With the election looming and the beginning of annual open enrollment periods for health insurance plans, it is vital to pull back the curtain on the influx of money from Big Insurance corporations to political campaigns and lobbying.
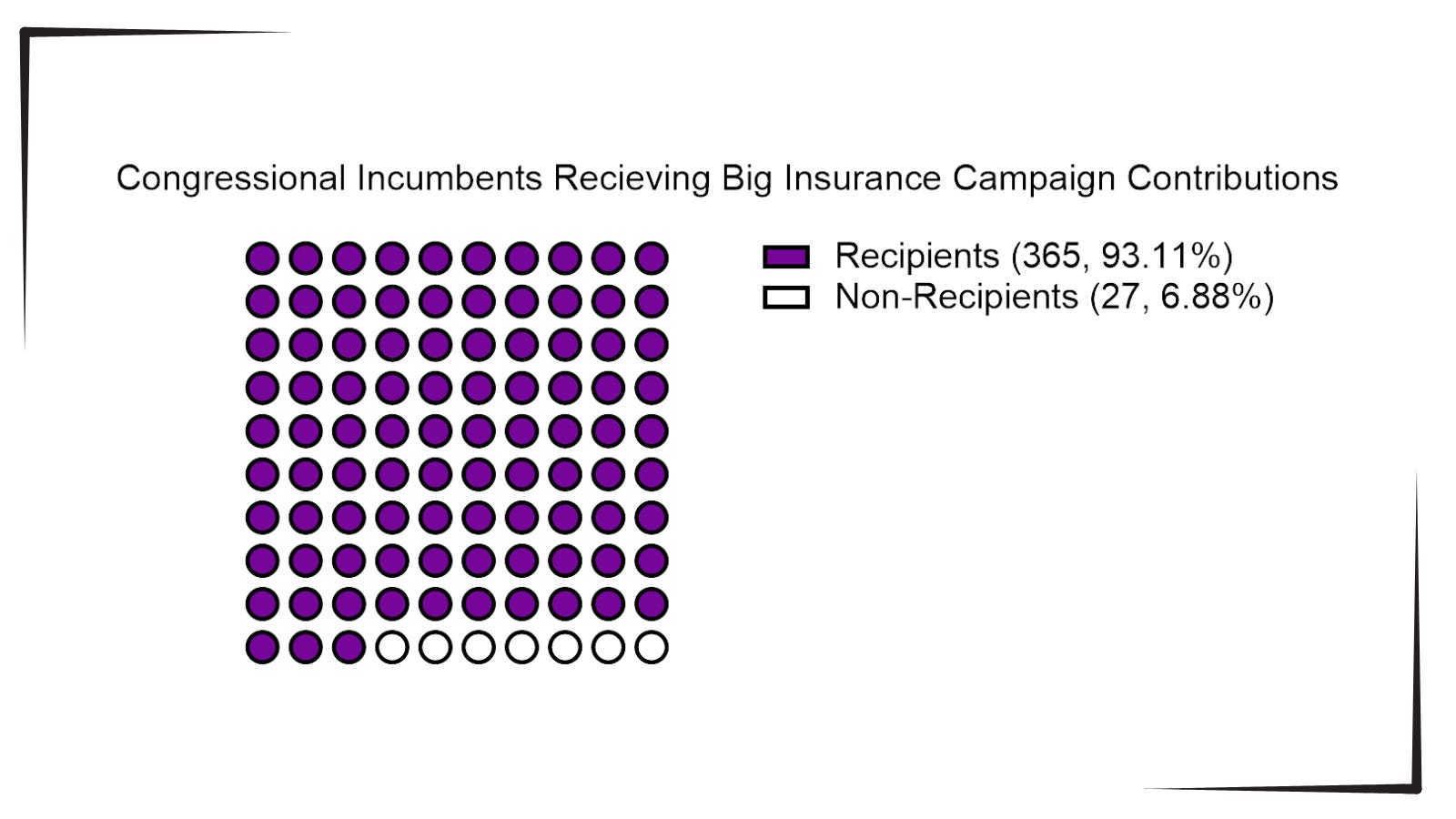
Data available from OpenSecrets.com thus far in 2024 shows that 93% of Congressional incumbents running in 2024 received contributions from Big Insurance, including 100% of Senate incumbents. These insurance corporations run the ten largest Medicare Advantage plans in the country and are known to deny needed health care and defraud the government, but face little to no consequences.
Insurance corporations included in this analysis are UnitedHealth Group, Humana, CVS/Aetna, Kaiser Permanente, Elevance Health, Centene Corp, Cigna, Blue Cross Blue Shield Association (which represents many MA plans, including two of the largest: BCBSMichigan and Highmark), and SCAN.
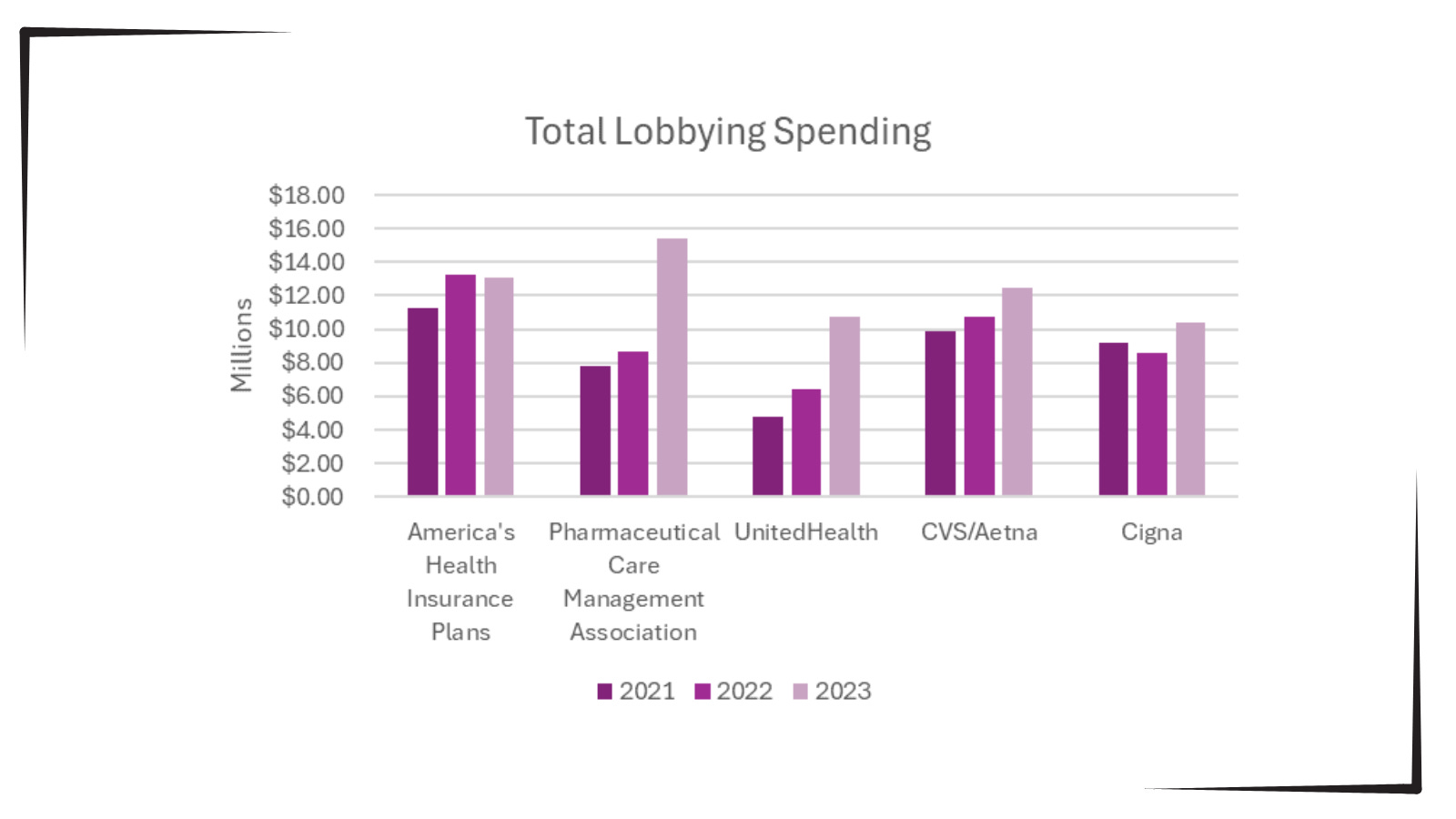
Additionally, as bipartisan scrutiny of pharmacy benefit managers (PBMs) and Medicare Advantage plans has intensified, spending by Big Insurance on lobbying has increased.
Total lobbying spending by America’s Health Insurance Plans; Pharmaceutical Care Management Association; UnitedHealth; CVS/Aetna; and Cigna for the years 2021, 2022 and 2023.
This open enrollment season, people struggling to choose a health insurance plan that they can afford and that provides the care they need may ask themselves, “Why is our health care system like this?” The immense amounts of money Big Insurance spends to blanket members of Congress with contributions and lobbying hold the answer.
Additional analysis following the election will allow evaluation of just how much Big Insurance spends on politics to help protect industry profits and will give health reform advocates an idea of how to overcome this influence to pass policies for patients, not profits.
Innovation in the American economy over the past 30 years has been nothing short of stunning—one remarkable technological advance after another. Industry by industry and product by product, corporate innovation has profoundly changed the way we navigate our economic and consumer lives. From this context of technological and innovative change came the corporate belief that healthcare could be “significantly improved” through the same application of aggressive corporate strategy and innovation.
So along came Walmart, Walgreens, CVS, and Amazon with all the resources in the world and with the best intentions to contemporize primary care.
The goals of all this were front and center: change the definition of the healthcare gatekeeper, lower costs, improve quality, and create a much more consumer-friendly care experience. Yet here we see that American business has proven—once again—that the best intentions, the smartest ideas, and a lot of money are still no guarantee of commercial success. How quickly the corporate retail re-invention of primary care all came apart.
Between 2017 and 2022, retail clinic claims grew 200%, spiking particularly during the pandemic, according to Healthcare Finance. And yet now, Walmart has abandoned its primary care strategy, Walgreens is pulling back significantly—even after announcing significant expansion plans as little as a year ago—and CVS is facing uncertainty after a leadership shakeup.
Under corporate leadership and strategy, primary care has become a catalog of woes. Let’s unpack that catalog.
Walmart opened its first health center in 2019, offering a range of basic services with prices posted. At first, it focused on patients who could pay cash, but eventually evolved to accept a range of insurance plans. Walmart brought a level of strategic aggression to its primary care initiative by announcing in 2023 it would nearly double the number of clinics it operated. But in an abrupt about face, the megaretailer shuttered all 51 primary care locations in April, citing an unsustainable business model with an inability to maximize revenue and adequately control expenses.
Walgreens, on the other hand, opted to invest in existing providers. In 2020 and 2021, Walgreens spent $6.2 billion on the primary care clinic chain VillageMD, establishing it as the majority owner. In 2022, Walgreens sunk another $3.5 billion, through a mix of debt and equity, into VillageMD’s $8.9 billion acquisition of Summit Health. Walgreens, like Walmart, suffered for its primary care investments. The company was forced to take a $5.8 billion write-down on Village MD in the second quarter of this year.
During an October 15 earnings call, Walgreens CEO Tim Wentworth said the company “is reorienting to its legacy strength as a retail pharmacy-led company,” according to the Wall Street Journal. “We are in the early stages of a turnaround that will take time.” And that comment came with the potential closure of 1,200 Walgreens retail locations, following on the heels of 160 primary care clinic closures earlier this year.
CVS, too, has not been immune to primary care turbulence, as CVS Health CEO Karen Lynch was forced to step down last month after presiding over an expansion of healthcare clinics but then closing dozens of them in California and New England. CVS’s strategic approach revolved around its $10.6 billion acquisition of Oak Street Health in 2023 and its intention to expand primary care in 1,100 MinuteClinics. That strategy now seems to be up in the air with the departure of Ms. Lynch. The CVS board is now suggesting an approach that may involve a spinoff of its insurance and pharmacy benefits manager units, Aetna and Caremark.
Amazon, however, at the moment shows no signs of abandoning its foray into primary care. Rather than focusing its efforts on solely brick-and-mortar locations, Amazon organized its primary care strategy around the 2023 $3.9 billion acquisition of One Medical, a concierge-style service designed to facilitate both in-person and virtual visits. While Amazon’s primary care strategy remains somewhat opaque, it seems to revolve around partnering with employers and health systems to cultivate primary care patient loyalty through a membership program that builds on the Amazon Prime brand.
Each company took a slightly different approach to primary care, but all four planned to leverage their exceptional size to achieve profitability.
Interestingly, scale has not been sufficient to solve the challenges of primary care. American Medical Association President Bruce A. Scott wrote recently: “If retail giants can’t make today’s care delivery model work financially, how on earth can physicians in private practice?” It’s no wonder the ongoing shortage of about 20,000 primary care physicians is expected to persist. A recent AAMC report found that by 2036, that number could double.
Primary care has been unsuccessful as a transactional business; retailers sell goods at a set price and send customers on their way. In healthcare, payment models are nowhere near as straightforward. Patients, particularly in areas where access to care is limited, may have continuous, rather than episodic, needs. All of this complexity has seemed to add up to higher costs and lower margins. Primary care seems to require a much more complex business model, one robust enough to remain patient as that business model experiments with various approaches or is vast enough to offset losses with other lines of revenue.
So where does all of the above lead us? Are there any useful conclusions or lessons to be learned? Maybe so.
Primary care is an essential component of any hospital system of care. Done right, it acts as both an important gatekeeper and as a trusting component of the continuity of healthcare service.
At the moment, there is not enough primary care to meet the demand. Stories abound of patients whose longtime primary care physicians retire and said physicians cannot be replaced without a great effort—or often not at all.
Right now, the economics of primary care don’t work as a standalone service. Many have tried and—regardless of whether they were big or small, for profit or not-for-profit—this essential patient-centered service can only operate when subsidized by a larger enterprise. Walmart, Walgreens, and CVS have all tired of those subsidies.
The overall healthcare system and its quality of care and delivery is significantly damaged by the current state of primary care. Too many patients receive delayed diagnosis and treatment and slow or little necessary follow-up. Patients that should be seen in the office are instead funneled to the emergency room. Care, of course, remains well-intentioned but often is instead inconsistent and chaotic. Conditions that might have been deftly managed instead become chronic.
All this leads to the importance of not giving up on primary care. Patients prefer to be seen in the primary care ecosystem. They tend to trust that level of care and attention. Patients also prefer to be seen in-person when they are feeling particularly poorly, and they appreciate prompt answers about concerning health issues. What this all suggests is that we are at a moment when hospitals need to double down on the primary care dilemma. Primary care needs to be examined as an essential component of the overall enterprise-wide strategic plan both clinically and—especially—financially.
Corporate America, with all of its economic power and resources and scale, has found primary care to be a confounding and, so far, unsuccessful business model. So, after all of the recent noise and promises and slide decks, the problem and promise of primary care is back in the mission-driven hands of America’s not-for-profit hospitals—exactly where it should have been all along.
While speculation swirls around key cabinet appointments in the incoming Trump administration, much is being written about how things might change for industries and the companies that compose them. Healthcare is no exception.
Speculation about possible changes originates from media coverage, healthcare trade associations, law firms, consultancies, think tanks and academics. Their views are primarily based on Trump Healthcare 1.0 initiatives (2017-2021), presumed Trump 2.0 leverage in the U.S. Senate, House and conservative Supreme Court and a belief by the Trump-team leaders that their mandate is to lower costs for “everyday Americans” and tighten border security.
Thus, Trump Healthcare 2.0 policy changes will be extensive, leveraging legislation, executive orders, agency administrative actions, court decisions and appropriations processes to reset the U.S. health system.
Context:
The red shift that enabled the 45th President to regain the White House was fueled by discontent and fear: discontent with prices paid by ordinary consumers and fear that illegal immigration was an existential threat. Abortion was an important concern to women but inflation and prices for gas, groceries, housing and healthcare mattered more. Exit polls indicate voter concern about how Trump 2.0 economic policies (tariffs et al) might inflate consumer prices or add up to $7 trillion to the national debt was low. And the fate of the Affordable Care Act was a non-issue: assurance about protection for pre-existing condition coverage neutered attention to other elements of the ACA that will get attention in Trump Healthcare 2.0 (i.e. subsidies, short-term plans, et al).
The Four Pillars of Trump Healthcare 2.0 Policy Changes
The new administration is inclined toward a transactional view of the U.S. health system. It does not envision transformational change; instead, it sees opportunity for the system to perform significantly better. Its policies, leadership appointments and actions will be predicated on these four pillars:
Access to the U.S. healthcare system is a right to be earned. Fundamentally, Trump Healthcare 2.0 builds on its moral conviction that there should be NO FREE LUNCHES whether it’s illegal immigrants or patients who use the health system without doing their part. Trump Healthcare 2.0 will advance mechanisms to enable self-care, increase personal responsibility, promote cheaper/better alternatives to traditional insurance and health delivery and challenge lawmakers to limit financial support to free-loaders. The fundamental notions of public health and community benefit will be revisited and restrictions enacted.
The status quo is not working. Change is needed. Polls show the majority of Americans are dissatisfied with the health system. Affordability is their major concern: escalating, inexplicable costs are forcing their employers to share more responsibility. Trump Healthcare 2.0 will implement changes that lower spending and costs for consumers and employers. They’ll leverage coalitions of working-class voters and businesses to enact policies that expose waste, fraud and abuse in the system and direct the U.S. Department of Health & Human Services to streamline its structure and prioritize cost-effectiveness (the HHS Strategic Plan for 2022-2026 is up for review).
Private solutions solve public problems better than government. Trump Healthcare 2.0 posits that government is broken including the federal and state agencies that control healthcare oversight and funding. Reducing regulatory barriers to consolidation and innovation and lessening risks for private investors whose ventures align with Trump Healthcare 2.0 priorities will be foci. Fundamentally, Trump Healthcare 2.0 believes the private sector is better able to address problems than government bureaucrats: key Trump Healthcare 2.0 leadership positions will be filled by successful private sector operators instead of re-cycled DC luminaries desiring attention.
Price transparency fuels competition and value. Trump Healthcare 1.0 mandated hospital price transparency via its 2019 Executive Order: Trump Healthcare 2.0 will expand the scope and usefulness of price transparency mandates in hospital, ancillary and outpatient services, physician services, insurance and others. It will facilitate accelerated use of Artificial Intelligence in decision-making by consumers, providers and payers. It will expand timely access to data on prices, direct costs, overhead, executive compensation, outcomes, user experiences and other elements of care management provided by hospitals, physicians and other providers. And it will move quickly to implement site neutral payments in the 119th Trump Healthcare 2.0 holds that providers, insurers and drug companies are not inclined to transparency despite strong support from elected officials and voters. They’ll advance these policy changes anticipating pushback from industry insiders. Trump Healthcare 2.0 believes price transparency in healthcare will produce transformational changes that enable more competition and lower costs.
Looking ahead:
The Trump 2.0 team’s immediate task is to assemble its Cabinet: that’s taken prior administrations 38 days on average to complete. In tandem, temporary fixes for CMS’ pending Physician Pay Cut and telehealth expansion will pass as Congress’ lame duck session begins this week.
Looking to 2025, the Trump Healthcare 2.0 team will focus initially on issues in Congress where Bipartisan support appears strong i.e. regulation of PBMs, implementation of site neutral payment policies, expansion of drugs subject to Inflation Reduction Act’s pricing limits and perhaps others. It will plan its legislative agenda coordinating with key committees (i.e. Senate HELP, House Ways and Means et al) and outside groups that share its predisposition. And it will use its political clout to build popular support for healthcare reforms that respond directly to consumer (voter) concern about affordability.
Trump Healthcare 2.0 will bring heightened transparency to the health system and be premised on pillars that are popular with working class voters. It will not be a duplicate of Trump Healthcare 1.0: it will be much more.
Congressional Republicans are beginning to discuss overhauling Medicaid using a process that would allow the Senate to bypass the required 60-vote threshold to pass certain priorities, according to GOP lawmakers.
Why it matters:
The changes could significantly reshape a safety net program that covers more than 70 million people, reducing federal spending and potentially leading to significant coverage losses.
Driving the news:
Perhaps the most likely Medicaid change would be imposing work requirements for recipients, according to GOP sources.
That idea was discussed as part of last year’s debt ceiling talks and is familiar to GOP lawmakers.
House Majority Leader Steve Scalise (R-La.) told Axios that Medicaid work requirements “potentially” could be included in a legislative package brought up under the fast-track budget procedure known as reconciliation.
Asked about other Medicaid spending changes, Scalise said members “have a lot of internal conversations to have about all the things that will be included.”
Yes, but:
It’s not clear how much, if any, health policy will be packed into a reconciliation bill, since the overriding focus of the package would be on extending major provisions of the Trump 2017 tax law.
There has been less recent enthusiasm for controversial health policy changes among Republicans, who’d prefer to focus on taxes, energy and immigration.
However, a health package could generate valuable savings to help pay for some of the tax cuts, and Medicaid is a large pot of money, costing over $800 billion per year.
Congressional scorekeepers previously estimated work requirements would save over $100 billion over 10 years — and 600,000 people would become uninsured.
What they’re saying:
Rep. Brett Guthrie (R-Ky.), one of two leading contenders to be chair of the House Energy and Commerce Committee in the next Congress, told Axios he is interested in capping Medicaid spending on each enrollee, known as a “per capita cap” or allotment.
This would be a revival of a proposal from the 2017 Affordable Care Act repeal-replace plan.
“We offered Medicaid reform in reconciliation in the repeal-and-replace package, and it was per capita allotments, which didn’t cut Medicaid but it does limit the growth,” Guthrie said.
“I do think it has to be discussed as part of the package” next year, he said, adding he hadn’t discussed the idea with leadership yet.
Between the lines:
Another potential change is reducing the federal share of spending on the Medicaid expansion population, currently at 90%, so that it matches the lower federal share for the traditional Medicaid population.
“It makes no sense for federal policy to pay states more for able-bodied enrollees than for disabled people, children and pregnant women on the program,” said Brian Blase, president of the Paragon Health Institute and a former Trump administration health official.
The flip side is that a cash crunch in the states could lead some to drop the Medicaid expansion altogether. Forty states have expanded their programs.
The big picture:
The first Trump administration approved Medicaid waivers for conservative-led states that imposed work and reporting requirements. But courts struck down many of the approvals.
Republicans could be wary of political blowback from efforts to reshape the entitlement program this time around.
Protests against Medicaid cuts, as well as possible resistance from some Republican governors, helped doom the repeal-replace effort in 2017.
Democrats also are sure to portray any Medicaid cuts as penalizing the poor to help lower taxes on the wealthy.
Rep. Morgan Griffith (R-Va.), an Energy and Commerce Committee member, acknowledged “people get scared” when Medicaid work requirements are discussed, but he noted the possibility of exemptions for people with disabilities or those in school.
There have been “some private conversations” though “nothing formal” in the committee about Medicaid changes, he said.
The bottom line:
“It’s hard to make adjustments to reduce federal spending without touching people who rely on the program,” said Robin Rudowitz, director of the Program on Medicaid and the Uninsured at KFF.
Back in February, Dr. Philip Verhoef and I wrote an op-ed for STAT News warning both patients and investors to steer clear of the health insurance industry’s private version of Medicare, which the government continues to allow insurers to market as Medicare Advantage.
As we enter the open enrollment period in which America’s seniors and disabled people are able to choose between the traditional Medicare program and a bewildering array of private plans, it’s a good time to remind you why you need to steer clear of Medicare Advantage.
Millions of people enrolled in those private plans are now getting notices from their insurers that their plans will not be available in 2025 because
three of the biggest insurance corporations (Humana, CVS/Aetna and Cigna) – and probably several smaller insurers – have decided to stop selling MA plans in hundreds of communities across the country, which means that MA enrollees in all those places are going to have to go through the agonizing chore of finding a replacement.
Why? Because Wall Street, which until this year was head-over-heels in love with Medicare Advantage, is now filing for divorce.
Investors have been running for the exits since they began seeing danger signs in for-profit insurers’ earnings reports in the last quarter of 2023. For at least two of the biggest players in MA – Humana and CVS – that exodus has in recent weeks turned into a stampede. The stock prices of those two companies have been in steep decline all year, and you can be certain the top executives of those companies are now in panic mode.
People who’ve been following my work since I blew the whistle on the health insurance racket know I’ve been trying to educate seniors – and policymakers – for at least a dozen years, going back to my time at the Center for Public Integrity, about the many shortcomings of what I’ve often called Medicare Disadvantage. I’ve also called Medicare Advantage the biggest heist of taxpayers’ dollars in American history. It’s truly epic.
The truth is that MA has been a broken system since the beginning, especially for patients. The business worked only as long as insurers were able to extract inappropriately large payments from the Medicare fund through methods like upcoding, where plans list false or exaggerated diagnoses on patient charts to get more money while providing no additional care.
In fact, the MA model relies on providing as little care as possible in general, with insurers putting care approval behind a wall of delays and denials to save money and leaving patients suffering without necessary treatment.
We wrote that op-ed just as the government began taking long-overdue steps to rein in some of those abuses and, to Wall Street’s shock, announced at the end of February that it would not be giving MA plans as much money going forward as the industry had expected. That announcement, coupled with the reins-tightening, really spooked investors.
But that wasn’t all that soured them on Medicare Advantage. The big MA insurers had to admit to Wall Street when they released quarterly earnings that despite their best efforts to delay and deny as much care as possible, seniors nevertheless were using more health care than before.
The insurers’ medical loss ratios were ticking up, meaning they were having to use more of their customers’ premiums (and Medicare fund money) paying claims than they had anticipated. And folks, Wall Street HATES it when insurers do that.
Phil and I wrote that:
Before, investors had assumed MA plans could keep the business humming along, that private insurers would always be able to keep their enrollees’ use of medical goods and services in check, and that policymakers would always look the other way as the government doled out billions in overpayments annually. They now see that these assumptions are failing, and many have sold their holdings in these companies as a result.
The selling has continued apace throughout 2024, and the biggest loser on Wall Street has been Humana, which currently has an 18% share of the MA market, second behind UnitedHealth’s 29%. CVS/Aetna’s shares have also been dropping like a rock.
Humana got another kick to the stomach from investors this week when it admitted that it likely will lose billions of dollars in payments in the future because far fewer of its MA enrollees will be in so-called four-star rated MA plans – 25% in 2025 compared to 94% in 2024. The feds give four-star rated MA plans a lot more money than lower-rated plans.
When the New York Stock Exchange closed yesterday, Humana’s share price had fallen to $241.37. That’s down more than 54% since the 52-week high of $530.54 it reached in October 2023. But get this: on Wednesday the share price reached a 52-week low of $213.31 before inching back up later in the day as some investors apparently saw a way to make money at some point down the road by buying at that low price.
And folks, that was not just a 52-week low. The last time Humana’s share price was in that territory was on April 25, 2017, when the low for the day was $214.51.
All this turmoil has led Bank of America Securities to downgrade the stock to “underperform,” another word for sell. Piper Sandler also downgraded the company yesterday. Those downgrades – and possibly more to come – could cause the stock price to sink even further.
Having worked closely with Humana’s C-suite and investor relations people when I headed corporation communications there before going to Cigna, I can assure you the company’s top brass are grasping at any levers they can get their hands on to stop the freefall. I would not want to be one of them, and I certainly would not want to be one of their customers or investors.
As I mentioned, Humana, UnitedHealth and CVS/Aetna are by far the biggest players in the MA game. Earlier this year, those three companies captured 86% of the 1.7 million new MA enrollees, thanks to spending untold millions of federal dollars on deceptive TV ads and other marketing schemes.
Humana is now dumping hundreds of thousands of its MA enrollees because they somehow managed to get the care they needed. The company is doing that for one single reason: to try to get back into Wall Street’s good graces.
Next week we’ll look at how the other two big players in Medicare Advantage, UnitedHealthcare and CVS/Aetna, are faring on Wall Street. It is a tale of two cities, as you’ll see.
In a surprising turn of events, sources say that CVS Health is exploring the possibility of breaking up its business empire — a move that could unravel years of aggressive vertical integration, including its $70 billion acquisition of health insurer Aetna back in 2017.
While details are still slim, such a move signals just how dire the situation has become for CVSHealth as it navigates mounting financial and regulatory pressures on multiple fronts.
It’s yet another chapter in a story that has seen CVSHealth evolve from a retail pharmacy chain into a health care behemoth — but perhaps one that grew too big, too fast. And to be honest, I’m not surprised. I’ve seen this movie before. In fact, I saw it many times – although each time with different stars – during my 20 years in the health insurance business. One of the most memorable featured Aetna, which in the late 1990s and early 2000s had to retrench, at Wall Street’s insistence, after a buying spree of smaller health insurers that brought the company a ton of unprofitable accounts and disappointing bottom lines. Aetna followed its buying spree with a purging spree, dumping as many as eight million health plan enrollees in short order to get back into Wall Street’s good graces.
It seems that CVSHealth also bought too much too fast. The results? Rising expenses, frustrated patients, and now potential cracks in the corporate structure itself.
CVS: A Cautionary Tale of Vertical Integration
Large corporations like CVS and its peers have used their size to dominate various aspects of health care—whether it’s insurance, retail pharmacy, physician practices and clinics, and controlling the drug supply chain. But as these mega-corporations continue to grow, they also become harder to manage, and their inefficiencies start to become evident.
CVS’s acquisition of Aetna was hailed at the time as a strategic masterstroke — a way to streamline health care by bringing together the different parts of the system under one corporate umbrella. It was supposed to deliver “efficiencies” that would benefit both the company and patients.
But it’s not just the purchase of Aetna. From pharmacy benefit manager Caremark to Aetna to health care providers Signify Health and Oak Street Health — CVS’s business model has become increasingly complex, making it difficult to navigate regulatory scrutiny, rising costs and fierce competition in the retail pharmacy space.
The latest reports suggest that CVS’s board is trying to figure out where Caremark would land in the event of a breakup. Would it stay with the retail side or with the insurance arm?
This isn’t just an internal debate; it’s emblematic of the broader issue—CVS has built a vertically integrated structure that was supposed to work together to improve care, but investors are now questioning how and even if these pieces should fit together.
It’s Been a Hard Few Years for CVS
Federal Trade Commission’s Legal Action Against CVS’s Caremark and Other PBMs
Instead, those supposed efficiencies have largely translated into higher costs for consumers and increased scrutiny from regulators, especially with CVS’s Caremark at the center of anti-competitive practices allegations by the Federal Trade Commission (FTC). PBMs like Caremark control the drug pricing landscape in ways that lack transparency and disproportionately affect patients and independent pharmacies.
Now, as CVS grapples with rising medical costs within its Aetna business — just like its biggest competitors, UnitedHealth and Humana —the company’s management appears to be in damage control mode. While nothing is certain, discussions about splitting the business have reached the boardroom level, according to sources familiar with the matter. This comes as activist investors, like Glenview Capital, push for structural changes to improve CVS’s declining financial performance.
CVS’s Aetna Medicare Advantage Loss in New York City
New York City Mayor Eric Adams had a plan to force city municipal retirees out of traditional Medicare and into a corporate Aetna Medicare Advantage plan. The NYC Organization of Public Service Retirees vehemently opposed the move and spent months fighting it.
In August, a Manhattan Supreme Court judge permanently halted the mayor and Aetna’s attempts.
Wall Street Woes
For CVS Health, 2024 started off bad. CVS missed Wall Street financial analyst’s earnings-per-share expectations for the first quarter of 2024 by several cents. Shareholders’ furor sent CVS’ stock price tumbling from $67.71 to a 15-year low of $54 at one point.
Also in August, CVS Health cut its 2024 forecast for a third time, citing troubles covering seniors via the company’s private Medicare Advantage business. Operating income for CVS Health’s insurance arm, Aetna, dropped a whopping 39% in Q3, which forced the company to shake up its leadership – moving CEO Karen Lynch into the role of managing insurance and publicly firing one of her lieutenants, Executive Vice President Brian Kane.
What’s Next?
The notion that CVS could split its operations would effectively unwind one of the most high-profile health care mergers in recent memory. A split up of the company would mark the end of an era in which health care conglomerates could grow unchecked. CVS’s struggle isn’t happening in isolation—other companies, like Walgreens and Rite Aid, are facing similar financial difficulties and structural questions.
CVS’s potential breakup could signal a broader industry trend toward unwinding massive, vertically integrated health care corporations.
Whether CVS breaks up or not, it’s clear that the model of health care mega-mergers, designed to consolidate power and increase corporate profits, is facing serious headwinds. Cigna recently announced that it is getting out of the Medicare Advantage business and Humana is getting out of the commercial insurance market. UnitedHealth, meanwhile, so far seems to be weathering those headwinds, but it, too, will be facing even more scrutiny by lawmakers and regulators in the months and years ahead.
UnitedHealth Group has taken a beating on Wall Street this week after admitting that its Medicare Advantage plans had to pay out more in medical claims in the third quarter of this year than investors had expected. As I’ve noted many times, Wall Street can’t stand it and gets very spiteful when Big Insurance uses more of our premium dollars paying for patients’ care because that means there’s less money left over to enrich shareholders.
At the end of trading at the New York Stock Exchange Tuesday, UnitedHealth’s share price was down 8.11% — almost $50 a share — falling like a rock from $605.40 to $556.29 as soon as the market opened. It had reached a 52-week high just the day before but fell off a cliff Tuesday morning. This despite the fact that the company still made $8.7 billion in operating profits during the third quarter.
What investors didn’t like at all was the fact that UnitedHealthcare’s medical loss ratio (MLR) climbed to 85.2% from 82.3% for the same period last year.
By other measures, the company did just fine, especially when you look at how much money it made during the first nine months of this year: a whopping $24.5 billion in profits.
Enrollment in both the company’s commercial and Medicare Advantage plans increased, but it posted a significant decline in the number of people enrolled in the Medicaid plans its administers for several states. That’s because of the Medicaid “unwinding” that has been going on since the official end of the pandemic.
And here is another couple of numbers of note from the third quarter:
UnitedHealth’s Optum division, which encompasses its massive pharmacy benefit manager, Optum Rx, made more money for the parent company than the health plan division: $4.5 billion in profits vs. $4.2 billion for UnitedHealthcare.
PBMs have become even more of a cash cow for Big Insurance than Medicare Advantage, which despite the higher MLRs of late is still a reliable money-gushing ATM for the industry.
In my report June 10, I wrote: “The major sources of physician discontent are administrative hassles and unwelcome clinical oversight that create dissonance. They conflict with a false sense of autonomy that the majority of physicians imagined when choosing medicine. Cuts to reimbursement, participation in alternative payment models and medical inflation are manifestations of a system in which ‘suits’ are intruders who make rules, exact handsome salaries, generate corporate profits and distance physicians from patient care purposely… “
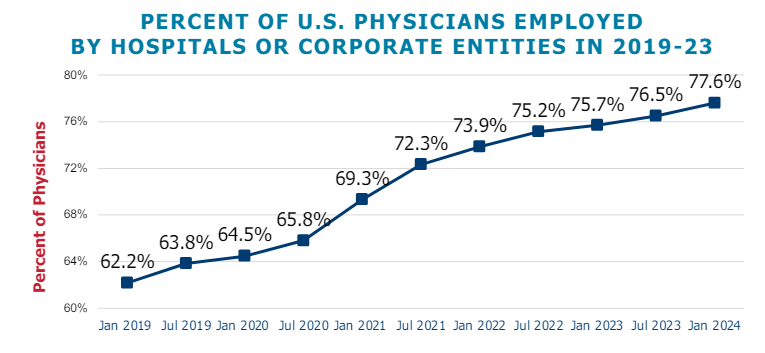
This assessment remains true today. Discontent among physicians is palpable and it’s magnified by a growing sense of financial despair among many clinicians. And it poses a unique challenge to hospitals that now employ more than half of America’s physician workforce.
In the “good ole days”, hospitals provided a place for physicians to ply their trade. They were credentialled to practice their chosen specialty, granted special parking, food and amenities and treated as the hospital’s most welcome customer. Made sense: physicians controlled most patient decisions about the hospital services they use. Physicians controlled the hospital’s revenue, sustainability and bonuses earned by administrators. Insurers brought privately-insured patients to doctors who charged them 1.6-2.5 times what Medicare paid and physician income was not threatened. That was then. This is now.
Today, insurers play a larger role. Consumer expectations have changed. Policymakers are paying more attention. And demand has shifted from inpatient services to outpatient, home and office settings for health and wellbeing services in addition to acute care. And the current forecast by CMS through 2032 predicts spending for hospitals will increase at a compound rate of 5.7% vs. 5.6% for physicians adding more hospital-physician financial tension to the system. Both well-above inflation and CDP growth prompting heightened pressure to spend less.
In anticipation, consolidation of hospitals into multi-hospital systems has been a staple in recent years: only 1 in 5 hospitals is independent these days, and most of these are small, rural or otherwise destined to independence for their uncertain future. Whether public, investor-owned or not-for-profit (or tax exempt as some prefer), the economic realities of running hospitals coupled with the regulatory constraints imposed by state and federal law forced all to re-think their future.And, for most, employing physicians directly was a means to an end of staying alive while the dust settles.
But the unintended consequence of physician employment is soured relationships between the employed physicians and their hospital:
their financial and emotional security has become tangled up by interactions with hospital leaders and former peers appointed to oversee their work.
And their views about their hospital have morphed to negativity based on four underlying beliefs:
Hospitals spend too much on overhead and executive salaries and not enough on direct patient care.
Hospitals are run poorly: we could run them better but they don’t listen to us.
Hospitals get rate increases from Medicare and physicians get screwed.
Hospitals need us more than we need them. But they don’t understand that.
On March 9, 2024, President Biden signed the Consolidated Appropriations Act, 2024, which included a 2.93% update to the CY 2024 Physician Fee Schedule (PFS) Conversion Factor (CF) for dates of service March 9 through December 31, 2024. But physicians saw that as not enough since their overhead increased even more. And for 2025, CMS is proposing to reduce average payment rates under the MPFS by2.93% compared to the average amount reimbursed for these services in CY 2024 based on CY 2025 MPFS conversion factor decrease of $0.93 (or 2.8%) from the current CY 2024 conversion factor.
Understandably, physicians are upset. They’re not delusional that private insurers will make up the difference nor imagining hospitals will divert funds their way from brick, stick and tech priorities. But they’re speaking out expressing their views to anyone who’ll listen.
For hospitals that employ physicians, the issue of their financial anxiety requires urgent attention–not as one of many alongside 340B, site neutral payments and others but as the one at the top of the list. The issue is not whether physician income relative to other professions and average households is high. The issue is about managing physician expectations about their livelihood realistically and practically while improving their clinical acumen as professionals.
The core beliefs held by employed physicians about their hospitals may not be fair, objective or accurate, but they’re no less deeply felt and impactful. Hospital boards and C suite leaders would be well-served to refresh plans accordingly.
On October 15, the open enrollment period for Medicare begins running through December 7 for coverage starting in January 2025. In this period, 67 million Medicare eligible seniors can review features of Medicare plans offered in their area, switch from traditional Medicare to a Medicare Advantage (MA) plan (or vice versa), change their MA selection and add/change their Medicare Part D prescription drug plans.
In 2024, Medicare Advantage plans enrolled 33 million seniors and Medicare paid private insurers $462 billion to pay for their care.
But conditions for Medicare Advantage have changed in recent years prompting many to ask ‘what is the Medicare Advantage?’
Background:
Medicare began July 30, 1965 as a key element in President Lyndon Baines Johnson’s Great Society program offering federal-government-paid insurance coverage for seniors at the age of 65. “Original Medicare” had two parts: Part A to cover hospitals and Part B to cover physicians and outpatient services. In 1972, coverage for adults with disabilities was added, and in 2003, coverage for prescription drugs (Part D) was added.
Its funding comes from payroll taxes paid by employers and their employees, and those who are self-employed PLUS income taxes paid on Social Security benefits, interest earned on the Medicare trust fund’s investments and Part A premiums from people who aren’t eligible for premium-free Part A.
Along the way, Congress authorized seniors the option of accessing Medicare through private insurers aka Part C (Balanced Budget Act of 1997), expanded its scope (Medicare Modernization Act of 2003) and supplemented its funding differential above Original Medicare (Patient Protection and Affordable Care Act 2010) to stimulate enrollment growth. The rationale for MA was straightforward: it offered federal regulators a lab to test care management for seniors with the dual aims of lowering their health costs and improving their health. Private insurers responded. By design, funding for MA was set above Original Medicare rates to encourage private insurer participation.
It worked. This year, the average MA enrollee had 43 plans from which to choose. By three measures, Medicare Part C has been successful:
Enrollment growth: Enrollment in MA plans has increased from 31% of Medicare eligible adults in 2014 to 51% in 2024 and is projected to increase in 2025. Notably, enrollment in special needs and employer-sponsored MA plans has increased faster than the individual MA market which is subject to open enrollment periods. Satisfaction appears high (69% of members do not shop for another plan during open enrollment periods) and member churn is low.
Medicare has saved money: Per the 2024 Medicare Trustees’ Report, MA has contributed to slower growth in Medicare spending than forecast. “The Social Security and Medicare programs both continue to face significant financing issues…The Hospital Insurance (HI) Trust Fund will be able to pay 100% of total scheduled benefits until 2036, 5 years later than reported last year. At that point, that fund’s reserves will become depleted and continuing program income will be sufficient to pay 89% of total scheduled benefits.”
Private insurer participation has been strong: For health insurers, Medicare Advantage is profitable: PMPM contribution margins are 50-100% higher than individual and group lines of business. And, as CMS payments to MA have tightened, the MA insurer market consolidated with 3 (UnitedHealth, Humana, CVS-Aetna) taking advantage of operating pressures on small players to increase their share to 58% of total enrollment. Advantage: Seniors, Medicare and Corporate Insurance.
But conditions going forward suggest the MA advantage might not be as strong. The market signals are clear:
Insurer belt tightening: Since 2023, seniors’ use of hospitals, specialty care and prescription drugs has returned to pre-pandemic normalcy cutting into insurer margins. In its CY 2025 Rate Announcement September 27, CMS announced “The average monthly plan premium for all MA plans, which includes MA plans that provide prescription drug coverage and MA Special Needs Plans (SNPs), is projected to decrease from $18.23 in 2024 to $17.00 in 2025. Benefit options will remain stable, including MA supplemental benefit offerings such as hearing, dental, and vision. The amount of rebate dollars, which can be used for supplemental benefits, will remain stable, with a slight increase, from 2024 to 2025. Enrollment in MA is projected to be 35.7 million in 2025, an increase from 2024, with MA enrollment representing approximately 51% of all people enrolled in Medicare.” This translates to lower margins for MA plans, fewer supplemental benefits for enrollees and lower payments to hospitals and physicians.
Increased regulatory scrutiny: The Medicare Payment Advisory Commission (MedPAC) concluded that MA plans receive payments from CMS that are 122%of spending for similar beneficiaries in traditional Medicare, on average, translating to an estimated $83 billion in overpayments in 2024. Congress is investigating. In 2023, CMS adopted tougher audit standards specific to diagnosis codes used by private MA plans to bill Medicare on behalf of their enrollees. Audits conducted by the U.S. Department of Human Services’ Office of Inspector General (OIG) applying the new standards found the majority of private MA plans guilty of upcoding and thereby overpaid by Medicare. In 2025, cut points used by CMS to award star ratings have been modified resulting in fewer plans getting 4-star ratings that enable their participation in 5% bonus payments—a major reason recent stock declines for UHG, HUM, CVS and others. Regulatory scrutiny of MA plan marketing practices, coding, denials and prior authorization procedures will intensify reflecting bipartisan intent to constrain MA profits.
Understandably, tension between MA insurers and providers has intensified as insurers seek to protect their margins. The Change Healthcare (CH) cyber-attack (February 21, 2024) that disabled insurer payments to hospitals and physicians stoked animosity since CH is a subsidiary of UnitedHealth Group–the largest sponsor of MA plans and the healthcare juggernaut. Though operating margins for half of U.S. hospitals have recovered, insurer cuts coupled with labor and prescription drug costs have decimated care delivery in almost every community. Participation in MA plan provider networks, once SOP is now a tough call for hospitals, medical groups and other providers.
My take:
What is the Medicare Advantage?
As a lab for innovation in care management for seniors, it’s promising.
As an engine to drive lower costs for senior health and extended solvency to the Medicare program, it’s unclear.
As a platform to shift incentives from fee-for-service to value across the system, it’s helpful.
But until and unless hospitals, physicians, insurers, business leaders and regulators commit to implement a transformed system of health that’s comprehensive, affordable, efficient and accountable, the Medicare Advantage will be marginalized.
In many ways, the headwinds facing MA are part of the larger narrative facing healthcare:
public sentiment against consolidation and corporatization has eroded its cherished trust and confidence. It’s true for insurance, hospitals, prescription drug companies and PBMs. The blame is shared: no one of these owns the moral high ground (though a few organizations in their ranks aspire).
With days before voters decide the composition of the 119th U.S. Congress and the next White House occupant, the immediate future for U.S. healthcare is both predictable and problematic:
It’s predictable that…
1-States will be the epicenter for healthcare legislation and regulation; federal initiatives will be substantially fewer.
At a federal level, new initiatives will be limited: continued attention to hospital and insurer consolidation, drug prices and the role of PBMs, Medicare Advantage business practices and a short-term fix to physician payments are likely but little more. The Affordable Care Act will be modified slightly to address marketplace coverage and subsidies and CMSs Center for Medicare and Medicaid Innovation (CMMI) will test new alternative payment models even as doubt about their value mounts. But “BIG FEDERAL LAWS” impacting the U.S. health system are unlikely.
But in states, activity will explode: for example…
In this cycle, 10 states will decide their abortion policies joining 17 others that have already enacted new policies.
3 will vote on marijuana legalization joining 24 states that have passed laws.
24 states have already passed Prescription Drug Pricing legislation and 4 are considering commissions to set limits.
40 have expanded their Medicaid programs
35 states and Washington, D.C., operate CON programs; in 12 states, CONs have been repealed.
14 have legislation governing mental health access.
5 have passed or are developing commissions to control health costs.
And so on.
Given partisan dysfunction in Congress and the surprising lack of attention to healthcare in Campaign 2024 (other than abortion coverage), the center of attention in 2025-2026 will be states. In addition to the list above, attention in states will address protections for artificial intelligence utilization, access to and pricing for weight loss medications, tax exemptions for not-for-profit health systems, telehealth access, conditions for private equity ownership in health services, constraints on contract pharmacies, implementation of site neutral payments, new 340B accountability requirements and much more. In many of these efforts, state legislatures and/or Governors will go beyond federal guidance setting the stage for court challenges, and the flavor of these efforts will align with a state’s partisan majorities: as of September 30th, 2024, Republicans controlled 54.85% of all state legislative seats nationally, while Democrats held 44.19%. Republicans held a majority in 56 chambers, and Democrats held the majority in 41 chambers. In 2024, 27 states are led by GOP governors and 23 by Dems and 11 face voters November 5. And going into the election, 22 states are considered red, 21 are considered blue and 7 are tagged as purple.
The U.S. Constitution affirms Federalism as the structure for U.S. governance: it pledges the pursuit of “life, liberty and the pursuit of happiness” as its purpose but leaves the lion’s share of responsibilities to states to figure out how. Healthcare may be federalism’s greatest test.
2-Large employers will take direct action to control their health costs.
Per the Kaiser Family Foundation’s most recent employer survey, employer health costs are expected to increase 7% this year for the second year in a row. Willis Towers Watson, predicts a 6.4% increase this year on the heels of a 6% bump last year. The Business Group on Health, which represents large self-insured employers, forecasts an 8% increase in 2025 following a 7% increase last year. All well-above inflation, ages and consumer prices this year.
Employers know they pay 254% of Medicare rates (RAND) and they’re frustrated. They believe their concerns about costs, affordability and spending are not taken seriously by hospitals, physicians, insurers and drug companies. They see lackluster results from federal price transparency mandates and believe the CMS’ value agenda anchored by accountable care organizations are not achieving needed results. Small-and-midsize employers are dropping benefits altogether if they think they can. For large employers, it’s a different story. Keeping health benefits is necessary to attract and keep talent, but costs are increasingly prohibitive against macro-pressures of workforce availability, cybersecurity threats, heightened supply-chain and logistics regulatory scrutiny and shareholder activism.
Maintaining employee health benefits while absorbing hyper-inflationary drug prices, insurance premiums and hospital services is their challenge. The old playbook—cost sharing with employees, narrow networks of providers, onsite/near site primary care clinics et al—is not working to keep up with the industry’s propensity to drive higher prices through consolidation.
In 2025, they will carefully test a new playbook while mindful of inherent risks. They will use reference pricing, narrow specialty specific networks, technology-enabled self-care and employee gainsharing to address health costs head on while adjusting employee wages. Federal and state advocacy about Medicare and Medicaid funding, insurer and hospital consolidation and drug pricing will intensify. And some big names in corporate America will step into a national debate about healthcare affordability and accountability.
Employers are fed up with the status quo. They don’t buy the blame game between hospitals, insurers and drug companies. And they don’t think their voice has been heard.
3-Private equity and strategic investors will capitalize on healthcare market conditions.
The plans set forth by the two major party candidates feature populist themes including protections for women’s health and abortion services, maintenance/expansion of the Affordable Care Act and prescription drug price controls. But the substance of their plans focus on consumer prices and inflation: each promises new spending likely to add to the national deficit:
Per the Non-Partisan Committee for a Responsible Federal Budget, over the next 10 years, the Trump plan would add $7.5 trillion to the deficit; the Harris plan would add $3.5 trillion.
Per the Wharton School at the University of Pennsylvania, Harris’ proposals would add $1.2 trillion to the national deficits over 10 years and Trump’s proposals would add $5.8 trillion over the same period
Per the Congressional Budget Office, federal budget deficit for FY2024 which ended September 30 will be $1.8 trillion– $139 billion more than FT 2023. Revenues increased by an estimated $479 billion (or 11 percent). Revenues in all major categories, but notably individual income taxes, were greater than they were in fiscal year 2023. Outlays rose by an estimated $617 billion (or 10 percent). The largest increase in outlays was for education ($308 billion). Net outlays for interest on the public debt rose by $240 billion to total $950 billion.
The federal government spent $6.75 trillion in 2024, a 10% increase from the prior year. Spending on Social Security (22% of total spending) and healthcare programs (28.5% of total spending) also increased substantially. The U.S. debt as of Friday was $37.77 trillion, or $106 thousand per citizen.
The non-partisan Congressional Budget Office (CBO) reports that federal debt held by the public averaged 48.3 % of GDP for the half century ending in 2023– far above its historic average. It projects next year’s national debt will hit 100% for the first time since the US military build-up in the second world war. And it forecast the debt reaching 122.4% in 2034 potentially pushing interest payments from 13% of total spending this year to 20% or more.
Adding debt is increasingly cumbersome for national lawmakers despite campaign promises, and healthcare is rivaled by education, climate and national defense in seeking funding through taxes and appropriations. Thus, opportunities for private investors in healthcare will increase dramatically in 2025 and 2026. After all, it’s a growth industry ripe for fresh solutions that improve affordability and cost reduction at scale.
Combined, these three predictions foretell a U.S. healthcare system that faces a significant pressure to demonstrate value.
They require every healthcare organization to assess long-term strategies in the likely context of reduced funding, increased regulation and heightened attention to prices and affordability. This is problematic for insiders accustomed to incrementalism that’s protected them from unwelcome changes for 3 decades.
Announcements last week by Walgreens and CVS about changes to their strategies going forward reflect the industry’s new normal: change is constant, success is not. In 2025, regardless of the election outcome, healthcare will be a major focus for lawmakers, regulators, employers and consumers.