In 2020, a record-breaking 19 rural hospitals closed their doors due to a combination of worsening economic conditions, changing payer mix, and declining patient volumes. But many more are looking to affiliate with larger health systems to remain open and maintain access to care in their communities. The graphic above illustrates how rural hospital affiliations (including acquisitions and other contractual partnerships) have increased over time, and the resulting effects of partnerships.
Affiliation rose nearly 20 percent from 2007 to 2016; today nearly half of rural hospitals are affiliated with a larger health system.
Economic stability is a primary benefit: the average rural hospital becomes profitable post-affiliation, boosting its operating margin roughly three percent in five years. But despite improved margins, many affiliated rural hospitals cut some services, often low-volume obstetrics programs, in the years following affiliation.
Overall, the relationship likely improves quality: a recent JAMA study found that rural hospital mergers are linked to better patient mortality outcomes for certain conditions, like acute myocardial infarction. Still, the ongoing tide of rural hospital closures is concerning, leaving many rural consumers without adequate access to care. Late last month, the Department of Health and Human Services announced it would distribute another $7.5B in American Rescue Plan Act funds to rural providers.
While this cash infusion may forestall some closures, longer-term economic pressures, combined with changing consumer demands, will likely push a growing number of rural hospitals to seek closer ties with larger health systems.
Several hospitals across the U.S. are laying off workers over the next three months.
Below are nine hospitals and health systems that laid off employees or announced plans to implement layoffs since Oct. 1.
1. Community Hospital Long Beach (Calif.) plans to lay off 328 employees early next year, according to a notice filed with state regulators. The hospital said the layoffs are set to begin after Jan. 31, 2022, and may come in stages. The layoffs are a result of Community Hospital Long Beach ending acute care and closing its emergency department.
2. Watsonville (Calif.) Community Hospital is preparing to lay off 677 workers, according to a notice filed with the state Nov. 29. The hospital entered Chapter 11 bankruptcy Dec. 5 and announced a tentative sale agreement with the Pajaro Valley Healthcare District Project. If the sale to the nonprofit group or another buyer is finalized by Jan. 28, all 677 employees will be terminated by Watsonville Community Hospital. CEO Steven Salyer said all potential buyers are being asked to offer employment to the hospital’s workers. If the sale isn’t finalized, the hospital will close after the bankruptcy court authorizes those steps, and all employees would be terminated Jan. 28, according to the notice to the state. Funds made available through the bankruptcy process may allow the hospital to delay the layoffs.
3. Pensacola, Fla.-based Baptist Health Care said in a notice filed with state regulators that it is eliminating 233 jobs in February when it outsources various services to Wayne, Pa.-based Compass One Healthcare. Affected employees were offered positions with Compass One at the same or higher wages, according to the Nov. 22 layoff notice.
4. West Reading, Pa.-based Tower Health filed a notice in early November with state regulators indicating it would lay off 293 employees by Dec. 31. The health system said the layoffs would affect workers at Jennersville Hospital in West Grove, Pa., which Tower Health was planning to close by the end of the year. In late November, the health system announced it entered into a definitive agreement to sell Jennersville Hospital and another facility to Canyon Atlantic Partners, a hospital management firm based in Austin, Texas. The health system subsequently called off that deal. It plans to close Jennersville Hospital on Dec. 31 and Brandywine Hospital in Coatesville, Pa., on Jan. 31. The closures will result in the loss of more than 800 jobs, according to the Philadelphia Business Journal.
5. Columbia University Irving Medical Center in New York City is laying off 56 workers in February, but affected employees will be offered employment with NewYork-Presbyterian Hospital, according to a notice filed with the state Nov. 8. The layoffs are due to the integration of electronic medical records systems at Columbia University Irving Medical Center and NewYork-Presbyterian Hospital, according to the notice.
6. Ascension Technologies, the IT subsidiary of St. Louis-based Ascension, outsourced about 330 tech jobs in November, according to a notice filed with the state. Affected employees could apply for other positions within Ascension Technologies or with the new vendor that took over the tech support for application and platforms, collaboration and end-user engineering, network and telecom and field services areas.
7. Middletown, N.Y.-based Garnet Healthlaid off 66 workers Oct. 29 when it closed its skilled nursing unit, according to a notice filed with the state.
8. Kindred Hospital Northwest Indiana, a 70-bed long-term acute care hospital in Hammond, is closing, resulting in 110 layoffs, according to a notice filed with the state in August. The layoffs started Oct. 10. Kindred said the closure is a result of Mishawaka, Ind.-based Franciscan Health’s decision to downsize its Hammond hospital, a move that will eliminate Kindred’s space on the campus.
9. Garland (Texas) Behavioral Hospital, part of King of Prussia, Pa.-based Universal Health Services, is closing and laying off its 119 employees, according to the Dallas Morning News. The layoffs started Oct. 7, according to a notice filed with the state.
COVID-19-related hospitalizations have been on an upward trend in New York state since last month, but there appears to be a drastic divide between the Big Apple and some of the state’s more rural areas, health data shows.
In New York City, the seven-day average of new COVID-19 hospitalizations per 100,000 people rose from 0.5 on Nov. 10 to 1.1 on Dec. 7, the New York State Department of Health said.
The story is different in several counties hundreds of miles north, where new COVID-19 hospitalizations are rising at a higher rate. In the Finger Lakes region, officials in several counties declared a state of emergency after the seven-day average of new COVID-19 hospitalizations per 100,000 people went from 2.9 on Nov. 10 to 4.9 on Dec. 7.
David Larsen, an associate professor of public health at Syracuse University, told ABC News that there are several factors behind this divide, but the most important one is the lower vaccination rates in certain counties upstate.
“At the end of the day, you’re more likely to get severe COVID-19 symptoms and go to the hospital if you’re not vaccinated,” Larsen said.
Health experts and state officials predict the situation upstate is only going to get worse during the holidays and colder months, but the tide can be turned if more people get their shots and heed health warnings.
As of Dec. 8, 74.9% of all New York state residents have at least one COVID-19 vaccine dose, but those numbers vary by region, according to state health data.
New York City and Long Island had over 78% of their populations with at least one shot, the state data showed. Further north, the rates for at least one dose in the Mohawk Valley, the Finger Lakes and North Country sections were 60.6%, 68.5%, and 63% respectively.
There is even more division within the regions when it comes to vaccination, the data shows; for example, counties that are along the Interstate 87 corridor, such as Hamilton, Schenectady and Saratoga, all have rate of at least one dose above 75% of their populations.
Counties directly west of those locations, Schoharie, Fulton and Montgomery, have one-dose vaccination rates under 65%, the state data showed.
New York Gov. Kathy Hochul has repeatedly highlighted that the unvaccinated are the ones suffering and being hospitalized.
“It is a conscious decision not to be vaccinated. And the direct result is a higher rate of individuals in those regions upstate as well as it has a direct correlation to the number of hospitalizations,” she said during a Dec. 2 news conference.
Dr. Isaac Weisfuse, an adjunct professor of public health at Cornell University, told ABC News that there are fewer options for upstate residents to turn to for medical help and fewer hospitals in the area are handling patients from more locations.
Weisfuse, a former deputy health commissioner for New York City’s Health Department, noted that New York City residents have much closer access to amenities like free testing sites and medical clinics than their upstate counterparts.
“If you live in a rural county in New York state and it takes a while to get to a doctor, you may put it off. So when you do eventually go get care, you may be sicker versus someone who lives closer and gets a quicker diagnosis,” he said.
Larsen added that there has been pandemic fatigue across the country, and many Americans have scaled back on mitigation measures, especially mask-wearing indoors.
“We’re doing less mask wearing. What that does is it increases transmission, which is fine for the vaccinated people but it does go to the unvaccinated people and they are higher risk,” he said.
Weisfuse said the hospitalizations are likely to grow upstate and have ripple effects for those regions. The governor has ordered elective surgeries to be postponed at 32 hospitals upstate that have seen their available beds decrease.
State officials said they are beefing up their marketing efforts to encourage eligible New Yorkers to get their shots.
Weisfuse said this outreach needs to be done meticulously if upstate officials want to avoid more overcrowded emergency rooms this winter.
“The state needs to take a good look at the pockets of non-vaccination,” he said. “They need to make some targeted intervention in those neighborhoods.”
Anyone who needs help scheduling a free vaccine appointment can log onto vaccines.gov.
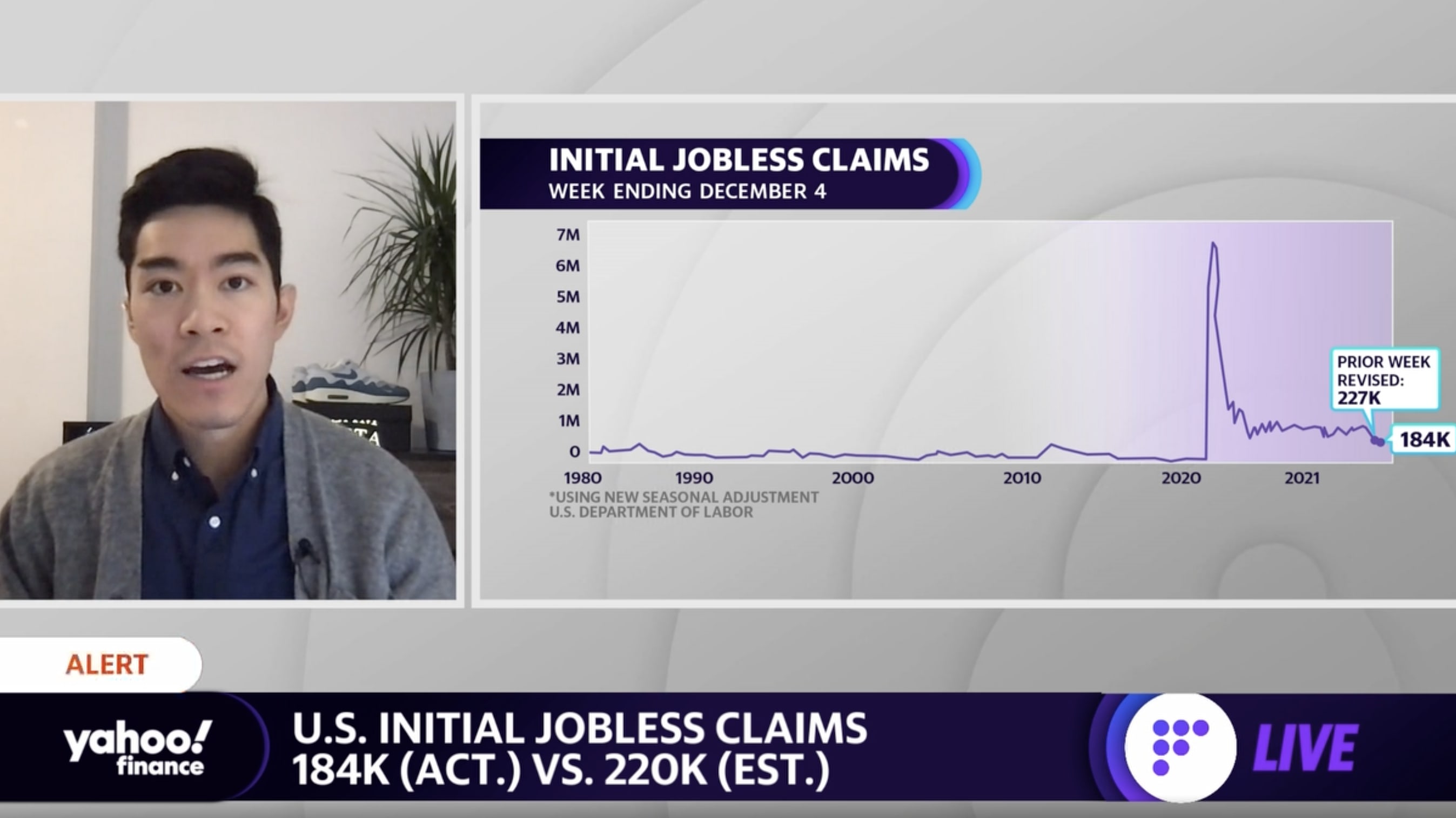
New initial jobless claims improved much more than expected last week to reach the lowest level in more than five decades, further pointing to the tightness of the present labor market as many employers seek to retain workers.
Initial unemployment claims, week ended Dec. 4: 184,000 vs. 220,000 expected and an upwardly revised 227,000 during prior week
Continuing claims, week ended Nov. 27: 1.992 millionvs. 1.910 million expected and a downwardly revised 1.954 million during prior week
Jobless claims decreased once more after a brief tick higher in late November. At 184,000, initial jobless claims were at their lowest level since Sept. 1969.
“The consensus always looked a bit timid, in light of the behavior of unadjusted claims in the week after Thanksgiving in previous years when the holiday fell on the 25th, but the drop this time was much bigger than in those years, and bigger than implied by the recent trend,” Ian Shepherdson, chief economist for Pantheon Macroeconomics, wrote in an email Thursday morning. “A correction next week seems likely, but the trend in claims clearly is falling rapidly, reflecting the extreme tightness of the labor market and the rebound in GDP growth now underway.”
After more than a year-and-a-half of the COVID-19 pandemic in the U.S., jobless claims have begun to hover below even their pre-pandemic levels. New claims were averaging about 220,000 per week throughout 2019. At the height of the pandemic and stay-in-place restrictions, new claims had come in at more than 6.1 million during the week ended April 3, 2020.
Continuing claims, which track the number of those still receiving unemployment benefits via regular state programs, have also come down sharply from pandemic-era highs, and held below 2 million last week.
“Beyond weekly moves, the overall trend in filings remains downward and confirms that businesses facing labor shortages are holding onto workers,” wrote Rubeela Farooqi, chief U.S. economist for High Frequency Economics, in a note on Wednesday.
Farooqi added, however, that “the decline in layoffs is not translating into faster job growth on a consistent basis, which was evident in a modest gain in non-farm payrolls in November.”
“For now, labor supply remains constrained and will likely continue to see pandemic effects as the health backdrop and a lack of safe and affordable child care keeps people out of the workforce,” she added.
Other recent data on the labor market have also affirmed these lingering pressures. The November jobs report released from the Labor Department last Friday reflected a smaller number of jobs returned than expected last month, with payrolls growing by the least since December 2020 at just 210,000. And the labor force participation rate came in at 61.8%, still coming in markedly below its pre-pandemic February 2020 level of 63.3%.
And meanwhile, the Labor Department on Wednesday reported thatjob openings rose more than expected in October to top 11 million, coming in just marginally below July’s all-time high of nearly 11.1 million. The quits rate eased slightly to 2.8% from September’s record 3.0% rate.
“There is a massive shortage of labor out there in the country that couldn’t come at a worst time now that employers need workers like they have never needed them before. This is a permanent upward demand shift in the economy that won’t be alleviated by companies offering greater incentives to their new hires,” Chris Rupkey, FWDBONDS chief economist, wrote in a note Wednesday. “Wage inflation will continue to keep inflation running hot as businesses fall all over themselves in a bidding war for talent.”
Top US scientist Anthony Fauci said Tuesday that while it would take weeks to judge the severity of the new Covid-19 variant Omicron, early indications suggested it was not worse than prior strains, and possibly milder.
Speaking to AFP, President Joe Biden’s chief medical advisor broke down the knowns and unknowns about Omicron into three major areas: transmissibility, how well it evades immunity from prior infection and vaccines, and severity of illness.
The new variant is “clearly highly transmissible,” very likely more so than Delta, the current dominant global strain, Fauci said.
Accumulating epidemiological data from around the world also indicates re-infections are higher with Omicron.
Fauci, the long-time director of the National Institute of Allergies and Infectious Diseases (NIAID), said lab experiments that tested the potency of antibodies from current vaccines against Omicron should come in the “next few days to a week.”
On the question of severity, “it almost certainly is not more severe than Delta,” said Fauci.
“There is some suggestion that it might even be less severe, because when you look at some of the cohorts that are being followed in South Africa, the ratio between the number of infections and the number of hospitalizations seems to be less than with Delta.”
But he added it was important to not over-interpret this data because the populations being followed skewed young, and were less likely to become hospitalized.
“I think that’s going to take another couple of weeks at least in South Africa,” where the variant was first reported in November, he said.
“As we get more infections throughout the rest of the world, it might take longer to see what’s the level of severity.”
Fauci said a more transmissible virus that doesn’t cause more severe illness and doesn’t lead to a surge of hospitalizations and deaths was the “best case scenario.”
“The worst case scenario is that it is not only highly transmissible, but it also causes severe disease and then you have another wave of infections that are not necessarily blunted by the vaccine or by people’s prior infections,” he added.
“I don’t think that worst case scenario is going to come about, but you never know.”