Regular readers of HEALTH CARE un-covered know that I write frequently about the huge amounts of money the health insurance industry’s pharmacy benefit managers (PBMs) extract from the prescription drug supply chain. I also submitted a comment letter to the Federal Trade Commission two and a half years ago urging it to launch an investigation into PBM business practices that have contributed to the closure of hundreds of independent pharmacies across the country and to millions of Americans walking away from the pharmacy counter without their medications.
On a bipartisan basis, the FTC did launch an inquiry into the PBM business, and today the Commission issued a damning interim report that confirmed what industry critics, including me, have been saying:
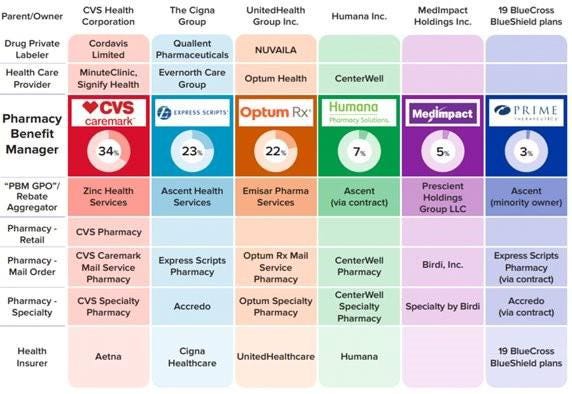
Just six companies now control 95% of the pharmacy benefit market, and these Big Insurance-owned middlemen “profit at the expense of patients by inflating drug costs and squeezing Main Street pharmacies.” Below you’ll find the commission’s statement on its preliminary findings.
Last year, we also published a profile of one of the industry’s most vocal critics in Congress, Rep. Earl L. “Buddy” Carter (R-Ga.), a pharmacist by trade who has seen PBM’s profiteering firsthand. In a press release this morning, Carter said:
Since day one in Congress, I’ve been calling on the FTC to investigate PBMs, which use deceptive and anti-competitive practices to line their own pockets while reducing patients’ access to affordable, quality health care. I’m proud that the FTC launched a bipartisan investigation into these shadowy middlemen, and its preliminary findings prove yet again that it’s time to bust up the PBM monopoly. We are losing more than one pharmacy per day in this country, causing pharmacy deserts and taking the most accessible health care professionals in America out of people’s communities. I am calling on the FTC to promptly complete its investigation and begin enforcement actions if – and when – it uncovers illegal and anti-competitive PBM practices.
Carter and several other members of Congress have introduced bipartisan bills to rein in PBMs. The House has passed PBM reform legislation but the Senate has not yet done so, but there is growing support in both chambers to enact one or more bills by the end of the year. The FTC’s interim report should make that more likely to happen.
Read the FTC’s full press release below:
FTC Releases Interim Staff Report on Prescription Drug Middlemen
Report details how prescription drug middleman profit at the expense of patients by inflating drug costs and squeezing Main Street pharmacies
The Federal Trade Commission today published an interim report on the prescription drug middleman industry that underscores the impact pharmacy benefit managers (PBMs) have on the accessibility and affordability of prescription drugs.
The interim staff report, which is part of an ongoing inquiry launched in 2022 by the FTC, details how increasing vertical integration and concentration has enabled the six largest PBMs to manage nearly 95 percent of all prescriptions filled in the United States.
This vertically integrated and concentrated market structure has allowed PBMs to profit at the expense of patients and independent pharmacists, the report details.
“The FTC’s interim report lays out how dominant pharmacy benefit managers can hike the cost of drugs—including overcharging patients for cancer drugs,” said FTC Chair Lina M. Khan. “The report also details how PBMs can squeeze independent pharmacies that many Americans—especially those in rural communities—depend on for essential care. The FTC will continue to use all our tools and authorities to scrutinize dominant players across healthcare markets and ensure that Americans can access affordable healthcare.”
The report finds that PBMs wield enormous power over patients’ ability to access and afford their prescription drugs, allowing PBMs to significantly influence what drugs are available and at what price. This can have dire consequences, with nearly 30 percent of Americans surveyed reporting rationing or even skipping doses of their prescribed medicines due to high costs, the report states.
The interim report also finds that PBMs hold substantial influence over independent pharmacies by imposing unfair, arbitrary, and harmful contractual terms that can impact independent pharmacies’ ability to stay in business and serve their communities.
The Commission’s interim report stems from special orders the FTC issued in 2022, under Section 6(b) of the FTC Act, to the six largest PBMs—Caremark Rx, LLC; Express Scripts, Inc.; OptumRx, Inc.; Humana Pharmacy Solutions, Inc.; Prime Therapeutics LLC; and MedImpact Healthcare Systems, Inc. In 2023, the FTC issued additional orders to Zinc Health Services, LLC, Ascent Health Services, LLC, and Emisar Pharma Services LLC, which are each rebate aggregating entities, also known as “group purchasing organizations,” that negotiate drug rebates on behalf of PBMs.
PBMs are part of complex vertically integrated health care conglomerates, and the PBM industry is highly concentrated. As shown in the below image, this concentration and integration gives them significant power over the pharmaceutical supply chain. The percentages reflect the amount of prescriptions filled in the United States.
The interim report highlights several key insights gathered from documents and data obtained from the FTC’s orders, as well as from publicly available information:
Concentration and vertical integration: The market for pharmacy benefit management services has become highly concentrated, and the largest PBMs are now also vertically integrated with the nation’s largest health insurers and specialty and retail pharmacies.
The top three PBMs processed nearly 80 percent of the approximately 6.6 billion prescriptions dispensed by U.S. pharmacies in 2023, while the top six PBMs processed more than 90 percent.
Pharmacies affiliated with the three largest PBMs now account for nearly 70 percent of all specialty drug revenue.
Significant power and influence: As a result of this high degree of consolidation and vertical integration, the leading PBMs now exercise significant power over Americans’ ability to access and afford their prescription drugs.
The largest PBMs often exercise significant control over what drugs are available and at what price, and which pharmacies patients can use to access their prescribed medications.
PBMs oversee these critical decisions about access to and affordability of life-saving medications, without transparency or accountability to the public.
Self-preferencing: Vertically integrated PBMs appear to have the ability and incentive to prefer their own affiliated businesses, creating conflicts of interest that can disadvantage unaffiliated pharmacies and increase prescription drug costs.
PBMs may be steering patients to their affiliated pharmacies and away from smaller, independent pharmacies.
These practices have allowed pharmacies affiliated with the three largest PBMs to retain high levels of dispensing revenue in excess of their estimated drug acquisition costs, including nearly $1.6 billion in excess revenue on just two cancer drugs in under three years.
Unfair contract terms: Evidence suggests that increased concentration gives the leading PBMs leverage to enter contractual relationships that disadvantage smaller, unaffiliated pharmacies.
The rates in PBM contracts with independent pharmacies often do not clearly reflect the ultimate total payment amounts, making it difficult or impossible for pharmacists to ascertain how much they will be compensated.
Efforts to limit access to low-cost competitors: PBMs and brand drug manufacturers negotiate prescription drug rebates some of which are expressly conditioned on limiting access to potentially lower-cost generic and biosimilar competitors.
Evidence suggests that PBMs and brand pharmaceutical manufacturers sometimes enter agreements to exclude lower-cost competitor drugs from the PBM’s formulary in exchange for increased rebates from manufacturers.
The report notes that several of the PBMs that were issued orders have not been forthcoming and timely in their responses, and they still have not completed their required submissions, which has hindered the Commission’s ability to perform its statutory mission. FTC staff have demanded that the companies finalize their productions required by the 6(b) orders promptly. If, however, any of the companies fail to fully comply with the 6(b) orders or engage in further delay tactics, the FTC can take them to district court to compel compliance.
The FTC remains committed to providing timely updates as the Commission receives and reviews additional information.
The Commission voted 4-1 to allow staff to issue the interim report, with Commissioner Melissa Holyoak voting no. Chair Lina M. Khan issued a statement joined by Commissioners Rebecca Kelly Slaughter and Alvaro Bedoya. Commissioners Andrew N. Ferguson and Melissa Holyoak each issued separate statements. The Federal Trade Commission develops policy initiatives on issues that affect competition, consumers, and the U.S. economy. The FTC will never demand money, make threats, tell you to transfer money, or promise you a prize. Follow the FTC on social media, read consumer alerts and the business blog, and sign up to get the latest FTC news and alerts.
On Tuesday, health system leaders testified before the House Energy and Commerce Subcommittee onOversight and Investigations about potential changes to the 340B Drug Pricing Program.
The committee was receptive to witnesses’ claims that the program is essential to the financial survival of many systems, but representatives stated that “the status quo is not acceptable” and that they had a responsibility to “step in and provide oversight.”
There was little interest expressed in broad overhauls to the program, but both witnesses and representatives focused on how it could benefit from greater transparency, for example requiring hospitals to disclose 340B revenue, how savings are used, and which patient populations are served through the program.
Meanwhile, Republicans and Democrats in both houses have introduced multiple bills this session that focus on various aspects of the 340B program, including transparency.
The Gist: It’s encouraging to see members of congress recognize how essential the 340B program is to health system finances, and of the potential reforms on the table, increased transparency is a relatively palatable option.
Congress is exploring statutory tweaks to the program in response to the myriad legal challenges concerning it, many of which involve the Department of Health and Human Services. Several of these lawsuits stem from more than 20 major drugmakers restricting 340B discounts at contract pharmacies, which has led multiple states to enact legislation protecting these discounts, in turn prompting further lawsuits.
The mess of conflicting rulings these cases have produced so far is a clear sign that the 340B statute will be amended, and health system advocates should continue working with Congress to find solutions that preserve the integrity of the program.
VillageMD, which is majority owned by Walgreens Boots Alliance, plans to shell out nearly $9 billion to pick up medical practice Summit Health, the parent company of urgent care clinic chain CityMD.
The deal, announced Monday morning, is valued at $8.9 billion and includes investments from Walgreens Boots Alliance and Cigna Corp’s healthcare unit Evernorth, which will also become a minority owner in VillageMD. Bloomberg first reported on a potential deal back in late October.
The deal will expand Walgreen’s reach into primary, specialty and urgent care. The transaction creates one of the largest independent provider groups in the U.S., the organizations said. Combined, VillageMD and Summit Health will operate more than 680 provider locations in 26 markets. The two companies will have 20,000 employees.
Walgreens said Monday it will invest $3.5 billion through an even mix of debt and equity to support the acquisition, which is expected to close in the first quarter of 2023. The company will remain the largest and consolidating shareholder of VillageMD with about 53% stake.
Walgreens also raised its fiscal year 2025 sales goal for its U.S. healthcare business to between $14.5 billion and $16 billion from $11 billion to $12 billion previously. That business segment is now expected to achieve positive adjusted EBITDA by the end of fiscal year 2023.
Last year, Walgreens invested $5.2 billion in VillageMD and said it planned to open at least 600 Village Medical at Walgreens primary-care practices across the country by 2025 and 1,000 by 2027.
The deal comes amid a frenzy of M&A activity in the past two years. Major retailers like CVS, Walgreens and Amazon are ramping up their focus on providing medical services to gain bigger footholds in the healthcare market.
Drugstore rival CVS Health won the bidding war for home health and technology services company Signify Health and plans to shell out $8 billion to acquire the company. Amazon also plans to buy primary care provider One Medical for $3.9 billion.
The M&A move signals that Walgreens wants to become a “dominant entity in the overall healthcare services ecosystem,” according to David Larsen, healthcare IT and digital health analyst at financial services firm BTIG.
“Walgreens Boots Alliance is graduating up from being a drug retail store to owning the life-cycle of members’ health,” he wrote in an analyst’s note. “We view this transaction as being a statement by the market that primary care continues to be one of the key drivers of healthcare long-term.”
The deal also will put additional pressure on CVS Health to break into the primary care business “sooner rather than later,” Larsen wrote.
“I think at the most strategic level, I think there continues to be recognition that an integrated, coordinated, connected model of care is one that will ultimately deliver the best results. You see this through Optum’s acquisition of Kelsey-Seybold Clinic and VillageMD’s acquisition of Summit Health,” Tim Barry, CEO and chair of VillageMD, said in an interview with Fierce Healthcare.
“If we’re going to ultimately stem the rising tide of this fee-for-service healthcare system, we need a better solution, and that solution needs to have doctors working with other doctors in a coordinated way and trying to solve the unique problems that these patients have and making sure that the right doctors are accessing the patient at the right time, and doing it all underneath the umbrella of a risk-based contract,” Barry said.
He added, “We think that this is going to continue to be where healthcare goes. And, we have to do it in a way that is integrated and value-oriented. Any organization focused on doing that, and doing that at size and scale, is going to continue, I think, to be the successful winners of our healthcare system.”
In 2019, Summit Medical Group, a physician-owned and governed multispecialty group, merged with CityMD, a leading urgent care company in New York City. The combined organization, Summit Health, has more than 370 locations in New Jersey, New York, Connecticut, Pennsylvania and Oregon.
VillageMD provides value-based primary care for patients at traditional free-standing practices, Village Medical at Walgreens practices, at home and via virtual visits. VillageMD and Village Medical have grown to 22 markets and are responsible for more than 1.6 million patients, according to the company.
Barry said the combination of VillageMD and Summit Health-CityMD will enable the organizations to scale up value-based care and build out integrated primary and specialty care services.
“If you look at the long history of Summit Health, it’s an organization that has done some very innovative things. The way that they deliver multispecialty care, it is truly integrated, it’s truly connected and they are known as the preeminent brand in their marketplace. They also have CityMD, which is one of the more unique and differentiated urgent care models out there in the market. They really are a best-of-breed organization,” he said.
“When I look at what we’ve been able to do at VillageMD, we built this incredible model of value-based primary care delivery. The idea of bringing these two organizations together to bring those best-of-breed capabilities under one umbrella was just so compelling. We will soon be able to offer a more comprehensive, integrated and connected model by also offering other specialty services to our patients, but all still done through a value or risk-based reimbursement structure.”
Barry is bullish on the combined capabilities of the two companies in the primary and specialty care markets.
“We’ll be delivering a consistent value-based model of integrated, multispecialty care in a way that delivers the best clinical results on the planet,” he said.
Jeff Alter, CEO of Summit Health-CityMD, said in a statement that the deal adds Summit Health’s expertise and geographic coverage to VillageMD’s proven value-based primary care approach.
The acquisition also expands Walgreens’ reach into providing medical care directly to patients. “This transaction accelerates growth opportunities through a strong market footprint and wide network of providers and patients across primary, specialty and urgent care,” Roz Brewer, CEO of Walgreens Boots Alliance, said in a statement.
With Cigna’s investment, the combined company will be able to tap into Evernorth’s health services capabilities to potentially lower healthcare costs, Barry said. Evernorth encompasses Cigna’s health services businesses including pharmacy benefit manager Express Scripts
“In order to be a risk-based provider or a value-based provider, you have to have contracts with a payer that allows you to work in this value or risk-based construct. We learned over the years that Cigna has been a really good partner to us on that journey,” Barry said.
“There are companies that [Cigna] has purchased over the years that have different specializations and capabilities that we believe ultimately will allow us to deliver better care to our patients,” he noted. “Evernorth has some capabilities tied to behavioral health, and they have some capabilities tied to the management of specialty pharmaceutical spend, which everyone knows those costs continue to be soaring. We both liked the idea of supporting an organization like ours that’s going to continue to grow and continues to be focused on risk and value.”
With the investment in VillageMD and Summit Health, Cigna gets a leg up in the primary care space as it looks to build out its Evernorth division.
“Our collaboration with VillageMD accelerates our efforts to improve the way care is accessed and delivered,” said Eric Palmer, CEO of Evernorth, in a statement. “Harnessing the breadth of Evernorth’s health services capabilities and connecting them with physicians who provide care in a value-based model like VillageMD, helps more people to get the right care at the right time—driving better health and value.”
CELINA, Tenn. — It was about 1 a.m. on April 19, 2016, when a burglary alarm sounded at Dale Hollow Pharmacy in Celina, a tiny town in the rolling, wooded hills near the Kentucky border.
Two cops responded. As their flashlights bobbed in the darkness, shining through the pharmacy windows, they spotted a sign of a break-in: pill bottles scattered on the floor.
The cops called the co-owner, Thomas Weir, who arrived within minutes and let them in. But as quickly as their flashlights beamed behind the counter, Weir demanded the cops leave. He said he’d rather someone “steal everything” than let them finish their search, according to a police report and body camera footage from the scene.
“Get out of there right now!” Weir shouted, as if shooing off a mischievous dog. “Get out of there!”
The cops argued with Weir as he escorted them out. They left the pharmacy more suspicious than when they’d arrived, triggering a probe in a small town engulfed in one of the most outsize concentrations of opioids in a pill-ravaged nation.
Nearly six years later, federal prosecutors have unveiled a rare criminal case alleging that Celina pharmacy owners intentionally courted opioid seekers by filling dangerous prescriptions that would have been rejected elsewhere. The pharmacies are accused of giving cash handouts to keep customers coming back, and one allegedly distributed its own currency, “monkey bucks,” inspired by a pet monkey that was once a common sight behind the counter. Two pharmacists admitted in plea agreements they attracted large numbers of patients from “long distances” by ignoring red flags indicating pills were being misused or resold. In their wake, prosecutors say, these Celina pharmacies left a rash of addiction, overdoses, deaths, and millions in wasted tax dollars.
“I hate that this is what put us on the map,” said Tifinee Roach, 38, a lifelong Celina resident who works in a salon not far from the pharmacies and recounted years of unfamiliar cars and unfamiliar people filling the parking lots. “I hate that this is what we’re going to be known for.”
Celina, an old logging town of 1,900 people about two hours northeast of Nashville, was primed for this drug trade: In the shadow of a dying hospital, four pharmacies sat within 1,000 feet of each other, at the crux of two highways, dispensing millions of opioid pills. Before long, that intersection had single-handedly turned Tennessee’s Clay County into one of the nation’s pound-for-pound leaders of opioid distribution. In 2017, Celina pharmacies filled nearly two opioid prescriptions for every Clay County resident — more than three times the national rate — according to the Centers for Disease Control and Prevention.
Visitors once came to Celina to tour its historical courthouse or drop their lines for smallmouth bass in the famed fishing lake nearby. Now they came for pills.
Soon after Weir’s police encounter in 2016, the Drug Enforcement Administration set its sights on his two Celina pharmacies, three doors apart — Dale Hollow Pharmacy and Xpress Pharmacy. Separately, investigators examined the clinic of Dr. Gilbert Ghearing, which sat directly between Dale Hollow and Xpress and leased office space to a third pharmacy in the same building, Anderson Hometown Pharmacy. Its owners and operators have not been charged with any crime.
In December, a federal judge unsealed indictments against Weir and the other owners of Dale Hollow and Xpress pharmacies, Charles “Bobby” Oakley and Pamela Spivey, alleging they profited from attracting and filling dangerous and unjustifiable opioid prescriptions. Charges were also filed against William Donaldson, the former pharmacist and owner of Dale Hollow, previously convicted of drug dealing, who allegedly recruited most of the customers for the scheme.
The pharmacists at Dale Hollow and Xpress, John Polston and Michael Griffith, pleaded guilty to drug conspiracy and health care fraud charges and agreed to cooperate with law enforcement against the other suspects.
Ghearing was indicted on drug distribution charges for allegedly writing unjustifiable opioid prescriptions in a separate case in 2019. He pleaded not guilty, and his case is expected to go to trial in September.
‘An American Tragedy’
The Celina indictment comes as pharmacies enter an era of new accountability for the opioid crisis. In November, a federal jury in Cleveland ruled pharmacies at CVS, Walgreens, and Walmart could be held financially responsible for fueling the opioid crisis by recklessly distributing massive amounts of pain pills in two Ohio counties. The ruling — a first of its kind — is expected to reverberate through thousands of similar lawsuits filed nationwide.
Criminal prosecutions for such actions remain exceedingly rare. The Department of Justice in recent years increased prosecutions of doctors and pain clinic staffers who overprescribed opioids but files far fewer charges against pharmacists, and barely any against pharmacy owners, who are generally harder to hold directly responsible for prescriptions filled at their establishments.
In a review of about 1,000 news releases about legal enforcement actions taken by the Department of Health and Human Services since 2019, KHN identified fewer than 10 similar cases involving pharmacists or pharmacy owners being criminally charged for filling opioid prescriptions. Among those few similar cases, none involved allegations of so many opioids flowing readily through such a small place.
The Celina case is also the first time the Department of Justice sought a restraining order and preliminary injunction against pharmacies under the Controlled Substances Act, said David Boling, a spokesperson for the U.S. Attorney’s Office for the Middle District of Tennessee. DOJ used the civil filing to shut down Dale Hollow and Xpress pharmacies quickly in 2019, allowing prosecutors more time to build a criminal case against the pharmacy owners.
Former U.S. Attorney Don Cochran, who oversaw much of the investigation, said the crisis in Celina was so severe it warranted a swift and unique response.
Cochran said it once made sense for small pharmacies to be clustered in Celina, where a rural hospital served the surrounding area. But as the hospital shriveled toward closure, as have a dozen others in Tennessee, the competing pharmacies turned to opioids to sustain themselves and got hooked on the profits, he said.
“It’s an American tragedy, and I think the town was a victim in this,” Cochran said. “The salt-of-the-earth, blue-collar folks that lived there were victimized by these people in these pharmacies. I think they knew full well this was not a medical necessity. It was just a money-making cash machine for them.”
And much of that money came from taxpayers. In its court filings, DOJ argues the pharmacies sought out customers with Medicaid or Medicare coverage — or signed them up if they didn’t have it. To keep these customers coming back, the pharmacies covered their copays or paid cash kickbacks whenever they filled a prescription, prosecutors allege. The pharmacies collected more than $2.4 million from Medicare for opioids and other controlled substances from 2012 to 2018, according to the court filings.
Prosecutors say the pharmacies also paid kickbacks to retain profitable customers with non-opioid prescriptions. In one case, Dale Hollow gave $100 “payouts” to a patient whenever they filled his prescription for mysoline, an anti-seizure drug, then used those prescriptions to collect more than $237,000 from Medicare, according to Polston’s plea agreement.
Attorneys for Weir, Oakley, Donaldson, Spivey, Polston, and Griffith either declined to comment for this article or did not respond to requests for comment.
Ronald Chapman, an attorney for Ghearing, defended the doctor’s prescriptions, saying he’d done “the best he [could] with what was available” in a rural setting with no resources or expertise in pain management.
Chapman added that, while he does not represent the other Celina suspects, he had a theory as to why they drew the attention of federal law enforcement. As large corporate pharmacies made agreements with the federal government to be more stringent about opioid prescriptions, they filled fewer of them. Customers then turned to smaller pharmacies in rural areas to get their drugs, he said.
“I’m not sure if that’s what happened in this case, but I’ve seen it happen in many small towns in America. The only CVS down the street, or the only Rite Aid down the street, is cutting off every provider who prescribes opioids, leaving it to smaller pharmacies to do the work,” Chapman said.
Donaldson, reached briefly at his home in Celina on March 9, insisted the allegations levied against Dale Hollow and Xpress could apply to many pharmacies in the region.
“It wasn’t just them,” Donaldson said.
The Monkey and the Monkey Bucks
Long before it was called Dale Hollow Pharmacy, the blue-and-white building that moved millions of pills through Celina was Donaldson Pharmacy, and Donaldson was behind the counter doling out pills.
Donaldson owned and operated the pharmacy for decades as the eccentric son of one of the most prominent families in Celina, where a street, a park, and many businesses bear his surname. Even now, despite Donaldson’s prior conviction for opioid crimes and his new indictment, an advertisement for “Donaldson Pharmacy” hangs at the entrance of a nearby high school.
“Bill has always had a heart of gold, and he would help anyone he could. I just think he let that, well …” said Pam Goad, a neighbor, trailing off. “He’s always had a heart of gold.”
According to interviews with about 20 Celina residents, including Clay County Sheriff Brandon Boone, Donaldson is also known to keep a menagerie of exotic animals, at one point including at least two giraffes, and a monkey companion, “Carlos,” whom he dressed in clothing.
The monkey — a mainstay at Donaldson Pharmacy for years — both attracted and deterred customers. Linda Nelson, who owns a nearby business, said Carlos once escaped the pharmacy and, during a scrap with a neighbor’s dogs, tore down her mailbox by snapping its wooden post in half.
But the monkey wasn’t the only reason Donaldson Pharmacy stood out.
According to a DEA opioid database published by The Washington Post, Donaldson Pharmacy distributed nearly 3 million oxycodone and hydrocodone pills from 2006 to 2014, making it the nation’s 20th-highest per capita distributor during that period. It retained its ranking even though the pharmacy closed in 2011, when Donaldson was indicted for dispensing hydrocodone without a valid prescription.
Donaldson confessed to drug distribution and was sentenced to 15 months in prison. The pharmacy’s name was changed to Dale Hollow and ended up with Donaldson’s brother-in-law, Oakley. In 2014, Oakley sold 51% of the business to Weir, who also bought a majority stake of Xpress Pharmacy, three doors away, according to the DOJ’s civil complaint.
Under Weir’s leadership, these two pharmacies became an opioid hub with few equals, prosecutors say. From 2015 to 2018, Dale Hollow and Xpress pharmacies were the fourth-and 11th-highest per capita opioid purchasers in the nation, according to the DOJ, citing internal DEA data.
Many of these prescriptions were for Subutex, an opioid that can be used to treat addiction but is itself prone to abuse. Unless the patient is pregnant or nursing or has a documented allergy, Tennessee law requires doctors instead to prescribe Suboxone, an alternative that is much harder to abuse.
But at the Celina pharmacies, prescriptions for Subutex outnumbered those for Suboxone by at least 4-to-1, prosecutors say. In their plea agreements, pharmacists from Dale Hollow and Xpress described stores that thrived on the trade in Subutex, and said Weir set “mandates” for how many Subutex prescriptions to fill and instructed them to “never run out.”
Griffith, the head pharmacist at Xpress, said the pharmacy in 2015 created flyers specifically advertising Subutex, then delivered them on trays of cookies to practices throughout Tennessee, including some hours away. In the following two years, the amount of Subutex dispensed by Xpress increased by about eightyfold, according to his plea agreement.
Dale Hollow didn’t need flyers or cookies. It had Donaldson.
After getting out of prison in 2014, Donaldson was hired by the pharmacy he once owned, where he “recruited and controlled” about 50% to 90% of customers, according to the indictment filed against him. The pharmacy also enticed customers by distributing a Monopoly-like currency called “monkey bucks” — an apparent callback to Carlos — that could be spent at the pharmacy like cash, the indictment states.
Prosecutors also allege that, from a desk inside Dale Hollow, Donaldson would sign customers up for Medicare or Medicaid, then use a vehicle provided by the pharmacy to drive them to a doctor’s office to get opioid prescriptions, then back to Dale Hollow where he’d offer to cover their copays himself if they kept their business at the pharmacy. Sometimes, he would text the Dale Hollow pharmacist with instructions to fill specific prescriptions, or just to fill more of them, according to federal court records.
“Y’all have got to get your numbers up. Fill fill,” Donaldson texted Polston in 2018, according to his plea agreement.
By then, however, all those prescriptions had drawn unwanted attention.
In August 2018, Dale Hollow and Xpress pharmacies were raided by DEA agents, who brought with them Fox News’ Geraldo Rivera and a television crew. Six months later, DOJ filed its civil complaint, persuading a federal judge to immediately close both pharmacies.
Today, Dale Hollow Pharmacy sits shuttered, as it has been for the past three years, and a paper sign taped to the door says animals are not allowed inside by order of the DEA. The building that was once Xpress Pharmacy reopened this year as an unrelated pharmacy with a fresh coat of paint. Ghearing’s clinic and Anderson Hometown Pharmacy are closed.
Most of Celina’s opioid prescriptions are gone, too. According to the latest available CDC data, Clay County reported about 32 opioid prescriptions per 100 residents in 2020 — one-sixth the rate of 2017’s.
Late last week, retail giant Walmart announced its plan to acquire national telemedicine provider MeMD, for an undisclosed sum. According to Dr. Cheryl Pegus, Walmart’s executive vice president for health, the acquisition “complements our brick-and-mortar Walmart Health locations”, allowing the company to “expand access and reach consumers where they are”.
MeMD, founded in 2010, provides primary care and mental health services to five million patients nationally. The acquisition extends Walmart’s health delivery capabilities beyond the handful of in-store and store-adjacent clinics it runs, and follows the launch of its own Medicare Advantage-focused broker business, and partnership with Medicare Advantage start-up Clover Health to offer a co-branded insurance product.
Walmart has been climbing the healthcare learning curve for several years, building on its sizeable retail pharmacy business, and seems to have hit on a successful formula in its latest in-person clinic model, which includes primary care, behavioral health, vision, and dental services. The retailer plans to add 22 new clinic locations by the end of this year, and its new telemedicine offering will allow it to expand its virtual reach even further.
The MeMD acquisition alsorepresents a new front in Walmart’s head-to-head competition with Amazon, which launched its own national telemedicine service earlier this year. That service, Amazon Care, is targeted at the employer market, and right on cue, Amazon announced its first customer sale last week—to Precor, a fitness equipment company.
Both retail giants are slowly circling the $3.6T healthcare industry, targeting inefficiencies by deploying their expertise in convenience and consumer engagement.Incumbents beware.
Uber Health is partnering with e-prescription startup ScriptDrop in a deal expanding the ride-hailing giant’s prescription delivery footprint from a few cities to dozens of U.S. states.
Uber first forayed into medication delivery in several metro areas in August through a deal with digital delivery marketplace NimbleRx, as the pandemic caused a surge in patient demand for the service.
With this latest deal, Uber’s hundreds of thousands of drivers will be accessible to pharmacies using ScriptDrop in 37 states across the U.S. ScriptDrop, a third-party tech platform connecting patients and pharmacies with couriers nationwide, will pay Uber for the cost of each delivery.
But the San Francisco-based company is also hoping the crowded but lucrative at-home prescription drug delivery market will be profitable, following mounting losses last year as the coronavirus pandemic pummeled ride-hailing companies.
Growth in Uber’s delivery business has outpaced plummeting ridesharing revenue during COVID-19. In fourth quarter earnings released February, Uber’s gross bookings in its mobility business were down 50% year over year, while gross bookings in its delivery segment were up 130%.
This latest deal suggests Uber is doubling down on delivery, banking that demand for at-home drug delivery remains high beyond COVID-19.
ScriptDrop integrates with a pharmacy’s software system to provide same-day shipping medication delivery options, and also has a consumer-facing portal for drop-offs. As of today, Uber is integrated with ScriptDrop via an application programming interface, and will become the default option for select pharmacies depending on location and driver availability, the companies said.
ScriptDrop doesn’t share the exact number of U.S. pharmacies working with its platform, but a spokesperson told Healthcare Dive they partner with thousands. ScriptDrop clients include prominent pharmacies like Albertsons, Kmart and Safeway; pharmacy systems such as PDX and a number of courier companies, health systems and insurers.
The partnership is operational in 37 states as of today, including California, Florida, New York and Texas. Uber and ScriptDrop have additional plans for near-term expansion, in some cases in new states in the next couple of weeks, the spokesperson said.
Uber first launched consumer-facing prescription delivery in several U.S. cities through the Uber Eats app, in the partnership with NimbleRx. That’s grown from a pilot in Seattle and Dallas to cities including New York, Miami, Austin and Houston, with more metro areas to come, according to Uber.
Prescription drug delivery companies have reported skyrocketing utilization during COVID-19. Columbus, Ohio-based ScriptDrop has said delivery volume jumped 363% from February to April last year, while revenue tripled between October 2019 and October 2020. The startup announced a $15 million funding round in October to drive growth, bringing its total funding to $27 million since launching in 2017.
Partially as a result of COVID-19 tailwinds, the prescription tech sector, which includes e-prescription vendors like NimbleRx and ScriptDrop, is expected to grow at a compound annual growth rate of 16%, the quickest of the enterprise health and wellness segments, according to a February report from Pitchbook.
Despite consumer demand for at-home prescription delivery, it’s a crowded market. Most major pharmacies, including CVS Health and Walgreens, have hustled to build out their delivery networks in the past few years, facing potential disruption from outside entrants, notably Amazon.
COVID-19 accelerated a number of trends already brewing in the healthcare industry, and that’s not likely to change this year, according to a new report from CVS Health.
The healthcare giant released its annual Health Trends Report on Tuesday, and the analysis projects several industry trends that are likely to define 2021 in healthcare, ranging from technology to behavioral health to affordability.
“We are facing a challenging time, but also one of great hope and promise,” CVS CEO Karen Lynch said in the report. “As the pandemic eventually passes, its lessons will serve to make our health system more agile and more responsive to the needs of consumers.”
Here’s a look at four of CVS’ predictions:
1. A looming mental health crisis
Behavioral health needs were a significant challenge in healthcare prior to COVID-19, but the number of people reporting declining mental health jumped under the pandemic.
Cara McNulty, president of Aetna Behavioral Health, said in a video attached to the report that it will be critical to “continue the conversation around mental health and well-being” as we emerge from the pandemic and to reduce stigma so people who need help seek it out.
“We’re normalizing that it’s important to take care of our mental well-being,” she said.
Data released in December by GoodRx found that prescription fills for depression and anxiety medications hit an all-time high in 2020. GoodRx researchers polled 1,000 people with behavioral health conditions on how they were navigating the pandemic, and 63% said their depression and/or anxiety symptoms worsened.
McNulty said symptoms to look for when assessing whether someone is struggling with declining mental health include whether they’re withdrawn or agitated or if there’s a notable difference in their self-care routine.
2. Pharmacists take center stage
CVS dubbed 2021 “the year of the pharmacist” in its report.
The company expects pharmacists to be a key player in a number of areas, especially in vaccine distribution as that process inches toward broader access. They also offer a key touchpoint to counsel patients about their care and direct them to appropriate services, CVS said.
CVS executives said in the report that they see a significant opportunity for pharmacists to have a positive impact on the social determinants of health.
“We’ve found people are not only open and willing to share social needs with their pharmacists but in many cases, they listen to and act on the advice and recommendations of pharmacists,” Peter Simmons, vice president of transformation, pharmacy delivery and innovation at CVS Health, said in the report.
3. Finding ways to mitigate the cost of high-price therapies
Revolutionary drugs and therapies are coming to market with eye-popping price tags; it’s not uncommon to see new pharmaceuticals priced at $1 million or more. For pharmacy benefit managers, this poses a major cost challenge.
To address those prices, CVS expects value-based contracting to take off in a big way. And drugmakers are comfortable with the idea, according to the report. Novartis, for example, is offering insurers a five-year payment plan for its $2 million gene therapy Zolgensma, with refunds available if the drug doesn’t achieve desired results.
CVS said the potential for these therapies is clear, but many payers want to see some type of results before they fork over hundreds of thousands.
“Though the drug may promise to cure these patients for life, these are early days in their use,” said Joanne Armstrong, M.D., enterprise head of women’s health and genomics at CVS Health, in the report. “What we’re saying is, show us the clinical value proposition first.”
CVS said it’s also offering a stop-loss program for gene therapy to self-funded employers contracted with Aetna and/or Caremark to assist them in capping the expenses associated with these drugs.
4. Getting into the community to address diabetes
Diabetes risk is higher among vulnerable populations, such as Black patients, and addressing it will require local and community-based solutions, CVS executives said in the report. Groups at the highest risk for the disease are less likely to live in areas with easy access to a supermarket, for example, which boosts their risk of unhealthy eating, according to the report.
The two key hurdles to addressing this issue are access and affordability. The rise in retail clinics and ambulatory care centers can get at the access issue, as they can offer a way to better meet patients where they are.
At CVS’ MinuteClinics, patients can walk in and receive a number of services to assist them in managing diabetes, including screenings, consultations with providers and connections to diabetes educators who can assist with lifestyle changes.
Retail locations can also assist with medication costs, creating a one-stop-shop experience that’s easier for many diabetes patients to slot into their daily lives, CVS said.
“Diabetes is a case study in how a more connected experience can translate to simpler, affordable and more accessible care for underserved communities,” said Dan Finke, executive vice president of CVS Health and president of its healthcare benefits division.