Ahead of my Congressional testimony last week before the Senate HELP committee, I compiled data on the profits, revenues and CEO compensations of big health insurers in 2024. The curiosity from senators on both sides of the aisle signaled, to me, that lawmakers are as interested as I’ve ever seen in the industry’s rampant profiteering.
What I found was that the seven biggest publicly traded health insurance companies collectively made $71.3 billion in profits, up more than half a billion dollars from 2023. All while millions of Americans continued to skip their medications, rationed insulin and delayed care due to insurers’ out-of-pocket demands.
Let’s break it down.
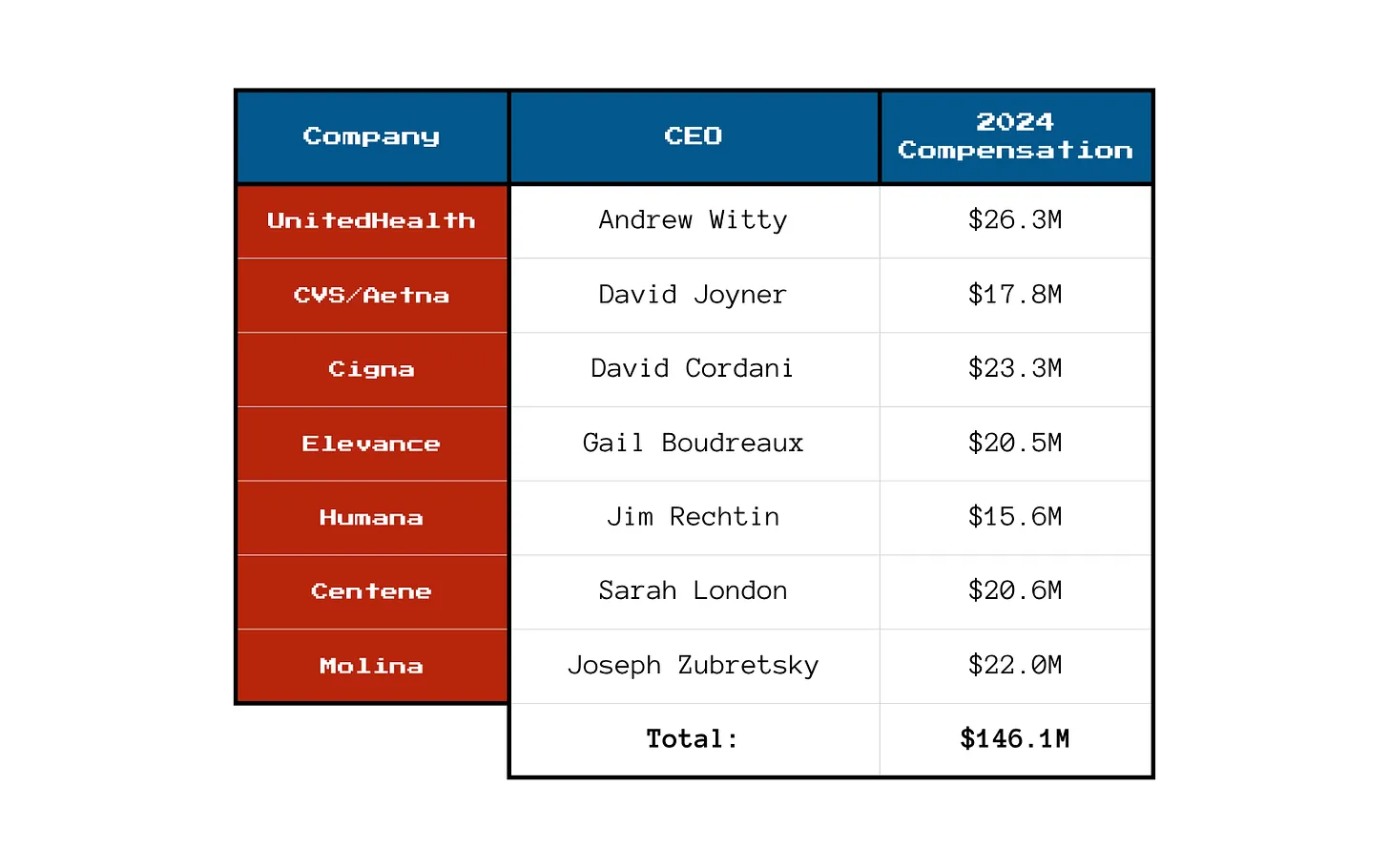
You won’t be surprised to learn that shareholders are not the only ones benefiting from the care-restricting barriers insurers have erected to boost profits. The CEOs of those seven companies took home a combined $146.1 million in 2024 compensation. That’s enough to cover annual premiums for thousands of American families.
Here’s what the top brass made:
Meanwhile, patients across the country report increasing out-of-pocket costs, more aggressive prior authorizations and narrower provider networks. But for these executives, the real measure of success is how high they can push their stock prices and not how many people can afford to see a doctor.
So, What’s Driving the Revenue Surge?
One word: Gouging.
Insurers continued to jack up premiums for their commercial customers and overcharge the government. Despite watchdog warnings, Uncle Sam continues to pour money into private Medicare Advantage plans even as audits and investigations uncover widespread fraud and upcoding. And Medicaid managed care is a gold mine, too. These insurers now dominate state Medicaid contracts and can quietly extract billions through behind-the-scenes ownership of pharmacies, PBMs and providers.
It’s not just health insurance anymore — it’s a monopolized empire.
All that said, to the dismay of shareholders, the big seven insurers have had to admit that so far in 2025, they’ve paid more medical claims than they had expected, which means their profits were down somewhat during the first months of the year. I’ll shed more light on that in a future post. No need for you to shed any tears for them, though, because we’re still talking billions and billions in profits.
So if you’re wondering why your premiums, deductibles and costs at the pharmacy counter keep going up — just look at those 2024 numbers. We all paid more for health insurance and got less for the hard-earned money we had to shovel out for our “coverage.”
And expect even more financial pain (and difficulty getting the care you need) as these companies do all they can to get their profit margins back to where Wall Street wants them.
July 2025 will be the month U.S. healthcare leaders recognize as the industry’s modern turning point. Consider…
On July 4, the One Big Beautiful Bill Act was signed into law setting in motion $960 billion in Medicaid cuts over the decade and massive uncertainty among those most adversely impacted—low income and under-served populations dependent on public programs, 8 to 11 million who used now-suspended marketplace subsidies to buy insurance coverage, and hundreds of state and local health agencies left in funding limbo.
On July 15, the Bureau of Labor Statistics reported the June Consumer Price Index rose .3% bumping the LTM to 2.7% (lower than LTM of 3.4% for medical services). Prices have edged up.
On July 31, President Trump issued an Executive Order to 17 drug companies ordering them to reduce prices on their drugs by September 29 or else. And CMS issued final rules for FY2026 Medicare payments to hospitals, rehab and other providers reflecting increases ranging from 2.5-3.3% effective October 1.
And on the same day, the Bureau of Labor issued its July 2025 jobs report that showed a disappointing net gain of 73,000 jobs plus downward revisions for May and June of 258,000 sparking Wall Street anxiety and President Trump to call the results “rigged” before firing BLS head Erika McEntarfer. Note: healthcare added 55,000 in July—the biggest of any sector and more than its 42,000 average monthly increase.
Collectively, these actions reflect rejection of the health industry by the GOP-led Congress.
It follows 15 years of support vis a vis the Affordable Care Act (2010) and pandemic recovery emergency funding (2020-2021). In that 15-year period, the bigger players got bigger in each sector, investment of private equity in each sector became more prevalent, costs increased, affordability for consumers and employers decreased, and the public’s overall satisfaction with the health system declined precipitously.
For the four major players in the system, the passage of the “big, beautiful bill” was a disappointment. Their primary concerns were not addressed:
Physicians wanted relieffrom annual payment cuts by Medicare preferring reimbursement tied directly to medical inflation. And insurer’ prior authorization and provider reimbursement was a top issue. Status: Not much has changed though adjustments are promised.
Hospitals wanted continuation of federal Medicaid funding, protection of the 340B drug purchasing program, rejection of site-neutral payment policies, higher Medicare reimbursement and relief from insurer prior authorization frustrations. Status: Medicaid funding is being cut forcing the issue for states. CMS payment increases for 2026 are lower than operating cost increases. Insurers have promised prior-auth relief but details about how and when are unknown. And Congress posture toward hospitals seems harsh: price transparency compliance, safety event reporting, and cost concerns are bipartisan issues.
Insurers wanted sustained funding for state Medicaid and Medicare Advantage programs and federal pushback against drug prices and hospital consolidation. Status: Congress appears sympathetic to enrollee complaints and anxious to address insurer “waste, fraud and abuse” including overpayments in Medicare Advantage.
Drug companies oppose “Most Favored Nation” pricing and want protections of their patents and limits on how much insurers, pharmacy benefits managers, wholesalers, online distributors and other “middlemen” earn at their expense. Status: to date, little action despite sympathetic rhetoric by lawmakers. Status: to date, Congress has taken nominal action beyond the Inflation Reduction Act (2022) though 23 states have passed legislation requiring PBMs, insurers and manufacturers to disclose drug prices and 12 states have established Prescription Drug Affordability Boards to monitor prices.
My take:
The landscape for U.S. healthcare is fundamentally changed as a result of the July actions noted above. It is compounded by public anxiety about the economy at home and global tensions abroad.
These July actions were a turning point for the industry: responding appropriately will require fresh ideas and statesmanship. Transparency about prices, costs, incentives and performance is table stakes. Leaders dedicated to the greater good will be the difference.
Imagine you’re facing your midyear performance review with your boss. You dread it, even though you’ve done all you thought possible and legal to help the company meet Wall Street’s profit expectations, because shareholders haven’t been pleased with your employer’s performance lately.
Now let’s imagine your employer is a health insurance conglomerate like, say, UnitedHealth Group. You’ve watched as the stock price has been sliding, sometimes a little and on some days crashing through lows not seen in years, like last Friday (down almost 5% in a single day, to $237.77, which is down a stunning 62% since a mid-November high of $630 and change).
You know what your boss is going to say. We all have to do more to meet the Street’s expectations. Something has changed from the days when the government and employers were overly generous, not questioning our value proposition, always willing to pick up the tab and pay many hidden tips, and we could pull our many levers to make it harder for people to get the care they need.
Despite government and media reports for years that the federal government has been overpaying Medicare Advantage plans like UnitedHealth’s – at least $84 billion this year alone – Congress has pretended not to notice. There is evidence that might be changing, with Republicans and Democrats alike making noises about cracking down on MA plans.
Employers have complained for ages about constantly rising premiums, but they’ve sucked it up, knowing they could pass much of the increase onto their workers – and make them pay thousands of dollars out of their own pockets before their coverage kicks in. Now, at least some of them are realizing they don’t have to work with the giant conglomerates anymore.
Doctors and hospitals have complained, too, about burdensome paperwork and not getting paid right and on time, but they’ve largely been ignored as the big conglomerates get bigger and are now even competing with them.
UnitedHealth is the biggest employer of doctors in the country. But doctors and hospitals are beginning to push back, too.
Since last fall, UnitedHealth and its smaller but still enormous competitors have found that “headwinds” are making it harder for them to maintain the profit margins investors demand. That is mainly because, despite the many barriers patients have to overcome to get the care they need, many of them are nevertheless using health care, often in the most expensive setting – the emergency room. They put off seeing a doctor so long because of insurers’ penny-wise-pound-foolishness that they had some kind of event that scared them enough to head straight to the ER.
It’s not just you who is dreading your midyear review. Everybody, regardless of their position on the corporate ladder, and even the poorly paid folks in customer service, are in the same boat. And so is your boss. Nobody will put the details of what has to be done in writing. They don’t have to. Your boss will remind you that you have to do your part to help the company achieve the “profitable growth” Wall Street demands, quarter after quarter after quarter. It never, ever ends. You know this because you and most other employees watch what happens after the company releases quarterly financials. You also watch your 401K balance and you see the financial consequences of a company that Wall Street isn’t happy with. And Wall Street is especially unhappy with UnitedHealth these days.
And when things are as bad as they are now at UnitedHealth’s headquarters in Minnesota, you know that a big consulting firm like McKinsey & Company has been called in, and that those suits will recommend some kind of “restructuring” and changes in leadership to get the ship back on course. You know the drill. Everybody already is subject to forced ranking, meaning that at the end of the year, some of your colleagues, regardless of job title, will fall below a line that means automatic termination. You pedal as fast as you can to stay above that line, often doing things you worry are not in the best interest of millions of people and might not even be lawful. But you know that if you have any chance of staying employed, much less getting a raise or bonus, you have to convince your superiors you are motivated and “engaged to win.” No one is safe. Look what happened to Sir Andrew Witty, whose departure as CEO to spend more time with his family (in London) was announced days after shareholders turned thumbs down on the company’s promises to return to an acceptable level of profitability.
If you are at UnitedHealth, you listened to what the once and again CEO, Stephen Hemsley, and CFO John Rex, who got shuffled to a lesser role of “advisor” to the CEO last week, laid out a new action plan to their bosses – big institutional investors who have been losing their shirts for months now. You know that what the C-Suite promised on their July 29 call will mean that you will have to “execute” to enable the company to deliver on those promises. And you know that you and your colleagues will have to inflict a lot more pain on everybody who is not a big shareholder – patients, taxpayers, employers, doctors, hospital administrators. That is your job. And you will try to do it because you have a mortgage, kids in college and maxed-out credit cards.
Here’s what Hemsley and his leadership team said, out loud in a public forum, although admittedly one that few people know about or can take an hour-and-a-half to listen to:
Even though UnitedHealth took in billions more in revenue, its margins shrank a little because it had to pay more medical claims than expected.
Still, the company made $14.3 billion in profits during the second quarter. That’s a lot but not as much as the $15.8 billion in 2Q 2024, and that made shareholders unhappy.
Enrollment in its commercial (individual and employer) plans increased just 1%, but enrollment in its Medicare Advantage plans increased nearly 8%. That’s normally just fine, but something happened that the company’s beancounters couldn’t stop.
Those seniors figured out how to get at least some care despite the company’s high barriers to care (aggressive use of prior authorization, “narrow” networks of providers, etc.)
To fix all of this, Hemsley and team promised:
To dump 600,000 or so enrollees who might need care next year
To raise premiums “in the double digits” – way above the “medical trend” that PriceWaterhouseCoopers predicts to be 8.5% (high but not double-digit high)
Boot more providers it doesn’t already own out of network
Reduce benefits
Throughout the call with investors (actually with a couple dozen Wall Street financial analysts, the only people who can ask questions), Hemsley and team went on and on about the “value-based care” the company theoretically delivers, without providing specifics. But here is what you need to know: If you are enrolled in a UnitedHealth plan of any nature – commercial, Medicare or Medicaid or VA (yes, VA, too) – expect the value of your coverage to diminish, just as it has year after year after year.
The term for this in industry jargon is “benefit buydown.”
That means that even as your premiums go up by double digits, you will soon have fewer providers to choose from, you likely will spend more out-of-pocket before your coverage kicks in, you might have to switch to a medication made by a drug company UnitedHealth will get bigger kickbacks from, and you might even be among the 600,000 policyholders who will get “purged” (another industry term) at the end of the year.
Why do we and our employers and Uncle Sam keep putting up with this?
Yes, we pay more for new cars and iPhones, but we at least can count on some improvements in gas mileage and battery life and maybe even better-placed cup holders. You can now buy a massive high-def TV for a fraction of what it cost a couple of years ago. Health insurance? Just the opposite.
As I will explain in a future post, all of the big for-profit insurers are facing those same headwinds UnitedHealth is facing. You will not be spared regardless of the name on your insurance card. If you still have one come January 1. Pain is on the way. Once again.
Not long ago, Dr. Richard Menger, a neurosurgeon, was ready to operate on a 16-year-old with complex scoliosis. A team of doctors had spent months preparing for the surgery, consulting orthopedists and cardiologists, even printing a 3D model of the teen’s spine.
The surgery was scheduled for a Friday when Menger got the news: the teen’s insurer, Blue Cross Blue Shield of Alabama, had denied coverage of the surgery.
It wasn’t particularly surprising to Menger, who has been practicing in Alabama since 2019. Alabama essentially has one private insurer, Blue Cross Blue Shield of Alabama, which has a whopping 94% of the market of large-group insurance plans, according to the health policy nonprofit KFF. That dominance allows the insurer to consistently deny claims, many doctors say, charge people more for coverage, and pay lower rates to doctors and hospitals than they would in other states.
“It makes the natural problems for insurance that much more magnified because there’s no market competition or choice,” says Menger, who in 2023 wrote an op-ed in 1819 News, a local news site, arguing that ending Blue Cross Blue Shield of Alabama’s health insurance monopoly would make people in the state healthier.
Blue Cross Blue Shield of Alabama also has the largest share of individual insurance plans in the state, according to data from the Centers for Medicaid & Medicare Services. Perhaps not coincidentally, Alabama also had the highest denial rates for in-network claims by insurers on the individual marketplace in 2023, according to a KFF analysis: 34%. Neighboring Mississippi, where the majority insurer has less of the market share at 81%, has an average denial rate of 15%.
Alabama is an extreme case, but people in many other states face health insurance monopolies, too. One insurer, Premera Blue Cross Group, has a 94% share of the large-group market in Alaska, and Blue Cross Blue Shield of Wyoming has a 91% market share in that state. In 18 states, one insurer has 75% or more of the large-group health insurance marketplace, according to KFF data.
These monopolies drive up costs, says Leemore Dafny, a professor at Harvard Business School and Harvard Kennedy School who has long studied competition among health insurance companies and providers.
“More competitors tend to drive lower premiums and more generous benefits for consumers,” she says. “There’s a lot of concern from analysts like myself about concentration in a range of sectors, including health insurance.”
Bruce A. Scott, the immediate past president of the American Medical Association, has said that when the dominant insurer in his state of Kentucky was renegotiating its contract with his medical group, it offered lower rates than it had paid six years before. “This same type of financial squeeze play is found nationwide, and its frequency has been exacerbated by health insurance industry consolidation,” he wrote in The Hill in 2023.
What happened to competition? There used to be a lot more regional health insurers, Dafny says. But as costs started to rise, they didn’t have enough leverage to negotiate prices down with providers and stay profitable. As a result, many were happy to be acquired by larger companies. Then hospitals and doctor’s offices merged to get more leverage against the bigger insurers. Now, there’s a lot of concentration among both provider groups and insurers.
“None of this had anything to do with taking better care of patients,” she says. “It had to do with trying to get the upper hand.”
In a statement to TIME, Blue Cross Blue Shield of Alabama said that it was working to make the prior authorization process more transparent and reverse the requirement of prior authorization for certain in-network medical services. It will attempt to answer at least 80% of requests for prior authorization in near real-time by 2027, it says. (A coalition of major health insurers recently vowed to fix their prior authorization processes under pressure from the federal government.)
The insurer also says it welcomes competition. “We know Alabamians have a choice when it comes to choosing their health insurance carrier and we don’t take that for granted,” a spokesperson said in the statement. In the commercial and underwritten market—which represents the bulk of its business—Blue Cross Blue Shield Alabama competes with four other companies that sell individual, family, and group plans, the company says, and it competes with 68 companies who sell Medicare plans in Alabama. Its success in the state is partly because it sells policies in every county in Alabama, the insurer says, while others do not.
Other casualties of such a concentrated health-insurance marketplace are rural hospitals and providers. Small rural hospitals are often independent and have not merged with other systems like many of their large urban counterparts, so they have an even harder time negotiating with the one big insurer in the state, says Harold Miller, president and CEO of the Center for Healthcare Quality and Payment Reform, a national policy center that studies health-care costs. That means big insurers will often refuse to cover procedures or pay lower prices for services.
“I’ve had rural hospitals tell me they can’t even get the health plan on the phone,” Miller says.
In the past decade, the Department of Justice has stopped some mergers, but has not been very aggressive at stopping consolidation in the health-care industry, Dafny says. That may be in part because the courts require a high standard of evidence to block a transaction, and the government might have been worried it would have lost whatever cases it brought.
A few factors prevent insurers with a monopoly from driving costs too high, says Benjamin Handel, an economics professor at the University of California, Berkeley who studies health care. One is a regulation called minimum loss ratio that essentially requires insurers to spend a certain share of what they earn from premiums on medical care. Another is that an insurer with a monopoly that angers consumers might attract attention from regulators, he says.
Of course, there’s not a whole lot regulators can do to make a marketplace more competitive. A state could try to incentivize more insurers to enter their states with tax breaks or other sweeteners, but it’s very hard to enter a market and offer low rates right away. The establishment of the health-care marketplaces in the Affordable Care Act allowed new entrants, Dafny says, but many of them did not survive.
Menger, the Alabama doctor, says that he and his colleagues—and therefore their patients—are basically stuck. His staff has to spend 10-15 hours a week negotiating with the insurer to get prior authorizations that sometimes don’t come, even while patients pay higher premiums.
The teenage boy eventually got approved for the scoliosis surgery, but not after the family went through a lot of stress with postponements and uncertainty. “I think it’s pretty clear that the more competition, the better things are,” Menger says. “This prior authorization nonsense is really hurting patients.”
Elevance, which owns Blue Cross plans, is now reeling from Wall Street losses thanks to its Medicare Advantage business.
The company now known as Elevance, which owns Blue Cross plans in 14 states, took a drubbing on Wall Street yesterday after executives told shareholders that it had to pay out way more in medical claims during the second quarter than expected, especially in its Medicare Advantage business. As a reminder, Wall Street hates to hear such news, so much so that investors rushed to sell their shares in the company, sending the stock price to $296.39 – a 52-week low – before closing at $302.45 yesterday afternoon. That’s down 47% from the all-time high of $567.36 it reached last September.
The news was so distressing for people who still have investments in for-profit health insurers that many of them finally bailed, getting the message that the entire sector is likely not the best place to make money these days. All seven of the companies (Centene, Cigna, CVS/Aetna, Elevance, Humana, Molina and UnitedHealth) saw big drops in their stock price with two others (Centene and Molina) also falling to 52-week lows. The companies’ stock is continuing to tank today as I write this.
When Denial Becomes a Liability
UnitedHealth has historically been the first of the companies to release quarterly earnings, but it stepped back as leader of the pack this quarter after that giant’s recent troubles on Wall Street. UnitedHealth missed financial analysts’ profit expectations last quarter and withdrew its profit guidance for the year, an unprecedented move for that company, which terrified its shareholders. UnitedHealth’s stock price has lost nearly 55% of its value since reaching a high of $630.73 last November.
Like UnitedHealth, Elevance had been a Wall Street darling until a business practice common in the health insurance game – refusing to pay for patients’ medically necessary care – finally caught up with it.
I’m talking about prior authorization, the benign sounding term that covers a number of ways a health insurer banks money by saying no to a doctor’s plea to cover a patient’s treatment or medications. The fundamental problem is that by refusing to pay for care a patient needs, that patient likely will get sicker and wind up needing even more expensive care down the road. Insurance company beancounters know that can happen, but they also know there is a decent chance that that potentially high-cost patients will not even be enrolled in one of the company’s health plans when the day finally arrives that they have to go to the hospital, which, of course, might have been avoided if the initial treatment had been approved in the first place.
We’re not just talking about a stay in the hospital. One permutation of prior auth is called step therapy in which an insurer demands that a patient try other medications on the insurer’s list of preferred drugs (its “formulary”) before approving the drug a doctor believes will work best. Sometimes it’s called “fail first.” In other words, a patient must endure pain and suffering for weeks or months taking an ineffective drug on an insurer’s formulary – the price of which the insurer has negotiated to its financial advantage with a drug maker – before the insurer will agree to cover the medication the doctor believes will be more effective. The doctor will then have to persuade the insurer that the insurer’s preferred drug failed. We’ll dive deeper into that insurer-induced nightmare in a future post, but know for now that it is a big and expensive time-suck that doctors have to endure while insurers can keep unused premium dollars in their investment accounts.
The Conversion That Changed Everything
But let’s go back to Elevance, which until recently was called Anthem and before that WellPoint. Many of its subsidiaries still use the term Anthem in its branding, like the biggest under its corporate umbrella, Anthem Blue Cross of California. All of those Blues plans operated on a nonprofit basis until a savvy executive named Leonard Schaeffer, who was CEO of Anthem of California back when it was still a nonprofit, pulled off a deal that would put him on the path to considerable fame and fortune, a first-of-its-kind “conversion” that would prove to be a major reason why the U.S. has the most complex, expensive and inefficient health care system on the planet.
According to his official bio on the website of the Leonard D. Schaffer Fellows in Government Service, which is affiliated with some of the country’s most prestigious universities, Schaeffer was recruited as CEO of Blue Cross of California in 1986 when, we are told, it was near bankruptcy. We’re also told that Schaeffer “managed the turnaround of Blue Cross of California and the IPO (initial public offering, i.e., converting it to for-profit status) creating WellPoint in 1993. During his tenure, WellPoint made 17 acquisitions and endowed four charitable foundations with assets of over $6 billion. Under Schaeffer’s leadership, WellPoint’s value grew from $11 million to over $49 billion.”
One might think from reading that last sentence that Schaeffer himself wrote big personal checks to endow those foundations, but establishing those nonprofit foundations (which includes the California Endowment, the California Health Care Foundation and the California Wellness Foundation) was demanded by California regulators as a condition of their approval of the IPO. The money was referred to as a conversion fund (converting from nonprofit to for-profit status), and it came from the proceeds of the IPO.
But Schaffer did indeed make a ton of money from the deal and WellPoint’s subsequent acquisition by a rival company that also owned recently converted Blues plans, Anthem, in 2004.
One of the organizations that opposed the WellPoint-Anthem deal, Consumer Watchdog, wrote at the time that:
Payments to WellPoint executives after the company’s buyout by Anthem Inc. could top $600 million if regulators and shareholders do not modify the acquisition terms, according to documents received from California regulators by the Foundation for Taxpayer and Consumer rights under a Public Records Act Request late Tuesday.
The documents detail potential payments in excess of those estimated by the company to shareholders at $200 million in a recent proxy. Executives will receive cash bonuses worth between $146 million and $365 million under the proposed terms of the company buyout by Anthem, in addition to over $251 million in stock options. WellPoint CEO Leonard Schaeffer has already begun exercising his stock options as of June 1st at sweetheart prices – earning him $16 million on that one day alone and increasing the size of his shares by hundreds of thousands.
When we look back at the history of health insurance in this country, we can thank this one man for the rapid shifting of Americans out of what historically had been nonprofit health insurance plans that initially were community-rated, meaning they charged everybody the same premium, regardless of gender, health status, occupation or address, and did not use gimmicks like prior authorization to boost profits. Being nonprofits, they couldn’t even book profits, although many of them did amass millions more in “reserves” than regulators required for solvency reasons.
I was working at Cigna when WellPoint joined the club of big for-profit insurers in 1993, along with Aetna, Humana (where I also previously worked), UnitedHealth, which was a relatively small player back then, and giant “multiline” insurers like MetLife, Prudential and Travelers. All of those last three decided to sell their health insurance operations to UnitedHealth and Aetna, putting those companies on the path to becoming the behemoths they are today.
And Schaeffer would wind up being one of America’s richest men, and, to his credit, he has been personally philanthropic. We know that because his name shows up all over the place in U.S. health care think-tank world. Indeed, his name is now associated far more with groups and institutions engaged in public policy than the “platinum parachute,” to use Consumer Watchdog’s term, he got when he and a few colleagues engineered the sale of WellPoint to Anthem. As his bio notes:
In 2009, Schaeffer established the Schaeffer Center for Health Policy and Economics at the University of Southern California, which emphasizes the interdisciplinary approach to research and analysis to support evidence-based health policy. In 2015, he established the Schaeffer Fellows in Government Service program which has supported 418 undergraduates to date in high-level, summer government internships. In 2004, he established the Schaeffer Institute for Public Policy & Government Service. He has also endowed chairs in health care financing and policy at the Brookings Institution, Harvard Medical School, the National Academy of Medicine, UC Berkeley and USC.
If Schaeffer still owns shares in Elevance, he is a bit poorer today than he was yesterday morning, but he’s probably still doing OK. Shares of Elevance’s stock have increased 1731% in value since they started trading on the New York Stock Exchange in October 2001, even with the company’s very bad Thursday on the Street.
I’ve been at thisfor so long and have seen so much. And it’s hard to overstate how significant the latest revelations from The Wall Street Journal are. According to its reporting, the U.S. Department of Justice’s criminal health care-fraud unit is questioning former UnitedHealth Group employees about the company’s Medicare billing practices regarding how the company records diagnoses that trigger higher payments from taxpayers.
For years, independent policy experts and *some* regulators have warned that the private Medicare Advantage program has become a breeding ground for upcoding and tax dollar waste. The tactic being scrutinized by the DOJ is called “upcoding.” Essentially, Medicare Advantage companies have an incentive to “find” new illnesses — even among patients who might not need additional treatment because the more serious the diagnoses, the bigger the government payouts to the company.
According to the Journal, prosecutors, FBI agents, and the Health and Human Services Inspector General have been asking ex-employees about special training for doctors, software that flags profitable conditions, and even bonuses for physicians who recode patient files. One former UnitedHealth doctor told the Journal that prosecutors inquired about pressure to use certain diagnosis codes and bonus pay for certain health care decisions that financially favored UnitedHealth.
The Journal’s data shows that UnitedHealth’s members received certain lucrative diagnoses at higher rates than patients in other Medicare Advantage plans — billions of extra dollars that ultimately come from taxpayers. In one example, they reportedly pulled in about $2,700 more taxpayer dollars per patient visit when nurses went into seniors’ homes to hunt for additional conditions.
In a statement, UnitedHealth insists they “remain focused on what matters most: delivering better outcomes, more benefits, and lower costs for the people we serve.”
This latest criminal investigation joins at least two other DOJ probes into UnitedHealth’s billing and potential antitrust violations. And it’s yet another reminder that the Medicare Advantage program — which, much to many advocates alarm, now covers more than half of all Medicare enrollees – is desperately in need of real oversight.
If there’s any silver lining, it’s that courageous former employees are speaking up. They know what I know: This “profit-maximizing” through “upcoding” and “favorable selection” drains billions that could be better spent on actual patient care and pad Wall Street profits.
Administrative waste, denials, and deadly incentives — the U.S. model shows what happens when profit rules.
The United States is the only country where a health insurance executive has been gunned down in the street. But that’s not the only thing that’s unique about American health insurance.
Almost all of our peer countries – advanced, free-market democracies — have health insurance companies. In some cases (Germany, Switzerland, Japan), private health insurance is the chief way to pay for medical care. In others (such as Great Britain), private insurance works as a supplement to government-run health care systems. But there’s a fundamental difference between health insurance elsewhere and the U.S. system.
In all the other advanced democracies, basic health insurance is not for profit; the insurers are essentially charities. They exist not to pay large sums to executives and investors, but rather to keep the population healthy by assuring that everyone can get medical care when it’s needed.
America’s health insurance giants are profit-making businesses. Indeed, in the insurers’ quarterly earnings reports to investors, the standard industry term for any sums spent paying people’s medical bills is “medical loss.” They view paying your doctor bill as a loss that subtracts from the dividends they owe their stockholders.
When I studied health care systems around the world, I asked economists and doctors and health ministers why they want health insurance to be a nonprofit endeavor. Everyone gave essentially the same answer:
There’s a fundamental contradiction between insuring a nation’s health and making a profit on health insurance.
Health insurance exists to help people get the preventive care and treatment they need by paying their medical bills. But the way to make a profit on health insurance is to avoid paying medical bills. Accordingly, the U.S. insurance giants have devised ingenious methods for evading payment — schemes like high deductibles, narrow networks of approved doctors, limited lists of permitted drugs, and pre-authorization requirements, so that the insurance adjuster, not your doctor, determines what treatment you get.
Other countries don’t allow those gimmicks. In America, the patient pays twice — first the insurance premium, and then the bill that the insurer declines to pay. That’s why Americans hate health insurance companies — as reflected in the tasteless barrage of angry social media commentary aimed at the victim, not the perpetrator, of the sidewalk shooting in 2024 of UnitedHealthcare’s CEO Brian Thompson in New York City.
Another unique aspect of U.S.-style health insurance is the huge amount of money our big insurers waste on administrative costs. Any insurance plan has administrative expenses; you’ve got to collect the premiums, review the patients’ claims, and get the payments out to doctors and hospitals.
In other countries, the administrative costs are limited to about 5% of premium income; that is, insurers use 95% of all the money they take in to pay medical bills. But the U.S. insurance giants routinely report administrative costs in the range of 15% to 20%.
When the first drafts of the Affordable Care Act (“Obamacare”) were floated on Capitol Hill in 2009, the statutory language called for limiting insurers’ admin costs to 12% of premium income. Then the insurance lobby went to work. The final text of that law allows them to spend up to 20% of their income on salaries, marketing, dividends, and other stuff that doesn’t pay anybody’s hospital bill.
There is one American insurance system, however, that is as thrifty as foreign health insurance plans. Medicare, the federal government’s insurance program for seniors and the disabled, reports administrative costs in the range of 3% — about one-fifth as much as the big private insurers fritter away. And Medicare’s administrators — federal bureaucrats — are paid less than a tenth as much as the executives running the far less efficient private insurance firms.
Americans generally believe that the profit-driven private sector is more efficient and innovative than government. In many cases, that’s true. I wouldn’t want some government agency designing my cell phone or my hiking boots.
But when it comes to health insurance, all the evidence shows that nonprofit and government-run plans provide better coverage at lower cost than the private plans from America’s health insurance giants.
If we were to make basic health insurance a nonprofit endeavor, as it is everywhere else, or put everybody on a public plan like Medicare, the U.S. would save billions and improve our access to life-saving care. Then Americans might stop celebrating on social media when an insurance executive is killed.
The “Big Beautiful Budget Bill” appears headed for passage with cuts to Medicaid and potentially Medicare likely elements.
The economy is slowing, with a mild recession a possibility as consumer confidence drops, the housing market slows and uncertainty about tariffs mounts.
And partisan brinksmanship in state and federal politics has made political hostages of public and rural health safety net programs as demand increases for their services.
Last Wednesday, amidst mounting anxiety about the aftermath of U.S. bunker-bombing in Iran and escalating conflicts in Gaza and Ukraine, the Centers for Medicare and Medicaid Services (CMS) released its report on healthcare spending in 2024 and forecast for 2025-2033:
“National health expenditures are projected to have grown 8.2% in 2024 and to increase 7.1% in 2025, reflecting continued strong growth in the use of health care services and goods.
During the period 2026–27, health spending growth is expected to average 5.6%, partly because of a decrease in the share of the population with health insurance (related to the expiration of temporarily enhanced Marketplace premium tax credits in the Inflation Reduction Act of 2022) and partly because of an anticipated slowdown in utilization growth from recent highs. Each year for the full 2024–33 projection period, national health care expenditure growth (averaging 5.8%) is expected to outpace that for the gross domestic product (GDP; averaging 4.3%) and to result in a health share of GDP that reaches 20.3% by 2033 (up from 17.6% in 2023) …
Although the projections presented here reflect current law, future legislative and regulatory health policy changes could have a significant impact on the projections of health insurance coverage, health spending trends, and related cost-sharing requirements, and they thus could ultimately affect the health share of GDP by 2033.”
As has been the case for 20 years, spending for healthcare grew faster than the overall economy in 2024. And it is forecast to continue through 2033:
2024Baseline
2033Forecast
% Nominal Chg.2024-2033
National Health Spending
$5,263B
$8,585B
+63.1%
US Population
337,2M
354.8M
+5.2%
Per capita personal health spending
$13,227
$20,559
+55.7%
Per capita disposable personal income
$21,626
$31,486
+45.6%
NHE as % of US GDP
18.0%
20.3%
+12.8%
In its defense, industry insiders call attention to the uniqueness of the business of healthcare:
‘Healthcare is a fundamental need: the health system serves everyone.’
‘Our aging population, chronic disease prevalence and socioeconomic disparities are drive increased demand for the system’s products and services.’
‘The public expects cutting edge technologies, modern facilities, effective medications and the best caregivers and they’re expensive.’
‘Burdensome regulatory compliance costs contribute to unnecessary spending and costs.’
And they’re right.
Critics argue the U.S. health system is the world’s most expensive but its results (outcomes) don’t justify its costs. They acknowledge the complexity of the industry but believe “waste, fraud and abuse” are pervasive flaws routinely ignored. And they remind lawmakers that the health economy is profitable to most of its corporate players (investor-owned and not-for-profits) and its executive handsomely compensated.
Healthcare has been hit by a perfect storm at a time when a majority of the public associates it more with corporatization and consolidation than caring. This coalition includes Gen Z adults who can’t afford housing, small employers who’ve cut employee coverage due to costs and large, self-insured employers who trying to navigate around the 10-20% employee health cost increase this year, state and local governments grappling with health costs for their public programs and many more. They’re tired of excuses and think the health system takes advantage of them.
As a percentage of the nation’s GDP and household discretionary spending, healthcare will continue to be disproportionately higher and increasingly concerning. Spending will grow faster than other industries until lawmakers impose price controls and other mechanisms like at least 8 states have begun already.
Most insiders are taking cover and waiting ‘til the storm passes. Some are content to cry foul and blame others. Others will emerge with new vision and purpose centered on reality.
Storm damage is rarely predictable but always consequential. It cannot be ignored. The Perfect has Hit U.S. healthcare. Its impact is not yet known but is certain to be a game changer.
“We urge the Administration to consider the timing of these policies in the context of the broader scope of requirements and challenges facing the industry that require significant system changes.”
AHIP, March 13, 2023 (in a letter to CMS Administrator Chiquita Brooks-LaSure responding to CMS’s proposed rule on Advancing Interoperability and Improving Prior Authorization Processes, proposed Final Rule, CMS-0057-P)
“Health insurance plans today announced a series of commitments to streamline, simplify and reduce prior authorization – a critical safeguard to ensure their members’ care is safe, effective, evidence-based and affordable.”
After lobbying aggressively to delay implementation of the PA reforms proposed by the previous administration (successfully delayed one year and counting), AHIP, the big PR and lobbying group for health insurers, now claims the mantle of reformer, announcing a set of voluntary commitments to streamline prior authorization.
So naturally, the industry’s “commitments” deserve closer scrutiny. Let’s unpack them. As a former health insurance industry executive, I speak their language, so allow me to translate. AHIP, which has no enforcement power, by the way, claims that 48 large insurers will:
Develop and implement standards for electronic prior authorization using Fast Healthcare Interoperability Resources Application Programming Interfaces (FHIR APIs).Translation:CMS is already requiring all insurers to do this by 2027. We might as well take credit preemptively.
Reduce the volume of in-network medical authorizations. Translation:We already demand hundreds of millions of unnecessary prior authorizations for thousands of procedures and services, so cutting a few (who knows how many?) should be a layup and won’t cut into profits.
Enhance continuity of care when patients change health plans by honoring a PA decision for a 90-day transition period starting in 2026.Translation:We’re already required to do this in Medicare Advantage. And since we delayed implementation of e-authorization until 2027, we’re in the clear until then anyway.
Improve communications by providing members with clear explanations for authorization determinations and support for appeals. Translation:We’re already required by state and federal law to do this. We’ll double-check our materials.
Ensure 80% of prior authorizations are processed in real time and expand new API standards to all lines of business. Translation:We had to promise to hold ourselves accountable to at least one measurable goal. We will set the denominator – we’ll decide which procedures and medications require PA – so we’ll hit this goal, no problem, and we might even use more non-human AI algorithms to do it.
6. Ensuring medical review of non-approved requests. Translation:People will be relieved we’re not using robots. And we’ll avoid having Congress insist that reviews must be done by a same-specialty physician, as proposed in the Reducing Medically Unnecessary Delays in Care Act of 2025 (H.R. 2433).
Of course, I wasn’t in the room when AHIP drafted these commitments, so take my translations with a grain of salt. But let’s be honest: These promises are thin on specifics, short on accountability, and devoid of measurable impact.
It’s also rich coming from an industry still reliant on something called the X12 transaction standard – technology that is now over 40 years old – to process prior authorization requests, while simultaneously pointing the finger at providers for outdated technology and being slow to adopt modern systems. Many insurers did not start accepting electronic submissions of prior authorization until roughly 2019, nearly 20 years after clinicians started using online portals such as MyChart in their regular practice. The claim that providers are the ones behind on technology is another ploy by insurers to dodge scrutiny for their schemes.
We shouldn’t settle for incremental fixes when the system itself is the problem. Nor should we allow the industry that created this problem – and perpetuates it in its own self-interest – to dictate the pace or terms of reforming it.
As we argued in our recent piece, Congress should act to significantly curtail the use of prior authorization, limiting it to a narrow, evidence-based set of high-risk use cases. Insurers should also be required to rapidly adopt smarter, lower-friction cost-control methods, like gold-carding trusted clinicians (if it can be implemented with integrity and fairness), without compromising patient access or clinical autonomy.
Letting the fox design the hen house’s security perimeter won’t protect the hens. It’s time for Congress to build a better fence.
Nearly 12 million people would lose their health insurance under President Trump’s “big, beautiful bill,” an erosion of the social safety net that would lead to more unmanaged chronic illnesses, higher medical debt and overcrowding of hospital emergency departments.
Why it matters:
The changes in the Senate version of the bill could wipe out most of the health coverage gains made under the Affordable Care Act and slash state support for Medicaid and SNAP.
“We are going back to a place of a lot of uncompensated care and a lot of patchwork systems for people to get care,” said Ellen Montz, a managing director at Manatt Health who oversaw the ACA federal marketplace during the Biden administration.
The big picture:
The stakes are huge for low-income and working-class Americans who depend on Medicaid and subsidized ACA coverage.
Without health coverage, more people with diabetes, heart disease, asthma and other chronic conditions will likely go without checkups and medication to keep their ailments in check.
Those who try to keep up with care after losing insurance will pay more out of pocket, driving up medical debt and increasing the risk of eviction, food insecurity and depleted savings.
Uninsured patients have worse cancer survival outcomes and are less likely to get prenatal care. Medicaid also is a major payer of behavioral health counseling and crisis intervention.
Much of the coverage losses from the bill will come from new Medicaid work reporting requirements, congressional scorekeepers predict. Work rules generally will have to be implemented for coverage starting in 2027, but could be earlier or later depending on the state.
Past experiments with Medicaid work rules show that many eligible people fall through the cracks verifying they’ve met the requirements or navigating new state bureaucracies.
Often, people don’t find out they’ve lost coverage until they try to fill a prescription or see their doctor. States typically provide written notices, but contacts can be out of date.
Nearly 1 in 3 adults who were disenrolled from Medicaid after the COVID pandemic found out they no longer had health insurance only when they tried to access care, per a KFF survey.
Zoom out:
The Medicaid and ACA changes will also affect people who keep their coverage.
The anticipated drop-off in preventive care means the uninsured will be more likely to go to the emergency room when they get sick. That could further crowd already bursting ERs, resulting in even longer wait times.
Changes to ACA markets in the bill, along with the impending expiration of enhanced premium subsidies, may drive healthier people to drop out, Montz said, skewing the risk pool and driving up premiums for remaining enrollees.
States will likely have to make further cuts to their safety-net programs if the bill passes in order to keep state budgets functioning with less federal Medicaid funding.
The other side:
The White House and GOP proponents of the bill say the health care changes will fight fraud, waste and abuse, and argue that coverage loss projections are overblown.
Conservative health care thinkers also posit that there isn’t strong enough evidence that public health insurance improves health.
Reality check:
Not all insurance is created equally, and many people with health coverage still struggle to access care. But the bill’s impact would take the focus off ways to improve the health system, Montz said.
“This is taking us catastrophically backward, where we don’t get to think about the things that we should be thinking about how to best keep people healthy,” she said.
The bottom line:
The changes will unfold against a backdrop of Health Secretary Robert F. Kennedy Jr.’s purported focus on preventive care and ending chronic illness in the U.S.
But American health care is an insurance-based system, said Manatt Health’s Patricia Boozang. Coverage is what unlocks access.
Scrapping millions of people’s health coverage “seems inconsistent with the goal of making America healthier,” she said.