Cartoon – Importance of a Consistent Strategy


The latest statistics, as of July 10, show COVID-19-related deaths in U.S. are just under 1,000 per day nationally, which is down from a peak average of about 2,000 deaths per day in April. However, cases are once again rising very substantially, which is worrisome as it may indicate that substantial increases in COVID-19 deaths could follow. How do these numbers compare to deaths of other causes? Ron Fricker, statistician and disease surveillance expert from Virginia Tech, explains how to understand the magnitude of deaths from COVID-19.
Disease surveillance is the process by which we try to understand the incidence and prevalence of diseases across the country, often with the particular goal of looking for increases in disease incidence. The challenge is separating signal from noise, by which I mean trying to discern an increase in disease incidence (the signal) from the day-to-day fluctuations in that disease (the noise). The hope is to identify any increase as quickly as possible so that medical and public health professionals can intervene and try to mitigate the disease’s effects on the population.
A critical tool in this effort is data. Often disease data is collected and aggregated by local and state public health departments and the Centers for Disease Control and Prevention from data that is reported by doctors and medical facilities. Surveillance systems then use this data and a variety of algorithms to attempt to find a signal amidst the noise.
The CDC estimates the average number of flu-related deaths since 2010-11 is around 36,000 per year. This varies from a low of 12,000 deaths in 2011-12 to a high of 61,000 deaths in 2017-18. Thus, the number of COVID-19 deaths to date is three to four times greater than the annual average number of flu-related deaths over the past decade; it is 10 times larger when compared to the 2010-11 flu season but only about twice as large compared to 2017-18.
To make this a fair comparison, note that seasonal influenza mostly occurs over a few months, usually in late fall or early winter. So, the time periods are roughly comparable, with most of the COVID-19-related deaths occurring since late March. However, COVID-19 does not appear to be seasonal, and fatalities are a lagging measure because the time from infection to death is weeks if not months in duration, so the multiples in the previous paragraph will be greater by the end of the year.
Furthermore, while death rates have been coming down from a peak of more than 2,700 on April 21, 2020, the United States is now averaging just under 1,000 deaths per day as of July 10, and given the dramatic increase in cases of late, we should expect the fatality rate to further rise. For example, the University of Washington’s IHME model currently predicts slightly more than 208,000 COVID-19-related deaths by November 1.
So, by any comparison, the COVID-19 death rate is significantly higher than the seasonal influenza death rate.
As of this writing, more than 130,000 people have died of COVID-19, and that total could grow to 200,000 or more by fall. Those numbers are so big, they’re hard to grasp.
Michigan Stadium in Ann Arbor is the largest football stadium in the United States. It holds 107,420 people, so no football stadium in the country is large enough to hold everyone who has died from COVID-19 thus far. By the time bowl season comes along, assuming we have a football season this year, the number of COVID-19 fatalities will likely exceed the capacity of the Rose and Cotton bowl stadiums combined.
The state of Wyoming has a population of slightly less than 600,000 people, so it’s the equivalent of one out of every five people in that state dying in the last four months. By this fall, the COVID-19 death total will be the equivalent of fully one-third of the people in Wyoming dying.
The populations of Grand Rapids, Michigan; Huntsville, Alabama; and Salt Lake City, Utah are each just over 200,000 people. Imagine if everyone in one of those cities died over the course of six months. That’s what COVID-19 may look like by fall.
Today, COVID-19 ranks as the sixth leading cause of death in the United States, following heart disease, cancer, accidents, lower chronic respiratory diseases and stroke. Heart disease is the leading cause, with just over 647,000 Americans dying from it each year. Alzheimer’s disease, formerly the sixth largest cause of death, kills just over 121,000 people per year. If the University of Washington IHME model’s current prediction of COVID-19-related deaths comes to pass, COVID-19 will be the third leading cause of death in the United States by the end of the year.
The American Cancer Society estimates that in 2020 there will be an estimated 1.8 million new cancer cases diagnosed and 606,520 cancer deaths in the United States. Lung cancer is estimated to kill about 135,000 people in the US in 2020, so the number of COVID-19 deaths is currently equivalent and will exceed it soon. Of course, it is important to note that the COVID-19 deaths have occurred in about the past four months while the number of lung cancer deaths is for a year. So, COVID-19 deaths are occurring at roughly three times the rate of lung cancer deaths.
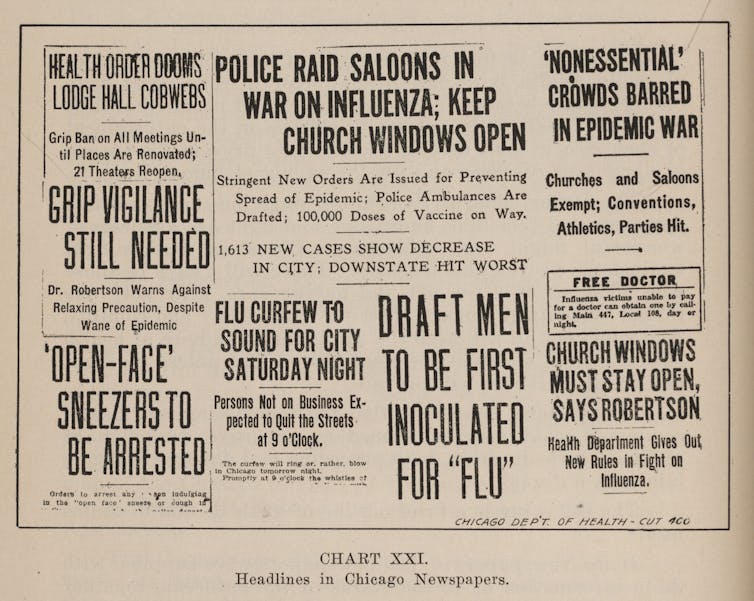
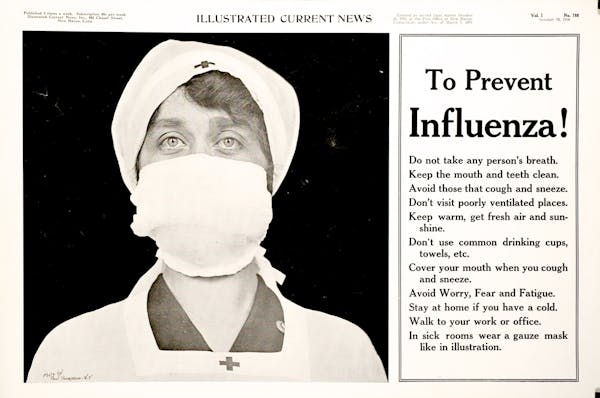
The 1918 influenza pandemic was similar in some ways to the current pandemic and different in other ways. One key difference is the age distribution of deaths, where COVID-19 is concentrated among older adults while the the 1918 pandemic affected all ages. In my state of Virginia, only 8% of the people who died in the 1918 pandemic were more than 50 years old, compared to more than 97% for COVID-19.
The CDC estimates that the 1918 pandemic resulted in about 675,000 deaths in the United States, so slightly more than five times the current number of COVID-19 deaths. In October of 1918, the worst month for the influenza pandemic, about 195,000 people died – well more than all who have died so far from COVID-19.
As with any historical comparison, there are important qualifiers. In this case, the influenza pandemic started in early 1918 and continued well into 1919, whereas COVID-19 deaths are for about one-third of a year (March through June). However, today the United States’ population is about three times the size of the population in 1918. These two factors roughly “cancel out,” and so it is reasonable to think about the 1918 epidemic being about five times worse than COVID-19, at least thus far.
In comparison to past wars, the U.S. has now had more deaths from COVID-19 than all the combat-related deaths in all the wars since the Korean War, including the Vietnam War and Operations Desert Shield and Desert Storm. In World War II there were 291,557 combat casualties. So the number of people who have died from COVID-19 thus far is about 45% of the WWII combat casualties. By the fall, it could be more than 70%.
Finally, note that the number of confirmed and probable deaths from COVID-19 in New York City (23,247 on July 10, 2020) is more than eight times the number who died in the 9/11 attack (2,753).
https://mailchi.mp/da2dd0911f99/the-weekly-gist-july-17-2020?e=d1e747d2d8
Recently, a senior executive shared a concern with us about his leadership style during the pandemic: “I have always thought of myself as a good leader. For the first time in my career, I feel like I’m failing.”
His worry was less about making the big decisions needed in a crisis, and more about the ongoing engagement and “forward motion” of his team.
When in-person meetings transitioned to Zoom calls, he was struck by how much of leadership and team building relies on in-person interaction, whether it’s formal group sessions to drive a decision, or the hundreds of informal one-on-one interactions every week in the office. As our small firm went virtual, it’s something we noticed, too. Virtual interactions require a different structure and pace, and it takes more work to engage the full group.
And while no one enjoys an hours-long videoconference, more frequent, shorter calls can build momentum. Dedicating time to sharing personal updates builds the connections lost when we’re not physically together.
But despite the risks, one CEO shared that in a crisis like COVID-19, showing up in person matters: “You can’t always stay at home or in your office. As a leader you have to be out and talking to staff. I know it’s risky but that is really what it takes.
Being there to clearly articulate the go-forward plan.” We’d love to hear your insights about how you’re adapting your leadership approach to navigate this balance, keeping your teams engaged through this difficult and unfamiliar time.
https://www.axios.com/europe-lessons-reopening-schools-b713801e-26d6-4ba1-bb9e-c0b0b5809a11.html

American parents and policymakers hoping for a safe return to schools in the fall have been looking to Europe, where several countries reopened as early as April without a subsequent spike in cases.
Why it matters: There’s a growing body of evidence suggesting that schools can operate safely, at least under certain circumstances. But no country that closed schools has attempted to reopen them with outbreaks still raging as they are across much of America.
Social distancing: Danish class sizes were initially limited to around 12, and arrival times were staggered to avoid crowding.
Masks: Similarly, countries including Austria initially required masks but loosened those restrictions over time.
“Bubbles”: When the U.K. fully reopens schools in September, smaller subsets of students will spend classes, lunch and recess together — an approach several other countries have experimented with.
Hybrid learning: Several countries have resumed in-person schooling on a more limited basis, supplemented by online education. School districts across the U.S. are designing such approaches now.
What to watch: It remains unclear how susceptible children are to the virus, though findings from a hard-hit town in France — which are consistent with other evidence — suggest it spreads significantly less easily among teens than adults, and hardly at all among young children.
The bottom line: The risks to schools remain uncertain, but will almost certainly depend on what’s happening outside their walls.
https://www.axios.com/coronavirus-pain-getting-worse-cd329f4c-9962-4f40-b401-7a7ac1a393cf.html

For months now, American workers, families and small businesses have been saying they can’t keep up their socially distanced lives for much longer. We’ve now arrived at “much longer” — and the pandemic isn’t going away anytime soon.
The big picture: The relief policies and stopgap measures that we cobbled together to get us through the toughest weeks worked for a while, but they’re starting to crumble just as cases are spiking in the majority of states.
Next week, the extra $600 per week in expanded unemployment benefits will expire. And there’s no indication that Congress has reached a consensus on extending this assistance or providing anything in its place.
Expect more furloughs and layoffs as more small businesses are pushed off the pandemic cliff.
And the question of whether schools will reopen looms.
The bottom line: “It’s the uncertainty that is anxiety-inducing,” says Despard. “If you give people a time horizon and say, ‘Look you have to get through these next 8 weeks of extreme shutdown,’ they’ll do it. Now it’s like, ‘How much longer?'”