
Cartoon – Implementing Artificial Intelligence


Companies grappling with liquidity concerns are looking to cut costs and streamline operations, according to a new survey.
Though inflationary pressures have eased since the height of the COVID-19 pandemic, healthcare CFOs remain cognizant of managing costs amid liquidity concerns, according to the report.
The firm polled 100 healthcare CFOs serving hospitals, medical groups, outpatient services, academic centers and home health providers with revenues from $250 million to $3 billion or more in October 2023.
Just over a third of organizations surveyed carried more than 60 days of cash on hand. In comparison, a recent analysis from KFF found that financially strong health systems carried at least 150 days of cash on hand in 2022.
Liquidity is a concern for CFOs given high rates of bond and loan covenant violations over the past year. More than half of organizations violated such agreements in 2023, while 41% are concerned they will in 2024, according to the report.
To remain solvent, 44% of CFOs expect to have more strategic conversations about their economic resiliency in 2024, exploring external partnerships, options for service line adjustments and investments in workforce and technology optimization.
The majority of CFOs surveyed are interested in pursuing external partnerships, despite increased regulatory roadblocks, including recent merger guidance that increased oversight into nontraditional tie-ups. Last week, the FTC filed its first healthcare suit of the year to block the acquisition of two North Carolina-based Community Health Systems hospitals by Novant Health, warning the deal could reduce competition in the region.
Types of deals that CFOs are exploring, as of Oct. 2023.
https://datawrapper.dwcdn.net/aiFBJ/1
Most organizations are interested in exploring sales, according to the report. Financially struggling organizations are among the most likely to consider deals. Nearly one in three organizations that violated their bond or loan covenants in 2023 are planning a carve-out or divestiture this year. Organizations with less than 30 days of cash on hand are also likely to consider carve-outs.
Organizations will also turn to automation to cut costs. Ninety-eight percent of organizations surveyed had piloted generative AI tools in a bid to alleviate resource and cost constraints, according to the consultancy.
“Healthcare leaders believe AI will be essential to helping clinicians operate at the top of their licenses, focusing their time on patient care and interaction over administrative or repetitive tasks,” authors wrote. Nearly one in three CFOs plan to leverage automation and AI in the next 12 months.
However, CFOs are keeping an eye on the risks. As more data flows through their organizations, they are increasingly concerned about cybersecurity. More than half of executives surveyed said data breaches are a bigger risk in 2024 compared to 2023.

CFOs and finance department recruiters have faced a workforce problem for years now, labor experts say: a shrinking pool of U.S. accounting professionals needed to close the books every quarter, complete audits, and make sure the company’s financials comply with GAAP and other regulations.
The hits that have chipped away at accounting labor health are myriad and the statistics stark. While the number of practicing accountants and auditors in the U.S. spiked in 2019, across the past decade since 2013 the total declined by about 10% to 1.62 million last year, with roughly 190,000 jobs disappearing from the work rolls, according to the Bureau of Labor Statistics.
Meanwhile, the total number of test takers who passed the CPA Exam fell to 18,847 in 2022 from 19,544 the year earlier, and the lowest level since 2007, according to the latest numbers available from the Association of International Certified Professional Accountants.
Studies and those analyzing the trend point to a variety of likely culprits: the onerous 150 hours of course credit — equivalent to a fifth year of college — students typically need to become a CPA, generally lower starting salaries compared to other areas of finance, and the demanding hours and rising regulations that lead some practicing accountants to look for the exits once they’re in the field. At the same time, the launch of the generative AI tool ChatGPT in late 2022 led to a new wave of questions about the industry’s future.
Tom Hood, executive vice president of business engagement and growth at the AICPA, is in the optimistic camp of those who believe the pipeline decline is poised to turn around, noting that he has seen other cycles when disruptive shocks such as Microsoft’s Excel in the 1980s damped interest and sparked doomsday talk around the possible “end of accounting.”
“We’ve had ebbs and flows, we’ve had these shortages before and every time that’s happened we as a profession have rallied together,” said Hood, a CPA, adding that AI will automate certain tasks in accounting but will not replace accountants. “We’ve moved this needle before and I think we’re already starting to see it move now.”
In 2024 professional associations and lawmakers are working on numerous initiatives as well as legislation to close the cracks that have leaked talent from the field. In the meantime, companies have found ways to get the staff needed to get their finance work done. CFO Dive talked to experts about some notable tactics that are likely to shape the accounting workforce this year.
States, CPAs and the 150-hour credit question
Currently state regulatory bodies that set the rules require those who want to to become a Certified Public Accountant to have 150 credit hours of education in accounting or related subjects to become a licensed CPA. But amid the growing shortage, there has been a controversial push by states to create another pathway to licensure which include cutting the college credit hour requirement back to 120 hours.
For example, this year Minnesota lawmakers are expected to consider new legislation introduced in the state’s Senate and House in 2023 that would allow candidates to earn a CPA certificate with only 120 hours of college credit, along with passing the CPA exam and some additional work experience or professional education. This alternative would be in addition to the current system that requires 150 hours and one year of work experience, plus passing the CPA exam.
Geno Fragnito, director of government relations for the Minnesota Society of CPAs that supports the change, notes that the current national shift to the 150 rule gained steam in the 1980s after Florida made the change amid a surplus of accountants due to many wanting to move to the state. Florida started the ball rolling by increasing the credit hour requirement to 150 hours in 1983, according to a Journal of Accountancy report.
But in recent years, the MNCPA’s members have consistently pinpointed the credit requirement as one of the main contributors to the drop in CPAs.
“I don’t think there was a meeting that either our CEO or I attended where it was not brought up organically. It was never on our agenda to discuss but it always came up,” Fragnito said. Looking ahead, Fragnito said that other states that are seeking to tweak the credit hour formula include South Carolina and Washington state.
A “volatile year” for CPA exam takers
Two exam-related changes are impacting accounting candidates this year in very different ways. “It’s an exciting time but I think 2024 will be a very volatile year,” Mike Decker, vice president of the CPA Examination & Pipeline Extension for AICPA, said in a recent interview. One of the changes is student-friendly: it’s designed to ease deadline pressures and address pandemic-related delays that might have affected some test takers. In a move announced last spring, the National Association of State Boards of Accountancy extended the window that a candidate has to complete the exam once they pass the first section from 18 months to 30 months. The move grew out of the AICPA’s effort to address the accounting shortage, known as its pipeline acceleration plan.
Meanwhile, this month marked the launch of a revamped CPA Exam called the CPA Evolution. The test has both new content and structure and a greater focus on technology in an effort to combat research that found that accounting firms were hiring fewer accountants in favor of non-accountants with tech backgrounds, according to a Nov. 7 report by Michael Potenza of Becker. “It’s not that CPA Evolution is meant to be harder than the previous version of the exam, it’s simply meant to better prepare you for the skills and competencies needed in modern accounting,” Potenza, a CPA, wrote.
Raises and remote work
Tactics that CFOs themselves are using to meet their staff needs include sweetened offers and going offshore or considering remote workers to gain talent. With most small and medium-size CPA firms unable to find enough qualified U.S. accountants, this summer a study found that over half of firms planned to hike starting salaries by 14%, CFO Dive previously reported. Lisa Simpson, vice president of firm services at AICPA, is hearing about similar approaches taken by firm leaders she’s spoken with. In the past few years, she said, firm leaders indicated they were providing several high percentage salary increases for new hires and existing employees. Last year firms gave raises at rates above inflation as well as continuing bonuses, and business leaders said they expect to continue raises into 2024.
Meanwhile, many firms are outsourcing U.S. accounting work to professionals in India, the Philippines, and Eastern European countries like Poland, according to Matt Wood, head of global FAO Services at Austin, Texas-based Personiv, a global outsourcing provider which serves those needs. While outsourcing to other companies was previously the domain of larger firms, the pandemic has led to more companies being comfortable with remote accounting staff, he said.
The shift to hiring accounting staff outside the U.S. “has been happening for a while now, but it really accelerated in 2020. The accounting talent pool was already shrinking, and businesses were feeling the impact of that pre-pandemic. Then, all of these other pieces fell into place; teams were working remotely and protecting cashflow took priority,” Wood said in an emailed response to questions from CFO Dive.

In Sunday’s Axios’ AM, Mike Allen observed “Republicans know immigration alone could sink Biden. So, Trump and House Republicans will kill anything, even if it meets or exceeds their wishes. Biden knows immigration alone could sink him. So he’s willing to accept what he once considered unacceptable — to save himself.”
Mike called this a “truth Bomb” and he’s probably right: the polarizing issue of immigration is tantamount to a bomb falling on the political system forcing well-entrenched factions to re-think and alter their strategies.
In 2024, in U.S. healthcare, three truth bombs are in-bound. They’re the culmination of shifts in the U.S.’ economic, demographic, social and political environment and fueled by accelerants in social media and Big Data.
Truth bomb: The regulatory protections that have buoyed the industry’s growth are no longer secure.
Despite years of effectively lobbying for protections and money, the industry’s major trade groups face increasingly hostile audiences in city hall, state houses and the U.S. Congress.
The focus of these: the business practices that regulators think protect the status quo at the public’s expense. Example: while the U.S. House spent last week in their districts, Senate Committees held high profile hearings about Medicare Advantage marketing tactics (Finance Committee), consumer protections in assisted living (Special Committee on Aging), drug addiction and the opioid misuse (Banking) and drug pricing (HELP). In states, legislators are rationalizing budgets for Medicaid and public health against education, crime and cybersecurity and lifting scope of practice constraints that limit access.
Drug makers face challenges to patents (“march in rights”) and state-imposed price controls. The FTC and DOJ are challenging hospital consolidation they think potentially harmful to consumer choice and so. Regulators and lawmakers are less receptive to sector-specific wish lists and more supportive of populist-popular rules that advance transparency, disable business relationships that limit consumer choices and cede more control to individuals. Given that the industry is built on a business-to-business (B2B) chassis, preparing for a business to consumer (B2C) time bomb will be uncomfortable for most.
Truth bomb: Affordability in U.S. is not its priority.
The Patient Protection and Affordability Act 2010 advanced the notion that annual healthcare spending growth should not exceed more than 1% of the annual GDP. It also advanced the premise that spending should not exceed 9.5% of household adjusted gross income (AGI) and associated affordability with access to insurance coverage offering subsidies and Medicaid expansion incentives to achieve near-universal coverage. In 2024, that percentage is 8.39%.
Like many elements of the ACA, these constructs fell short: coverage became its focus; affordability secondary.
The ranks of the uninsured shrank to 9% even as annual aggregate spending increased more than 4%/year. But employers and privately insured individuals saw their costs increase at a double-digit pace: in the process, 41% of the U.S. population now have unpaid medical debt: 45% of these have income above $90,000 and 61% have health insurance coverage. As it turns out, having insurance is no panacea for affordability: premiums increase just as hospital, drug and other costs increase and many lower- and middle-income consumers opt for high-deductible plans that expose them to financial insecurity. While lowering spending through value-based purchasing and alternative payments have shown promise, medical inflation in the healthcare supply chain, unrestricted pricing in many sectors, the influx of private equity investing seeking profit maximization for their GPs, and dependence on high-deductible insurance coverage have negated affordability gains for consumers and increasingly employers. Benign neglect for affordability is seemingly hardwired in the system psyche, more aligned with soundbites than substance.
Truth bomb: The effectiveness of the system is overblown.
Numerous peer reviewed studies have quantified clinical and administrative flaws in the system. For instance, a recent peer reviewed analysis in the British Medical Journal concluded “An estimated 795 000 Americans become permanently disabled or die annually across care settings because dangerous diseases are misdiagnosed. Just 15 diseases account for about 50.7% of all serious harms, so the problem may be more tractable than previously imagined.”
The inadequacy of personnel and funding in primary and preventive health services is well-documented as the administrative burden of the system—almost 20% of its spending. Satisfaction is low. Outcomes are impressive for hard-to-diagnose and treat conditions but modest at best for routine care. It’s easier to talk about value than define and measure it in our system: that allows everyone to declare their value propositions without challenge.
Truth bombs are falling in U.S. healthcare. They’re well-documented and financed. They take no prisoners and exact mass casualties.
Most healthcare organizations default to comfortable defenses. That’s not enough. Cyberwarfare, precision-guided drones and dirty bombs require a modernized defense. Lacking that, the system will be a commoditized public utility for most in 15 years.
PS: Last week’s report, “The Holy War between Hospitals and Insurers…” (The Keckley Report – Paul Keckley) prompted understandable frustration from hospitals that believe insurers do not serve the public good at a level commensurate with the advantages they enjoy in the industry. However, justified, pushback by hospitals against insurers should be framed in the longer-term context of the role and scope of services each should play in the system long-term. There are good people in both sectors attempting to serve the public good. It’s not about bad people; it’s about a flawed system.

Earlier this month, we released our year-end report on hospital and health system M&A activity in 2023. As a follow-up to that report, here are our thoughts on the five most interesting transactions announced in the past year.[1]
We are early in the year, but 2024 has started with a bang: the announced acquisition of Summa Health, based in Akron, Ohio, by General Catalyst’s Healthcare Assurance Transformation Corporation (HATCo).[3] The acquisition, when completed, would launch HATCo on its path to fulfill one of the three goals set forth during the October 2023 announcement of its formation: “acquiring and operating a health system for the long term where we can demonstrate the blueprint of [healthcare] transformation for the rest of the industry.”

The struggle continues as hospital executives work overtime to return their organizations to necessary profitability, essential competitiveness, and offering an appropriate level of clinical access.
As noted in this blog several months ago, management guru Peter Drucker always maintained that hospitals were the hardest of all American organizations to run successfully. If Drucker were still alive, he would—without question—double down on that observation.
The question must be asked whether historical hospital leadership structures and strategies are still adequate to cope with a fast-changing healthcare industry that features a different level of financial problems, an unrecognizable workforce, and a shape-shifting patient population? This is a leadership question that requires a thoughtful and sophisticated answer.
To paraphrase Albert Einstein, we cannot solve our hospital management problems with the same level of leadership that created them.
So, we are collectively on the hunt for leadership and managerial solutions. The leadership ideas must be different, original, and challenge conventional thinking. Successful healthcare executives these days must be active readers and learners. Winning ideas are everywhere but you need to be both curious and aggressive to find them.
In that regard, let’s turn our curiosity toward the theories and teachings of Coach John Wooden. For our younger readers, John Wooden was the coach of the of the UCLA men’s basketball program from 1948 to 1975. During that time, he won 10 NCAA national championships in 12 years and at one point his teams won 88 games in a row. ESPN’s “Page 2” readers voted him the greatest coach of all time.
But John Wooden wasn’t just a basketball coach; he was a manager, an executive, a teacher, and a philosopher. There was nothing random or laissez-faire about his approach to leadership. Coach Wooden led through a series of principles that he applied with absolute consistency.
Players changed, the opposition changed, and external factors changed, but Coach Wooden’s essential approach to leadership did not vary or change.
The central tenet of Coach Wooden’s leadership philosophy was the somewhat Zen-like principle of “be quick—but don’t hurry.”
At first blush, this organizing principle doesn’t seem to make much sense, especially to the casual reader. John Wooden believed and taught that there were two keys to successful performance, both in sports and otherwise. First, quickness and a sense of urgency was absolutely necessary to winning in a competitive environment. But for Coach Wooden, quickness itself was not sufficient for consistent success. Quickness had to be accompanied by emotional and professional balance in order to achieve team and organizational excellence. So, from Coach Wooden’s perspective, a great athlete or a great executive had to not just move and think quickly, but also had to make sure that he or she was moving to a place of personal balance. Coach Wooden believed that this concept of personal balance was the key to real success at both the team and individual level. To find that place of balance you needed to be quick, but to retain that balance you had to be sure not to hurry. In other words, “be quick—but don’t hurry.”
“Be quick—but don’t hurry” was the central principle of John Wooden’s leadership style but “be quick—but don’t hurry” was also the platform on which an entire management and leadership theory was built. This led to other key Wooden tenets including:
This blog covers just a few of Coach Wooden’s many approaches to and commentaries on management and leadership. But the above observations are a useful start. It is important to disclose that this blog post was guided by and drew quotes from an excellent book, Be Quick—But Don’t Hurry: Finding Success in the Teachings of a Lifetime, which was written by Andrew Hill (a former UCLA player) with the assistance of John Wooden. The book was published by Simon & Schuster in 2001 but as readers can easily see, the book by Messrs. Hill and Wooden remains absolutely relevant today. The book is a short read but will prove to be a good use of your time and your curiosity.
Learn and be smart. Those are the key attributes for today’s healthcare executives. Yesterday’s executive techniques are no longer getting the job done. Hospital leaders must be better in order to deal with the long list of obstacles that are preventing hospital success. Coach Wooden invented a unique roadmap to executive learning and leadership. That Wooden roadmap is definitely “old school,” but that roadmap and its attendant theories and methods are absolutely worth your attention.

https://mailchi.mp/cd8b8b492027/the-weekly-gist-january-26-2024?e=d1e747d2d8
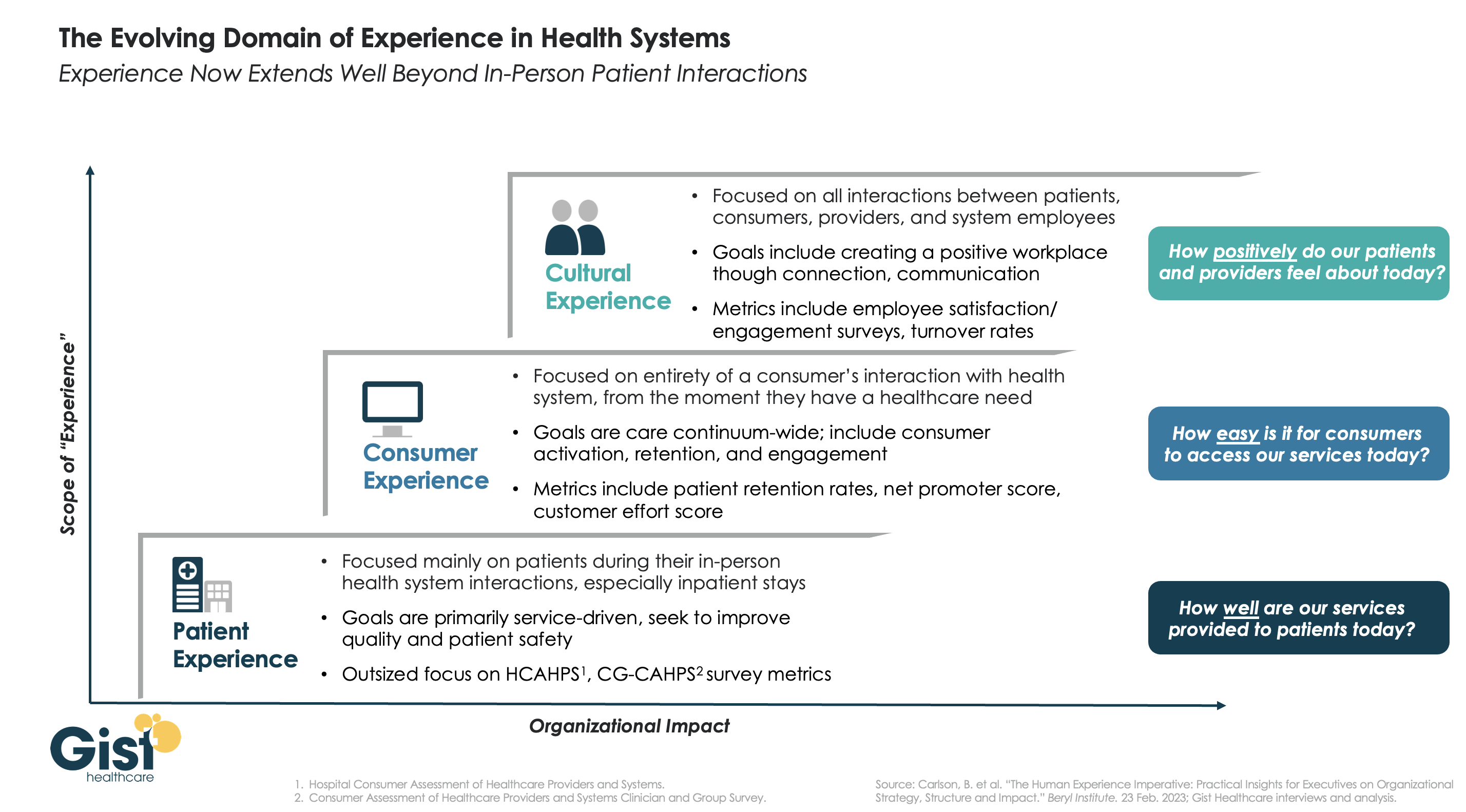
In this week’s graphic, we highlight the importance of broadening the domain of health system experience initiatives beyond patients to include consumers and even employees.
While reimbursements tied to HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) and CG-CAHPS (Clinician and Group Consumer Assessment of Healthcare Providers and Systems) scores have made patient experience a main focus for years, an increasingly consumer-driven healthcare industry means that health systems must consider the experience of all consumers in their markets, with the hopes of meeting their needs and eventually welcoming them as new—or retuning—patients.
Embracing this mindset requires focusing on the entirety of a consumer’s interactions with the health system and the tracking of non-traditional metrics that measure the strength and value of their relationship to the system. Some systems are expanding their experience purview even further by also focusing on the working conditions and morale of their providers and other staff, as a healthy workplace environment serves to better both the patient and consumer experience. Easily accessible services and positive interactions with providers and other staff can determine a consumer’s view of their experience before any care is actually delivered.
Cultural and strategic shifts that integrate experience from the top down into all operational facets of the health system will ultimately strengthen consumer loyalty, employee retention, and the financial health of the system.
