Only 10 days after a racially motivated mass shooting that killed 10 in a Buffalo, NY grocery store, 19 children and two teachers were murdered on Tuesday at an elementary school in Uvalde, TX. The Uvalde shooting was the 27th school shooting, and one of over 212 mass shootings, that have occurred this year alone.
Firearms recently overtook car accidents as the leading cause of childhood deaths in the US, and more than 45,000 Americans die from gun violence each year.
The Gist: Gun violence is, and has long been, a serious public health crisis in this country. It is both important to remember, yet difficult for some to accept, that many mass shootings are preventable.
Health systems, as stewards of health in their communities, can play a central role in preventing gun violence at its source, both by bolstering mental health services and advocating for the needed legislative actions—supported by a strong majority of American voters—to stem this public health crisis.
As Northwell Health CEO Michael Dowling said this week, “Our job is to save lives and prevent people from illness and death. Gun violence is not an issue on the outside—it’s a central public health issue for us. Every single hospital leader in the United States should be standing up and screaming about what an abomination this is. If you were hesitant about getting involved the day before…May 24 should have changed your perspective. It’s time.”
Everyone agrees that the US healthcare system is not working so great. Compared to the rest of the world, our healthcare is extremely expensive and yet we suffer worse health by many measures. And we can’t seem to agree on what’s to blame, or what we should do about it. Do we have too much, or not enough, competition? Should the government intervene in health care markets more or less?
Basic economics can help us better understand what’s happening.
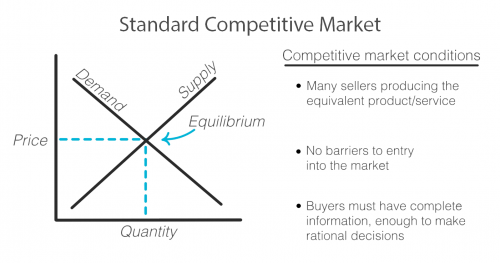
As with any exchange of goods and services, the standard competitive market model has the familiar upward sloping supply curve and downward sloping demand curve, illustrating that when prices are higher, demand decreases and supply increases as sellers are incentivized to produce more of that good or service at its higher price. Sellers and buyers arrive at what quantity to produce and consume and at what price based on where these two lines intersect, called the equilibrium. Both buyer and seller are happy with the deal they’ve struck!
But not every market works this way. There are actually standards that need to be met in order for a market to fit this model and for it to work efficiently for both the buyer and seller.
First, there must exist multiple sellers competing to sell the same goods or services and new sellers must be able to easily enter the market.
There must be a sufficient open exchange of information between buyer and seller about price, availability, and value of a service or good.
And buyers must make, or be in a position to make, rational decisions using the information they possess about the market.
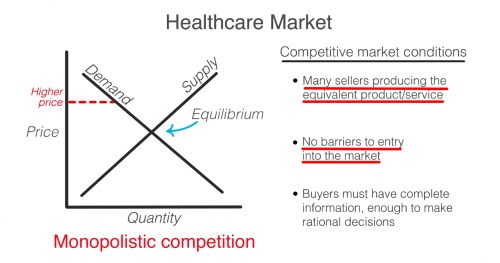
Healthcare does not meet these standards and when these standards are not met, the equilibrium cannot be reached or accurately known. Any price and quantity that falls outside of the equilibrium is considered a market failure. Using only this model, we can see how healthcare’s market failures contribute to high prices.
To start, it’s true that healthcare is failing the market standards when it comes to competition. The number of sellers in the market is decreasing due to both an increase in barriers to entry and due to consolidation, including hospital mergers. This causes an imbalance in power of the seller over the buyer that can begin to reflect what economists call monopolistic competition where sellers can charge a price above the perfect competition equilibrium. In the extreme, when there is only one seller, the market is a monopoly.
So then, don’t we just need more competition? Unfortunately, a lack of competition isn’t the only reason that healthcare fails the market standards.
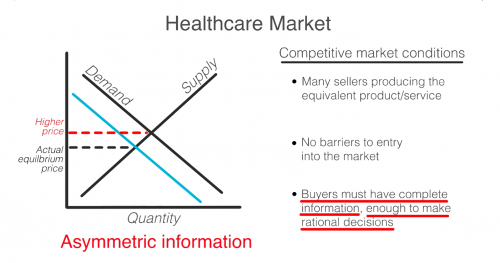
Another failure is that consumers in healthcare, patients, do not have all the information that providers, like doctors and hospitals, do. This is known as asymmetric information. Patients often have no idea before getting care how much it will cost, what the prices available to them elsewhere are, or what the quality will be. When consumers are in the dark about these basic features, the true demand and supply will be different than the model. The true demand may be lower if patients knew ahead of time how much it cost or how much less valuable the service is compared to how it is promoted. This means prices can be set higher than they likely would be if the true demand was known.
Even if patients had full information, they are not always in a position to act as rational consumers. A patient’s decision may be influenced by their concern for their health, or their ability to think rationally may itself be affected by their condition.
So, as you can see, the problem is that a lack of competition only accounts for part of the reason why healthcare doesn’t meet the market standards. No matter how much the government either steps back to allow for more competition or invests to foster competition, the market will never fix ALL of these failures on its own. Healthcare is not and can never be a free market. It simply does not fit this model.
In 1963, economist and later Nobel prize winner, Kenneth Arrow, warned us about this looming healthcare crisis. He explains that “If the actual market differs significantly from the competitive model […] coordination of purchases and sales must take place”
That coordination he is referring to is government intervention.
Dr. Mike Chernew, Health Economist and Professor of Health Policy at Harvard Medical School agrees…“an unregulated health care market is unlikely to lead to desired outcomes.”
In reality, health care always has, and always will, involve a combination of both government intervention and market forces to control prices and increase quality. The debate isn’t really whether or not the government should intervene, but by how much and in what way.
A certain segment of the health policy world spends a lot of time trying to get more states to expand Medicaid and reduce underinsurance.
But are we doing enough to make sure care is accessible once people enroll? One issue is access to physicians, who are less likely to treat patients on Medicaid than Medicare or private insurance because Medicaid payment rates are lower.
A new paper in Health Affairs by Avital Ludomirsky and colleagues looked at how well the networks of physicians supposedly participating in Medicaid reflect access to care. The researchers used claims data and provider directories from Medicaid managed care plans (the private insurers that most states contract with to run their Medicaid programs) in Kansas, Louisiana, Michigan and Tennessee from 2015 and 2017 to assess how the delivery of care to Medicaid patients was distributed among participating doctors. Their results were striking:
One-quarter of primary care physicians provided 86% of the care; one-quarter of specialists provided 75%.
One-third of both types of physicians saw fewer than 10 Medicaid patients per year, hardly contributing any “access” at all.
There was only one psychiatrist for every 8,834 Medicaid enrollees after excluding those seeing fewer than 10 Medicaid patients per year. This is especially concerning given that the COVID-19 pandemic has worsened mental health in the U.S., particularly among children.
The authors note that their study only covers primary care and mental health providers in four states, so it is not necessarily generalizable to other states or specialties. But these results are still concerning.
States have so-called network adequacy standards for their Medicaid managed care plans that are supposed to make sure there are enough providers. These standards typically rely on either a radius (a certain number of providers for a geographic area) or ratio (number of providers per enrollee), but the authors’ findings show these methods fall short if they are based on directories alone.
The authors specifically recommend states use claims-based assessments like the ones in the study and “secret shopper” programs — like this recently published one from Maryland by Abigail Burman and Simon Haeder — to better evaluate whether plans are offering adequate access to physicians. We absolutely need people to have coverage, but it needs to be more than just a card in their wallet.
Despite substantial operating margin declines during the first year of COVID-19, U.S. hospitals were able to keep their finances on track thanks to billions in government relief funds, Johns Hopkins researchers wrote in a new study published Friday in JAMA Health Forum.
Per their analysis of Centers for Medicare and Medicaid Services (CMS) Hospital Cost Reports data, researchers found that thousands of hospitals broadly maintained their overall profit margins thanks to a boost in “other nonoperating income,” the category under which hospitals recorded the collective $175 billion in subsidies Congress allocated to support healthcare facilities and clinicians.
This was particularly the case for government, rural and smaller hospitals that typically run on tighter margins, the researchers wrote. Because they, by design, received more targeted relief than other types of hospitals, these facilities were able to record higher overall profit margins in 2020 than in prior years.
“Hospital operations were really hit hard during the pandemic,” Ge Bai, professor in the Bloomberg School’s Department of Health Policy and Management, a professor of accounting at the Johns Hopkins Carey Business School and an author of the study, said in a statement.
“Our study shows that the relief funds provided an important lifeline to keep financially weak hospitals up and running.”
Among the study’s sample of 1,378 hospitals, mean operating margin declined from –1.0% in 2019 to –7.4% in 2020, representing the hit facilities took to their operations prior to the relief funding.
Those hospitals’ mean overall profit margin during the first year of the pandemic was 6.7%, which the researchers wrote was stable in light of the preceding four years and across all ownership types, geographic locations and hospital sizes.
The difference-maker, they wrote, was an increase in other nonoperating income as a share of a hospital’s total revenue. While that mean share was 4.4% in 2019, it jumped to 10.3% in 2020 thanks to the government relief funds.
Additionally, certain types of hospitals with traditionally lower overall profit margins saw significant improvements in 2020. These included government hospitals (3.7% to 7.2%), rural hospitals (1.9% to 7.5%) and hospitals with fewer admissions (3.5% to 6.7%).
“Hospitals that tend to serve socioeconomically disadvantaged patients and more who are uninsured are the most vulnerable to financial losses,” Yang Wang, a doctoral student in the Bloomberg School’s Department of Health Policy and Management and the study’s first author, said in a statement. “But the extra federal funding helped them stay operational.”
The researchers’ study included hospitals with fiscal years beginning in January whose financial data were compiled and processed as part of RAND Hospital Data, which in turn pulls its data from CMS’ Medicare Cost Reports. The findings persisted among a second sample of 785 hospitals from the database with fiscal years beginning in July.
The government’s distribution of COVID-19 relief funds to providers has faced some critique from healthcare policy researchers, some of whom suggested that the methodology led to funding skewed toward hospitals serving well-insured communities.
Much of the relief set aside for hospitals has since run dry or is on its last legs as of early 2022. With COVID hospitalizations again ticking upward and earlier surges still unaccounted for, industry groups and the Biden administration alike are pushing Congress for more relief support.
Private insurance plans paid hospitals on average 224% more compared with Medicare rates for both inpatient and outpatient services in 2020, a new study found.
Researchers at RAND Corporation looked at data from 4,000 hospitals in 49 states from 2018 to 2020. While the 224% increase in rates is high, it is a slight reduction from the 247% reported in 2018 in the last study RAND performed.
“This reduction is a result of a substantial increase in the volume of claims in the analysis from states with prices below the previous average price,” the study said.
The report showed that plans in certain states wound up paying hospitals more than others. It found that Florida, West Virginia and South Carolina had prices that were at or even higher than 310% of Medicare.
But other states like Hawaii, Arkansas and Washington paid less than 175% of Medicare rates.
“Employers can use this report to become better-informed purchasers of health benefits,” study lead author Christopher Waley said in a statement. “The work also highlights the levels and variation in hospital prices paid by employers and private insurers, and thus may help policymakers who may be looking for strategies to curb healthcare spending.”
The data come as the federal government has explored ways to lower healthcare costs, including going toe-to-toe with the hospital industry. The Centers for Medicare & Medicaid Services (CMS) has in recent years sought to cut payments to off-campus outpatient clinics in order to bring Medicare payments in line with payments paid to physicians’ offices but has met with stiff legal and lobbying opposition from the hospital industry that argues the extra payments are needed.
CMS has also published regulations that call on hospitals to increase transparency of prices, including a rule that mandates hospitals publish online the prices for roughly 300 shoppable services.
The hospital industry pushed back against RAND’s findings, arguing that the study is based on incomplete data. The industry group American Hospital Association said researchers only looked at 2.2% of overall hospital spending, a small portion of overall expenses.
“Researchers should expect variation in the cost of delivering services across the wide range of U.S. hospitals – from rural critical access hospitals to large academic medical centers,” said AHA CEO Rick Pollack in a statement to Fierce Healthcare. “Tellingly, when RAND added more claims as compared to previous versions of this report, the average price for hospital services declined.”
Corporate America is facing a flurry of questions about how it provides health benefits in the wake of a leaked U.S. Supreme Court draft that indicates the federal right to abortion could be overturned.
Why it matters: Businesses hoping to use reproductive health benefits as part of efforts to recruit and retain employees would have to be careful not to run afoul of laws should states be allowed to ban abortions.
The balancing act over the next several months could get messy, experts warn.
What they’re saying: “It’s a serious issue for employers,” said Candice Sherman, the CEO of the Northeast Business Group on Health. The group represents roughly 80 large companies such as American Express, Colgate, Moderna and Pfizer.
Limits on abortion coverage have the potential to impact the physical and mental health of the workforce and could come as many employers are addressing equity and inclusion for women, people of color and LGBTQ employees, Sherman said.
That is often communicated by companies through benefit design.
State of play: Some large companies like Amazon, Apple and Lyft have already announced plans to provide workarounds in those states with abortion restrictions.
But many others are still on the sidelines as they tease out employees’ priorities on abortion-related benefits, as well as the potential costs and legal risks.
Eleven states restrict insurance coverage of abortion in all private insurance plans written in the state, including those offered through Affordable Care Act markets, according to the Guttmacher Institute. Six other states require abortion coverage in private health insurance plans.
Zoom in: One of the most immediate questions is what kind of employer-sponsored abortion coverage — as well as enhanced benefits like travel stipends — might create legal liabilities for companies in states that ban abortion.
“There’s a question as to whether providing transportation benefits could be construed, or at least alleged by the states in enforcement, as aiding and abetting,” said Garrett Hohimer, director of policy and advocacy for the Business Group on Health. That group counts corporations like The Walt Disney Co., Walmart and General Motors among its members.
Yes, but: In the case of a challenge, companies would have a strong argument that federal protections for providing abortion care benefits preempt state laws, Emily Dickens, the head of government affairs for the Society for Human Resource Management, told Axios.
Dickens pointed specifically to the Pregnancy Discrimination Act which specifically says an employer is permitted to provide health insurance coverage for abortion, as well as protections under ERISA law.
But, but, but: It’s not a sure thing. For instance:“ERISA is not a get out of jail free card,” Hohimer warned, saying there is some question about how the law would be interpreted.
While experts largely believe the Affordable Care Act would provide protections for birth control coverage, it’s unclear how fertility benefits such as egg freezing, surrogacy or in vitro fertilization might be affected, Sherman said.
What to watch: Many large companies already offer health benefits allowing workers to travel to Centers of Excellence for procedures like joint replacements or cancer care.
Those kinds of benefits will likely gain more attention because of the attention surrounding reproductive health, Hohimer said.
Sherman said this may also raise questions about whether there’s flexibility in the tax code to expand the scope of Flexible Spending Accounts or Health Savings Accounts to cover travel for any health care issues.
The bottom line: “Assuming this discussion comes down the way we think it may, organizations are going to have to work very hard,” Sherman said.
COVID-19 hospitalizations are up 20 percent nationwide over the last 14 days, with 39 states and Washington, D.C., reporting an increase.
Nationwide, COVID-19 cases increased 58 percent over the past 14 days, according to HHS data collected by The New York Times. Reported case counts may be directionally helpful at this point of the pandemic, given the use of rapid, at-home COVID-19 tests that result in under-counting.
“I think that we’re dramatically undercounting cases,” former FDA commissioner Scott Gottlieb, MD, toldCBS News April 11. “We’re probably only picking up one in seven or one in eight infections.”
Hospitalizations are up 20 percent nationwide over the last 14 days, with a daily average of 19,694 people hospitalized with COVID-19 as of May 12. The CDC is keeping a close eye on the acuity of hospitalizations, with Director Rochelle Walensky, MD, noting that the agency is seeing less oxygen use, fewer ICU stays and no increase in associated death compared with earlier periods of the pandemic.
Here are the 14-day changes for hospitalizations in each state and Washington, D.C., reporting an increase, along with their daily average hospitalizations:
Hawaii: 64 percent (92 hospitalizations)
Maine: 61 percent (222)
Montana: 58 percent (25)
Massachusetts: 55 percent (703)
Pennsylvania: 47 percent (1,104)
Alaska: 45 percent (38)
Connecticut: 42 percent (337)
Michigan: 42 percent (812)
Rhode Island: 40 percent (87)
Wisconsin: 39 percent (314)
Delaware: 37 percent (188)
Iowa: 36 percent (113)
New Hampshire: 35 percent (112)
New York: 31 percent (2,627)
Virginia: 31 percent (383)
Minnesota: 28 percent (404)
Florida: 28 percent (1,380)
New Jersey: 27 percent (707)
Maryland: 25 percent (458)
West Virginia: 24 percent (120)
Illinois: 23 percent (815)
Nevada: 23 percent (161)
Ohio: 22 percent (734)
Oregon: 20 percent (284)
Kentucky: 19 percent (249)
Washington, D.C.: 19 percent (84)
Colorado: 18 percent (170)
Vermont: 17 percent (64)
Indiana: 15 percent (297)
California: 14 percent (1,463)
South Carolina: 13 percent (127)
Louisiana: 11 percent (65)
Kansas: 7 percent (79)
Georgia: 5 percent (576)
North Carolina: 5 percent (877)
Utah: 4 percent (72)
Idaho: 4 percent (45)
Missouri: 3 percent (384)
Nebraska: 2 percent (76)
Arkansas: 2 percent (97)
The 14-day changes for cases in each state reporting an increase, along with their daily average cases, can be found through HHS data collected by The New York Timeshere. Seven-day changes for cases in each state can be found here.
The more contagious omicron subvariant BA.2 makes up 68.1 percent of new cases in the U.S., according to the latest estimates from the CDC. New Jersey has the highest proportion of BA.2 cases of all states, according to the latest ranking of states by the subvariant’s prevalence.
President Joe Biden signed into law March 15 a sweeping $1.5 trillion bill that funds the government through September. The legislation did not include COVID-19 funding the White House had requested from Congress because of partisan disagreement about offsetting the funding.
The current lack of funding is affecting resources for COVID-19 testing and treatment. The Health Resources and Services Administration stopped accepting providers’ claims for COVID-19 testing and treatment of the uninsured March 22 because of a lack of sufficient funds, and stopped accepting claims for the vaccination of uninsured people April 5. The federal government is also cutting back shipments of monoclonal antibody treatments to states by 30 percent, and the U.S. supply of those treatments could run out as soon as May.
The U.S. may see a “pretty sizable wave” of COVID-19 infections this fall and winter as the virus continues to evolve and immunity wanes, White House Covid-19 Response Coordinator Ashish Jha, MD, said May 8 on ABC News‘ “This Week.”
Federal health officials are looking at a range of disease forecasting models, which suggest the U.S. could experience a large surge in late 2022, similar to the last two winters, according to Dr. Jha. On May 6, the White House projected 100 million COVID-19 infections could occur this fall and winter, according to The Washington Post.
“If we don’t get ahead of this thing … we may see a pretty sizable wave of infections, hospitalizations and deaths this fall and winter,” he said. “Whether that happens or not is largely up to us as a country. If we can prepare and if we can act, we can prevent that.”
More funding to purchase COVID-19 vaccines and therapeutics will be crucial to stave off a potential surge, according to Dr. Jha. The Biden administration is asking Congress for an additional $22.5 billion in emergency aid to support these efforts.
“If Congress does not do that now, we will go into this fall and winter with none of the capabilities that we have developed over the last two years,” Dr. Jha said.
If the leaked Supreme Court draft opinion overturning Roe v. Wade—which in 1973 established an individual’s constitutional right to an abortion—is finalized, as many as 26 states are either certain or likely to ban abortion. The resulting patchwork of abortion laws across the country could create confusion for providers and hospitals on multiple fronts, including cases related to the Federal Emergency Medical Treatment and Labor Act (EMTALA), as well as for health systems that operate in multiple states. Medical training on the procedure could become much more limited, as about half of the nation’s obstetrics and gynecology residencies are in states likely to ban abortion.
Recognizing the precarious position that abortion bans will put some providers in, the American Medical Association released a statement on Thursday saying that it is “deeply concerned” with the draft opinion, and that it “would lead to government interference in the patient-physician relationship, dangerous intrusion into the practice of medicine, and potentially criminalizing care.”
The Gist: Abortion is just one of a raft of issues where the provision of health services increasingly intersects with charged politics in this country. If Roe is overturned, medication abortion—the use of abortion pills—which already accounts for more than half of all abortions, will increase, although multiple states are already seeking to limit access.
Restricting access to safe abortions will also further exacerbate health disparities, driving up the already distressingly high US maternal mortality rate, especially among Black women. Andoverturning Roe would have implications far beyond access to abortion, especially for patients experiencing miscarriages, ectopic pregnancies, or other life-threatening medical conditions related to pregnancy.
The Department of Justice (DOJ) is appealing a Florida judge’s Monday decision to strike down the mask requirement for public transportation. Federal judge Kathryn Mizelle ruled the Centers for Disease Control and Prevention (CDC) exceeded its authority under the Public Health Service Act of 1944. Meanwhile, giddy passengers and flight crew have been discarding their face coverings as airlines, the Transportation Safety Administration, several local transit authorities, Uber and Lyft, all removed their mask requirements.
The Gist: Despite DOJ’s appeal, which appears to be aimed at preserving its own authority to act during health crises, rather than reinstating the current mask requirement (which was set to expire in two weeks anyway), the tone of the Biden administration is clearly shifting. Earlier this week President Biden told reporters that the decision to wear a mask is “up to them,” meaning individual Americans.
In the bumpy transition out of the emergency phase of the pandemic, we now have a patchwork of rules for masking. This is even true within healthcare facilities: some, including Houston Methodist and Iowa-based UnityPoint Health, are no longer requiring masks for visitors or employees who are not involved in patient care.
With COVID cases now rising in 41 states as mask mandates fall, the next month will prove critical in determining whether “endemic” COVID remains manageable, or once again stresses the healthcare system and other critical infrastructure.