LHC, a postacute care behemoth with several hundred home health and hospice locations, as well as a dozen long-term care hospitals, would greatly expand Optum’s ability to provide home-based and long-term care. The FTC’s second request for information threatens to delay the deal, which was set to close in the latter half of this year.
The Gist: The LHC deal is the second UnitedHealth Group (UHG) transaction that antitrust regulators have targeted recently. The Department of Justice filed alawsuit earlier this year to block UHG’s acquisition of Change Healthcare, alleging that acquiring a direct competitor for claims solutions would reduce competition.
The FTC has historically focused its efforts on horizontal integration, but the LHC scrutiny, in combination with a recent inquiry into pharmacy benefit managers, indicates its focus may be expanding to vertical integration.
At its annual meeting this week, the AMA’s policymaking arm voted to adopt resolutions opposing state efforts that criminalize abortion or limit access to reproductive healthcare. This comes ahead of the much-anticipated Supreme Court decision, which is expected to overturn the 1973 Roe v. Wade decision. The nation’s largest physician organization joined the American College of Obstetricians and Gynecologists in calling on the Food and Drug Administration to make birth control pills available over-the-counter and without age restrictions. The AMA also declared climate change a public health crisis, as physicians are already seeing negative health effects from heat-related injuries.
The Gist: As a new generation of physicians has entered the workforce, the policy priorities of physician lobbying organizations have evolved. We are seeing a growing interest in addressing hot-button social issues head-on. The AMA has declared both gun violence and racism to be public health issues, and supports health insurance coverage expansion, positions that would have been unimaginable a few decades ago.
Though progressive on social issues, however, the AMA is still advocating against state efforts to expand mid-level providers’ scope of practice—maintaining its traditional role as a protector of the physician guild.
Wilmington, Del.-based ChristianaCare plans to buy a shuttered hospital from West Reading, Pa.-based Tower Health.
The deal includes Jennersville Hospital in West Grove, Pa., two office buildings and a 24-acre parcel of land, according to a June 15 ChristianaCare news release. It does not include any personnel or practices that are currently operating.
The hospital will have the new name of ChristianaCare West Grove Campus. The deal is expected to close in 30 to 60 days.
Jennersville Hospital closed Dec. 31. Tower Health was supposed to sell the hospital, along with Coatesville, Pa.-based Brandywine Hospital, to Texas turnaround firm Canyon Atlantic Partners Jan. 1, but pulled out of the deal, stating that Canyon Atlantic was unable to demonstrate it could effectively take ownership.
A judge later ordered Tower Health to restart the sale, but Canyon Atlantic eventually ended the bid, saying it ran out of time to save the hospitals.
ChristianaCare also signed a letter of intent in February to acquire Springfield, Pa.-based Crozer Health from Los Angeles-based Prospect Medical Holdings.
Credit rating downgrades for several hospitals and health systems were tied to cash flow issues in recent months.
The following seven hospital and health system credit rating downgrades occurred since February:
1. Jupiter (Fla.) Medical Center — lowered in June from “BBB+” to “BBB” (Fitch Ratings) “The ‘BBB’ rating reflects JMC’s increased leverage profile with the issuance of $150 million in additional debt to fund various campus expansion and improvement projects,” Fitch said. “While favorable population growth in the service area and demonstrated demand for services in an increasingly competitive market justify the overall strategic plan and project, the additional debt weakens JMC’s financial profile metrics and increases the overall risk profile.”
2. ProMedica (Toledo, Ohio) — lowered in May from “BBB-” to “BB+” (Fitch Ratings) “The long-term ‘BB+’ rating and the assigned outlook to negative on ProMedica Health System’s debt reflects the system’s significant financial challenges as result of continued pressure of the coronavirus pandemic and escalating expenses, with ProMedica reporting a $252 million operating loss that follows several years of weak performance,” Fitch said.
3. Providence (Renton, Wash.) — lowered in April from “Aa3” to to “A1” (Moody’s Investors Service); lowered from “AA-” to “A+” (Fitch Ratings) “The downgrade to ‘A1’ is driven by the disaffiliation with Hoag Hospital, and the expectation that weaker operating, balance sheet, and debt measures will continue for the time being,” Moody’s said.
4. San Gorgonio Memorial Healthcare District (Banning, Calif.) — lowered in May from “Ba1” to “Ba2” (Moody’s Investors Service) “The downgrade to Ba2 reflects the district’s tenuous cash position and weak finances that have contributed to difficulty in securing a bridge loan financing for liquidity needs pending the delayed receipt of approximately $8 million to $9 million in intergovernmental transfers beyond the end of the fiscal year,” Moody’s said.
5. Willis-Knighton Medical Center (Shreveport, La.) — lowered in March from “A1” to “A2” (Moody’s Investors Service) “The downgrade to A2 reflects expectations that Willis-Knighton will continue to face challenges in achieving budgeted operating cash flow margins due to heightened wage pressures and volume softness,” Moody’s said.
6. OU Health (Oklahoma City) — lowered in March from “Baa3” to “Ba2” (Moody’s Investors Service) “The magnitude of the downgrade to Ba2 reflects projected cashflow in fiscal 2022 that will be materially below prior expectations, from an escalation of labor costs, and reliance on a financing to avoid a further decline in already weak liquidity and potential covenant breach,” Moody’s said. “Also, the rating action reflects execution risk given a prolonged period of management turnover with several key positions unfilled or filled with interim leaders, a governance consideration under Moody’s ESG classification.”
7. Catholic Health System (Buffalo, N.Y.) — lowered in February from “Baa2” to “B1” (Moody’s Investors Service) “The downgrade to ‘B1’ anticipates minimal cashflow and a further significant decline in liquidity this year, following material losses in fiscal 2021 from a 40-day labor strike and the disproportionately severe impact of the pandemic, both social risks under Moody’s ESG classification,” the credit rating agency said.
The U.S. Supreme Court sided with hospital groups June 15 in a case challenging HHS’ 340B payment cuts.
The case centered around whether CMS has the authority to make cuts to the program under its Medicare Outpatient Prospective Payment System. Under the payment rule, HHS cut the reimbursement rate for covered drugs by 28.5 percent in 2018, but it later lowered the reimbursement rate cut to 22.5 percent.
Under the 340B program, eligible hospitals can buy outpatient drugs at a discount. A hospital typically pays 20 percent to 50 percent below the average sales price for the drugs through the program.
The Supreme Court reversed a federal appeals court’s 2020 ruling that HHS had the authority to make the $1.6 billion annual reimbursement cut.
Justice Brett Kavanaugh, writing the opinion for the court’s unanimous decision, said that absent a survey of hospitals’ acquisition costs, HHS may not vary the reimbursement rate for 340B hospitals.
“HHS’s 2018 and 2019 reimbursement rates for 340B hospitals were therefore contrary to the statute and unlawful,” he wrote. The American Hospital Association, Association of American Medical Colleges and America’s Essential Hospitals said in a joint statement emailed to Becker’s following the decision that they look forward to working with HHS and the courts to develop a plan to reimburse 340B hospitals affected by the cuts while ensuring other hospitals are not disadvantaged as they also continue to serve their communities.
The right to bear arms has existed since we became a nation. So, too, has the risk of violence that extensive gun ownership creates in our society.
Unfortunately, recent mass shooting incidents, fueled by hatred or mental illness, have sparked a great deal of fear and confusion among Americans.
As healthcare leaders, our concern centers on the treatment of those who are victims of senseless gun violence. And not just those who are shot, but the other victims as well.
Healthcare providers must care for all victims — the ones who are traumatized because a loved one has been hurt or lost, the ones who were at the chaotic scene of the violence, or who are haunted by the endless media stories they cannot seem to tune out. The emotional toll of this violence is incomprehensible.
Healthcare facilities attempt to provide refuge from violence and seek to provide healing and hope to all victims of violence.
Unstable individuals with guns and other weapons of harm find their way into our buildings and hallways as well. Earlier this month, a man who blamed his physician for ongoing pain after a recent back surgery shot and killed his surgeon and three other people before fatally shooting himself in a Tulsa, Okla., medical facility. Also this month, a hospital security officer was shot and killed by a prison inmate who was receiving care in a Dayton, Ohio, emergency room.
These incidents are the latest horrifying tragedies in a wave of deadly gun violence occurring across our country, including two heart-breaking mass shootings in Buffalo, N.Y., and Uvalde, Texas. We mention these tragedies not to make a political statement, but to raise awareness of the consequences of this violence on healthcare providers and the public health.
As healthcare workers, healers, and caregivers, we work to fix what is broken and put people back together. We bring solutions. We engage with our hearts to stand together in the fear and vulnerabilities of those who need us so that we can help them through difficult challenges. We look to bring light to dark situations. We seek to be beacons of hope.
The escalation of recent shootings, suicides and other violent behaviors underscores the urgency for a national conversation on what has become a serious public health crisis. We believe health systems have a credible voice and can play a critical role beyond being places to physically and emotionally care for the victims of violence.
It’s easy to allow ourselves to become numb to the frequency of these unconscionable, violent acts. But we owe it to present and future generations not to let that happen. We recognize there are no easy answers to this national problem. After all, we are dealing with abnormal behavior — the decision to seriously harm or kill other people. That this behavior is increasing calls for something to be done to effect positive change.
People across our country and the communities we serve are hurting and vulnerable. Many people are weary from the pandemic that has impacted our hearts and our health. Violence and death, and particularly mass shootings, hit adults hard. Now consider what the prevalence and threat of school shootings have done to an entire generation of children, who are growing up with the fear of being shot and killed in a place they should feel safe.
We all can play a role. Recently, our two organizations decided to do something to reduce gun violence by sponsoring a law enforcement gun buyback program to help get guns off the street. This effort was part of the largest single-day gun buyback in New Jersey state history. It successfully removed over 2,800 guns statewide. Private organizations, companies, and individuals must think of additional creative ways beyond criticizing politicians, to bring about the change we need.
We encourage organizations and communities to come together, to pool their minds and their resources to address gun violence in society as the urgent public health crisis that it is. We must create meaningful public health campaigns around the safe storage and handling of firearms, and sensible and innovative ways to prevent gun violence in schools, healthcare settings and public places. Individuals should educate themselves on the issues surrounding gun violence so they may contribute to the effort to bring about necessary and meaningful change.
And yes, we need to accelerate efforts around our nation’s mental health crisis. We know from the data and what we are all experiencing that the COVID-19 pandemic has exacerbated what was already a growing nationwide mental health crisis.
Violence against any person in any venue is unspeakable. Yet just because it is unspeakable does not mean we should not speak up about it. Let us put our anger, shock and heartbreak into positive change. With the same unstoppable resolution that we seek to cure cancer or slow heart disease, let us advocate, educate and take meaningful action to end gun violence and all senseless violence that is taking such a tragic toll on our nation and our wellbeing.
About Virtua Health Virtua Health is an academic health system committed to helping the people of South Jersey be well, get well, and stay well by providing the complete spectrum of advanced, accessible, and trusted healthcare services. Virtua’s 14,000 colleagues provide tertiary care, including renowned cardiology and transplant programs, complemented by a community-based care portfolio. In addition to five hospitals, two satellite emergency departments, 30 ambulatory surgery centers, and more than 300 other locations, Virtua brings health services directly into communities through Hospital at Home, physical therapy and rehabilitation, mobile screenings, and its paramedic program. Virtua has 2,850 affiliated doctors and other clinicians, and its specialties include orthopedics, advanced surgery, and maternity. Virtua is academically affiliated with Rowan University, leading research, innovation, and immersive education at the Virtua Health College of Medicine & Health Sciences of Rowan University. Virtua is also affiliated with Penn Medicine for cancer and neuroscience, and the Children’s Hospital of Philadelphia for pediatrics. As a not-for-profit, Virtua is committed to the well-being of the community and provides innovative outreach programs that address social challenges affecting health, most notably the “Eat Well” food access initiative, which includes the unparalleled Eat Well Mobile Grocery Store. A Magnet-recognized health system ranked by U.S. News and World Report, Virtua has received many awards for quality, safety, and its outstanding work environment. For more information, visit Virtua.org. To help Virtua make a difference, visit GiveToVirtua.org.
About Cooper University Health Care Cooper University Health Care is a leading academic health system with more 8,500 employees and more than 800 employed physicians. Cooper University Hospital is the only Level 1 Trauma Center in South Jersey and the busiest in the region. Annually, nearly two million patients are served at Cooper’s 635-bed flagship hospital, outpatient surgery center, three urgent care centers, and more than 105 ambulatory offices throughout the community. The Cooper Health Sciences campus is home to Cooper University Hospital, MD Anderson Cancer Center at Cooper, Children’s Regional Hospital at Cooper, and Cooper Medical School of Rowan University. Visit CooperHealth.org to learn more.
The Federal Reserve just raised interest rates by three-quarters of a percentage point, the biggest single increase in interest rates since 1994. It’s another move in the Fed’s effort to tackle the fastest inflation in four decades.
I understand the Fed’s urgency, but it has entered dangerous territory. If the Fed continues down this path – as it has signaled it will – the economy will be plunged into a recession. Every time over the last half century the Fed has raised interest rates this much and this quickly, it has caused a recession.
Besides, interest rate increases will not remedy the major causes of the current inflation – huge pent-up worldwide demand from two years of pandemic, shortages of goods and services responding to that demand, Putin’s war in Ukraine, and big profitable corporations with enough pricing power to use inflation as a cover for pushing up prices even further.
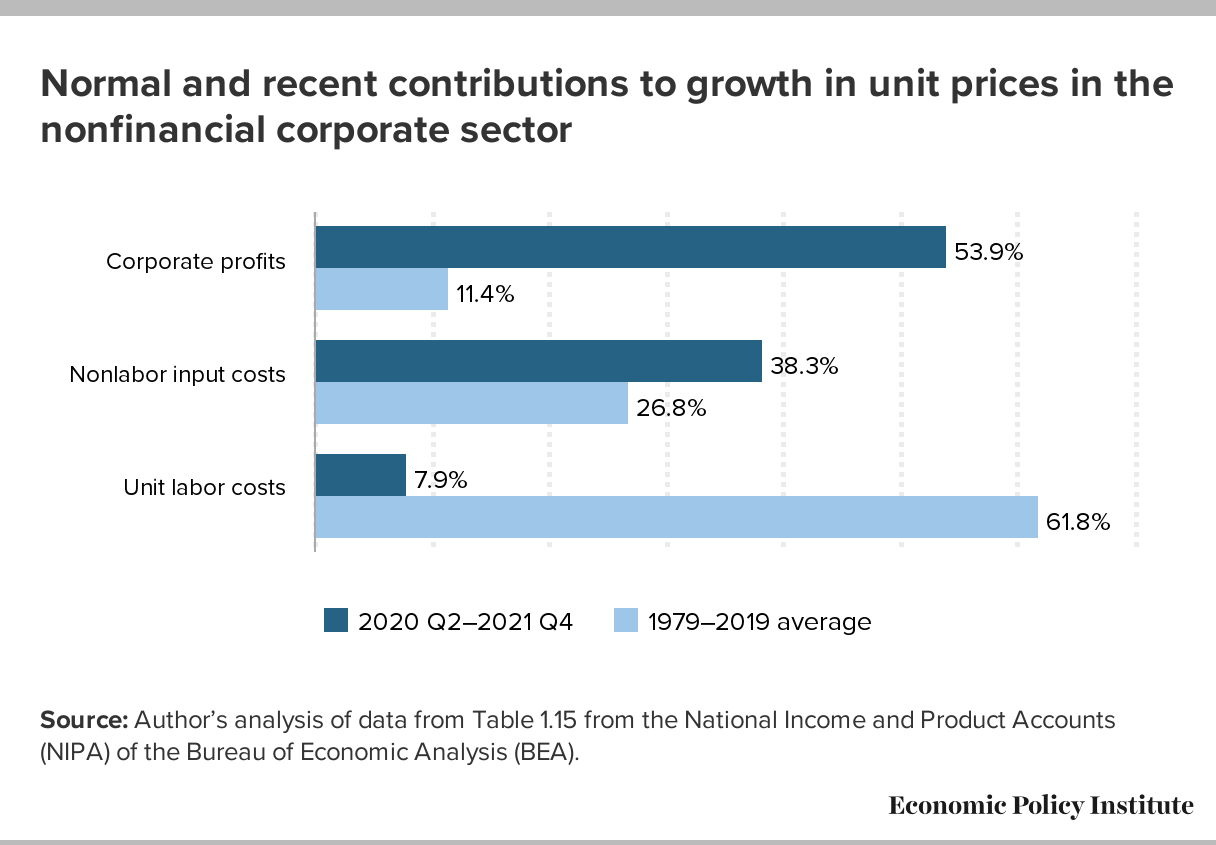
The Fed assumes that price increases are being driven by wage increases — so-called “wage-price inflation.” That’s incorrect. Wages are lagging behind inflation. A more accurate description of what we’re now seeing might be called “profit-price inflation” — prices driven upward by corporations seeking increased profits. (See chart below, from the Economic Policy Institute.)
A recession will be especially harmful to people who are most vulnerable to downturns in the economy — who are the first to be fired (and last to be hired again when the economy turns upward): lower-wage workers, disproportionately women and people of color.
Social factors impact a person’s health and their potential health outcomes. While this has long been discussed (especially by folks of color, individuals with lived experiences, and those in public health), it is finally now getting deserved mainstream attention, including by health insurers.
Medicare Advantage (MA) — a program that offers private plan alternatives to traditional Medicare — is one key player looking at social determinants of health. It’s a good thing, too; an estimated 42% of the Medicare population are enrolled in MA plans, and that share grows each year. MA plans have more flexibility in offering supplemental benefits and services, some of which can address social determinants of health.
In 2018, the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act passed with bipartisan support and marked a substantial shift in MA policy by including acknowledgment of the role of social determinants of health. It allows even greater flexibility for MA plans to help with the very conditions that impact how a person lives, such as providing financial assistance for nutritional needs, transportation to appointments, caregiver support, and even home construction projects. Interestingly, it does not mandate coverage, so it is still dependent on what plans an individual has access to and how health plans are choosing to move forward with this freedom.
The problem is, however, that most individuals aren’t eligible for Medicare until age 65 (there are some exceptions). If we wait until Medicare eligibility to act on social determinants of health, are we waiting too long?
The short answer is yes. Although addressing social determinants of health in the Medicare-eligible population is important, what we know suggests that more could be done earlier.
Why are social determinants important in Medicare Advantage?
Chronic disease is a significant issue among Medicare-eligible individuals, and one that’s exacerbated by social determinants of health. There are substantial implications for both beneficiaries and MA plans. For beneficiaries, chronic disease affects not only their quality of life, but also their wallet. From the plans’ perspectives, the presence of comorbid chronic diseases is a significant differentiator between so called “high cost” beneficiaries and those who are not.
Current MA enrollment trends also point to the need to sharpen the focus on social determinants of health. Although they make up a minority of MA enrollees, persons of color are enrolling in MA plans at a breakneck pace: especially among Black people, dual enrollees, and people living in disadvantaged neighborhoods.
Historically, these are folks most negatively impacted by social determinants of health, and the likelihood of poor health outcomes is only compounded when enrollees reside in disadvantaged neighborhoods. These are neighborhoods commonly characterized by high concentrations of poverty, crime, and harmful environmental exposures compounded by limited resources to support economic and social well-being, and research has consistently found strong associations between neighborhood disadvantage and health risks and outcomes.
Health systems must do more about social determinants earlier in life
Social determinants of health affect us all — regardless of age. Until recently, they have received relatively little attention from insurers.
It is difficult though to discern the extent that these actions are altruistic or opportunistic, especially when they can technically be both. While that might not be the worst thing, it does matter if it leaves out the very people it should be helping.
Let’s consider internet access, for example. If a patient isn’t connected to the web, they can’t participate in a telehealth visit, leaving in-person care as the only option. In a world where telehealth visits are reimbursed at a fraction of the in-person rate, there are substantial cost savings (read: profit) associated with facilitating and promoting virtual care. Critics have also pointed out that most of these steps can be attributed to insurers’ philanthropic apparatuses as opposed to any substantive change or innovation in member benefits.
What is also becoming readily apparent, is that while telehealth use is increasing, it does not make care accessible for everyone. It could even serve to increase disparities if it is not done properly.
However, administrative hurdles and societal stigma can challenge people’s willingness to participate in these programs no matter how beneficial they might be. We should all be asking what more the health system — providers, payers, and government — should be doing to improve social determinants of health earlier in life.
The CHRONIC Care Act has the potential to mitigate some of these harmful impacts of long-standing structural inequities by providing greater flexibility for plans to cover non-medical needs. The law illustrates that policymakers believe that health insurers should do more to address social determinants of health. Perhaps they should also focus on how plans can address these social factors earlier in the life cycle as well.
RWJBarnabas Health on Tuesday called off its attempt to acquire St. Peter’s Healthcare System in New Brunswick, N.J., days after the Federal Trade Commission sued to block the proposed transaction.