

Cartoon – Just a Warning Shot


Vaccine passports could become available soon to help people resume their lives — but they face numerous scientific, social and political barriers to being accepted.
The big picture: Reliable and accessible proof of vaccine-induced protection from the novel coronavirus could speed international travel and economic reopening, but obstacles to its wide-scale adoption are so great it may never fully arrive.
Driving the news: The secure digital identity app CLEAR and CommonPass, a health app that lets users access vaccination records and COVID-19 test results, will be working together to offer a vaccine passport service, my Axios colleague Erica Pandey reports.
Yes, but: There are numerous health, ethical and operational questions that need to be resolved before vaccine passports could become an effective part of daily life.
Health: Medical experts still don’t fully know how effective vaccinations — or exposure to the virus — are at preventing onward transmission of COVID-19.
Ethical: The most obvious use case for vaccine passports is for international travel, which has been crippled by onerous quarantine restrictions. But such a system risks locking out billions of people who are unable or unwilling to get the vaccine.
Operational: Passports for international travel are regulated by governments and have decades of history behind them, but there’s no such unified system for vaccine passports, which are being introduced by governments and businesses with different standards, making them a target for fraud.
Be smart: None of these obstacles are insurmountable on their own. But as we saw with the failures of digital contact tracing, just because a technological solution exists doesn’t mean it will be effective or adopted by the public.
The bottom line: Some form of vaccine visas will likely be introduced for international travel, but it seems unlikely they’ll become a passport to resuming normal life.

Kaiser Health News’ latest edition of its “Bill of the Month” series features a patient who was charged a “facility fee,” which drove up what she owed to more than 10 times higher than what she’d previously paid for the same care.
Why it matters: Facility fees — which are essentially room rental fees, as KHN puts it — are becoming increasingly controversial, and patients often receive the bill without warning.
What they’re saying: “Facility fees are designed by hospitals in particular to grab more revenue from the weakest party in health care: namely, the individual patient,” Alan Sager, a professor at the Boston University School of Public Health, told KHN.
Coronavirus cases are on the rise again in several states, partially a result of variants of the virus becoming more widespread, experts say.
Why it matters: Even though a remarkable 72% of Americans 65 and older have received at least one dose of the vaccine, millions of Americans — particularly younger Americans with underlying conditions — remain vulnerable.
Driving the news: Coronavirus cases are rapidly rising in places including Michigan, New York, New Jersey and other Northeastern states.
The big picture: “There are certainly many people who are not vaccinated who are still at severe risk themselves because of underlying medical issues,” said Leana Wen, a visiting professor at the Milken Institute School of Public Health at the George Washington University.
Between the lines: Those still vulnerable to the virus are disproportionately people of color.
What they’re saying: “To address areas of outbreak, we should allocate more of the increased vaccine supply coming into the market to places where penetration is low and infection rates high, like metro Detroit,” former FDA commissioner Scott Gottlieb tweeted.
https://mailchi.mp/3e9af44fcab8/the-weekly-gist-march-26-2021?e=d1e747d2d8

In our work over the years advising health systems on M&A, we’ve been struck by how often “social issues” cause deals that are otherwise strategically sound to go off the rails.
Of course, it’s an old chestnut that “culture eats strategy for breakfast”, but what’s been notable, especially recently, is how early in the process hot-button governance and leadership issues enter the discussions.
Where is the headquarters going to be? Who’s going to be the CEO of the combined entity? And most vexingly, how many board seats is each organization going to get? That last issue is particularly troublesome, as it’s often where negotiations get bogged down. But as one health system board member recently pointed out to us, getting hung up on whether board seats are split 7-6 or 8-5 is just silly—in her words, “If you’re in a position where board decisions turn on that close of a margin, you’ve got much bigger strategic problems.”
It’s an excellent point. While boards shouldn’t just rubber stamp decisions made by management, it’s incumbent on the CEO and senior leaders to enfranchise and collaborate with the board in setting strategy, and critical decisions should rarely, if ever, come down to razor-thin vote tallies.
If a merger makes sense on its merits, and the strategic vision for the combined organization is clear, quibbling over how many seats each legacy system “gets” seems foolish. No board should go into a merger anticipating a future in which small majorities determine the outcome of big decisions.
https://mailchi.mp/3e9af44fcab8/the-weekly-gist-march-26-2021?e=d1e747d2d8
Doctors and health systems with a significant portion of risk-based contracts weathered the pandemic better than their peers still fully tethered to fee-for-service payment. Lower healthcare utilization translated into record profits, just as it did for insurers.
We’re now seeing an increasing number of health systems asking again whether they should enter the health plan business—levels of interest we haven’t seen since the “rush to risk” in the immediate aftermath of the passage of the Affordable Care Act a decade ago.
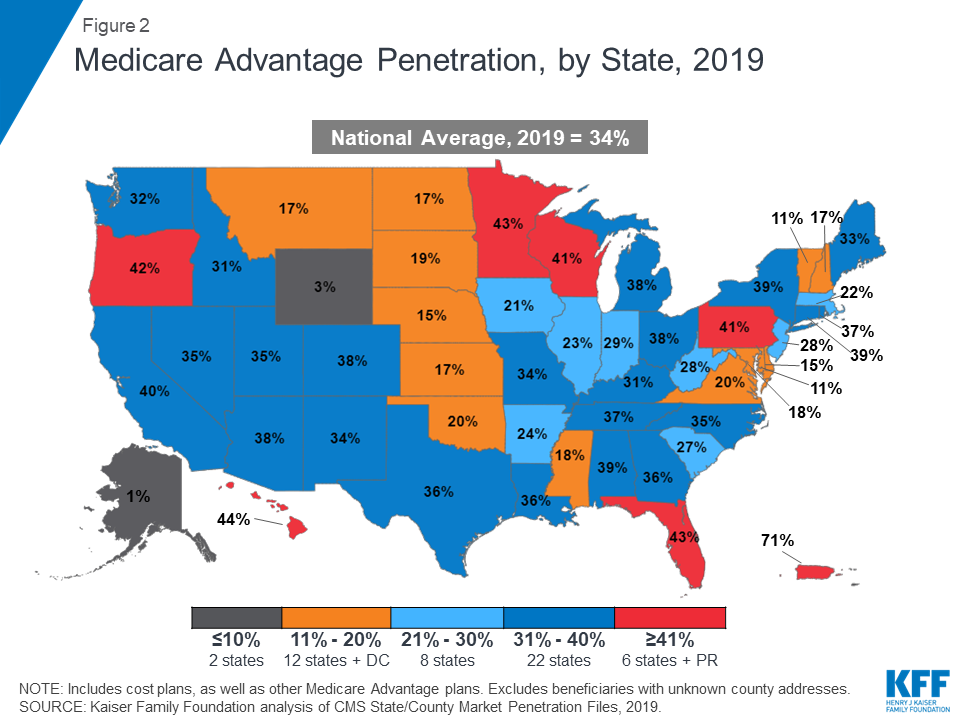
The discussions feel appreciably different this time around (which is a good thing, since many systems who launched plans in the prior wave had trouble growing and sustaining them). First, systems are approaching the market this time with a focus on Medicare Advantage, having seen that growing a base of covered lives with their networks is much easier than starting with the commercial market, where large insurers, particularly incumbent Blues plans, dominate the market, and many employers are still reticent to limit choice.
But foremost, there is new appreciation for the scale needed for a health plan to compete. In 2010, many executives set a goal of 100K covered lives as a target for sustainability; today, a plan with three times that number is considered small. Now many leaders posit that regional insurers need a plan to get to half a million lives, or more. (Somehow this doesn’t seem to hold for insurance startups: see the recent public offerings of Clover Health and Alignment Health, who have just 57K and 82K lives, respectively, nationwide.)
We’re watching for a coming wave of health system consolidation to gain the financial footing and geographic footprint needed to compete in the Medicare Advantage market, and would expect traditional payers to respond with regional consolidation of their own.
https://mailchi.mp/3e9af44fcab8/the-weekly-gist-march-26-2021?e=d1e747d2d8

Large health insurers no longer just provide coverage, but are instead repositioning themselves as vertically integrated healthcare organizations that span the care continuum.
The graphic above shows five-year total revenue growth by segment for the top five health insurance companies.
Some, like Anthem and Humana, are still in the early stages of revenue diversification, leveraging partnerships and investments to fill service gaps—in Humana’s case, these are mainly centered on the Medicare Advantage population.
On the other hand, the insurance revenue of Cigna and CVS Health is already dwarfed by pharmacy benefit management (PBM) revenue (as well as retail clinic revenue for CVS).
UnitedHealth Group (UHG) is clearly leading the pack, with a robust revenue diversification and vertical integration strategy.
Its Optum subsidiary grew 62 percent over the last five years, nearly double the rate of its UnitedHealthcare insurance business. Already the largest employer of physicians in the country, Optum recently announced plans to acquire Massachusetts-based 715-physician group, Atrius Health. It also announced its intent to acquire Change Healthcare, one of the largest providers of revenue and payment cycle management solutions.
Given the outsized role of the Optum division in driving UHG’s growth and profitability, it may soon face a dilemma that other publicly traded, diversified companies have had to confront: shareholder demands to unlock value by spinning off the business into a separate company.
Central to fending off that kind of activism by shareholders: demonstrable steps to integrate the myriad businesses the company has acquired into a functional whole. Just as Amazon’s hugely profitable Web Services business has become a target of spin-off demands, so too, eventually, may UHG’s Optum.
https://mailchi.mp/3e9af44fcab8/the-weekly-gist-march-26-2021?e=d1e747d2d8

If you’re looking for an issue that can unite a heavily divided Congress, it seems nearly all Senators can get behind delaying payment cuts to providers during a pandemic. On Thursday the Senate voted 90-2 to pause the 2 percent sequester cuts to Medicare payment slated to go into effect on April 1.
The bill is expected to be passed by the House and signed into law by President Biden, delaying the cuts through the coronavirus public emergency. While hospitals, many of whom are still recovering from increased costs and volume loss during the pandemic, can breathe a sigh of relief, providers face an even larger 4 percent payment cut in the fall due to the PAYGO, or “pay as you go”, statute, which would trigger automatic payments cuts due to the deficit increases caused by the COVID relief bill.
We’d gamble that intense industry lobbying to delay the PAYGO cuts will prove successful—again, legislators will be reticent to dock provider payment as pandemic recovery continues. But eventually, in a more normal world, hospitals can expect policymakers to shift their focus from pandemic relief to cost control—and it will likely not prove possible to delay the inevitable reckoning over the high cost of our health system.
