At a recent health system physician leadership retreat, two cardiologists presented a fascinating update on the electrophysiology (EP) service line. Electrophysiologists use advanced heart mapping and ablation technologies to diagnose, pinpoint, and treat abnormal heart rhythms, and the field has made dramatic advances over the past decade. The success rate of interventions has risen, and procedures which used to take hours in a cath lab are now performed in a fraction of the time—with some patients even able to go home same-day.
This increased efficiency has expanded the EP program’s capacity, but the system still finds itself overwhelmed with demand. The system is located in a high-growth market, and demand is also fueled by shifting demographics, with more aging Baby Boomers seeking care. But a key driver of growthhas been the spread of “smart watches” like the Apple Watch and Fitbit, which tout the ability to detect abnormal heart rhythms like atrial fibrillation. With “half of the community walking around with an EKG on their wrist”, the number of patients seeking evaluations for “a-fib” has skyrocketed: at this system, over 50 percent growth in patient volume, leading to 25 jump in procedures during the pandemic.
While the doctors were excited about growth, they also stressed the need to rethink care pathways to make sure that electrophysiologists’ time was prioritized for the patients who needed it most. The system should look to develop care pathways and technology that enable other physicians to readily triage and manage routine atrial fibrillation.
But smartwatch-driven self-diagnosis raises larger questions about how doctors and hospitals must adapt when consumer technology outpaces the science evaluating its effectiveness, and the health system’s ability to meet new demand. With private equity firms now focused on acquiring cardiology practices, this massive spike of demand, coupled with the ability to move more heart rhythm procedures outpatient, is seen by investors as a significant profit opportunity—making it even more critical for doctors, researchers, and hospitals to ensure that sound clinical guidelines are developed to drive high-quality, appropriate management.
Hospitals are experiencing significant increases in expenses for workforce, drugs and medical supplies
Introduction
For over two years since the outset of the COVID-19 pandemic, America’s hospitals and health systems have been on the front lines caring for patients, comforting families and protecting communities.
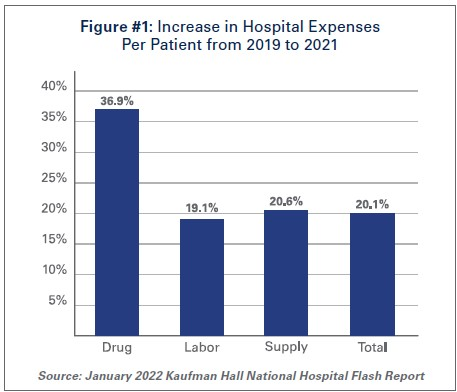
With over 80 million cases1, nearly 1 million deaths2, and over 4.6 million hospitalizations3, the pandemic has taken a significant toll on hospitals and health systems and placed enormous strain on the nation’s health care workforce. During this unprecedented public health crisis, hospitals and health systems have confronted many challenges, including historic volume and revenue losses, as well as skyrocketing expenses (See Figure #1).
Hospitals and health systems have been nimble in responding to surges in COVID-19 cases throughout the pandemic by expanding treatment capacity, hiring staff to meet demand, acquiring and maintaining adequate supplies and personal protective equipment (PPE) to protect patients and staff and ensuring that critical services and programs remain available to the patients and communities they serve. However, these and other factors have led to billions of dollars in losses over the last two years for hospitals, and over 33% of hospitals are operating on negative margins.
The most recent surges triggered by the delta and omicron variants have added even more pressure to hospitals. During these surges, hospitals saw the number of COVID-19 infected patients rise while other patient volumes fell, and patient acuity increased. This drove up expenses and added significant financial pressure for hospitals. Moreover, hospitals did not receive any government assistance through the COVID-19 Provider Relief Fund (PRF) to help mitigate rising expenses and lost revenues during the delta and omicron surges. This is despite the fact that more than half of COVID-19 hospitalizations have occurred since July 1, 2021, during these two most recent COVID-19 surges.
At the same time, patient acuity has increased, as measured by how long patients need to stay in the hospital. The increase in acuity is a result of the complexity of COVID-19 care, as well as treatment for patients who may have put off care during the pandemic. The average length of a patient stay increased 9.9% by the end of 2021 compared to pre-pandemic levels in 2019.4
As hospitals treat sicker patients requiring more intensive treatment, they also must ensure that sufficient staffing levels are available to care for these patients, and must acquire the necessary expensive drugs and medical supplies to provide high-quality care. As a result, overall hospital expenses have experienced considerable growth.
Data from Kaufman Hall, a consulting firm that tracks hospital financial metrics, shows that by the end of 2021, total hospital expenses were up 11% compared to pre-pandemic levels in 2019. Even after accounting for changes in volume that occurred during the pandemic, hospital expenses per patient increased significantly from pre-pandemic levels across every category. (See Figure #1)
The pandemic has strained hospitals’ and health systems’ finances. Many hospitals operate on razorthin margins, so even slight increases in expenses can have dramatic negative effects on operating margins, which can jeopardize their ability to care for patients. These expense increases have been more challenging to withstand in light of rising inflation and growth in input prices. In fact, despite modest growth in revenues compared to pre-pandemic levels, median hospital operating margins were down 3.8% by the end of 2021 compared to pre-pandemic levels, according to Kaufman Hall. Further exacerbating the problem for hospitals are Medicare sequestration cuts and payment increases that are well below increases in costs. For example, an analysis by PINC found that for fiscal year 2022, hospitals received a 2.4% increase in their Medicare inpatient payment rate, while hospital labor rates increased 6.5%.5
These levels of increased expenses and declines in operating margins are not sustainable. This report highlights key pressures currently facing hospitals and health systems, including:
Each of these issues separately presents significant challenges to the hospital field. Taken together, they represent conditions that would be potentially catastrophic for most organizations, institutions and industries. However, the fact that the nation’s hospitals and health systems continue to serve on the front lines of the ongoing pandemic is a testament to their resiliency and steadfast commitment to their mission to serve patients and communities around the country.
Hospitals and health systems are the cornerstones of their communities. Their patients depend on them for access to care 24 hours a day, seven days a week. Hospitals are often the largest employers in their community, and large purchasers of local services and goods. Additional support is needed to help ensure hospitals have the adequate resources to care for their communities.
I. Workforce and Contract Labor Expenses
The hospital workforce is central to the care process and often the largest expense for hospitals. It is no surprise then that even before the pandemic, labor costs — which include costs associated with recruiting and retaining employed staff, benefits and incentives — accounted for more than 50% of hospitals’ total expenses. Therefore, even a slight increase in these costs can have significant impacts on a hospital’s total expenses and operating margins.
As the pandemic has persisted for over two years, the toll on the health care workforce has been immense. A recent survey of health care workers found that approximately half of respondents felt “burned out” and nearly a quarter of respondents said they anticipated leaving the health care field.6
This has been mirrored by a significant and sustained decline in hospital employment, down approximately 100,000 employees from pre-pandemic levels.7 At the height of the omicron surge, approximately 1,400 hospitals or 30% of all U.S. hospitals reporting data to the government, indicated that they anticipated a critical staffing shortage within the week.8This high percentage of hospitals reporting a critical staffing shortage stayed relatively consistent throughout the delta and omicron surges.
The combination of employee burnout, fewer available staff, increased patient acuity and higher demand for care especially during the delta and omicron surges, has forced hospitals to turn to contract staffing firms to help address staffing shortages.
Though hospitals have long worked with contract staffing firms to bridge temporary gaps in staffing, the pandemic-driven-staffing-shortage has created an expanded reliance on contract staff, especially contract or travel registered nurses. Travel nurses are in particularly high demand because they serve a critical role in delivering care for both COVID-19 and non-COVID-19 patients and allow the hospital to meet the demand for care, especially during pandemic surges.
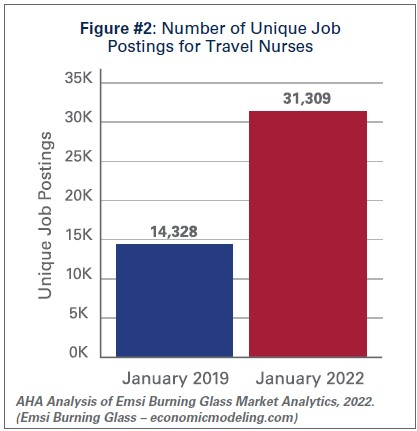
According to a survey by AMN Healthcare, one of the nation’s largest health care staffing agencies, 95% of health care facilities reported hiring nurse staff from contract labor firms during the pandemic.9Staffing firms have increased their recruitment of contract or travel nurses, illustrating the significant growth in their demand. According to data from EMSI/Burning Glass, there has been a nearly 120% increase in job postings for contract or travel nurses from pre-pandemic levels in January 2019 to January 2022. (See Figure #2)
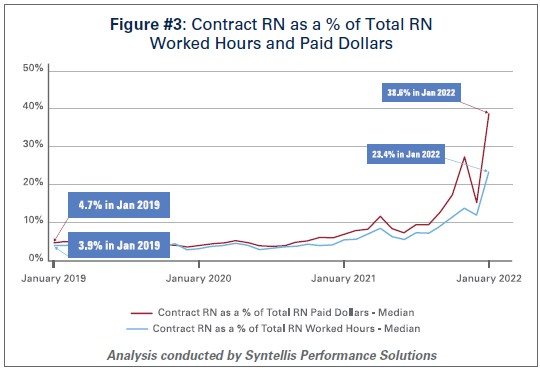
Similarly, the hours worked by contract or travel nurses as a percentage of total hours worked by nurses in hospitals has grown from 3.9% in January 2019 to 23.4% in January 2022, according to data from Syntellis Performance Solutions. (See Figure #3) In fact, a quarter of hospitals have experienced nearly a third of their total nurse hours accounted for by contract or travel nurses.
As the share of contract travel nurse hours has grown significantly compared to before the pandemic, so too have the costs of employing travel nurses compared to pre-pandemic levels. In 2019, hospitals spent a median of 4.7% of their total nurse labor expenses for contract travel nurses, which skyrocketed to a median of 38.6% in January 2022. (See Figure #3) A quarter of hospitals — those who have had to rely disproportionately on contract travel nurses — saw their costs for contract travel nurses account for over 50% of their total nurse labor expenses. In fact, while contract travel nurses accounted for 23.4% of total nurse hours in January 2022, they accounted for nearly 40% of the labor expenses for nurses. (See Figure #3) This difference has grown considerably compared to pre-pandemic levels in 2019, suggesting that the exorbitant prices charged by staffing companies are a primary driver of higher labor expenses for hospitals.
Data from Syntellis Performance Solutions show a 213% increase in hourly rates charged to hospitals by staffing companies for travel nurses in January 2022 compared to pre-pandemic levels in January 2019. This is because staffing agencies have exploited the situation by increasing the hourly rates billed to hospitals for contract travel nurses more than the hourly rates they pay to travel nurses. This is effectively the “margin” retained by the staffing agencies. During pre-pandemic levels in 2019, the average “margin” retained by staffing agencies for travel nurses was about 15%. As of January 2022, the average “margin” has grown to an astounding 62%. (See Figure #4)
These high “margins” have fueled massive growth in the revenues and profits of health care staffing companies. Several staffing firms have reported significant growth in their revenues to as high as $1.1 billion in just the fourth quarter of 202110, tripling their revenues and net income compared to 2020 levels.11
The data indicate that the growth in labor expenses for hospitals and health systems was in large part due to the exorbitant rates charged by contract staffing firms. By the end of 2021, hospital labor expenses per patient were 36.9% higher than pre-pandemic levels, and increased to 57% at the height of the omicron surge in January 2022.12 A study looking at hospitals in New Jersey found that the increased labor expenses for contract staff amounted to $670 million in 2021 alone, which was more than triple what their hospitals spent in 2020.13High reliance on contract or travel staff prevents hospitals and health systems from investing those costs into their existing employees, leading to low morale and high turnover, which further exacerbates the challenges hospitals and health systems have been facing.
II. Drug Expenses
Prescription drug spending in the U.S. has grown significantly since the pandemic. In 2021, drug spending (including spending in both retail and non-retail settings) increased 7.7%14, which was on top of an increase of 4.9%15 in 2020. While some of this growth can be attributed to increased utilization as patient acuity increased during the pandemic, a significant driver has been the continued increase in prices of existing drugs as well as the introduction of new products at very high prices. A study by GoodRx found that in January 2022 alone, drug companies increased the price of about 810 brand and generic drugs that they reviewed by an average of 5.1%.16 These price increases followed massive price hikes for certain drugs often used in the hospital such as Hydromorphone (107%), Mitomycin (99%), and Vasopressin (97%).17 For another example, the drug manufacturer of Humira, one of the most popular brand drugs used to treat rheumatoid arthritis, increased the price of the drug by 21% between 2019 and 2021.18 A study by the Kaiser Family Foundation found that in Medicare Part B and D markets, half of all drugs in each market experienced price increases above the rate of inflation between 2019 and 2020 – in fact, a third of these drugs experienced price increases of greater than 7.5%.19 At the same time, according to a report by the Institute for Clinical and Economic Review (ICER), eight drugs with unsupported U.S. drug price increases between 2019 and 2020 alone accounted for an additional $1.67 billion in drug spending, further illustrating that drug companies’ decisions to raise the prices of their drugs are simply an unsustainable practice.20
As hospitals have worked to treat sicker patients during the pandemic, they have been forced to contend with sky-high prices for drugs, many of which are critical and lifesaving for their patients. For example, in 2020, 16 of the top 25 drugs by spending in Medicare Part B (hospital outpatient settings) had price increases greater than inflation — two of the top three drugs, Keytruda and Prolia — experienced price increases of 3.3% and 4.1%, respectively.21
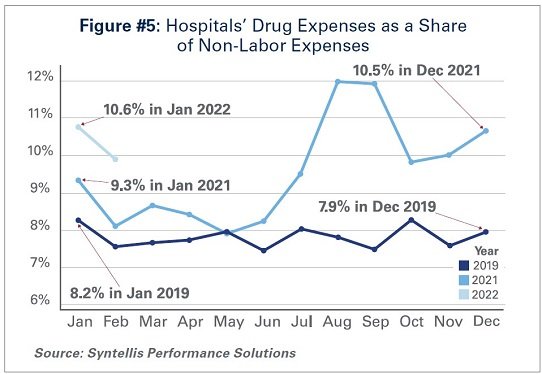
As a result of these price increases, hospital drug expenses have skyrocketed. By the end of 2021, total drug expenses were 28.2% higher than pre-pandemic levels.22 When taken as a share of all non-labor expenses, drug expenses have grown from approximately 8.2% in January 2019, to 9.3% in January 2021, and to 10.6% in January 2022. (See Figure #5) Even when considering changes in volume during the pandemic, drug expenses per patient compared to pre-pandemic levels in 2019 saw significant increases, with a 36.9% increase through 2021.
While continued drug price increases by drug companies have been a major driver of the growth in overall hospital drug expenses, there also are other important driving factors to consider:
Drug Treatments for COVID-19 Patients:Remdesivir, one of the primary drugs used to treat COVID-19 patients in the hospital, has become the top spend drug for most hospitals since the pandemic. This drug alone accounted for over $1 billion in sales in the fourth quarter of 2021.23 Priced at an average of $3,12024, Remdesivir’s cost was initially covered by the federal government. However, hospitals must now purchase the drug directly.
Limitation of 340B Contract Pharmacies: The 340B program allows eligible providers, including hospitals that treat many low-income patients or treat certain patient populations like children and cancer patients, to buy certain outpatient drugs at discounted prices and use those savings to provide more comprehensive services to the patients and communities they serve. Since July 2020, several of the largest drug manufacturers have denied 340B pricing to eligible hospitals through pharmacies with whom they contract, despite calls from the Department of Health and Human Services that such actions are illegal. Because of these actions, many 340B hospitals, especially rural hospitals who disproportionately rely on contract pharmacies to ensure access to drugs for their patients, have lost millions in 340B drug savings.25 In addition, these manufacturers have required claim-level data submissions as a condition of receiving 340B discounts, which has increased costs to deliver the data as well as staff time and expense to manage that process. The loss of 340B savings coupled with increased burden of providing detailed data to drug companies have contributed to increasing drug expenses.
Health Plans’/Pharmacy Benefit Managers’ (PBMs’) “White Bagging” Policies: Health plans and PBMs have engaged in a tactic that steers hospital patients to third-party specialty pharmacies to acquire medication necessary for clinician-administered treatments, known as “white-bagging.” This practice disallows the hospital from procuring and managing the handling of a drug — typically drugs that are infused or injected requiring a clinician to administer in a hospital or clinic setting — used in patient care. These policies not only create serious patient safety concerns, but create delays and risks in patient care; add to administration, storage and handling costs; and create important liability issues for hospitals.
Taken together, these factors increase both drug expenses and overall hospital expenses.
III. Medical Supply and PPE Expenses
The U.S., like most countries in the world, relies on global supply chains for goods and services. This is especially true for medical supplies used at hospitals and other health care settings. Everything from the masks and gloves worn by staff to medical devices used in patient care come from a large network of global suppliers. Prior to the global pandemic, hospitals had established relationships with distributors and other vendors in the global health care supply chain to deliver goods as necessitated by demand. After the pandemic hit, many factories, distributors and other vendors shut down their operations, leaving hospitals, which were on the front lines facing surging demand, to fend for themselves. In fact, supply chain disruptions across industries, including health care, increased by 67% in 2020 alone.26
As a result, hospitals turned to local suppliers and non-traditional suppliers, often paying significantly higher rates than they did prior to the pandemic. Between fall 2020 and early 2022 costs for energy, resins, cotton and most metals surged in excess of 30%; these all are critical elements in the manufacturing of medical supplies and devices used every day in hospitals.27 As COVID-19 cases surged, demand for hospital PPE, such as N95 masks, gloves, eye protection and surgical gowns, increased dramatically causing hospitals to invest in acquiring and maintaining reserves of these supplies. Further, downstream effects from other global events such as the war in Ukraine and the energy crisis in China, as well as domestic issues, such as labor shortages and rising fuel and transportation costs, have all contributed to drive up even higher overall medical supply expenses for hospitals in the U.S.28 For instance, according to the Health Industry Distributors Association, transportation times for medical supplies are 440% longer than pre-pandemic times resulting in massive delays.29
Compared to 2019 levels, supply expenses for hospitals were up 15.9%30 through the end of 2021. When focusing on hospital departments involved most directly in care for COVID-19 patients − primarily hospital intensive care units (ICUs) and respiratory care departments − the increase in expenses is significantly higher. Medical supply expenses in ICUs and respiratory care departments increased 31.5% and 22.3%, respectively. Further, accounting for changes in volume during surge and non-surge periods of the pandemic, medical supply expenses per patient in ICUs and respiratory care departments were 31.8% and 25.9% higher, respectively. (See Figure #6) These numbers help illustrate the magnitude of the impact that increases in supply costs have had on hospital finances during the pandemic.
IV. Impact of Rising Inflation
Higher economy-wide costs have serious implications for hospitals and health systems, increasing the pressures of higher labor, supply, and acquisition costs; and potentially lower consumer demand. Inflation is defined as the general increase in prices and the decrease in purchasing power. It is measured by the Consumer Price Index (CPI-U). In April 2021, the Bureau of Labor Statistics (BLS) reported that the CPI-U had the largest 12-month increase since September 2008. The CPI-U hit 40-year highs in February 2022.31 Overall, consumer prices rose by a historic 8.5% on an annualized basis in March 2022 alone.32
As inflation measured by consumer prices is at record highs, below are key considerations on the potential impact of higher general inflation on hospital prices:
Labor Costs and Retention: Labor costs represent a significant portion of hospital costs (typically more than 50% of hospital expenses are related to labor costs). As the cost-of-living increases, employees generally demand higher wages/total compensation packages to offset those costs. This is especially true in the health care sector, where labor demands are already high, and labor supply is low.
Supply Chain Costs: Medical supplies account for approximately 20% of hospital expenses, on average. As input/raw good costs increase due to general inflation, hospital supplies and medical device costs increase as well. Furthermore, shortages of raw materials, including those used to manufacture drugs, could stress supply chains (i.e., medical supply shortages), which may result in changes in care patterns and add further burden on staff to implement work arounds.
Capital Investment Costs: Capital investments also may be strained, especially as hospitals have already invested heavily in expanding capacity to treat patients during the pandemic (e.g., constructing spaces for testing and isolation of COVID-19 patients). One of the areas that has seen the largest increase in prices/shortages is building materials (e.g., lumber). Additionally, a historically large increase in inflation has resulted in increases in interest rates, which may hamper borrowing options and add to overall costs.
Consumer Demand: Higher inflation also may result in decreases in demand for health care services, specifically if inflation exceeds wage growth. Specifically, higher costs for necessities (food, transportation, etc.) could push down demand for health care services and, in turn, dampen hospital volumes and revenues in the long run.
Health care and hospital prices are not driving recent overall inflation increases. The BLS has cited increases in the indices for gasoline, shelter and food as the largest contributors to the seasonally adjusted all items increase. The CPI-U increased 0.8% in February on a seasonally adjusted basis, whereas the medical care index rose 0.2% in February. The index for prescription drugs rose 0.3%, but the hospital index for hospital services declined 0.1%.33
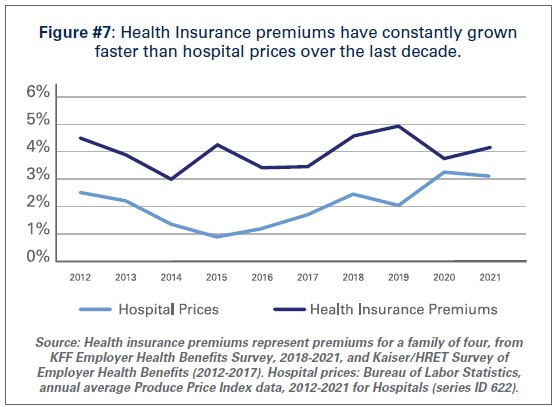
This is consistent with pre-pandemic trends. Despite persistent cost pressures, hospital prices have seen consistently modest growth in recent years. According to BLS data, hospital prices have grown an average 2.1% per year over the last decade, about half the average annual increase in health insurance premiums. (See Figure #7) More recently, hospital prices have grown much more slowly than the overall rate of inflation. In the 12 months ending in February 2022, hospital prices increased 2.1%. In fact, even when excluding the artificially low rates paid to hospitals by Medicare and Medicaid, average annual price growth has still been below 3% in recent years.34
Conclusion
While we hope that our nation is rounding the corner in the battle against COVID-19, it is clear that the pandemic is not over. During the week of April 11, there have been an average of over 33,000 cases per day35 and reports suggest that a new subvariant of the virus (Omicron BA.2) is now the dominant strain in the U.S.36As a result, the challenges hospitals and health systems are currently facing are bound to last much longer.
As COVID-19 infections and hospitalizations are decreasing in some parts of the U.S. and increasing in others, hospitals and health systems continue to care for COVID-19 and non-COVID-19 patients. With additional surges potentially on the horizon, the massive growth in expenses is unsustainable. Most of the nation’s hospitals were operating on razor thin margins prior to the pandemic; and now, many of these hospitals are in an even more precarious financial situation. Regardless of potential new surges of COVID-19, hospitals and health systems continue to face workforce retention and recruitment challenges, supply chain disruptions and exorbitant expenses as outlined in this report.
Hospitals appreciate the support and resources that Congress has provided throughout the pandemic; however, additional support is needed now to keep hospitals strong so they can continue to provide care to patients and communities.
Hospitals and health systems have lost billions over the last two years, leaving more than 33 percent of them with negative margins, according to an April 25 report by the American Hospital Association.
Six findings:
1. Employment is down by 100,000 jobs compared to pre-pandemic levels, the U.S. Bureau of Labor Statistics found. But at a time when hospitals are desperately trying to fill positions, labor expenses per patient were 19.1 percent higher in 2021 than in 2019. Labor expenses are more than 50 percent of hospitals’ total expenses, meaning a small increase in labor costs can have a major effect on hospital’s total expenses and operating margins.
2. The report attributed the increase in labor expenses to hospitals’ dependence on contract staff, specifically nurses. In 2019, travel nurses accounted for a median of 4.7 percent of hospitals’ total nurse labor expenses, compared to a median of 38.6 percent in January.
3. Hourly billing rates for contract employees rose 213 percent compared to pre-pandemic levels. This created a 62 percent profit margin for staff agencies.
4. Drug expenses soared by 36.9 percent per patient compared to pre-pandemic levels.
5. Medical supply expenses also rose through 2021, by 20.6 percent, compared to pre-pandemic levels. For intensive care units and respiratory care departments — which were most involved in COVID-19 care — medical supply expenses grew 31.5 percent and 22.3 percent, respectively.
6. Economywide, the consumer price index saw major increases, the Bureau of Labor Statistics found. Meanwhile, hospital prices rose modestly, by an average of 2.1 percent per year in the last decade, about half the average annual increase in health insurance premiums.
Several hospitals are scaling back inpatient services or ending inpatient care.
Below are seven hospitals that announced plans to scale back or end inpatient care since February.
1. Marietta, Ga.-based WellStar Health System is closing the emergency department and ending inpatient care at Atlanta Medical Center South in May. The hospital will be converted into an outpatient site, and inpatient services will be consolidated to Atlanta Medical Center’s main campus, Wellstar said.
2. Tampa, Fla.-based Shriners Hospitals for Children is ending inpatient care at its campus in Springfield, Mass. The hospital gave the Massachusetts Department of Public Health a 120-day notice of the plan on March 31.
3. Kanakanak Hospital in Dillingham, Alaska, stopped accepting inpatient admissions April 8 because of a staffing shortage. The hospital’s owner said it expects to resume accepting inpatients again on May 1.
4. Boston-based Tufts Children’s Hospital is closing its pediatric inpatient units in July to convert its 41 pediatric inpatient beds to adult ICU and medical/surgical beds. Tufts will refer children to Boston Children’s Hospital for care.
5. Henrico Doctors’ Hospital in Richmond, Va., ended pediatric inpatient services April 1. The hospital attributed the decision in part to a low number of patients. The hospital said it’s seeing an increased demand for adult inpatient medical and surgical care. Although the pediatric units are closing, the hospital will continue to provide emergency medical care to children via designated emergency room space.
6. Mercyhealth ended inpatient care at Javon Bea Hospital-Rockton in Rockford, Ill., and transitioned it to an outpatient facility in March. Inpatient services were consolidated to Javon Bea Hospital-Riverside in Rockford. Javon Bea Hospital-Rockton offers outpatient services, including cancer care, pain management, outpatient surgery and pediatrics.
7. Ascension St. John Medical Center plans to close its pediatric intensive care and general pediatric inpatient care unit at the end of April. The Tulsa, Okla.-based hospital said the decision was based on a community needs assessment and analysis of services offered in the community. Pediatric ambulatory, surgical and neonatal ICU services will not be affected, the hospital said.
Changes are coming to Washington’s state charity care law July 1.
Four things to know:
1. The new law establishes mandatory discount standards for patients from 101 percent to 200 percent of the federal poverty level, according to the Washington State Hospital Association.
2. It establishes two tiers of hospitals and establishes mandated free and discounted care for each based on a patient’s family size and income relative to the federal poverty level, according to the association. Tier 1 includes hospitals that are part of larger systems. Tier 2 includes smaller, independent, and rural hospitals.
3. Hospitals must adopt procedures to identify patients eligible for retroactive Medicaid eligibility and assist them in applying for coverage, according to the association. Hospitals are not required to provide charity care to patients who do not make reasonable efforts to comply with the application process.
4. The law establishes a definition of “indigent persons” who may qualify for charity care, according to the Washington State Hospital Association. It specifies that indigent persons are those who meet the federal poverty level thresholds and have exhausted any third-party coverage.
Stanford Health Care and Lucile Packard Children’s Hospital administrators have notified union leaders that its nurse members who strike later in April risk losing pay and health benefits, according to Palo Alto Weekly.
The Committee for Recognition of Nursing Achievement, a union at Stanford Health Care and Stanford Children’s Health that represents about 5,000 nurses, has scheduled a strike to begin April 25. The nurses’ contract expired March 31.
If the strike moves forward, Stanford Health Care and the Lucile Packard Children’s Hospital, both based in Palo Alto, Calif., are prepared to continue to provide safe, quality healthcare, according to a statement from Dale Beatty, DNP, RN, chief nurse executive and vice president of patient care services for Stanford Health Care, and Jesus Cepero, PhD, RN, senior vice president of patient care and chief nursing officer for Stanford Children’s Health.
But the statement, which was shared with Becker’s, said nurses who choose to strike will not be paid for shifts they miss.
“In addition, employer-paid health benefits will cease on May 1 for nurses who go out on strike and remain out through the end of the month in which the strike begins,” Drs. Beatty and Cepero said.
The leaders quoted from Committee for Recognition of Nursing Achievement’s “contingency manual” that the union provided to nurses: “If a strike lasts beyond the end of the month in which it begins and the hospitals discontinue medical coverage, you will have the option to pay for continued coverage.”
Drs. Beatty and Cepero said nurses who strike may pay to continue their health coverage through the Consolidated Omnibus Budget Reconciliation Act.
In a separate statement shared with Becker’s, Committee for Recognition of Nursing Achievement President Colleen Borges called Stanford and Packard management’s move regarding nurses’ health benefits “cruel” and “immoral.”
“Health benefits should not be used against workers, especially against the very healthcare professionals who have made Stanford a world-class health system,” said Ms. Borges, who is also a pediatric oncology nurse at Lucile Packard Children’s Hospital. “We have spent our careers caring for others and putting others first — now more than ever we need solutions that will ensure sustainability, safe staffing and strong benefits to retain nurses. But instead of taking our proposals seriously, hospitals are spending their time and energy weaponizing our medical benefits. We refuse to be intimidated from standing up for the fair contracts that we need in order to continue delivering world-class patient care.”
The union has organized a petition to tell Stanford not to cut off medical benefits for nurses and their families during the strike. As of April 19, the petition had more than 25,150 signatures.
Sacramento-based Sutter Health said nurses who went on strike April 18 will not be allowed to return to work until the morning of April 23, the San Francisco Chronicle reported.
The strike affected nurses and healthcare workers at Sutter Health facilities in Northern California. The nurses are members of the California Nurses Association, and the other workers are members of the Caregivers and Healthcare Employees Union, an affiliate of the California Nurses Association.
More than 8,000 registered nurses and healthcare workers were expected to participate in the strike, according to an April 18 news release from the unions.
In a statement shared with Becker’s, Sutter Health said the organization conducted strike contingency planning, which included “securing staff to replace nurses who have chosen to strike, and those replacement contracts provide the assurance of five days of guaranteed staffing amid the uncertainty of a widespread work stoppage.”
“As always, our top priority remains safe, high-quality patient care and nurses may be reinstated sooner based on operational and patient care needs,” the statement said.
The California Nurses Association described Sutter Health’s decision as retaliatory, as well as “completely unnecessary and vindictive.”
“Nurses who are regularly scheduled to work during this lockout period will lose those days of pay,” the union said in a statement shared with Becker’s. “We urge Sutter to respect the nurses’ strike and let all nurses return to work.”
Sutter Health workers authorized a strike in March, and union officials announced an official strike notice April 8. Union members cited lack of transparency about the stockpile of personal protective equipment supplies and contact tracing as a reason for the strike. They also said they seek a contract that will help retain experienced nurses and provide sufficient staffing and training.
Nurses have been in contract negotiations since June.
Livonia, Mich.-based Trinity Health and Chicago-based CommonSpirit Health have signed an agreement for Trinity to acquire all MercyOne Health System assets and facilities.
Clive, Iowa-based MercyOne has 16 medical centers, 27 affiliate organizations and more than 420 care sites, according to a joint news release. It employs more than 20,000 people.
Trinity and CommonSpirit decided it would be best for MercyOne and the communities it serves for it to have a sole parent company, according to the news release. MercyOne facilities will transition to Trinity’s strategies and operations.
The transaction is expected to be finalized this summer.
“True to our shared Catholic mission, our goal is to provide high-quality, compassionate care with the best patient/member experience possible. We will accomplish that goal through a holistic approach, with a range of health services and technologies that are fully connected and coordinated,” Mike Slubowski, president and CEO of Trinity Health, said in the news release. “This agreement creates a fully integrated MercyOne to care for more people in a unified way.”
Tampa, Fla.-based Shriners Hospitals for Children is transitioning its Springfield, Mass., campus into an outpatient clinic model, NBC/CW affiliate WWLP reported April 20.
Current outpatient services won’t be affected, except that ambulatory surgery will end.
The hospital gave the Massachusetts Department of Public Health a 120-day notice of the plan on March 31, Western Mass News reported April 20.
“The advancement of surgical procedures has resulted in very few patients requiring admission for inpatient pediatric services, which are the cornerstone of a hospital facility,” Shriners said in a letter obtained by Western Mass News. “Accordingly, after evaluating the needs of our patients, we have determined that Shriners Hospitals for Children may best serve our patients and fulfill our charitable mission by transitioning this location from a hospital to an outpatient clinic model.”
Here are 16 hospitals and health health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings, Moody’s Investors Service and S&P Global Ratings.
1. Morristown, N.J.-based Atlantic Health System has an “Aa3” rating and stable outlook with Moody’s. The health system has strong operating performance and liquidity metrics, Moody’s said. The credit rating agency expects Atlantic Health System to sustain strong performance to support capital spending.
2. Children’s Hospital of Akron (Ohio) has an “AA-” rating and stable outlook with Fitch. The hospital has strong operating performance and a leading market position as Akron’s only standalone pediatric hospital, Fitch said. The credit rating agency expects the organization’s strong profitability and limited capital needs to lead to liquidity growth.
3. Milwaukee-based Children’s Wisconsin has an “Aa3” rating and stable outlook with Moody’s. The health system has a leading statewide market share for children’s healthcare services, solid cash flow, strong revenue growth and a robust balance sheet, Moody’s said. The credit rating agency expects Children’s Wisconsin’s balance sheet and debt metrics to remain strong.
4. Greensboro, N.C.-based Cone Health has an “AA” rating and stable outlook with Fitch. The health system has a leading market share and a favorable payer mix, Fitch said. The health system’s broad operating platform and strategic capital investments should enable it to return to stronger operating results, the credit rating agency said.
5. El Camino Health has an “AA-” rating and stable outlook with Fitch. El Camino Health, which includes hospital campuses in Los Gatos, Calif., and Mountain View, Calif., has a solid market share in a competitive market and a stable payer mix, Fitch said. The credit rating agency said El Camino Health’s balance sheet provides moderate financial flexibility.
6. Falls Church, Va.-based Inova Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has a consistently strong operating cash flow margin and ample balance sheet resources, Moody’s said. Inova’s financial excellence will remain undergirded by its favorable regulatory and economic environment, the credit rating agency said.
7. Mass General Brigham has an “Aa3” rating and stable outlook with Moody’s and an “AA-” rating and stable outlook with S&P. The Boston-based health system has an excellent clinical reputation, good financial performance and strong balance sheet metrics, Moody’s said. The credit rating agency said it expects Mass General Brigham to maintain a strong market position and stable financial performance.
8. Rochester, Minn.-based Mayo Clinic has an “Aa2” rating and stable outlook with Moody’s. The credit rating agency said Mayo Clinic’s strong market position and patient demand will drive favorable financial results. The health system “will continue to leverage its excellent reputation and patient demand to continue generating favorable operating performance while maintaining strong balance sheet ratios,” Moody’s said.
9. Memorial Sloan Kettering Cancer Center in New York City has an “AA” rating and stable outlook with Fitch and an “AA-” rating and stable outlook with S&P. Memorial Sloan Kettering Cancer Center’s national and international reputation as a premier cancer hospital will continue to support the organization’s growth, Fitch said. The hospital has a leading and growing market share for its specialty services, according to the credit rating agency.
10. Methodist Health System has an “Aa3” rating and stable outlook with Moody’s. The Dallas-based system has strong operating performance, and investments in facilities have allowed it to continue to capture more market share in the fast-growing Dallas-Fort Worth, Texas, area, Moody’s said. The credit rating agency said it expects Methodist Health System’s strong operating performance and favorable liquidity to continue.
11. Albuquerque, N.M.-based Presbyterian Healthcare Services has an “Aa3” rating and stable outlook with Moody’s and an “AA” rating and stable outlook with Fitch. The health system has a leading statewide market share, strong revenue growth and a healthy balance sheet, Moody’s said. The credit rating agency said it expects Presbyterian Healthcare Services’ operations to continue to improve and its balance sheet and debt metrics to remain strong.
12. Chicago-based Rush Health has an “AA-” rating and stable outlook with Fitch. The health system has a strong financial profile and a broad reach for high-acuity services as a leading academic medical center, Fitch said. The credit rating agency expects Rush’s services to remain profitable over time.
13. Stanford (Calif.) Health Care has an “AA” rating and stable outlook with Fitch. The health system has extensive clinical reach in a competitive market and its financial profile is improving, Fitch said. The health system’s EBITDA margins rebounded in fiscal year 2021 and are expected to remain strong going forward, the crediting rating agency said.
14. St. Clair Hospital in Pittsburgh has an “AA-” rating and stable outlook with Fitch. The hospital has a strong financial profile and a solid market position in the competitive greater Pittsburgh-area healthcare market, Fitch said. The credit rating agency expects the hospital’s margins to remain solid, driven by growth in key service lines.
15. University of Chicago Medical Center has an “AA-” rating and stable outlook with Fitch. The credit rating agency said it expects University of Chicago Medical Center’s capital-related ratios to remain strong, in part because of its broad reach of high-acuity services.
16. University of Iowa Hospitals and Clinics has an “Aa2” rating and stable outlook with Moody’s. The Iowa City-based health system, the only academic medical center in Iowa, has strong patient demand and excellent financial management, Moody’s said. The credit rating agency said it expects the health system to continue to manage the pandemic with improved operating cash flow margins.