About Nurses: How much do you make?

Hundreds of nurses at University Hospitals are facing a decrease in pay as the Cleveland-based health system pivots from its COVID-19 pandemic model, cleveland.com reported.
A spokesperson told Becker’s the pay adjustment is effective June 16 and applies to 350 Enterprise Staffing Services nurses.
“UH’s Enterprise Staffing Services is an in-house staffing agency formed in response to the once-in-a-lifetime global health pandemic that stretched our resources and workforce to the extreme,” a UH statement shared with Becker’s said. “During the pandemic, hospitals across the country (including UH) increased their use of agency nurses to fill gaps in staffing with government funding assistance, with agency costing up to twice as much or more than our hospital-based full-time nurses.
“Nurses are the heartbeat of our health system and we will never be able to thank them enough for their commitment and dedication to our patients during the pandemic. Unfortunately, the pandemic care model is not sustainable in today’s environment.”
The statement said those affected by the pay adjustment, representing 1% of the health system’s workforce, will still be paid about twice the national average.
Pay for staffing services nurses on night shift will decrease from $75 to $65 an hour, a 13% cut, UH said, according to cleveland.com, which obtained a health system memo related to the change. Pay for staffing services nurses on day shift will decrease 8%, from $60 to $55 an hour.
Pay for a new staffing services job without benefits will be $75 per hour for night shift, and $65 per hour for day shift, UH said in the memo, which also encouraged staffing services nurses to apply for other health system roles, according to cleveland.com.
“As we continue to exit from our pandemic model, external nursing staffing agencies and internal hospital nurse staffing agencies nationwide are adjusting pay accordingly,”
UH’s statement said. “We have provided cutting-edge, compassionate care to our neighbors in Northeast Ohio since 1866. We’re taking the appropriate steps to ensure we can continue fulfilling our mission for future generations.”

The lawsuit filed in federal court seeks to represent thousands of other UPMC employees.
UPMC has grown steadily over the past few decades into the largest private employer in Pennsylvania, employing 95,000 workers overall.
From 1996 to 2018, the system acquired 28 competing healthcare providers, greatly expanding its market power, according to the lawsuit. The acquisitions also shrunk the availability of healthcare services. Over the same period, UPMC closed four hospitals and downsized operations in three other facilities, eliminating 1,800 full- and part-time jobs, the lawsuit said.
UPMC relied on “draconian” mobility restrictions and labor law violations to lock employees into lower pay and subcompetitive working conditions, according to the 44-page complaint.
Specifically, the system enacted restraints like noncompete clauses and “do-not-rehire blacklists” to stop workers from leaving. Meanwhile, UPMC allegedly suppressed workers’ labor law rights to prevent them from unionizing.
“Each of these restraints alone is anticompetitive, but combined, their effects are magnified. UPMC wielded these restraints together as a systemic strategy to suppress worker bargaining power and wages,” the lawsuit said. “As a result, UPMC’s skilled healthcare workers were required to do more while earning less — while they were also subjected to increasingly unfair and coercive workplace conditions.”
According to the complaint, UPMC has faced 133 unfair labor practice charges since 2012, and 159 separate allegations. Roughly 74% of the violations were related to workers’ efforts to unionize, the lawsuit said.
Meanwhile, UPMC workers’ wages have fallen at a rate of 30 to 57 cents per hour on average compared to other hospital workers for every 10% increase in UPMC’s market share, said the lawsuit, citing a consultant’s economic analysis.
The lawsuit also noted that UPMC’s staffing ratios have been decreasing, even as staffing ratios on average have increased at other Pennsylvania hospitals.
The alleged labor abuses and UPMC’s market power are linked, according to the complaint.
“Had UPMC been subject to competitive market forces, it would have had to raise wages to attract more workers and provide higher staffing levels in order to avoid degrading the care it provided to its patients, and in order to prevent losing patients to competitors who could provide better quality care,” the lawsuit said.
UPMC is facing similar labor allegations. In May, two unions filed a complaint asking the Department of Justice to investigate labor abuses at the nonprofit.
Hospitals were plagued by staffing shortages during the COVID-19 pandemic. Many facilities still bemoan the difficulty of hiring and retaining full-time workers, and point to shortages (of nurses in particular) as the reason for overworked employees and poor staffing ratios.
Yet some studies suggest that’s not the case. One recent analysis of Bureau of Labor Statistics data found employment in hospitals — including registered nurses — is now slightly higher than it was at the start of the pandemic.
Despite the controversy, UPMC — which now operates 40 hospitals with annual revenue of $26 billion — continues to try and expand its market share. Late last year, the system signed a definitive agreement to acquire Washington Health Care Services, a Pennsylvania system with more than 2,000 employees and two hospitals. The deal faces pushback from local unions.

A Los Angeles jury awarded $41.49 million to a former nurse who said Kaiser Permanente’s hospitals and health plan retaliated against and eventually terminated her for raising issues with patient safety and care quality, MyNewsLA reported Dec. 12.
The former nurse, Maria Gatchalian, was awarded $11.49 million in compensatory damages, including $9 million for emotional distress, and $30 million in punitive damages.
“We stand by her termination and are surprised and disappointed in the verdict,” Murtaza Sanwari, senior vice president and area manager for Kaiser Permanente Woodland Hills/West Ventura County, told Becker’s in a statement. “Kaiser Permanente plans to appeal this decision and will maintain our high standards in protecting the health and safety of all our patients.”
Before her termination in 2019, Ms. Gatchalian had worked at the Kaiser Permanente Woodland Hills Medical Center since 1989, first as a registered nurse in the neonatal intensive care unit and later as a charge nurse in that unit.
According to MyNewsLA, Ms. Gatchalian said she had repeatedly raised concerns with Kaiser management about patient safety and care quality related to alleged understaffing and was discouraged from submitting formal complaints. Oakland, Calif.-based Kaiser argued in court that Ms. Gatchalian admitted she had placed her bare feet on equipment in the NICU, and the organization made the decision to terminate her following her conduct.
“We work hard to make Kaiser Permanente a great place to work and a great place to receive care,” Mr. Sanwari said. “The allegations in this lawsuit are at odds with the facts we showed in the courtroom.”
“To be clear, this charge nurse’s job was to be a leader for other nurses, ensure the standards of care were followed and to protect the neonatal babies entrusted to our care. She was terminated in 2019 following an incident where she was found sitting in a recliner in the neonatal intensive care unit, on her personal phone and resting her bare feet on an isolette with a neonatal infant inside. Neonatal intensive care units are critical care units designed for critically ill babies most often born prematurely and very susceptible to infections.
The isolette, where this nurse placed her bare feet, is a protective environment designed to shield the infant from infection causing germs. Placing her bare feet on the isolette may have created risk to the infant which could have been life threatening. Her actions were egregious and in violation of our infection control policies and standards.”
https://mailchi.mp/27e58978fc54/the-weekly-gist-august-11-2023?e=d1e747d2d8
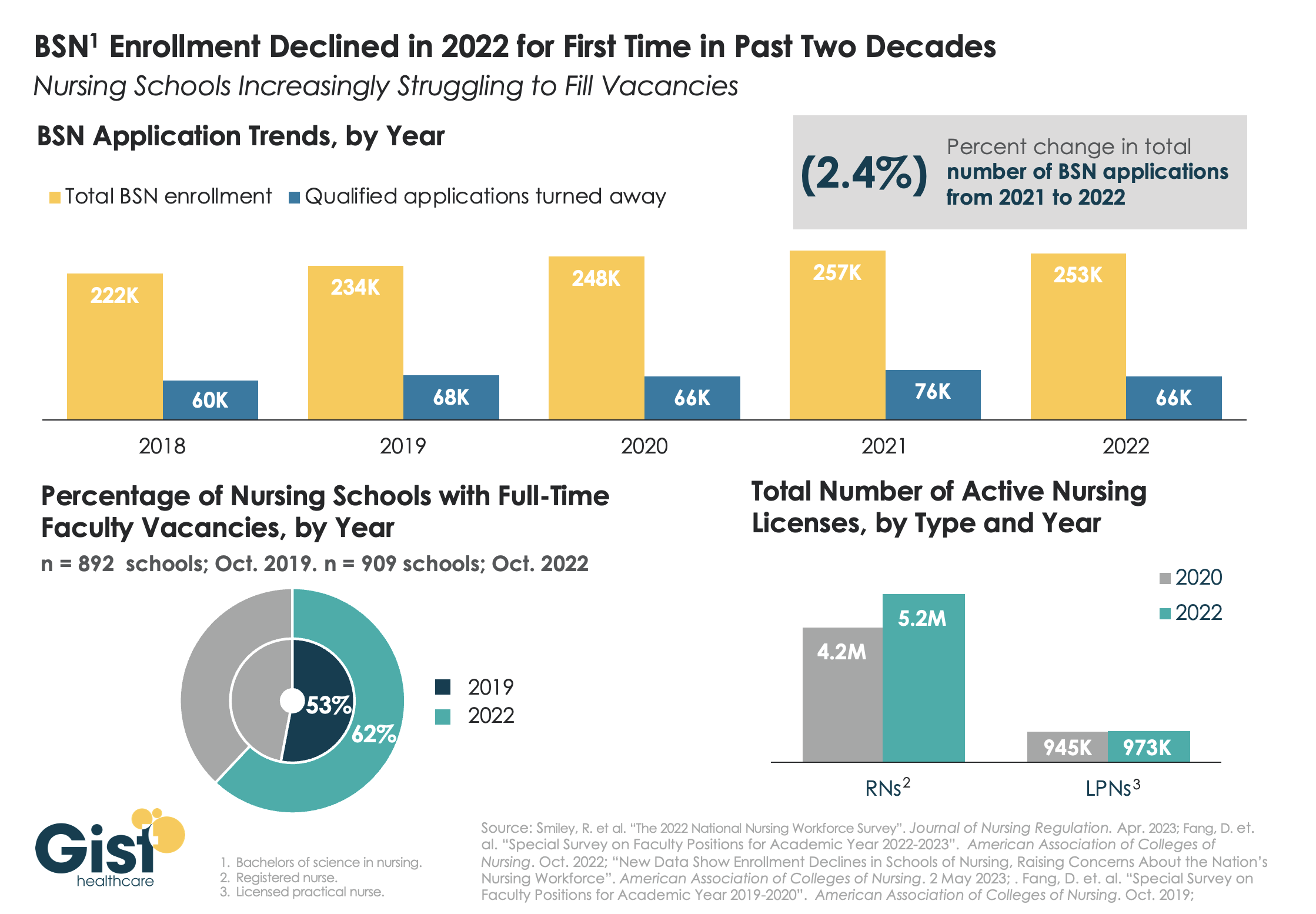
While last week’s graphic looked at how a wave of retirements has hit the nursing workforce, this week we take a look at the pipeline of nurses in training to fill that gap. In recent years, there has been a consistent stream of qualified applicants who want to become BSN nurses, but schools don’t have the capacity to admit them.
One reason: an ongoing shortage of nursing faculty, which recent retirements have exacerbated. The percentage of nursing schools with at least one full-time faculty vacancy grew from 53 percent in 2019 to 62 percent in 2022.
Looking at registered nurses (RNs), the number with active licenses has continued to grow at a much higher rate than the supply of licensed practice nurses (LPNs) with active licenses.
The relatively small LPN workforce is especially significant, given rising interest in team-based nursing care, which aims to utilize a higher number of LPNs, supervised by RNs and BSNs.
Expanding training programs with an eye toward the skills and mix needed to deliver team-based care will be critical to ensuring a stable, efficient nursing workforce for future decades.
https://mailchi.mp/8f3f698b8612/the-weekly-gist-january-27-2023?e=d1e747d2d8

As hospitals and health system leaders continue to grapple with persistently high nursing vacancy rates and severe staffing challenges, and face growing pressure to cut costs, we’re beginning to hear serious—if paradoxical—consideration being given to sharpening the axe, with an eye on a long-standing sacred cow: “Magnet” status.
For years, leading systems have invested significant time and resources to earn Magnet status, a designation of nursing quality granted by the American Nursing Association through its American Nurses’ Credentialing Center. Applying for—and then renewing—the designation can cost millions of dollars and involve significant process changes and staff time. In return, participants can market themselves as “Magnet hospitals”, presumably garnering additional patient business and giving them a leg up in recruiting high-quality nurses. At a time of severe nursing shortage, you might expect interest in earning or maintaining Magnet status to be spiking.
But that’s not what we’re hearing. “It’s just too expensive,” shared one system CEO recently. “We haven’t really seen it move the needle on volume, and our Magnet-designated facilities are just as stretched as the non-Magnet ones, with equally low morale.” Plus, at a time when the ability to pursue flexible staffing models is at a premium, keeping up with Magnet standards is increasingly handcuffing some hospitals looking to evaluate alternative staffing solutions.
“We can achieve all of the benefits of Magnet without having to jump through their hoops on process and data collection,” a system chief nursing officer told us. “We’re working on our own, internally-branded alternative to Magnet—something our own staff comes up with, rather than something artificially imposed from an outside organization.”
Ironically, this may be another area—like the battle against contract labor—in which systems now find themselves aligned with nursing unions, which have long opposed the Magnet program as just a marketing gimmick. There’s no question that programs like Magnet have helped increase the visibility of nursing as a driver of quality care. But given the current economic environment, it’ll be interesting to see how much hospitals are willing to continue to invest to maintain the designation.

Radio Advisory’s Rachel Woods sat down with Optum EVP Dr. Jim Bonnette to discuss the sustainability of modern-day hospitals and why scaling down might be the best strategy for a stable future.
Read a lightly edited excerpt from the interview below and download the episode for the full conversation.https://player.fireside.fm/v2/HO0EUJAe+Rv1LmkWo?theme=dark
Rachel Woods: When I talk about hospitals of the future, I think it’s very easy for folks to think about something that feels very futuristic, the Jetsons, Star Trek, pick your example here. But you have a very different take when it comes to the hospital, the future, and it’s one that’s perhaps a lot more streamlined than even the hospitals that we have today. Why is that your take?
Jim Bonnette: My concern about hospital future is that when people think about the technology side of it, they forget that there’s no technology that I can name that has lowered health care costs that’s been implemented in a hospital. Everything I can think of has increased costs and I don’t think that’s sustainable for the future.
And so looking at how hospitals have to function, I think the things that hospitals do that should no longer be in the hospital need to move out and they need to move out now. I think that there are a large number of procedures that could safely and easily be done in a lower cost setting, in an ASC for example, that is still done in hospitals because we still pay for them that way. I’m not sure that’s going to continue.
Woods: And to be honest, we’ve talked about that shift, I think about the outpatient shift. We’ve been talking about that for several years but you just said the change needs to happen now. Why is the impetus for this change very different today than maybe it was two, three, four, five years ago? Why is this change going to be frankly forced upon hospitals in the very near future, if not already?
Bonnette: Part of the explanation is regarding the issues that have been pushed regarding price transparency. So if employers can see the difference between the charges for an ASC and an HOPD department, which are often quite dramatic, they’re going to be looking to say to their brokers, “Well, what’s the network that involves ASCs and not hospitals?” And that data hasn’t been so easily available in the past, and I think economic times are different now.
We’re not in a hyper growth phase, we’re not where the economy’s performing super at the moment and if interest rates keep going up, things are going to slow down more. So I think employers are going to become more sensitized to prices that they haven’t been in the past. Regardless of the requirements under the Consolidated Appropriations Act, which require employers to know the costs, which they didn’t have to know before. They’re just going to more sensitive to price.
Woods: I completely agree with you by the way, that employers are a key catalyst here and we’ve certainly seen a few very active employers and some that are very passive and I too am interested to see what role they play or do they all take much more of an active role.
And I think some people would be surprised that it’s not necessarily consumers themselves that are the big catalyst for change on where they’re going to get care, how they want to receive care. It’s the employers that are going to be making those decisions as purchasers themselves.
Bonnette: I agree and they’re the ultimate payers. For most commercial insurance employers are the ultimate payers, not the insurance companies. And it’s a cost of care share for patients, but the majority of the money comes from the employers. So it’s basically cutting into their profits.
Woods: We are on the same page, but I’m going to be honest, I’m not sure that all of our listeners are right. We’re talking about why these changes could happen soon, but when I have conversations with folks, they still think about a future of a more consolidated hospital, a more outpatient focused practice is something that is coming but is still far enough in the future that there’s some time to prepare for.
I guess my question is what do you say to that pushback? And are there any inflection points that you’re watching for that would really need to hit for this kind of change to hit all hospitals, to be something that we see across the industry?
Bonnette: So when I look at hospitals in general, I don’t see them as much different than they were 20 years ago. We have talked about this movement for a long time, but hospitals are dragging their feet and realistically it’s because they still get paid the same way until we start thinking about how we pay differently or refuse to pay for certain kinds of things in a hospital setting, the inertia is such that they’re going to keep doing it.
Again, I think the push from employers and most likely the brokers are going to force this change sooner rather than later, but that’s still probably between three and five years because there’s so much inertia in health care.
On the other hand, we are hitting sort of an unsustainable phase of cost. The other thing that people don’t talk about very much that I think is important is there’s only so many dollars that are going to health care.
And if you look at the last 10 years, the growth in pharmaceutical spend has to eat into the dollars available for everybody else. So a pharmaceutical spend is growing much faster than anything else, the dollars are going to come out of somebody’s hide and then next logical target is the hospital.
Woods: And we talked last week about how slim hospital margins are, how many of them are actually negative. And what we didn’t mention that is top of mind for me after we just come out of this election is that there’s actually not a lot of appetite for the government to step in and shore up hospitals.
There’s a lot of feeling that they’ve done their due diligence, they stepped in when they needed to at the beginning of the Covid crisis and they shouldn’t need to again. That kind of savior is probably not their outside of very specific circumstances.
Bonnette: I agree. I think it’s highly unlikely that the government is going to step in to rescue hospitals. And part of that comes from the perception about pricing, which I’m sure Congress gets lots of complaints about the prices from hospitals.
And in addition, you’ll notice that the for-profit hospitals don’t have negative margins. They may not be quite as good as they were before, but they’re not negative, which tells me there’s an operational inefficiency in the not for-profit hospitals that doesn’t exist in the for-profits.
Woods: This is where I wanted to go next. So let’s say that a hospital, a health system decides the new path forward is to become smaller, to become cheaper, to become more streamlined, and to decide what specifically needs to happen in the hospital versus elsewhere in our organization.
Maybe I know where you’re going next, but do you have an example of an organization who has had this success already that we can learn from?
Bonnette: Not in the not-for-profit section, no. In the for-profits, yes, because they have already started moving into ambulatory surgery centers. So Tenet has a huge practice of ambulatory surgery centers. It generates high margins.
So, I used to run ambulatory surgery centers in a for-profit system. And so think about ASCs get paid half as much as a hospital for a procedure, and my margin on that business in those ASCs was 40% to 50%. Whereas in the hospital the margin was about 7% and so even though the total dollars were less, my margin was higher because it’s so much more efficient. And the for-profits already recognize this.
Woods: And I’m guessing you’re going to tell me you want to see not-for-profit hospitals make these moves too? Or is there a different move that they should be making?
Bonnette: No, I think they have to. I think there are things beyond just ASCs though, for example, medical patients who can be treated at home should not be in the hospital. Most not-for-profits lose money on every medical admission.
Now, when I worked for a for-profit, I didn’t lose money on every Medicare patient that was a medical patient. We had a 7% margin so it’s doable. Again, it’s efficiency of care delivery and it’s attention to detail, which sometimes in a not-for-profit friends, that just doesn’t happen.

https://mailchi.mp/cfd0577540a3/the-weekly-gist-november-11-2022?e=d1e747d2d8
There’s an old trope among human resources leaders that people don’t quit companies, they quit managers. There’s certainly truth to it. If an employee has a difficult or inattentive boss, they are at much greater risk of leaving for another opportunity. But a “bad” manager is not always someone lacking in the skills necessary to engage employees; sometimes the problem is that their own roles are structured in ways that make it nearly impossible to succeed.
We’ve recently heard stories from leaders at several health systems describing the untenable management scope for many of their mid-level nursing leaders. It’s common to hear that nurse managers have dozens of direct reports, and a few systems reported that some of their managers have well over a hundred individuals reporting to them. With that scope, it’s impossible to develop relationships with everyone on the team, much less be able to customize roles, or provide tailored feedback and support.
For younger workers, the manager relationship is critical for engagement, skill development, and building loyalty.
Given today’s intense margin pressures, it’s tempting to cut clinical managers and increase the span of control for those who remain—but underinvestment here is short-sighted, and will surely exacerbate challenges maintaining critical capacity in the near-term, as well as building the foundation for future growth.