One welcome side effect of the current economic challenges health systems face has been the return to prominence of the chief nursing officer (CNO) as a pivotal driver of system strategy.
So many of a hospital’s important operating and margin pressures intersect with the CNO’s domain: staffing shortages, nurse recruiting and retention, workplace violence, rising union activity, care model redesign, adoption of new care technologies (including AI), the shift of the clinical workforce into non-hospital settings, and on and on.
Never has the role of the CNO been more important to ensuring systems’ continued ability to deliver high-quality, cost-effective care in a sustainable way.
Even more heartening, we’ve been part of a number of system board retreats and strategy discussions over the past several months at which the CNO has been an important voice in the room.
We’d argue that, given how important these issues will be over the coming years, it may be time to give CNOs a permanent role in health system governance, just as boards often include physician members.
One additional agenda item that will be critical for systems to address, given the demographics of nursing executives:
what’s being done to cultivate the next generation of strong nursing leadership to fill the CNO role? A topic worth keeping an eye on.
Nurses who work for staffing agencies are much more satisfied than their counterparts who serve hospitals, health systems, home healthcare providers and senior living facilities, according to an Oct. 18 report from MIT Sloan Management Review.
Researchers identified 200 of the largest healthcare employers in the U.S., and calculated how highly nurses rate the organization and senior leadership on Glassdoor from the beginning of COVID-19 through June 2023 (view their ranking here).
The five highest-ranked employers in the sample were staffing agencies, according to the report — and higher compensation only accounts for part of nurses’ satisfaction. Researchers analyzed the free text on Glassdoor to determine how positively nurses spoke about 200 topics, and found that nurses spoke more highly of staffing agencies on issues other than pay.
Overall, 75% of nurses’ comments about staffing agencies were positive, compared with 23% of nurses’ comments about health systems.
Staffing agencies have other healthcare employers beat in problem resolution, the researchers found. Seventy-three percent of nurses said staffing agencies resolved problems efficiently, compared to 31% of nurses employed by hospitals and health systems. The difference was even greater when it came to resolving problems effectively — 55% of nurses say staffing agencies do this, compared to 9% of nurses at hospitals and health systems.
Nurses also rated staffing agencies more highly on several measures related to honesty, according to the report. Three-quarters of nurses employed by staffing agencies spoke highly of their organizations’ speed in replying to inquiries; less than one-quarter of nurses employed by hospitals and health systems praised their organization on timely replies. Staffing agencies scored 41 percentage points higher on transparency, 36 points higher on trust and 46 points higher on honesty than their hospital and health system counterparts.
Although nurses employed by staffing agencies also ranked their compensation and work-related stress levels significantly better than nurses employed by hospitals and health systems, the latter took the lead in some metrics. Nurses prefer hospitals and health systems for health and retirement benefits, learning and development opportunities, and connection with colleagues: all “important aspects of organizational life,” according to the report.
“Healthcare systems can learn from staffing agencies, but they can also leverage their own distinctive advantages to attract and retain nurses,” the report says. “Healthcare systems should invest in their comparative advantages and emphasize them when communicating their value proposition to potential and current employees.”
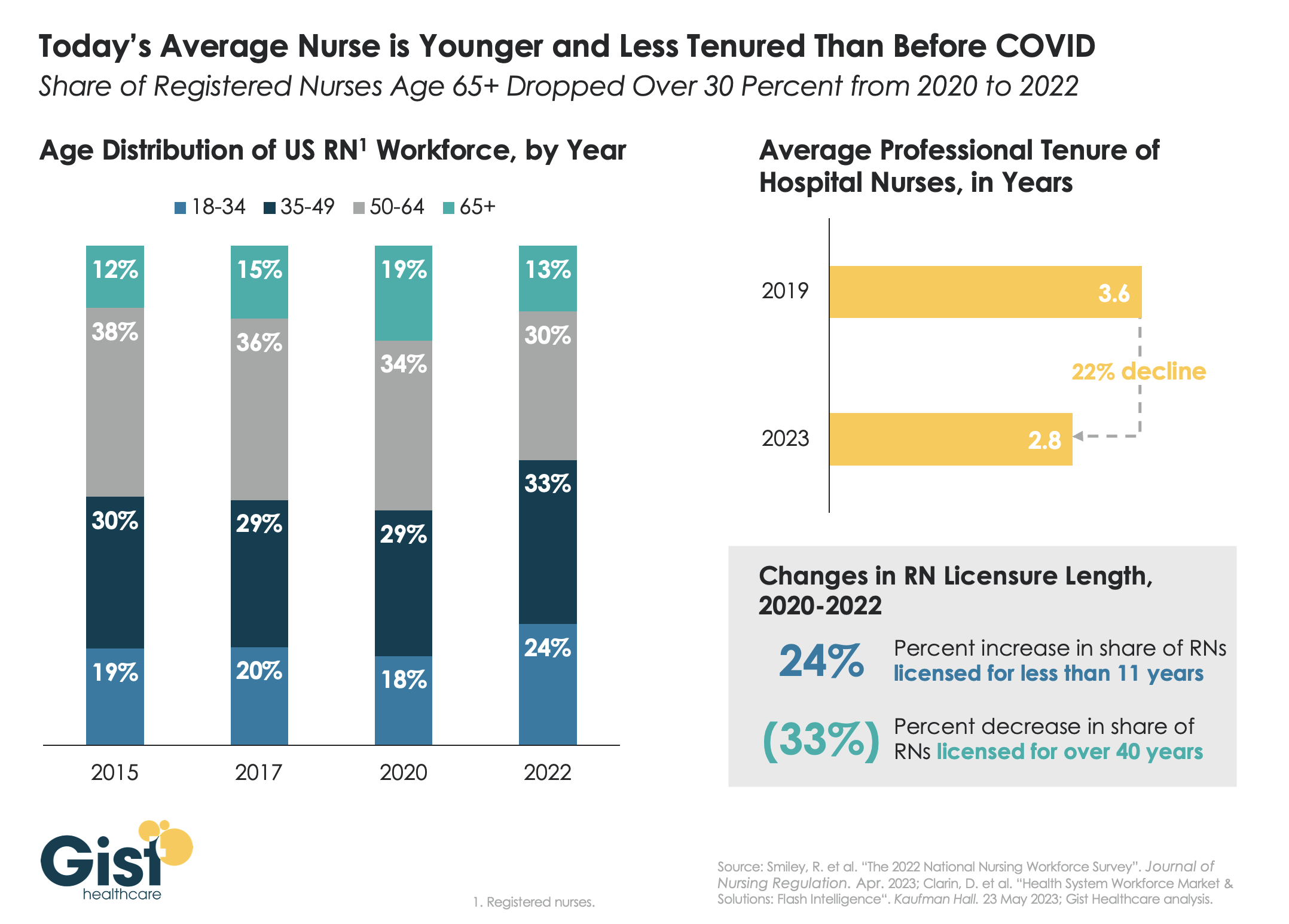
Last week we discussed how hospitals are still struggling to retain talent. This week’s graphic offers one explanation for this trend:
a significant share of older nurses, who continued to work during the height of the pandemic, have now exited the workforce, and health systems are even more reliant on younger nurses.
Between 2020 and 2022, the number of nurses ages 65 and older decreased by 200K, resulting in a reduction of that age cohort from 19 percent to 13 percent of the total nursing workforce. While the total number of nurses in the workforce still increased, the younger nurses filling these roles are both earlier in their nursing careers (thus less experienced), and more likely to change jobs.
Case in point:
From 2019 to 2023, the average tenure of a hospital nurse dropped by 22 percent. The wave of Baby Boomer nurse retirements has also resulted in a 33 percent decrease from 2020 to 2022 in the number of registered nurses who have been licensed for over 40 years.
Given these shifts, hospitals must adjust their current recruitment, retention, training, and mentorship initiatives to match the needs of younger, early-career nurses.
Of all the pandemic’s impacts still felt today, disruptions to the healthcare workforce and rising labor costs may be most impactful to current health system operations.
Over the next three editions of the Weekly Gist, we’ll be exploring the lingering effects of this workforce crisis, with a focus on nurse staffing and recruitment.
While wage increases helped reduce hospital registered nurse (RN) turnover rates from 27 percent in 2021 to 23 percent in 2022, nurses—along with hospital employees in general—are still changing jobs at higher rates than before the pandemic.
Over half of all hospitals still face nurse vacancy rates above 15 percent, a slight improvement from 2022 but still far more than before the pandemic.
While the worst of nursing turnover appears to have passed, the “rebasing” of wages (for nursing, 27 percent higher compared to 2019) will provide ongoing pressure to strained hospital margins.
The Great Nursing Resignation, and hospitals’ growing reliance on expensive agency labor (a.k.a. “travelers”) has grabbed headlines, for good reason. But lately we’ve heard a couple of anecdotes from health system leaders about the second-order impacts of the phenomenon that are worth considering as well.
First, as the ranks of agency nurses at hospitals have swelled, full-time employed nurses’ morale has plummeted—tenured nurses are having to orient their new temporary co-workers, then watch them earn up to three times as much money for the same work.
At the same time, willingness to work overtime among employed nurses has dropped. That’s not just because of burnout—it turns out that the nurses who were most likely to take overtime shifts are also more likely to have chosen to leave full-time employment to become travelers, where they are even more richly rewarded for working extra shifts. So, the “productivity” of the remaining corps of staff nurses has dropped, even as caseloads have increased.
One other implication we’ve heard about recently: the economic impact of “observation” cases, where patients are held in a staffed bed but not admitted—already a bad bargain for hospitals—has gotten worse. That’s because the cost of deploying staff to care for those patients has gone up, due to wage inflation and use of travelers. It’s hard to overstate the level of staffing crisis at most hospitals today, and the rapid growth in reliance on temporary staff will have consequences lasting well beyond the current surge.
The American Hospital Association, the American Medical Association and the American Nurses Association teamed up to release a new “Forever Grateful” TV and digital ad campaign on Monday to thank health care workers.
Why it matters: The campaign comes in the face of record levels of reported health care worker burnout tied, in part, to the prolonged emergency response to COVID-19.
The AHA also released a new video thanking health care professionals working in America’s hospitals and health systems for their work.
The hourly mean wage for registered nurses in the U.S. is $38.47, according to the U.S. Bureau of Labor Statistics’ latest occupational employment and wage statistics survey.
Among 10 metropolitan areas with the highest employment level in registered nurses, registered nurses have the highest hourly mean wage in the Los Angeles area and the lowest in the Miami area.
Ten hourly mean wages for RNs by metropolitan area, in descending order:
Dr. Christine Choi, 32, a medical resident at Harbor-UCLA Medical Center in Torrance, prepares to enter an isolation area for COVID-19 inpatients. Health care providers must face daily patient death and suffering.
Soon after the COVID-19 pandemic began last spring, Christine Choi, DO, a second-year medical resident at Harbor-UCLA Medical Center, volunteered to enter COVID-19 patient rooms. Since then, she has worked countless nights in the intensive care unit in full protective gear, often tasked with giving the sickest patients and their families the grim choice between intubation or near-certain death.
“I’m offering this guy two terrible options, and that’s how I feel about work: I can’t fix this for you and it sucks, and I’m sorry that the choices I’m giving you are both terrible,” Choi told the Los Angeles Times’ Soumya Karlamangla about one patient encounter.
While Choi exhibits an “almost startlingly positive attitude” in her work, it’s no match for the psychological burdens placed on her shoulders by the global pandemic, Karlamangla wrote. When an older female COVID-19 patient died in the hospital recently, her husband — in the same hospital with the same diagnosis — soon began struggling to breathe. Sensing that he had little time left, Choi held a mobile phone at his bedside so that each of his children could come on screen to tell him they loved him. “I was just bawling in my [personal protective equipment],” Choi said. “The sound of the family members crying — I probably will never forget that,” she said.
It was not the first time the young doctor helped family members say goodbye to a loved one, and it would not be the last. Health care providers like Choi have had to work through unimaginable tragedies and unprecedented circumstances because of COVID-19, with little time to dedicate to their own mental health or well-being.
It has been nearly a year since the US reported what was believed at the time to be its first coronavirus death in Washington State. Since then, the pandemic death toll has mushroomed to nearly 500,000 nationwide, including 49,000 Californians. These numbers are shocking, and yet they do not capture the immeasurable emotional weight that falls on the health care providers with the most intimate view of COVID-19’s deadly progression.“The horror of the pandemic has unfolded largely outside public view and inside hospitals, piling a disproportionate share of the trauma on the people whose work takes them inside their walls,” Karlamangla wrote.
Experts are deeply concerned about the psychological and physical burdens that providers must bear, and the fact that there is still no end in sight. “At least with a natural disaster, it happens, people get scattered all over the place, property gets damaged or flooded, but then we begin to rebuild,” Lawrence Palinkas, PhD, MA, a medical anthropologist at USC, told Karlamangla. “We’re not there yet, and we don’t know when that will actually occur.”
Sixty-eight percent of providers said they feel emotionally drained from their work, 59% feel burned out, 57% feel overworked, and 50% feel frustrated. The poll asked providers who say they feel burned out what contributes most to that viewpoint. One doctor from the Central Valley wrote:
“Short staffed due to people out with COVID. I’m seeing three times as many patients, with no time to chart or catch up. Little appreciation or contact from my bosses. I have never had an N95 [mask]. The emotional toll this pandemic is taking. Being sick myself and spreading it to my wife and young kids. Still not fully recovered but needing to be at work due to physician shortages. Lack of professional growth, and a sense of lack of appreciation at work and feeling overworked. The sadness of the COVID-related deaths and the stories that go along with the disease. That’s a lot of stuff to unpack.”
The pandemic has been especially challenging for female health providers, who compose 77% of health care workers with direct patient contact. “The pandemic exacerbated gender inequities in formal and informal work, and in the distribution of home responsibilities, and increased the risk of unemployment and domestic violence,” an international group of experts wrote in the Lancet. “While trying to fulfill their professional responsibilities, women had to meet their families’ needs, including childcare, home schooling, care for older people, and home care.”
For one female doctor from the Bay Area who responded to the CHCF survey, the extra burdens of the pandemic have been unrelenting: “Having to work more, lack of safe, affordable, available childcare while I’m working. As a single mother, working 15 hours straight, then having to care for my daughter when I get home. Just exhausted with no days off. So many Zoom meetings all day long. Miss my family and friends.”
It is unclear how the pandemic will affect the health care workforce in the long term. For now, the damage “can be measured in part by a surge of early retirements and the desperation of community hospitals struggling to hire enough workers to keep their emergency rooms running,” Andrew Jacobs reported in the New York Times.
One of the early retirements Jacobs cited was Sheetal Khedkar Rao, MD, a 42-year-old internist in suburban Chicago. Last October, she decided to stop practicing medicineafter “the emotional burden and moral injury became too much to bear,” she said. Two of the main factors driving her decision were a 30% pay cut to compensate for the decline in revenue from primary care visits and the need to spend more time at home after her two preteen children switched to remote learning.
“Everyone says doctors are heroes and they put us on a pedestal, but we also have kids and aging parents to worry about,” Rao said.
Working Through Unremitting Sickness and Death
In addition to the psychological burden, health care providers must cope with a harsh physical toll. People of color account for most COVID-19 cases and deaths among health care workers, according to a KFF issue brief. Some studies show that health care workers of color “are more likely to report reuse of or inadequate access to [personal protective equipment] and to work in clinical settings with greater exposure to patients with COVID-19.”
“Lost on the Frontline,” a collaboration of Kaiser Health News and the Guardian, has counted more than 3,400 deaths among US health care workers from COVID-19. Eighty-six percent of the workers who died were under age 60, and nurses accounted for roughly one-third of the deaths.
“Lost on the Frontline” provides the most comprehensive picture available of health care worker deaths, because the US still lacks a uniform system to collect COVID-19 morbidity and mortality data among health care workers. A year into the project, the federal government has decided to take action. Officials at the US Department of Health and Human Services cited the project when asking the National Academies of Sciences, Engineering, and Medicine for a rapid expert consultation to understand the causes of deaths among health care workers during the pandemic.
The National Academies’ report, published December 10, recommends the “adoption and use of a uniform national framework for collecting, recording, and reporting mortality and morbidity data” along with the development of national reporting standards for a core set of morbidity impacts, including mental well-being and psychological effects related to working through public health crises. Some health care experts said the data gathering could be modeled on the federal government’s World Trade Center Health Program, which provides no-cost medical monitoring and treatment for workers who responded to the 9/11 terrorist attacks 20 years ago.
“We have a great obligation to people who put their lives on the line for the nation,” Victor J. Dzau, MD, president of the National Academy of Medicine, told Jacobs.
Dressed in blue scrubs and carrying a stethoscope around her neck, an oncology nurse in Salem, Ore., looked to the Grinch as inspiration while suggesting that she ignored coronavirus guidelines outside of work.
In a TikTok video posted Friday, she lip-dubbed a scene from “How the Grinch Stole Christmas” to get her point across to her unaware colleagues: She does not wear a mask in public when she’s not working at Salem Hospital.
“When my co-workers find out I still travel, don’t wear a mask when I’m out and let my kids have play dates,” the nurse wrote in a caption accompanying the video, which has since been deleted.
Following swift online backlash from critics, her employer, Salem Health, announced Saturday that the nurse had been placed on administrative leave. In a statement, the hospital said the nurse, who has not been publicly identified by her employer, “displayed cavalier disregard for the seriousness of this pandemic and her indifference towards physical distancing and masking out of work.”
“We also want to assure you that this one careless statement does not reflect the position of Salem Health or the hardworking and dedicated caregivers who work here,” said the hospital, adding that an investigation is underway.
Salem Health did not respond to The Washington Post’s request for comment as of early Monday.
The nurse’s video offers a startling and rare glimpse of a front-line health-care worker blatantly playing down a virus that has killed at least 266,000 Americans. It also has been seen in some coronavirus patients, some on their deathbeds, who still refuse to believe the pandemic is real.
The incident comes at a time when Oregon has continued to see a spike in new coronavirus cases and virus-related hospitalizations. Just last week, the state’s daily reported deaths and hospitalizations rose by 33.3 and 24.2 percent respectively, according to The Post’s coronavirus tracker. At least 74,120 Oregonians have been infected with the virus since late February; 905 of them have died.
The clip posted to TikTok on Friday shows the nurse mocking the health guidelines while using audio from a scene in which the Grinch reveals his true identity to Cindy Lou Who.
Although the original video was removed, TikTok users have shared a “duet” video posted by another user critical of the nurse, which had more than 274,000 reactions as of early Monday.
Soon after she posted the clip, hundreds took to social media and the hospital’s Facebook page to report the nurse’s video and demand an official response from her employer. Some requested that the nurse be removed from her position and that her license be revoked.
Hospital officials told the Salem Statesman Journal that the investigation is aiming to figure out which other staff members and patients have come in contact with the nurse, who works in the oncology department.
But for some, the hospital’s apologies and actions were not enough.
“The video supplied should be evidence enough,” one Facebook user commented. “She needs to be FIRED. Not on PAID leave. As someone fighting cancer, I can only imagine how her patients feel after seeing this news.”
The hospital thanked those who alerted them of the incident, emphasizing that its staff, patients and visitors must adhere to the Centers for Disease Control and Prevention guidelines.
“These policies are strictly enforced among staff from the moment they leave their cars at work to the moment they start driving home,” hospital officials told the Statesman Journal.