A group of health system leaders in Missouri challenged state-reported hospital bed data, saying it could lead to a misunderstanding about hospital capacity, according to a Nov. 19 report in the St. Louis Business Journal.
A consortium of health systems, including St. Louis-based BJC HealthCare, Mercy, SSM Health and St. Luke’s Hospital, released urgent reports warning that hospital and ICU beds are nearing capacity while state data reports show a much different story.
The state reports, based on data from TeleTracking and the CDC-managed National Healthcare Safety Network, show inpatient hospital bed capacity at 35 percent and remaining ICU bed capacity at 29 percent on Nov. 19. However, the consortium reported hospitals are fuller, at 84 percent capacity as of Nov. 18, and ICUs at 90 percent capacity based on staffed bed availability. The consortium says it is using staffed bed data while the state’s numbers are based on licensed bed counts; the state contends it does take staffing into account, according to the report.
Stephanie Zoller Mueller, a spokesperson for the consortium, said the discrepancy between the state’s data and consortium’s data could create a “gross misunderstanding on the part of some and can be a dangerous message to the community.”
From El Centro Regional Medical Center, the largest hospital in California’s Imperial County, it takes just 30 minutes to drive to Mexicali, the capital of the Mexican state of Baja California. The international boundary that separates Mexicali from Imperial County is a bridge between nations. Every day, thousands of people cross that border for work or school. An estimated 275,000 US citizens and green card holders live in Baja California. El Centro Regional Medical Center has 60 employees who reside in Mexicali and commute across the border, CEO Adolphe Edward told Julie Small of KQED.
Now these inextricably linked places have become two of the most concerning COVID-19 hot spots in the US and Mexico. While Imperial County is one of California’s most sparsely populated counties, it has the state’s highest per capita infection rate — 836 per 100,000, according to the California Department of Public Health. This rate is more than four times greater than Los Angeles County’s, which is second-highest on that list. Imperial County has 4,800 confirmed positive cases and 64 deaths, and its southern neighbor Mexicali has 4,245 infections and 717 deaths.
The COVID-19 crisis on the border is straining the local health care system. El Centro Regional Medical Center has 161 beds, including 20 in its intensive care unit (ICU). About half of all its inpatients have COVID-19, Gustavo Solis reported in the Los Angeles Times, and the facility no longer has any available ventilators.
When Mexicali’s hospitals reached capacity in late May, administrators alerted El Centro that they would be diverting American patients to the medical center. “They said, ‘Hey, our hospitals are full, you’re about to get the surge,’” Judy Cruz, director of El Centro’s emergency department, recounted to Rebecca Plevin in the Palm Springs Desert Sun.
By the first week of June, El Centro was so overburdened that “a patient was being transferred from the hospital in El Centro every two to three hours, compared to 17 in an entire month before the COVID-19 pandemic,” Miriam Jordan reported in the New York Times.
Border Hospitals Filled to Capacity
Since April, hospitals in neighboring San Diego and Riverside Counties have been accepting patient transfers to alleviate the caseload at the lone hospital in El Centro, but the health emergency has escalated and now those counties need relief. “We froze all transfers from Imperial County [on June 9] just to make sure that we have enough room if we do have more cases here in San Diego County,” Chris Van Gorder, CEO of Scripps Health, told Paul Sisson in the San Diego Union-Tribune. El Centro patients are now being airlifted as far as San Francisco and Sacramento.
According to the US Census Bureau, nearly 85% of Imperial County residents are Latino, and statewide, Latinos bear a disproportionate burden of COVID-19. The California Department of Public Health reports that Latinos make up 39% of California’s population but 57% of confirmed COVID-19 cases.
Nonessential travel between the US and Mexico has been restricted since March 21, with the measure recently extended until July 21. However, jobs in Southern California, such as in agricultural fields and packing houses, require regular movement between the two countries. “I’m always afraid that people are imagining this rush on the border,” Andrea Bowers, a spokesperson for the Imperial County Public Health Department, told Small. “It’s just folks living their everyday life.”
These jobs, some of which are considered essential because of their role in the food supply chain, may have contributed to the COVID-19 crisis on the border. Agricultural workers often lack access to adequate personal protective equipment and are unable to practice physical distancing. They also are exposed to air pollution, pesticides, heat, and more — long-term exposures that can cause the underlying health conditions that raise the risk of death for COVID-19 patients.
Comite Civico del Valle, a nonprofit focused on environmental health and civic engagement in Imperial Valley, set up 40 air pollution monitors throughout the county and found that levels of tiny, dangerous particulates violated federal limits, Solis reported.
“I can tell you there’s hypertension, there’s poor air pollution, there’s cancers, there’s asthma, there’s diabetes, there’s countless things people here are exposed to,” David Olmedo, an environmental health activist with Comite Civico del Valle, told Solis.
Fear of New Surges
With summer socializing in full swing, health experts worry that COVID-19 spikes will follow. Imperial County saw surges after Mother’s Day and Memorial Day, probably because of lapsed physical distancing and mask use at social events.
Latinos in California are adhering to recommended public health behaviors to slow the spread of the virus. CHCF’s recent COVID-19 tracking poll with Ipsos asked Californians about their compliance with recommended behaviors. Eighty-four percent of Californians, including 87% of Latinos, say they routinely wear a mask in public spaces all or most of the time. Seventy-two percent of Californians, including 73% of Latinos, say they avoid unnecessary trips out of the home most or all of the time, and 90% of Californians, including 91% of Latinos, say they stay at least six feet away from others in public spaces all or most of the time.
A Push to Reopen Anyway
Most counties in California have met the state’s readiness criteria for entering the “Expanded Stage 2” phase of reopening. Imperial County has not. In the past two weeks, more than 20% of all COVID-19 tests in the county came back positive, the Sacramento Bee reported. The state requires counties to have a seven-day testing positivity rate of no more than 8% to enter Expanded Stage 2.
Still, the Imperial County Board of Supervisors is pushing Governor Gavin Newsom for local control over its reopening timetable. The county has a high poverty rate — 24% compared with the statewide average of 13% — and “bills are stacking up,” Luis Pancarte, chairman of the board, said on a recent press call.
He worries that because neighboring areas like Riverside and San Diego have opened some businesses with physical distancing measures in place, Imperial County residents will travel to patronize restaurants and stores. This movement could increase transmission of the new coronavirus, just as reopening Imperial County too soon could as well.
More than 1,350 residents have signed a petition asking Newsom to ignore the Board of Supervisor’s request, Solis reported. The residents called on the supervisors to focus instead on getting the infection rate down and expanding economic relief for workers and businesses.
Cruz, who has been working around the clock to handle the county’s COVID-19 crisis, agrees with the petitioners. The surges after Mother’s Day and Memorial Day made her “really concerned about unlocking and letting people go back to normal,” she told Plevin. “It’s going to be just like those little gatherings that happened [on holidays], but on a bigger scale.”
With recent flare-up in neighboring counties, L.A.-area hospital leaders want the county to work with the state to keep surge hospitals open.
Healthcare officials on Tuesday called for Los Angeles County leaders to work with the state to reopen its “surge” hospital and recommended that another in Long Beach swing open its doors, citing the need to fully reopen medical centers while also dealing with an expected surge in coronavirus cases.
The state-funded Los Angeles Surge Hospital, which opened on April 13 at the former site of the St. Vincent Medical Center amid heightened concern about having enough beds to deal with Covid-19 patients, has closed.
But Dr. Hector Flores, an Adventist Health White Memorial physician, told the county’s Board of Supervisors and his fellow members on the county’s Economic Resiliency Task Force that county officials should work to bring it back online. He also recommended that Long Beach Community Hospital — which has long been on the cusp of reopening — become a surge hospital.
The context in June is different, however, than it was in March and April, when public health officials were intensely concerned that the county’s hospital capacity would be overwhelmed by a never-before-seen virus that was spreading and killing exponentially.
Along with many other businesses, hospitals, too, shut down many services in an effort to grow bed capacity for COVID-19 patients. But those services were essential for many hospitals’ bottom line — everything from elective procedures to vital surgeries. Couple that with patients who were delaying or outright canceling vital non-coronavirus visits, and in the first 90 days of the pandemic in L.A. County, hospitals — typically among the largest employers — were shedding jobs and occupancy (which fell to about 40% collectively, according to Flores).
“Hospitals are like hotels. If they are not fully occupied they are losing money,” said Flores, who heads a working group on the county’s task force.
Ultimately, the industry took an estimated $15 billion hit, he said, and only now, in the past two weeks is it starting to recover as health orders are eased and 15,000 doctors and medical support staffs make their way back to their once-shuttered practices.
Flores, and his committee of healthcare leaders have been devising a framework for recovery in the healthcare sector of the county’s economy. They want to maintain those jobs in the $100-billion-a-year healthcare industry.
It’s a larger goal among county leaders, who started the resiliency task force to figure out how several of the region’s economic sectors can recover after being shut down for months.
But there’s a looming concern: A second wave of the virus.
Flores said recent coronavirus spikes in Orange and Ventura counties — which saw large crowds gathering at beaches over the Memorial Day holiday — are giving him pause.
And that’s prompted Flores and others to call for the county to work with state officials to reopen and keep surge hospitals open. The move would help regular hospitals keep their non-COVID business going but allow for more capacity, if needed.
As it stands, non-COVID patients are coming back. Hospitals over the last two to three weeks have gone from 40% to 85% occupancy rates.
“What that tells us is that if there is a surge there won’t be the same capacity that we had for the first 90 days (of the pandemic),” he said. “We’re concerned about the uptick we see in Ventura and Orange County, since on Memorial Day weekend they opened beaches, hiking trails and parks. Sadly, many people took advantage of that open environment without protection of masks and often congregating in clusters. We’re also waiting to see the impact of the protests in two weeks.”
State and local officials have repeatedly said that public health data will guide local decisions, and have held out the possibility that public health orders could be re-tightened.
During Tuesday’s meeting, Supervisor Sheila Kuehl questioned whether Flores meant the county should keep surge hospitals “available” or actually open them.
Flores said as hospitals reopen and perform essential surgeries, they need “safe units” where patients can recover from an operation without the threat of being infected by the virus. And to do that, they need more space, he said.
“As we see a smaller number of beds available in hospitals, we are eventually going to rely on surge hospitals … because we anticipate there is quite likely going to be another surge if the patterns we see in Ventura and Orange counties come to play in Los Angeles,” Flores said.
The shuttered St. Vincent’s hospital, on a 10-acre campus in the Westlake District near Downtown Los Angeles, seemed essential when it was pressed into duty on April 13 after being closed in January. It quickly became part of the state’s plan to outfit roughly 50,000 more hospital beds to handle a surge of infected patients.
Ultimately, though, that surge never came. The hospital treated 65 people at a cost to taxpayers of nearly $15 million, the Southern California News Group reported.
It may very well stay that way. A spokesperson for the hospital said Tuesday that the hospital is “officially closed at the present time, there are no plans to reopen.”
Long Beach Community Hospital, too, was eyed. City leaders and officials from Molina, Wu, Network, Inc. — the hospital’s new operator — scurried to reopen it in the early COVID-19 days.
MWN said in late March that the facility was “days away” from opening, as Long Beach looked for capacity. That never came. Plus, the U.S. Navy hospital ship Mercy, which arrived in Los Angeles in late March to help treat non-coronavirus patients, returned to San Diego after treating just 77 patients.
Meanwhile, regular hospitals were scambling to find room for the expected surge of COVID patients. But between that and the March “Safer-at-Home” order, hospitals suffered the unintended consequence of furlough and layoffs related to a shortage of “non-essential” medical work.
The county’s Department of Health Services says the decision to reopen the St. Vincent’s property lies with the state, which in consultation with Dignity Health and Kaiser, closed down operations as its contract was due to run out by the end of June.
Could it come back online?
“The opinion of the County is that a) currently we project having sufficient overall beds in the county to meet demand (with the exception of ICU which can be resolved by flexing bed types within existing hospitals) and b) surging our existing hospitals,” according to a statement.
Officials say adding beds at existing hospitals is a “better approach” because it makes use of the existing infrastructure. County health services officials add that all hospitals have the ability “to surge patients at least 20% above their normal capacity.”
As for Long Beach Community Hospital, health officials noted that it has not yet been approved to operate by licensing through the state.
“We would welcome LBCH coming on line as an additional acute care hospital, but need for them to meet state licensing criteria,” according to the statement.
L.A. County Public Health officials predict that with no change in the transmission rate of the disease, the demand for hospital beds will remain relatively stable, with some slight “up-trending” because of the easing of health-order restrictions.
Hospitalizations across the county were down to 1,285 as of Monday from a peak of nearly 2,000 in late April. While the numbers have been down considerably, some hospitals have experienced a slight uptick in recent days. Whether that increase is the result of an oncoming surge has yet to be seen, according to Molly Lawson, spokeswoman for Centinela Hospital Medical Center in Inglewood.
“It’s really too early to tell,” Lawson said. “This week we had anticipated seeing the community impact of some of the protests and marches and all the activities happening of late.”
Centinela Hospital, which according to Lawson had one of the higher levels of hospitalization rates, treated about 70 COVID-19 patients in late April and early May. Patients occupied two full units, Lawson said. As of Tuesday, the hospital had 17 patients, just half a unit.
At Torrance Memorial Medical Center, which saw a peak of about 55 patients just as “Safer-at-Home” orders went into effect in late March, the hospital has been treating 15 to 21 patients for the past several weeks, according to spokeswoman Sandy Rodriguez. The lowest number of COVID-19 patients the hospital had admitted was 11.
“We have seen some intermittent increases, but no surge,” Rodriguez said.
ProPublica deputy managing editor Charles Ornstein wanted to know why experts were wrong when they said U.S. hospitals would be overwhelmed by COVID-19 patients. Here’s what he learned, including what hospitals can do before the next wave.
The prediction from New York Gov. Andrew Cuomo was grim.
In late March, as the number of COVID-19 cases was growing exponentially in the state, Cuomo said New York hospitals might need twice as many beds as they normally have. Otherwise there could be no space to treat patients seriously ill with the new coronavirus.
“We have 53,000 hospital beds available,” Cuomo, a Democrat, said at a briefing on March 22. “Right now, the curve suggests we could need 110,000 hospital beds, and that is an obvious problem and that’s what we’re dealing with.”
The governor required all hospitals to submit plans to increase their capacity by at least 50%, with a goal of doubling their bed count. Hospitals converted operating rooms into intensive care units, and at least one replaced the seats in a large auditorium with beds. The state worked with the federal government to open field hospitals around New York City, including a large one at the Jacob K. Javits Convention Center.
But when New York hit its peak in early April, fewer than 19,000 people were hospitalized with COVID-19. Some hospitals ran out of beds and were forced to transfer patients elsewhere. Other hospitals had to care for patients in rooms that had never been used for that purpose before. Supplies, medications and staff ran low. And, as The Wall Street Journal reported on Thursday, many New York hospitals were ill prepared and made a number of serious missteps.
All told, more than 30,000 New York state residents have died of COVID-19. It’s a toll worse than any scourge in recent memory and way worse than the flu, but, overall, the health care system didn’t run out of beds.
“All of those models were based on assumptions, then we were smacked in the face with reality,” said Robyn Gershon, a clinical professor of epidemiology at the NYU School of Global Public Health, who was not involved in the models New York used. “We were working without situational awareness, which is a tenet in disaster preparedness and response. We simply did not have that.”
Cuomo’s office did not return emails seeking comment, but at a press briefing on April 10, the governor defended the models and those who created them. “In fairness to the experts, nobody has been here before. Nobody. So everyone is trying to figure it out the best they can,” he said. “Second, the big variable was, what policies do you put in place? And the bigger variable was, does anybody listen to the policies you put in place?”
So, why were the projections so wrong? And how can political leaders and hospitals learn from the experience in the event there is a second wave of the coronavirus this year? Doctors, hospital officials and public health experts shared their perspectives.
The Models Overstated How Many People Would Need Hospital Care
The models used to calculate the number of people who would need hospitalization were based on assumptions that didn’t prove out.
Early data from the U.S. Centers for Disease Control and Prevention suggested that for every person who died of COVID-19, more than 11 would be hospitalized. But that ratio was far too high and decreased markedly over time, said Dr. Christopher J.L. Murray, director of the Institute for Health Metrics and Evaluation at the University of Washington. IHME’s earliest models on hospitalizations were based on that CDC data and predicted that many states would quickly run out of hospital beds.
A subsequent model, released in early April, assumed about seven hospitalizations per death, reducing the predicted surge. Currently, Murray said, the ratio is about four hospital admissions per death.
“Initially what was happening and probably what we saw in the CDC data is doctors were admitting anybody they thought had COVID,” Murray said. “With time they started admitting only very sick people who needed oxygen or more aggressive care like mechanical ventilation.”
A patient with COVID-19 is taken into Mount Sinai Hospital in New York on May 3. (Alexi Rosenfeld/Getty Images)
A model created by the Harvard Global Health Institute made a different assumption that also turned out to be too high. Data from Wuhan, China, suggested that about 20% of those known to be infected with COVID-19 were hospitalized. Harvard’s model, which ProPublica used to build a data visualization, assumed a hospitalization rate in the United States of 19% for those under 65 who were infected and 28.5% for those older than 65.
But in the U.S., that percentage proved much too high. Official hospitalization rates vary dramatically among states, from as low as 6% to more than 20%, according to data gathered from states by The COVID Tracking Project. (States with higher rates may not have an accurate tally of those infected because testing was so limited in the early weeks of the pandemic.) As testing increases and doctors learn how to treat coronavirus patients out of the hospital, the average hospitalization rate continues to drop.
New York state’s testing showed that by mid-April, approximately 20% of the adult population in New York City had antibodies to COVID-19. Given the number hospitalized in the city and adjusting for the time needed for the body to produce antibodies, this means that the city’s hospitalization rate was closer to 2%, said Dr. Nathaniel Hupert, an associate professor at Weill Cornell Medicine and co-director of the Cornell Institute for Disease and Disaster Preparedness.
Dr. Ashish Jha, director of the Harvard Global Health Institute, and his team also assumed that between 20% and 60% of the population would be infected with COVID-19 over six to 18 months. That was before stay-at-home orders took effect nationwide, which slowed the virus’s spread. Outside of New York City, a far lower percentage of the population has been infected. Granted, we’re not even six months into the pandemic.
A number of factors go into disease models, including the attack rate (the percentage of the entire population that eventually becomes infected), the symptomatic rate (how many people are going to show symptoms), the hospitalization rate for different age groups, the fraction of those hospitalized that will need intensive care and how much care they will need, as well as how the disease travels through the population over time (what is known as “the shape of the epidemic curve”), Hupert said.
Before mid-March, Hupert’s best estimate of the impact of COVID-19 in New York state was that it would lead to a peak hospital occupancy of between 13,800 to 61,000 patients in both regular medical wards and intensive care. He shared his work with state officials.
David Muhlestein, chief strategy and chief research officer at Leavitt Partners, a health care consulting firm, said one takeaway from COVID-19 is that models can’t try to predict too far into the future. His firm has created its own projection tool for hospital capacity that looks ahead three weeks, which Muhlestein said is most realistic given the available data.
“If we were held to our very initial projection of what was going to happen, everybody would be very wrong in every direction,” he said.
Hospitals Proved Surprisingly Adept at Adding Beds
When calculating whether hospitals would run out of beds, experts used as their baseline the number of beds in use in each hospital, region and state. That makes sense in normal times because hospitals have to meet stringent rules before they are able to add regular beds or intensive care units.
Workers prepare dozens of extra beds that were delivered to Mount Sinai on March 31. (Spencer Platt/Getty Images)
But in the early weeks of the pandemic, state health departments waived many rules and hospitals responded by increasing their capacity, sometimes dramatically. “Just because you only have six ICU beds doesn’t mean they will only have six ICU beds next week,” Muhlestein said. “They can really ramp that up. That’s one of the things we’re learning.”
Take Northwell Health, a chain of 17 acute-care hospitals in New York. Typically, the system has 4,000 beds, not including maternity beds, neonatal intensive care unit beds and psychiatric beds. The system grew to 6,000 beds within two weeks. At its peak, on April 7, the hospitals had about 5,500 patients, of which 3,425 had COVID-19.
The system erected tents, placed patients in lobbies and conference rooms, and its largest hospital, North Shore University Hospital, removed the chairs from its 300-seat auditorium and replaced them with a unit capable of treating about 50 patients. “We were pulling out all the stops at that point,” Senior Vice President Terence Lynam said. “It was unclear if the trend was going to go the other way. We did not end up needing them all.”
Northwell went from treating 49 COVID-19 inpatients on March 16 to 3,425 on April 7. “I don’t think anybody had a clear handle on what the ceiling was going to be,” Lynam said. As of Wednesday, the system was still caring for 367 COVID-19 patients in its hospitals.
As hospitals found ways to expand, government leaders worked with the Army Corps of Engineers to build dozens of field hospitals across the country, such as the one at the Javits Center. According to an analysis of federal spending by NPR, those efforts cost at least $660 million. “But nearly four months into the pandemic, most of these facilities haven’t treated a single patient,” NPR reported. As they began to come online, stay-at-home orders started producing results, with fewer positive cases and fewer hospitalizations.
Demand for Non-COVID-19 Care Plummeted More Than Expected
Hospitals across the country canceled elective surgeries, from hip replacements to kidney transplants. That greatly reduced the number of non-COVID-19 patients they had to treat. “We generated a lot more capacity by getting rid of elective procedures than any of us thought was possible,” Harvard’s Jha said.
Northwell canceled elective surgeries on March 16, and over the span of the next week and a half, its hospitals discharged several thousand patients in anticipation of the coming surge. “In retrospect, it was a wise move,” Lynam said. “It just ballooned after that. If we had not discharged those patients in time, there would have been a severe bottleneck.”
What’s more, experts say, it’s clear that some patients with true emergencies also stayed home. A recent report from the CDC said that emergency room visits dropped by 42% in the early weeks of the pandemic. In 2019, some 2.1 million people visited ERs each week from late March to late April. This year, that dropped to 1.2 million per week. That was especially true for children, women and people who live in the Northeast.
In New York City, emergency room visits for asthma practically ceased entirely at the peak, Cornell’s Hupert said. “You wouldn’t imagine that asthma would just disappear,” he said. “Why did it go away? … Nobody has seen anything like that.”
Undoubtedly some people experienced heart attacks and strokes and didn’t go to the hospital because they were fearful of getting COVID-19. “I didn’t expect that,” Jha said. A draft research paper available on a preprint server, before it is reviewed and published in an academic journal, found that heart disease deaths in Massachusetts were unchanged in the early weeks of the pandemic compared to the same period in 2019. What that may mean is that those people died at home.
The Coronavirus Attacked Every Region at a Different Pace
Some initial models forecast that COVID-19 would hit different regions in similar ways. That has not been the case. New York was hit hard early; California was not, at least initially.
In recent weeks, hospitals in Montgomery, Alabama, saw a lot of patients. Arizona’s health director has told hospitals in the state to “fully activate” their emergency plans in light of a spike in cases there. The Washington Post reported on Tuesday that hospitalizations in at least nine states have been rising since Memorial Day.
St. Luke’s, a closed hospital in Phoenix, is prepared to receive overflow patients on April 23. Arizona initially wasn’t hit hard, but cases are now spiking. (Ross D. Franklin/AP Photo)
Dr. Mark Rupp, medical director of the Department of Infection Control and Epidemiology at the University of Nebraska Medical Center in Omaha, said his region hasn’t seen a tidal wave like New York. “What we’ve seen is a rising tide, a steady increase in the number of cases.” Initially that was associated with outbreaks at specific locations like meatpacking and food processing plants and to some degree long-term care facilities.
But since then, “it has just plateaued,” he said. “That has me concerned. This is a time when I feel like we should be working as hard as we can to push these numbers as low as possible.”
Rupp’s hospital has been caring for 50 to 60 COVID-19 patients on any given day. The hospital has started to perform surgeries and procedures that had been on hold because “elective cases stay elective for only so long.”
The hospital’s general medical/surgical beds are 70% to 80% filled, and its ICU beds are 80% to 90% full. “We don’t have a big cushion.”
Even in New York City, the virus hit boroughs differently. Queens and the Bronx were hard hit; Manhattan, Brooklyn and Staten Island less so. “Maybe we can’t even model a city as big as New York,” Hupert said. “Each neighborhood seemed to have a different type of outbreak.”
That needs further study but could be attributable to both social and demographic conditions and the type of jobs residents of the neighborhoods had, among other factors.
What We Can Learn From Coronavirus “Round One”
While hospitals were able to add beds more quickly than experts realized they could, some other resources were harder to come by. Masks, gowns and other personal protective equipment were tough to get. So were ventilators. Anesthesia agents and dialysis medications were in short supply. And every additional bed meant the need for more doctors, nurses and respiratory therapists.
In early February, before any cases were discovered in New York, Northwell purchased $5 million in PPE, ventilators and lab supplies just in case, Lynam said. “It turned out to be a wise move,” he said. “What’s clear is that you can never have enough.”
Northwell has spent $42 million on PPE alone. “We were going through 10,000 N95 masks a day, just a crazy amount,” he said. “One of the lessons learned is you have to stockpile the PPE. There’s got to be a better procurement process in place.”
If there’s one thing the system could have done differently, Lynam said, it’s bringing in more temporary nurses earlier. Northwell brought in 500 nurses from staffing agencies. “They came in a week later than they should have.”
Dr. Robert Wachter, chair of the department of medicine at the University of California, San Francisco, agreed. “I’ve helped run services in hospitals for 25 years,” he said. “I’ve probably given two minutes of thought to the notions of supply chains and PPE. You realize that is absolutely central to your preparedness. That’s a lesson.”
Experts and hospital leaders agree that everyone can do better if another wave hits. Here’s what that entails:
Having testing readily available, as it now is, to more quickly spot a resurgence of the virus.
Stocking up now on PPE and other supplies. “We definitely have to stockpile PPE by the fall,” Gershon of NYU said. “We have to. … [Hospitals and health departments] have to really get those contracts nailed down now. They should have been doing this, of course, all the time, but no one expected this kind of event.”
Being able to quickly move personnel and equipment from one hot spot to the next.
Planning for how to care for those with other medical ailments but who are scared of contracting COVID-19. “We have to have some sort of a mechanism by which we can offer people assurance that if they come in, they won’t get sick,” Jha said. “We can’t repeat in the fall what we just did in the spring. It’s terrible for hospitals. It’s terrible for patients.”
Providing mental health resources for front-line caregivers who have been deeply affected by their work. The intensity of the work, combined with watching patients suffer and die alone, was immensely taxing.
Coming up with ways to allow visitors in the hospital. Wachter said the visitor bans in place at many hospitals, though well intentioned, may have backfired. “When all hell was breaking loose and we were just doing the best we could in the face of a tsunami, it was reasonable to just keep everybody out,” he said. “We didn’t fully understand how important that was for patients, how much it might be contributing to some people not coming in for care when they really should have.”
Lynam of Northwell said he’s worried about what lies ahead. “You look back on the 1918 Spanish flu and the majority of victims from that died in the second wave. … We don’t know what’s coming on the second wave. There may be some folks who say you’re paranoid, but you’ve got to be prepared for the worst.”
If 20% of the US population were to become infected with COVID-19, it would result in an average of $163.4 billion in direct medical costs.
One of the major concerns about the COVID-19 coronavirus pandemic has been the burden that cases will place on the healthcare system. A new study published April 23 in the journal Health Affairs found that the spread of the virus could cost hundreds of billions of dollars in direct medical expenses alone and require resources such as hospital beds and ventilators that may exceed what is currently available.
The findings demonstrate how these costs and resources can be cut substantially if the spread of COVID-19 coronavirus can be reduced to different degrees.
The study was led by the Public Health Informatics, Computational and Operations Research team at the City University of New York Graduate School of Public Health and Health Policy, along with the Infectious Disease Clinical Outcomes Research Unit at the Los Angeles Biomedical Research Institute, Harbor-UCLA Medical Center and Torrance Memorial Medical Center.
The team developed a computer simulation model of the entire U.S. that could then simulate what would happen if different proportions of the population end up getting infected with the COVID-19 coronavirus. In the model, each infected person would develop different symptoms over time and, depending upon the severity of those symptoms, visit clinics, emergency departments or hospitals.
The resources each patient would require – such as healthcare personnel time, medication, hospital beds and ventilators – would then be based on the health status of each patient. The model then tracks the resources involved, the associated costs and the outcomes for each patient.
For example, if 20% of the U.S. population were to become infected with the COVID-19 coronavirus, there would be an average of 11.2 million hospitalizations and 1.6 million ventilators used, costing an average of $163.4 billion in direct medical costs during the course of the infection.
The study shows the factors that could push this amount up to 13.4 million hospitalizations and 2.3 million ventilators used, costing an average of $214.5 billion. If 50% of the U.S. population were to get infected with COVID-19, there would be 27.9 million hospitalizations, 4.1 million ventilators used and 156.2 million hospital bed days accrued, costing an average of $408.8 billion in direct medical costs during the course of the infection.
This increases to 44.6 million hospitalizations, 6.5 million ventilators used and 249.5 million hospital bed days (general ward plus ICU bed days) incurred, costing an average of $654 billion during the course of the infection if 80% of the U.S. population were to get infected. The significant difference in medical costs when various proportions of the population get infected show the value of any strategies that could reduce infections and, conversely, the potential cost of simply letting the virus run its course – the “herd immunity” approach.
Simply put, allowing people to get infected until herd immunity thresholds are met would come at a tremendous cost, and even if social-distancing measures were relaxed and the country “opened up” too early, the healthcare system, as well as the broader economy, would come close to buckling under the weight of the additional costs.
WHAT’S THE IMPACT?
The study shows how costly the coronavirus is compared to other common infectious diseases. For example, a single symptomatic COVID-19 infection costs an average of $3,045 in direct medical costs during the course of the infection alone. This is four times higher than a symptomatic influenza case and 5.5 times higher than a symptomatic pertussis case. Factoring in the costs from longer lasting effects of the infection such as lung damage and other organ damage increased the average cost to $3,994.
Importantly, for a sizable proportion of those who get infected, healthcare costs don’t end when the active infection ends, and costs will likely stay high even after the bulk of the pandemic has passed.
A continuing concern is that the U.S. healthcare system will become overloaded with the surge of COVID-19 coronavirus cases and will subsequently not have enough person-power, ventilators and hospital beds to accommodate the influx of patients. The study shows that even when only 20% of the population gets infected, the current number of available ventilators and ICU beds will not be sufficient.
According to the Society of Critical Care Medicine, there are approximately 96,596 ICU beds and 62,000 full-featured mechanical ventilators in the U.S., substantially lower than what would be needed when only 20% of the population gets infected.
THE LARGER TREND
Data released this week by Kaufman Hall illustrates the extent to which U.S. hospitals are already suffering financially due to the coronavirus.
Looking at earnings before interest, taxes, depreciation and amortization, hospitals’ operating margins fell more than 100% in March, dropping a full 13 percentage points relative to last year. Compared to most months, that’s a much greater change. Operating EBITDA margin was up just 1% in March 2019, for example, and down 1% in February of this year.
These margins likely fell even further across broader health systems, which often include substantial physician and ambulatory operations outside of the hospital, Kaufman Hall found. Overall, operating margins fell 170% below budget for the month.
Peak demand for hospital resources due to COVID-19 is expected this week in the U.S., according to updated projections from the University of Washington’s Institute for Health Metrics and Evaluation in Seattle.
The model, first released in late March, presents estimates of predicted health service utilization and deaths due to COVID-19 for each state in the U.S. if social distancing measures are maintained through May. Researchers used state-level hospital capacity data, data on confirmed COVID-19 deaths from the World Health Organization, and observed COVID-19 utilization from select locations.
When IHME first released its model, the only place where the number of daily deaths had already peaked was Wuhan, China. The data from Wuhan formed the basis for IHME’s estimation of the time from implementation of social distancing policies to the peak day of deaths. That estimation is now based on data from Wuhan and seven locations in Spain and Italy where the number of daily deaths appears to be peaking or to have peaked. The model has also been updated to use three different weighting schemes to better approximate the variation in potential policy impact across social distancing mandates.
Projections for peak demand for resources, namely hospital beds and ventilators, also changed after IHME incorporated new data sources into its model and made changes to its analytical framework. Access more information about the changes here.
According to the most recent projections, which use data updated April 8, peak demand for hospital resources will occur at the national level on April 11. However, this varies by state. Below is the projected date of peak demand for hospital beds, ICU beds and ventilators in each state according to the IHME model.
April 1 Vermont
April 2 Washington
April 4 Louisiana
April 7 Michigan
April 8 Colorado
New York
Ohio
April 9 Delaware
District of Columbia
April 11 Illinois
New Jersey
April 12 Hawaii
April 13 California
Pennsylvania
Wisconsin
April 14 Idaho
Indiana
April 15 North Carolina
West Virginia
April 16 Mississippi
New Hampshire
April 17 Alaska
Maine
Maryland
Nevada
Tennessee
April 20 Alabama
Georgia
Kansas
Massachusetts
Montana
Virginia
April 21 Connecticut
Florida
Kentucky
Missouri
New Mexico
North Dakota
Esther Choo is an emergency physician and associate professor at the Oregon Health & Science University. She is a popular science communicator who has used social media to talk about racism and sexism in healthcare. She was the president of the Academy of Women in Academic Emergency Medicine and is a member of the American Association of Women Emergency Physicians.
As the coronavirus pandemic sweeps the globe, it’s hard to know where to turn or what to think. TED Connects is a free, live, daily conversation series featuring experts whose ideas can help us reflect and work through this uncertain time with a sense of responsibility, compassion and wisdom.
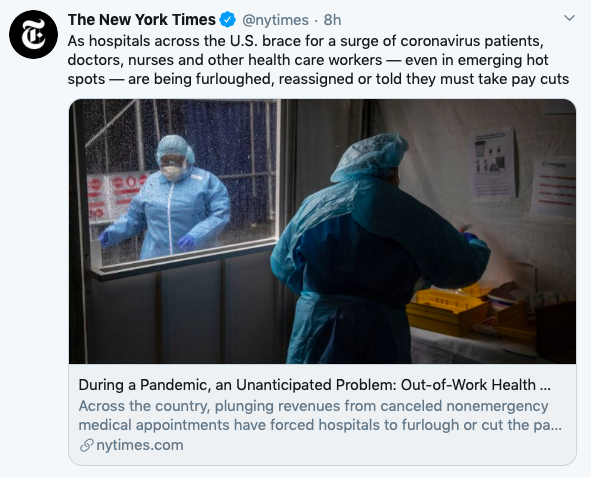
As hospitals across the country brace for an onslaught of coronavirus patients, doctors, nurses and other health care workers — even in emerging hot spots — are being furloughed, reassigned or told they must take pay cuts.
The job cuts, which stretch from Massachusetts to Nevada, are a new and possibly urgent problem for a business-oriented health care system whose hospitals must earn revenue even in a national crisis. Hospitals large and small have canceled many elective services — often under state government orders — as they prepare for the virus, sending revenues plummeting.
That has left trained health care workers sidelined, even in areas around Detroit and Washington, where infection rates are climbing, and even as hard-hit hospitals are pleading for help.
“I’m 46. I’ve never been on unemployment in my life,” said Casey Cox, who three weeks ago worked two jobs, one conducting sleep research at the University of Michigan and another as a technician at the St. Joseph Mercy Chelsea Hospital near Ann Arbor, Michigan. Within a week, he had lost both.
Mayor Bill de Blasio of New York has begged doctors and other medical workers from around the country to come to the city to help in areas where the coronavirus is overwhelming hospitals.
“Unless there is a national effort to enlist doctors, nurses, hospital workers of all kinds and get them where they are needed most in the country in time, I don’t see, honestly, how we’re going to have the professionals we need to get through this crisis,” de Blasio said Friday morning on MSNBC.
And the Department of Veterans Affairs is scrambling to hire health care workers for its government-run hospitals, especially in hard-hit New Orleans and Detroit, where many staff members have fallen ill. The department moved to get a federal waiver to hire retired medical workers to beef up staff levels.
But even as some hospitals are straining to handle the influx of coronavirus patients, empty hospital beds elsewhere carry their own burden.
“We’re in trouble,” said Gene Morreale, the chief executive of Oneida Health Hospital in upstate New York, which has not yet seen a surge in coronavirus patients.
Governors in dozens of states have delivered executive orders or guidelines directing hospitals to stop nonurgent procedures and surgeries to various degrees. Last month, the U.S. surgeon general, Dr. Jerome M. Adams, also implored hospitals to halt elective procedures.
That has left many health systems struggling to survive.
Next week, Morreale said, Oneida will announce that it is putting 25% to 30% of its employees on involuntary furlough. They will have access to their health insurance through June. Physicians and senior staff at the hospital have taken a 20% pay cut.
“We’ve been here 121 years, and I’m hoping we’re still there on the other side of this,” Morreale said.
Appalachian Regional Healthcare, a 13-hospital system in eastern Kentucky and southern West Virginia, has seen a 30% decrease in its overall business because of a decline in patient volume and services related to the pandemic. Last week, the hospital system announced it would furlough about 8% of its workforce — around 500 employees.
Hospital executives across the country are cutting pay while also trying to repurpose employees for other jobs.
At Intermountain Healthcare, which operates 215 clinics and 24 hospitals in Utah, Idaho and Nevada, about 600 of the 2,600 physicians, physicians assistants and registered nurses who are compensated based on volume will see their pay dip by about 15%, said Daron Cowley, a company spokesman.
Those reductions are tied to the drop in procedures, which has fallen significantly for some specialties, he said. The organization is working to preserve employment as much as possible, in part by trying to deploy 3,000 staff members into new roles.
“You have an endoscopy tech right now that may be deployed to be at hospital entrances” where they would take the temperatures of people coming in, Cowley explained.
In Boston, a spokesman for Partners HealthCare, with 12 hospitals, including Massachusetts General and Brigham and Women’s, said staff members whose work has decreased are being deployed to other areas or will be paid for up to eight weeks if no work is available.
But redeployment is not always an option. Janet Conway, a spokeswoman for Cape Fear Valley Health System in Fayetteville, North Carolina, said many of the company’s operating room nurses trained in specialized procedures have been furloughed because their training did not translate to other roles.
“Those OR nurses, many have never worked as a floor nurse,” she said.
Conway said nearly 300 furloughed staff members have the option to use their paid time off, but beyond that, the furlough would be unpaid. Most employees are afforded 25 days per year.
Some furloughed hospital workers are likely to be asked to return as the number of coronavirus cases rise in their communities. But the unpredictable virus has offered little clarity and left hospitals, like much of the economy, in a free fall.
Many health systems are making direct cuts to their payrolls, eliminating or shrinking performance bonuses and prorating paychecks to mirror reduced workload until operations stabilize.
Scott Weavil, a lawyer in California who counsels physicians and other health care workers on employment contracts, said he was hearing from doctors across the country who were being asked to take pay cuts of 20% to 70%.
The requests are coming from hospital administrators or private physician groups hired by the hospitals, he said, and are essentially new contracts that doctors are being asked to sign.
Many of the contracts do not say when the cuts might end, and are mostly affecting doctors who are not treating coronavirus patients on the front lines, such as urologists, rheumatologists, bariatric surgeons, obstetricians and gynecologists.
Such doctors are still being asked to work — often in a decreased capacity — yet may be risking their health going into hospitals and clinics.
“It’s just not sitting well,” Weavil said, noting that he tells doctors they unfortunately have few options if they want to work for their institution long term.
“If you fight this pay cut, administration could write your name down and remember that forever,” he said he tells them.
In other cases, physicians are continuing to find opportunities to practice in a more limited capacity, like telemedicine appointments. But that has not eliminated steep pay cuts.
“Physicians are only paid in our clinic based on their productivity in the work they do,” said Dr. Pam Cutler, the president of Western Montana Clinic in Missoula. “So they’re automatically taking a very significant — usually greater than 50% or 25% — pay cut just because they don’t have any work.”
In some areas, layoffs have left behind health care workers who worry that they will not be able to find new roles or redeploy their skills.
Cox in Michigan said he was briefly reassigned at his hospital, helping screen and process patients coming in with coronavirus symptoms, but eventually the people seeking reassignments outgrew the number of roles.
He also expressed concern that inevitable changes in the health care industry after the pandemic — paired with the possibility of a lengthy period of unemployment — could make it difficult to get his job back.
“I’m just concerned that the job I got laid off from may not be there when this is over,” Cox said. “The longer you’re away, the more you worry, ‘Am I going to be able to come back?’ So there’s a lot of anxiety about it.”
Even as many of the largest hospital networks grapple with sudden financial uncertainty, much smaller practices and clinics face a more immediate threat.
According to a statistical model produced by HealthLandscape and the American Academy of Family Physicians, by the end of April, nearly 20,000 family physicians could be fully out of work, underemployed or reassigned elsewhere, particularly as cities like New York consider large-scale, emergency reassignments of physicians.
“Many of these smaller practices were living on a financial edge to start with, so they’re not entering into this in a good position at all,” said Dr. Gary Price, the president of the Physicians Foundation. “Their margins are narrower, their patients don’t want to come in, and many of them shouldn’t anyway, so their cash flow has been severely impacted and their overhead really hasn’t.”
Peak demand for hospital resources due to COVID-19 is expected by mid-April in the U.S., according to an analysis from the University of Washington’s Institute for Health Metrics and Evaluation in Seattle.
The study presents estimates of predicted health service utilization and deaths due to COVID-19 for each state in the U.S. if social distancing measures are maintained. Researchers used state-level hospital capacity data, data on confirmed COVID-19 deaths from the World Health Organization, and observed COVID-19 utilization from select locations.
While peak demand for resources, namely hospital beds and ventilators, will occur at the national level in two weeks, this varies by state. About a third of states, including New York, are projected to hit peak capacity in the first half of April, but some states will see the most demand for hospital resources in May.
Below is the projected date of peak hospital resource demand in each state according to the model, which uses data last updated April 1.
April 8 New Jersey
April 9 Louisiana
Michigan
New York
Vermont
April 11 Delaware
Washington
April 15 Alaska
Connecticut
District of Columbia
April 16 Massachusetts
April 17
Alabama
Colorado
Maine
New Hampshire
April 18 Pennsylvania
April 19 Indiana
Ohio
Tennessee
April 20 Illinois
Nevada
Rhode Island
April 21 Mississippi
North Dakota
April 22 Minnesota
April 23 Nebraska
Oklahoma
Utah
April 24 Georgia
New Mexico
April 26 Arkansas
California
Idaho
Montana
North Carolina
Healthcare Dive analyzed data to paint a picture of hospital capacity, pinpointing areas with a higher ratio of people to beds and signaling where there is a risk for capacity issues.
Fewer hospital beds in select regions make them especially vulnerable to the novel coronavirus as it’s expected to spread from big city hot spots to other areas of the country.
As the U.S. has become the next epicenter of the outbreak, hospitals are preparing for the worst. The pathogen threatens to overwhelm their facilities and resources, especially if mitigation efforts fail to blunt a surge of COVID-19 patients.
The latest figures from the Johns Hopkins Coronavirus Resource Center report more than 143,000 confirmed cases in the U.S. and more than 2,500 deaths as of Monday.
The New York City metro area has the most beds compared to the rest of the country. Still, that is not enough capacity to meet the crushing demand.
To illustrate hospital capacity across the country, Healthcare Dive sought to compare bed counts to population, and found population size isn’t always indicative of the number of beds available.
Population size is not always indicative of bed capacity in the top 20 metro areas
Below are the 20 most populated metro areas in the U.S., sorted by population. As you move down the chart, population size decreases, but bed counts do not always. Areas like D.C. and Seattle have fewer beds relative to population size, while Miami and Philadelphia have more beds relative to population.
Some areas like Washington, D.C., have relatively fewer beds compared to their population, while others like Miami, Philadelphia and St. Louis have more beds relative to the number of people in the region.
Some hospitals are turning to hotels and tents, and Vice President Mike Pence has said he’s working with the Department of Defense to get field hospitals and other options online.
Still, researchers cautioned there is a long way to go to meet projected demands. If America’s healthcare system was able to free up half of its beds by discharging patients, the country would still need three times as many beds, Ashish Jha, director of the Harvard Global Health Institute, told reporters during a call on Tuesday. That projection assumes 40% of Americans get infected over the next six months.
“What we know right now is that capacity to manage patients varies dramatically from community to community,” Jha said.
Areas with the highest ratio of people per bed
To paint a picture of hospital capacity across the country, Healthcare Dive used CMS cost reports and population data to calculate the ratio of people per bed in metropolitan areas and regions. In other words, how many residents are there for a single bed? It’s a way to pinpoint areas with a higher ratio of people to beds, signaling areas potentially at risk for capacity issues.
HOW HEALTHCARE DIVE ANALYZED HOSPITAL BED COUNTS
Hospitals certified by Medicare are required to submit annual cost reports to CMS, which include a vast array of information from bed counts to financials. Hospital beds analyzed in this report do not include all the beds a hospital may have reported to CMS.
Healthcare Dive excluded nursery, labor and delivery beds and psychiatric hospitals. In addition, due to the inconsistent reporting in ICU beds, Healthcare Dive did not highlight areas with higher ratios of people per ICU bed. It’s also important to note that some hospitals may have opened or closed since these latest CMS cost reports were published.
Healthcare Dive analyzed specific geographic areas, in this case metropolitan CBSAs, or core-based statistical areas, which are geographic areas that consist of an urban center of 50,000 people or more.
In the U.S., about 42% of the more than 143,000 cases are concentrated in New York, overwhelming available resources. Still, case counts are swelling in areas outside of New York including Chicago, Detroit and New Orleans. Indicating the outbreak is likely to be widespread in America.
Healthcare Dive found the Bloomsburg-Berwick, Pennsylvania, area has the lowest ratio in the nation with 86 people for each bed. Most areas have much higher ratios, the median being around 400 people per bed when comparing CBSAs. The metro area of New York City sits in the middle with 405 people per bed.
The Greeley, Colorado area has the nation’s highest ratio of people per bed, according to the data. About 60 miles northeast of Denver and with a population of more than 314,000, there are 1,397 people for every one hospital bed in the Greeley area.
The CMS data shows a total of 225 hospital beds in the Greeley area, operated by Banner Health’s North Colorado Medical Center.
However, a new 50-bed hospital opened recently and was not included in the most recent cost reports. It is operated by UCHealth.
Still, while those numbers may seem grim, Colorado’s hospital leaders cautioned that the state can and is working to tap into additional resources, citing freestanding emergency rooms and ambulatory surgical centers.
It’s imperative to look beyond just one locale or one hospital and consider the resources of the state as a whole, Colorado’s hospital leaders told Healthcare Dive.
Colorado has a total of 10,293 hospital beds (12,558 licensed beds) and at least 973 ICU beds, the Colorado Hospital Association said.
“It’s going to take the whole system for us to get through this,” Julie Lonborg, senior vice president at the Colorado Hospital Association, told Healthcare Dive.
There are only one or two hospitals in almost all of the 10 regions with the highest ratio of people per bed. Rounding out the top 10 areas with the highest ratio of people per bed following Greeley, include Albany, Oregon; Gettysburg, Pennsylvania; Merced, California; California-Lexington Park, Maryland; Bremerton-Silverdale, Washington; Lawrence, Kansas; Monroe, Michigan; Provo-Orem, Utah; and Ogden-Clearfield, Utah.
The data shows the total bed capacity in a region, but does not take into account the patients currently occupying those beds. However, in an effort to free up existing beds, many hospitals have halted elective surgeries, including in Greeley to free up resources and staff to be able to respond to a potential surge.
“UCHealth Greeley Hospital is caring for a large number of patients at this time, and by working together as a large system, UCHealth is able to redirect patients and admissions to other facilities to help even out our capacities at this and other hospitals,” Kelly Tracer, a spokesperson for the hospital, told Healthcare Dive.
In fact, many hospitals plan to lean on the larger systems they’re a part of to shuffle resources to respond to the pandemic.
In Gettysburg, Pennsylvania, there are 76 hospital beds and 1,353 people per hospital bed. WellSpan Health, which operates Gettysburg Hospital, said it plans to coordinate its response by using its eight other hospitals in different areas and some 200 locations.
“We are taking a comprehensive approach to this issue, developing a network of more than 10 outdoor testing locations across our five-county region and temporarily repurposing several of our outpatient medical practices to care locations dedicated solely for the treatment of patients who are suspected or confirmed to have COVID-19 and have non-emergency medical needs,” according to a statement WellSpan Health provided Healthcare Dive.
Other locations with the highest people per bed ratio are converting existing space into dedicated areas to treat COVID-19 patients to prepare for a crush of patients, including in Lawrence, Kansas, with 893 people for every bed.
Lawrence Memorial Hospital in Lawrence, Kansas, about 40 miles west of Kansas City, is prepared to up its capacity to 205, LMH said in a statement. The hospital reported 136 beds to CMS but said it is licensed for 174.
“At any given time we have upwards of 100 patients,” Traci Hoopingarner, vice president of clinical care and chief nursing officer for LMH Health, said in a statement.
As New York continues to grapple with mounting cases, leaders are issuing dire warnings to the rest of the country.
“New York is the canary in the coal mine.What happens to New York is going to wind up happening in California and Washington state and Illinois. It’s just a matter of time,” New York Gov. Andrew Cuomo said.
Below is an interactive table of hospital bed availability in different metros across the country. Search for your metro area to find the corresponding hospital capacity.













:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19782413/Covid_19_CFR_by_age_vs._US_Seasonal_Flu_3.png)

