s notable that the state’s hospitals viewed thebenefits of broader public insurance to be worth the elimination of CON rules restricting development of ambulatory surgery centers, which will surely increase competition from new insurer- and private equity-backed facilities.
North Carolina will become the fourth state to expand Medicaid using additional incentives from the American Rescue Plan, and there’s a chance Kansas will be next, given the recent push by Democratic Governor Laura Kelly.
Prospects for Medicaid expansion in the remaining nine states seem slim at best.
About 64% of adults in a Medicaid-enrolled family in December said they did not know they may lose coverage once pandemic-era policy ends and eligibility checks resume on April 1, according to a survey from the Robert Wood Johnson Foundation.
The percentage of respondents who said they heard nothing about upcoming Medicaid renewals rose from June, when 62% said they knew nothing about the changes, the survey found.
Awareness was low across the board regardless of geographic region or a state’s Medicaid expansion status, according to the survey.
Dive Insight:
The federal government barred states from resuming Medicaid eligibility checks amid widespread job losses and other challenges during the pandemic.
Once eligibility checks resume, as many as 18 million people are expected to lose coverage, according to the Robert Wood Johnson Foundation.
About 7 million of those people are expected to gain coverage through the individual markets or employer-sponsored plans, though 8 million will not and will likely become uninsured, according to a report from Moody’s Investor Services.
Awareness levels regarding looming redetermination checks remained low and varied only slightly regionally, the report found.
Similarly, above 60% of respondents reported unawareness of Medicaid redeterminations both in Medicaid expansion states and those that haven’t expanded Medicaid, “which suggests the need for widespread outreach and education efforts,” the report said.
“Reducing information gaps about the change is a critical first step,” the report said.
In non-expansion states, people will need help learning about navigating marketplace options, while in expansion states they’ll need information on how to stay enrolled, the report said.
The suspension of eligibility checks led Medicaid membership to rise substantially during the pandemic, growing from 70.7 million members in February 2020 to 90.9 million in September, according to the Moody’s Investor Services report.
The end of the policy is expected to deal a blow to payers that have touted recent enrollment growth while hospitals could see more self-pay patients and “higher bad debt” for facilities, the Moody’s report said.