The practical effect of the decision is likely to be months of delays, pushing the final outcome of the case beyond the 2020 election.
A federal appeals court in New Orleans handed Republicans a Christmas present.
The court had been considering a case with the potential to dismantle the entire Affordable Care Act, an outcome that could have set off waves of chaos and disruption leading up to the November election, and for which there was very little contingency planning.
The court had two main options. It could have agreed with the Trump administration, along with a set of Republican state officials and a district court in Texas, and overturned all of the law. Or it could have upheld Obamacare, undermining the arguments of the White House and its allies.
The court found a third way. In a decision at the close of business Wednesday, two of the three judges signaled their support for a key part of the Republicans’ legal argument. The two agreed with a lower court that Obamacare’s individual mandate had been made unconstitutional by a 2017 law that eliminated the financial penalty for remaining uninsured. But the judges punted on the case’s key question of what that meant for the rest of the health law, asking a lower court to reconsider it. The effect is likely to be months of delays, pushing the final outcome of the case beyond the 2020 election.
Starting in 2017, the Republicans’ failed effort to repeal and replace large portions of the health law was deeply unpopular and became a central campaign theme of the 2018 election, in which Democrats won a House majority. Democrats cast themselves as the protectors of Obamacare’s most popular provisions, especially its protections for Americans with pre-existing health conditions.
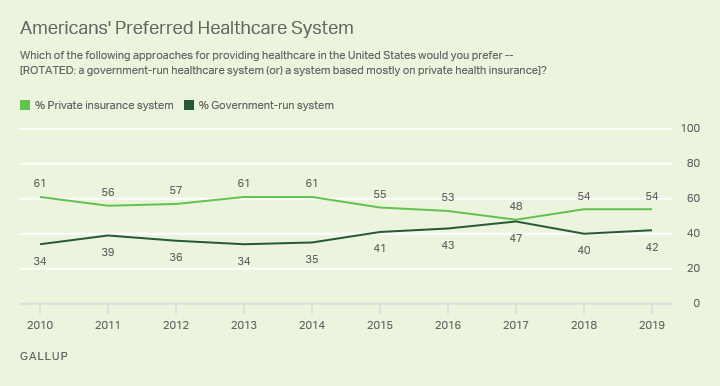
While most Democrats would have favored a court ruling that upheld Obamacare, a reprise of those politics could have given them a lift in an election year. Voters tend to trust Democrats more than Republicans on health care, but much of the debate during the primary season has focused on ambitious new expansions of government coverage. Those proposals do not enjoy the widespread support attached to the preservation of Obamacare’s core consumer protections.
Those dynamics have allowed Republicans to focus on arguments that they will protect private insurance and oppose socialism, without forcing them to articulate their own detailed health plans. President Trump has periodically hinted at an imminent Obamacare replacement plan, but he has yet to produce one. Mitch McConnell, the Senate majority leader, has declined to produce or advance a major health care bill in the Senate.
But if a court had ruled that all of Obamacare had to be wiped off the books, it would have been far harder for Republicans to avoid articulating their vision for health care. The public did not like their previous attempts in 2017, and there has been little progress, even behind the scenes, to produce an alternative plan more palatable to the public. Two concepts have emerged since then, one from a group of conservative think tanks, and one from the House Republican Study Committee. Neither has received much public attention by party leaders, and both share the basic structure of an earlier legislative plan that divided Republican legislators so much that it never made it to a vote.
Meanwhile, Democrats could have retreated to safer ground, by promising to reinstate popular Obamacare provisions.
If the court had overturned all of Obamacare, it could have meant major disruptions to the health system. Such a ruling, if upheld by the Supreme Court, would have eliminated consumer protections for people with pre-existing health conditions, and wiped away financial assistance that have helped millions of middle-class Americans buy their own coverage.
It would have erased the Medicaid expansion, which provides health insurance to millions of low-income Americans in three dozen states. It would have reversed Medicare policies that make prescription drugs more affordable for seniors, and Food and Drug Administration rules that have allowed cheaper copies of expensive biologic drugs to enter the market.
It would have undone major experiments in the delivery of care, meant to improve health care quality. It would have rolled back enhanced punishments for Medicare fraud. It would have reduced requirements that workplaces provide space for lactating mothers to pump breast milk, and requirements that chain restaurants post calorie counts for their food.
Around 20 million more Americans would have become uninsured, according to an estimate from the Urban Institute. Experts on Medicare policy said they were not even sure how some of the changes could have been carried out now that they have been enshrined in complex regulations and built on in subsequent laws.
None of those effects would have happened immediately, even if the Fifth Circuit had agreed in full with the lower court; the Supreme Court would have probably weighed in. But the prospect of such huge changes had the potential to reset the political conversation about health care in both parties. By avoiding a decision on the case’s consequences, the Fifth Circuit has effectively postponed that shift.
In a statement Wednesday night, President Trump applauded the court’s ruling that the individual mandate was unconstitutional. But he emphasized that the decision would not result in any meaningful changes to voters’ health care.
“The radical health care changes being proposed by the far left would strip Americans of their current coverage,” he said. “I will not let this happen. Providing affordable, high-quality health care will always be my priority. They are trying to take away your health care, and I am trying to give the American people the best health care in the world.”
Such a statement would have been harder to issue if the court panel had agreed with the arguments made by Mr. Trump’s lawyers and called for the reversal of Obamacare’s coverage expansions.
Democrats’ frustration with the court’s indecision was palpable. Chuck Schumer, the Senate minority leader, described the judges’ move as “cowardly.” The decision is “obviously an attempt to shield Republicans from the massive blowback they would receive from the public if the highest court in the land were to strike down the A.C.A. before the upcoming election,” he said in a statement.
It’s possible, of course, that the case will reach a final disposition sooner anyway. California’s attorney general, Xavier Becerra, announced that he and other Democratic state officials involved in the case would be appealing the decision to the Supreme Court. Even though the appellate court sent the case back to Texas, the country’s highest court could still choose to take it, should four justices wish to. But the most likely path involves months or years of additional litigation, with lingering uncertainty over the fate of Obamacare.