About 1.5 million people filed for state unemployment benefits last week, the Department of Labor announced Thursday, bringing the 13-week total for first-time claims to more than 45 million. Another 760,000 filed new claims for Pandemic Unemployment Assistance, a temporary program for workers such as independent contractors who ordinarily do not qualify for unemployment payments.
While new jobless claims continue to decline, falling for the 11th straight week, the numbers remain startlingly high relative to previous recessions, and some economists have expressed concerns that the labor market is not healing as rapidly as they had hoped.
“It’s not clear why claims are still so high,” said Ian Shepherdson, chief economist at Pantheon Macroeconomics, in a note to clients. “[I]s it the initial shock still working its way up through businesses away from the consumer-facing jobs lost in the first wave, or is it businesses which thought they could survive now throwing in the towel, or both? Either way, these are disappointing numbers and serve to emphasize that a full recovery is going to take a long time.”
The exponential nature of viral spread means that pandemics are fast-moving and dynamic.
Combine this with the high interconnectedness of modern life—even when social distancing and lockdowns are applied—and pandemics can evolve quickly. In just a few weeks, previous hotspots can cool down, while new high risk areas can crop up seemingly out of nowhere.
In the United States, like many other places in the world, the virus is hitting regions differently, and this landscape is constantly changing over time.
COVID-19 Growth, by State
Today’s first visualization above comes to us from Reddit user bgregory98, and it uses data from the New York Times to plot confirmed active COVID-19 cases by state.
States are organized by the date that weekly average cases peaked, from top to bottom. Data is normalized and is current until June 16th, and states are colored based on regional definitions (i.e. Northeast, Midwest, West, South) as defined by the U.S. Census Bureau.
As you can see, when looking purely at active cases, the situation has evolved considerably from a geographical perspective.
Early on, COVID-19 cases were more concentrated in coastal population centers, especially in the Northeast. New York, New Jersey, and Massachusetts, the three hardest hit states per capita so far, saw cases peak in April.
However, a look at the bottom half of the visualization shows that generally, states in the South and West are starting to heat up with cases. Recent daily numbers confirm this, with California, Texas, Florida, Arizona, and North Carolina all gaining more than 1,000 new cases on June 17th.
Growth by State, Part Deux
The following visualization by Reddit user jawsem17 is designed using a similar concept, and is current as of June 17th.
This version uses the same data set from the New York Times. However, it also includes deaths as a metric, showing a comparison of peak deaths to peak cases for each state.
Although one would expect peak deaths to follow peak cases, this is not always the case.
Peak deaths in Nevada, for example, occurred on April 24th, but peak cases have been in the last week. This same peculiar pattern can be seen in a variety of states, from California to Oklahoma.
Mapped: The Evolution of COVID-19 in the U.S.
As the pandemic spreads and the situation has evolved, the mean center of weekly COVID-19 cases has been moving in a southwest direction.
The following map, which also comes from Reddit user bgregory98, averages the center coordinates of all counties weighted by how many new confirmed cases they have had over the past week:
Originating in Ohio, the mean center of cases was initially heavily skewed by cases in the New York metro area. Since then, the mean center of cases has shifted and has now journeyed slightly past the mean center of U.S. population, located in Missouri.
This is partially a regression to the mean, but it is also driven by growing case counts in aforementioned states in the southern and western parts of the country.
Mapped: Peak County Totals
Finally, the progression of COVID-19 within the U.S. can be mapped in another useful way, revealing a geographical perspective to the virus’ spread.
These maps from Winston Saunders show places where current disease levels are below their previous peaks (blue), and where current COVID-19 cases are at highs (red) as of June 18:
Cases Below Previous Peaks
Cases at Peak Levels
This again shows the shift from the Northeast and Midwest parts of the country towards the West and South regions.
As always, the path of the virus’ spread will continue to change and evolve, and the picture could again look quite different in just a few weeks time.
Both college football and the NFL are currently prepared to move forward with their fall seasons, despite the ongoing public health crisis. Dr. Anthony Fauci has called into question whether that will be possible.
The NBA is pushing towards a July restart effectively in a “bubble” down at Disney property in Orlando. With 22 teams and fewer than 20 players on each, with support staff and others, the number of people in Orlando is large but manageable. Football presents much bigger problems.
Right now, the NFL and college football are set to play out schedules at home stadiums, whether or not fans can attend. Dr. Fauci says he thinks the NBA approach can work, but he has significant questions about how football will get underway.
“Unless players are essentially in a bubble, insulated from the community and they are tested nearly every day, it would be very hard to see how football is able to be played this fall,” Dr. Fauci said during a CNN appearance with Dr. Sanjay Gupta.
“If there is a second wave, which is certainly a possibility and which would be complicated by the predictable flu season, football may not happen this year,” Dr. Fauci added.
A second wave would definitely be a complicating factor, considering the first wave hasn’t really ended. While cases have been on a decline nationally, that is most due to a dip in the places where the virus was bad from the start, like New York.
At the same time, 22 states are currently peaking, including some major football hotbeds like Florida, South Carolina, and Texas after early reopening. The first wave in the country hasn’t ended, it has just started to hit new areas hard in recent weeks.
It would be nearly impossible for college football to implement some kind of bubble, and with the sheer size of NFL teams, and all 32 teams involved, it is unclear whether an NBA-style plan could work for the league. Football is definitely not out of the woods yet.
China is moving rapidly to seal off its capital of 22 million residents by canceling flights and trains amid growing fears that a potential second wave of covid-19 is gathering strength in Beijing and could spread to the rest of the country.
Authorities on Wednesday canceled 1,200 flights in and out of Beijing’s two airports and sharply reduced long-distance bus services. Beijingers were banned from making nonessential trips outside the city and required to take nucleic tests before they leave, municipal officials said at a briefing where they announced 31 new cases of the novel coronavirus.
While Beijing’s case numbers are low by global standards, they are vexing Chinese authorities who had touted their success in quickly stamping out the coronavirus and had taken pains to ensure it would not infect the seat of the ruling Communist Party. Government officials announced “wartime” measures on Saturday after dozens of cases were discovered at the Xinfadi wholesale market in southwest Beijing, which carried worrying echoes of the original outbreak in Wuhan late last year.
In the days since, Beijing has steadily reintroduced stricter measures, potentially foreshadowing the difficulty that many governments could face in warding off future waves of covid-19.
After classes resumed just a month ago, Beijing’s schools were again shut on Wednesday, as were some gyms, swimming pools and public attractions. The city raised its emergency response to the second-highest level, and entry and exit checkpoints and temperature checks returned to neighborhoods in the city center. The scenes were reminiscent of those during the outbreak’s peak in February and March, albeit with less-strict lockdown measures.
The risk of people in Beijing traveling in and out of the city and spreading infections countrywide is “severe,” acknowledged Chen Bei, Beijing’s deputy party chief. “We need to take decisive action . . . resolutely control this gathering epidemic and resolutely curb its spread inside and outside the city,” Chen said.
Officials said Beijing has tested 3.56 million people since June 13, underscoring the extent of their concern.
Adding to a sense of frustration with the virus’s reemergence, Chinese experts said it may have been lurking undetected for weeks.
“The Beijing outbreak very likely didn’t start in June, or May, but a month before that,” Gao Fu, head of the Chinese Center for Disease Control and Prevention, told reporters in Shanghai. “There can only be so many cases around us now if there were already many people with no symptoms or light symptoms back then. This is our current speculation, but we need to verify it.”
Chinese researchers say they are examining how the coronavirus made a sudden comeback. Fears that shipped livestock and produce could carry the virus — with potentially worrisome implications for international trade — began circulating this week after it was found at the Xinfadi market on cutting boards used for salmon, which is imported from Europe. The genetic material of viruses found at the market and in patients in Beijing also matched sequences typically found in patients in Europe.
Although the theory was fanned this week by nationalist media outlets including the party-run Global Times — which seized the opportunity to question whether the entire pandemic originated last year in Europe instead of China — Chinese and international experts, including the U.S. Food and Drug Administration, say there is relatively scant evidence that the virus is transmitted on food and packaging.
Wu Zunyou, the Chinese CDC’s top epidemiologist, said Tuesday that the virus was also found throughout the hall of the Xinfadi market, suggesting that the salmon was not necessarily the source. The strain of the virus found in Xinfadi is also prevalent in the United States, Wu added.
Michael Ryan, executive director of the World Health Organization’s Health Emergencies Program, also played down concerns about shipped food as a viral vector, saying the matter requires more study. “I’d be reticent to be in the position where all packaging and other things would need to be systematically tested,” Ryan said. “I don’t think it’s the primary hypothesis, but it needs to be explored.”
Meanwhile, supermarkets and restaurants in Beijing are not taking chances and have stopped selling salmon. The Beijing government said Wednesday it would carry out nucleic testing on all close contacts of people who visited the Xinfadi market, as well as workers in the city’s restaurants, which could number hundreds of thousands of people.
Cases in Beijing are expected to keep rising in the coming days because Xinfadi, which spans an area the size of 250 football fields, is such a large and central part of Beijing’s food distribution network, city officials warned.
As the capital fell again into quasi-lockdown this week, other Chinese cities, including Shanghai, began issuing quarantine requirements and restrictions for travelers from Beijing — a sudden reversal for residents who in normal times enjoy a privileged status.
Officials and state media have called for understanding and cooperation from Beijing residents while rallying citizens nationwide behind the city.
“Go Beijing! Go Zhajiang noodles!” said one popular meme on social media, referring to a classic Beijing dish.
ProPublica deputy managing editor Charles Ornstein wanted to know why experts were wrong when they said U.S. hospitals would be overwhelmed by COVID-19 patients. Here’s what he learned, including what hospitals can do before the next wave.
The prediction from New York Gov. Andrew Cuomo was grim.
In late March, as the number of COVID-19 cases was growing exponentially in the state, Cuomo said New York hospitals might need twice as many beds as they normally have. Otherwise there could be no space to treat patients seriously ill with the new coronavirus.
“We have 53,000 hospital beds available,” Cuomo, a Democrat, said at a briefing on March 22. “Right now, the curve suggests we could need 110,000 hospital beds, and that is an obvious problem and that’s what we’re dealing with.”
The governor required all hospitals to submit plans to increase their capacity by at least 50%, with a goal of doubling their bed count. Hospitals converted operating rooms into intensive care units, and at least one replaced the seats in a large auditorium with beds. The state worked with the federal government to open field hospitals around New York City, including a large one at the Jacob K. Javits Convention Center.
But when New York hit its peak in early April, fewer than 19,000 people were hospitalized with COVID-19. Some hospitals ran out of beds and were forced to transfer patients elsewhere. Other hospitals had to care for patients in rooms that had never been used for that purpose before. Supplies, medications and staff ran low. And, as The Wall Street Journal reported on Thursday, many New York hospitals were ill prepared and made a number of serious missteps.
All told, more than 30,000 New York state residents have died of COVID-19. It’s a toll worse than any scourge in recent memory and way worse than the flu, but, overall, the health care system didn’t run out of beds.
“All of those models were based on assumptions, then we were smacked in the face with reality,” said Robyn Gershon, a clinical professor of epidemiology at the NYU School of Global Public Health, who was not involved in the models New York used. “We were working without situational awareness, which is a tenet in disaster preparedness and response. We simply did not have that.”
Cuomo’s office did not return emails seeking comment, but at a press briefing on April 10, the governor defended the models and those who created them. “In fairness to the experts, nobody has been here before. Nobody. So everyone is trying to figure it out the best they can,” he said. “Second, the big variable was, what policies do you put in place? And the bigger variable was, does anybody listen to the policies you put in place?”
So, why were the projections so wrong? And how can political leaders and hospitals learn from the experience in the event there is a second wave of the coronavirus this year? Doctors, hospital officials and public health experts shared their perspectives.
The Models Overstated How Many People Would Need Hospital Care
The models used to calculate the number of people who would need hospitalization were based on assumptions that didn’t prove out.
Early data from the U.S. Centers for Disease Control and Prevention suggested that for every person who died of COVID-19, more than 11 would be hospitalized. But that ratio was far too high and decreased markedly over time, said Dr. Christopher J.L. Murray, director of the Institute for Health Metrics and Evaluation at the University of Washington. IHME’s earliest models on hospitalizations were based on that CDC data and predicted that many states would quickly run out of hospital beds.
A subsequent model, released in early April, assumed about seven hospitalizations per death, reducing the predicted surge. Currently, Murray said, the ratio is about four hospital admissions per death.
“Initially what was happening and probably what we saw in the CDC data is doctors were admitting anybody they thought had COVID,” Murray said. “With time they started admitting only very sick people who needed oxygen or more aggressive care like mechanical ventilation.”
A patient with COVID-19 is taken into Mount Sinai Hospital in New York on May 3. (Alexi Rosenfeld/Getty Images)
A model created by the Harvard Global Health Institute made a different assumption that also turned out to be too high. Data from Wuhan, China, suggested that about 20% of those known to be infected with COVID-19 were hospitalized. Harvard’s model, which ProPublica used to build a data visualization, assumed a hospitalization rate in the United States of 19% for those under 65 who were infected and 28.5% for those older than 65.
But in the U.S., that percentage proved much too high. Official hospitalization rates vary dramatically among states, from as low as 6% to more than 20%, according to data gathered from states by The COVID Tracking Project. (States with higher rates may not have an accurate tally of those infected because testing was so limited in the early weeks of the pandemic.) As testing increases and doctors learn how to treat coronavirus patients out of the hospital, the average hospitalization rate continues to drop.
New York state’s testing showed that by mid-April, approximately 20% of the adult population in New York City had antibodies to COVID-19. Given the number hospitalized in the city and adjusting for the time needed for the body to produce antibodies, this means that the city’s hospitalization rate was closer to 2%, said Dr. Nathaniel Hupert, an associate professor at Weill Cornell Medicine and co-director of the Cornell Institute for Disease and Disaster Preparedness.
Dr. Ashish Jha, director of the Harvard Global Health Institute, and his team also assumed that between 20% and 60% of the population would be infected with COVID-19 over six to 18 months. That was before stay-at-home orders took effect nationwide, which slowed the virus’s spread. Outside of New York City, a far lower percentage of the population has been infected. Granted, we’re not even six months into the pandemic.
A number of factors go into disease models, including the attack rate (the percentage of the entire population that eventually becomes infected), the symptomatic rate (how many people are going to show symptoms), the hospitalization rate for different age groups, the fraction of those hospitalized that will need intensive care and how much care they will need, as well as how the disease travels through the population over time (what is known as “the shape of the epidemic curve”), Hupert said.
Before mid-March, Hupert’s best estimate of the impact of COVID-19 in New York state was that it would lead to a peak hospital occupancy of between 13,800 to 61,000 patients in both regular medical wards and intensive care. He shared his work with state officials.
David Muhlestein, chief strategy and chief research officer at Leavitt Partners, a health care consulting firm, said one takeaway from COVID-19 is that models can’t try to predict too far into the future. His firm has created its own projection tool for hospital capacity that looks ahead three weeks, which Muhlestein said is most realistic given the available data.
“If we were held to our very initial projection of what was going to happen, everybody would be very wrong in every direction,” he said.
Hospitals Proved Surprisingly Adept at Adding Beds
When calculating whether hospitals would run out of beds, experts used as their baseline the number of beds in use in each hospital, region and state. That makes sense in normal times because hospitals have to meet stringent rules before they are able to add regular beds or intensive care units.
Workers prepare dozens of extra beds that were delivered to Mount Sinai on March 31. (Spencer Platt/Getty Images)
But in the early weeks of the pandemic, state health departments waived many rules and hospitals responded by increasing their capacity, sometimes dramatically. “Just because you only have six ICU beds doesn’t mean they will only have six ICU beds next week,” Muhlestein said. “They can really ramp that up. That’s one of the things we’re learning.”
Take Northwell Health, a chain of 17 acute-care hospitals in New York. Typically, the system has 4,000 beds, not including maternity beds, neonatal intensive care unit beds and psychiatric beds. The system grew to 6,000 beds within two weeks. At its peak, on April 7, the hospitals had about 5,500 patients, of which 3,425 had COVID-19.
The system erected tents, placed patients in lobbies and conference rooms, and its largest hospital, North Shore University Hospital, removed the chairs from its 300-seat auditorium and replaced them with a unit capable of treating about 50 patients. “We were pulling out all the stops at that point,” Senior Vice President Terence Lynam said. “It was unclear if the trend was going to go the other way. We did not end up needing them all.”
Northwell went from treating 49 COVID-19 inpatients on March 16 to 3,425 on April 7. “I don’t think anybody had a clear handle on what the ceiling was going to be,” Lynam said. As of Wednesday, the system was still caring for 367 COVID-19 patients in its hospitals.
As hospitals found ways to expand, government leaders worked with the Army Corps of Engineers to build dozens of field hospitals across the country, such as the one at the Javits Center. According to an analysis of federal spending by NPR, those efforts cost at least $660 million. “But nearly four months into the pandemic, most of these facilities haven’t treated a single patient,” NPR reported. As they began to come online, stay-at-home orders started producing results, with fewer positive cases and fewer hospitalizations.
Demand for Non-COVID-19 Care Plummeted More Than Expected
Hospitals across the country canceled elective surgeries, from hip replacements to kidney transplants. That greatly reduced the number of non-COVID-19 patients they had to treat. “We generated a lot more capacity by getting rid of elective procedures than any of us thought was possible,” Harvard’s Jha said.
Northwell canceled elective surgeries on March 16, and over the span of the next week and a half, its hospitals discharged several thousand patients in anticipation of the coming surge. “In retrospect, it was a wise move,” Lynam said. “It just ballooned after that. If we had not discharged those patients in time, there would have been a severe bottleneck.”
What’s more, experts say, it’s clear that some patients with true emergencies also stayed home. A recent report from the CDC said that emergency room visits dropped by 42% in the early weeks of the pandemic. In 2019, some 2.1 million people visited ERs each week from late March to late April. This year, that dropped to 1.2 million per week. That was especially true for children, women and people who live in the Northeast.
In New York City, emergency room visits for asthma practically ceased entirely at the peak, Cornell’s Hupert said. “You wouldn’t imagine that asthma would just disappear,” he said. “Why did it go away? … Nobody has seen anything like that.”
Undoubtedly some people experienced heart attacks and strokes and didn’t go to the hospital because they were fearful of getting COVID-19. “I didn’t expect that,” Jha said. A draft research paper available on a preprint server, before it is reviewed and published in an academic journal, found that heart disease deaths in Massachusetts were unchanged in the early weeks of the pandemic compared to the same period in 2019. What that may mean is that those people died at home.
The Coronavirus Attacked Every Region at a Different Pace
Some initial models forecast that COVID-19 would hit different regions in similar ways. That has not been the case. New York was hit hard early; California was not, at least initially.
In recent weeks, hospitals in Montgomery, Alabama, saw a lot of patients. Arizona’s health director has told hospitals in the state to “fully activate” their emergency plans in light of a spike in cases there. The Washington Post reported on Tuesday that hospitalizations in at least nine states have been rising since Memorial Day.
St. Luke’s, a closed hospital in Phoenix, is prepared to receive overflow patients on April 23. Arizona initially wasn’t hit hard, but cases are now spiking. (Ross D. Franklin/AP Photo)
Dr. Mark Rupp, medical director of the Department of Infection Control and Epidemiology at the University of Nebraska Medical Center in Omaha, said his region hasn’t seen a tidal wave like New York. “What we’ve seen is a rising tide, a steady increase in the number of cases.” Initially that was associated with outbreaks at specific locations like meatpacking and food processing plants and to some degree long-term care facilities.
But since then, “it has just plateaued,” he said. “That has me concerned. This is a time when I feel like we should be working as hard as we can to push these numbers as low as possible.”
Rupp’s hospital has been caring for 50 to 60 COVID-19 patients on any given day. The hospital has started to perform surgeries and procedures that had been on hold because “elective cases stay elective for only so long.”
The hospital’s general medical/surgical beds are 70% to 80% filled, and its ICU beds are 80% to 90% full. “We don’t have a big cushion.”
Even in New York City, the virus hit boroughs differently. Queens and the Bronx were hard hit; Manhattan, Brooklyn and Staten Island less so. “Maybe we can’t even model a city as big as New York,” Hupert said. “Each neighborhood seemed to have a different type of outbreak.”
That needs further study but could be attributable to both social and demographic conditions and the type of jobs residents of the neighborhoods had, among other factors.
What We Can Learn From Coronavirus “Round One”
While hospitals were able to add beds more quickly than experts realized they could, some other resources were harder to come by. Masks, gowns and other personal protective equipment were tough to get. So were ventilators. Anesthesia agents and dialysis medications were in short supply. And every additional bed meant the need for more doctors, nurses and respiratory therapists.
In early February, before any cases were discovered in New York, Northwell purchased $5 million in PPE, ventilators and lab supplies just in case, Lynam said. “It turned out to be a wise move,” he said. “What’s clear is that you can never have enough.”
Northwell has spent $42 million on PPE alone. “We were going through 10,000 N95 masks a day, just a crazy amount,” he said. “One of the lessons learned is you have to stockpile the PPE. There’s got to be a better procurement process in place.”
If there’s one thing the system could have done differently, Lynam said, it’s bringing in more temporary nurses earlier. Northwell brought in 500 nurses from staffing agencies. “They came in a week later than they should have.”
Dr. Robert Wachter, chair of the department of medicine at the University of California, San Francisco, agreed. “I’ve helped run services in hospitals for 25 years,” he said. “I’ve probably given two minutes of thought to the notions of supply chains and PPE. You realize that is absolutely central to your preparedness. That’s a lesson.”
Experts and hospital leaders agree that everyone can do better if another wave hits. Here’s what that entails:
Having testing readily available, as it now is, to more quickly spot a resurgence of the virus.
Stocking up now on PPE and other supplies. “We definitely have to stockpile PPE by the fall,” Gershon of NYU said. “We have to. … [Hospitals and health departments] have to really get those contracts nailed down now. They should have been doing this, of course, all the time, but no one expected this kind of event.”
Being able to quickly move personnel and equipment from one hot spot to the next.
Planning for how to care for those with other medical ailments but who are scared of contracting COVID-19. “We have to have some sort of a mechanism by which we can offer people assurance that if they come in, they won’t get sick,” Jha said. “We can’t repeat in the fall what we just did in the spring. It’s terrible for hospitals. It’s terrible for patients.”
Providing mental health resources for front-line caregivers who have been deeply affected by their work. The intensity of the work, combined with watching patients suffer and die alone, was immensely taxing.
Coming up with ways to allow visitors in the hospital. Wachter said the visitor bans in place at many hospitals, though well intentioned, may have backfired. “When all hell was breaking loose and we were just doing the best we could in the face of a tsunami, it was reasonable to just keep everybody out,” he said. “We didn’t fully understand how important that was for patients, how much it might be contributing to some people not coming in for care when they really should have.”
Lynam of Northwell said he’s worried about what lies ahead. “You look back on the 1918 Spanish flu and the majority of victims from that died in the second wave. … We don’t know what’s coming on the second wave. There may be some folks who say you’re paranoid, but you’ve got to be prepared for the worst.”
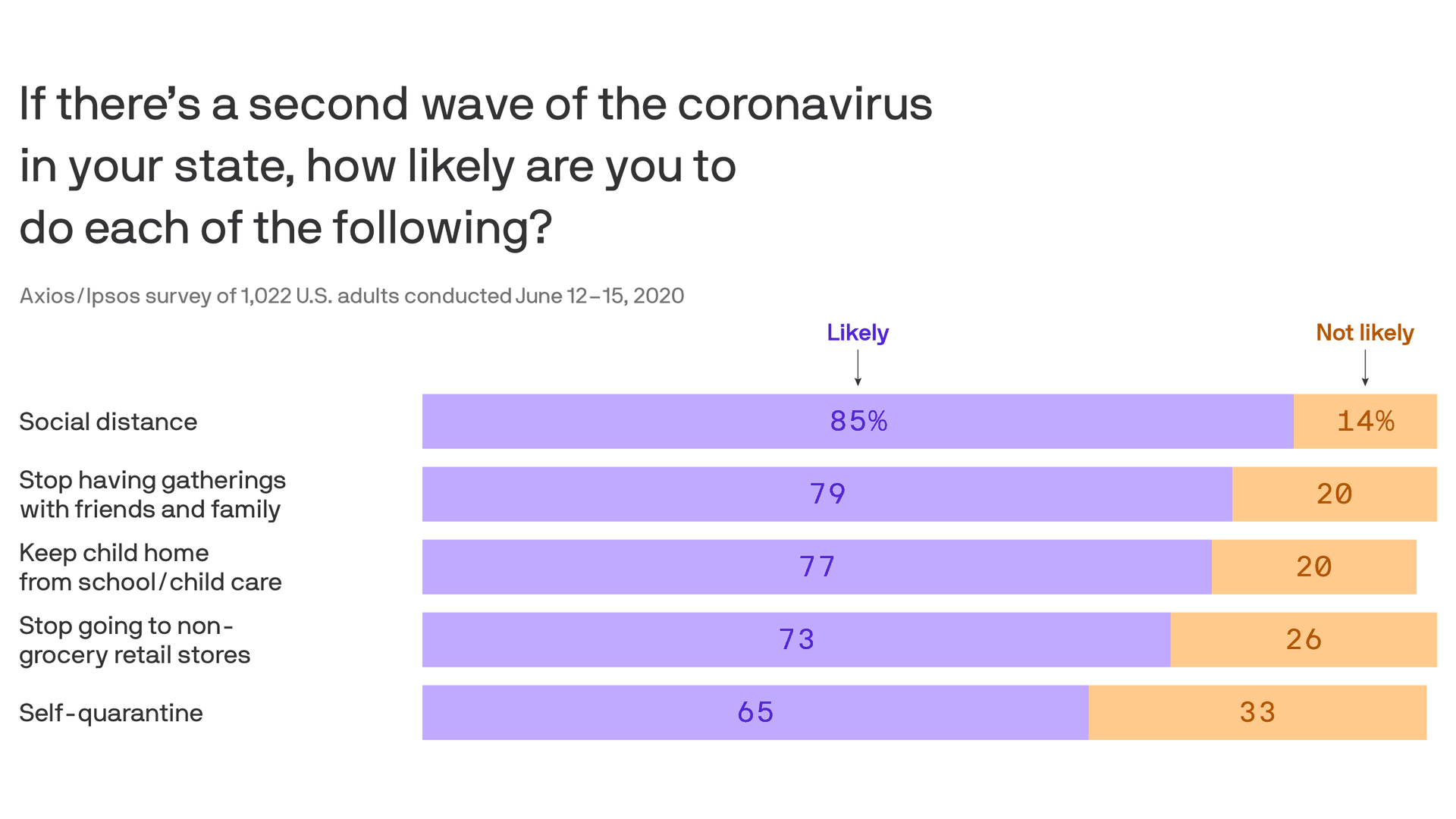
Eight in 10 Americans are worried about a second wave of the coronavirus, with large majorities saying they’ll resume social distancing, dial back shopping and keep their kids out of school if it happens, in Week 13 of the Axios-Ipsos Coronavirus Index.
Why it matters: Businesses and schools around the country are trying to assess how quickly and fully they should reopen based in part on what Americans will demand and tolerate. These findings underscore the challenges in predicting how they should proceed.
But getting Americans to swallow a second round of 14-day self-quarantining could be tougher than getting them to go back to social distancing, with one in three saying they likely won’t do it.
The biggest factor is partisan identification, with 81% of Democrats but only 49% of Republicans saying they’ll self-quarantine if a second wave hits.
The big picture: The latest installment of our national weekly survey shows a renewed sense of risk following reports of new hospitalizations since states began lifting stay-at-home orders — but quarantine fatigue is still driving people to take their chances.
People’s assessment of large or moderate risk grew last week for each of these categories: returning to their normal workplace, dining out, retail shopping, going to the hair salon or participating in protests.
But the share of those going out to eat rose from 31% to 41%. Those visiting friends or relatives rose from 56% to 60%. Those getting their hair done rose from 26% to 31%. Those attending demonstrations rose from 11% to 14%.
What they’re saying: “People are starting to be concerned about it again,” said pollster Chris Jackson, senior vice president for Ipsos Public Affairs. “We’re not yet seeing changes in the patterns of their behavior yet, though.”
“Their behaviors are not really catching up to their concern level.”
By the numbers: 81% say they’re concerned about a second wave — including those who are extremely (30%), very (26%) or somewhat (24%) concerned.
64% of those surveyed say returning to their normal pre-coronavirus life represents a large or moderate risk, up from 57% a week ago.
The share of people extremely or very concerned about getting sick rose from 32% to 40% last week. Those fearing U.S. economic collapse rose from 48% to 54%.
There also were upticks in people’s concerns about job security and the government’s response to the outbreak.
Americans’ ability to afford household goods also decreased.
One in 10 surveyed say they’ve been collecting unemployment benefits in recent weeks.
35% of Americans now know someone who’s tested positive, a new high for the survey.
Between the lines: The survey suggests an evolving understanding of the racial disparities in the pandemic.
The share of those saying they are extremely or very concerned that the coronavirus is doing greater damage to people of color rose from 36% to 42%.
The share of those extremely or very concerned that official responses are biased against certain groups also rose from 36% to 42%.
Prison officials have been reluctant to do widespread virus testing even as infection rates are escalating.
Cases of the coronavirus in prisons and jails across the United States have soared in recent weeks, even as the overall daily infection rate in the nation has remained relatively flat.
The number of prison inmates known to be infected has doubled during the past month to more than 68,000. Prison deaths tied to the coronavirus have also risen, by 73 percent since mid-May. By now, the five largest known clusters of the virus in the United States are not at nursing homes or meatpacking plants, but inside correction institutions, according to data The New York Times has been collecting about confirmed coronavirus cases since the pandemic reached American shores.
And the risk of more cases appears imminent: The swift growth in virus cases behind bars comes as demonstrators arrested as part of large police brutality protests across the nation have often been placed in crowded holding cells in local jails.
A muddled, uneven response by corrections officials to testing and care for inmates and workers is complicating the spread of the coronavirus. In interviews, prison and jail officials acknowledged that their approach has largely been based on trial and error, and that an effective, consistent response for U.S. correctional facilities remains elusive.
“If there was clearly a right strategy, we all would have done it,” said Dr. Owen Murray, a University of Texas Medical Branch physician who oversees correctional health care at dozens of Texas prisons. “There is no clear-cut right strategy here. There are a lot of different choices that one could make that are going to be in-the-moment decisions.”
The inconsistent response to the spread of the coronavirus in correctional facilities is in contrast with efforts to halt its spread in other known incubators of the virus: Much of the cruise ship industry has been closed down. Staff members and residents of nursing homes in several states now face compulsory testing. Many meat processing plants have been shuttered for extensive cleaning.
As the toll in prisons has increased, so has fear among inmates who say the authorities have done too little to protect them. There have been riots and hunger strikes in correctional facilities from Washington State to New York. And even the known case numbers are likely a significant undercount because testing has been extremely limited inside prisons and because some places that test do not release the results to the public.
“It’s like a sword hanging over my head,” said Fred Roehler, 77, an inmate at a California prison who has chronic inflammatory lung disease and other respiratory ailments. “Any officer can bring it in.”
Public officials have long warned that the nation’s correctional facilities would likely become vectors in the pandemic because they are often overcrowded, unsanitary places where social distancing is impractical, bathrooms and day rooms are shared by hundreds of inmates, and access to cleaning supplies is tightly controlled. Many inmates are 60 or older, and many suffer from respiratory illnesses or heart conditions.
In response, local jails have discharged thousands of inmates since February, many of whom had been awaiting trials to have charges heard or serving time for nonviolent crimes. State prison systems, where people convicted of more serious crimes are housed, have been more reluctant to release inmates.
Testing for the virus within the nation’s penal institutions varies widely, and has become a matter of significant debate.
Republican-led states like Texas, Tennessee and Arkansas — which generally spend less on prisoners than the national average — have found themselves at the forefront of testing inmates.
In Texas, the number of prisoners and staff members known to be infected has more than quadrupled to 7,900 during the past three weeks after the state began to test every inmate.
Yet states that typically spend far more on prisons have carried out significantly less testing.
California, which spends $12 billion annually on its prison system, has tested fewer than 7 percent of inmates in several of its largest, most crowded facilities, according to the state’s data. Other Democratic-led states that also spend heavily on prisons, including New York, Oregon and Colorado, have also conducted limited testing despite large outbreaks in their facilities.
New York has tested about 3 percent of its 40,000 prison inmates; more than 40 percent of those tested were infected.
Critics say that the dearth of testing in some facilities has meant that prison and public health officials have only vague notions about the spread of the virus, which has allowed some elected officials to suggest that it is not present at all.
“We have really no true idea of how bad the problem is because most places are not yet testing the way they should,” said Dr. Homer Venters, who served as chief medical officer for the New York City jail system and now works for a group called Community Oriented Correctional Health Services, which works to improve health care services in local jails. “I think a lot of times some of the operational challenges of either not having adequate quarantine policies or adequate medical isolation policies are so vexing that places simply decide that they can just throw up their hands.”
Most state prison systems have conducted few tests. Systems in Illinois, Mississippi and Alabama have tested fewer than 2.5 percent of inmates. And in Louisiana, officials had tested several dozen of its 31,000 inmates in March when the warden and medical director at one of the state’s largest prisons died of the coronavirus. The state has since announced plans to test every inmate.
Prison officials in states where only a limited number of inmates have been tested say they are following federal guidelines. The Centers for Disease Control and Prevention recommend that only prisoners with symptoms be tested.
Prisons that have conducted mass testing have found that about one in seven tests of inmates have come back positive, the Times database shows. The vast majority of inmates who have tested positive have been asymptomatic.
Public health officials say that indicates the virus has been present in prison populations for far longer than had previously been understood.
“If you don’t do testing, you’re flying blind,” said Carlos Franco-Paredes, an infectious-disease specialist at the University of Colorado School of Medicine.
But in California, there continues to be reluctance to test each of the state’s 114,000 inmates, despite growing criticism to take a more aggressive approach. One in six inmates in the state’s prisons have been tested, and the state has released some inmates who were later found to have the virus, raising fears that prison systems could seed new infections outside penal institutions.
“Nothing significant had been done to protect those most vulnerable to the virus,” said Marie Waldron, the Republican minority leader of the California State Assembly.
But J. Clark Kelso, who oversees prison health care in California, said that mass testing would provide only a snapshot of the virus’s spread.
“Testing’s not a complete solution,” Mr. Kelso said. “It gives you better information, but you don’t want to get a false sense of security.”
California’s health department has recommended that a facility’s prison inmates and staff members be given priority for testing once an infection has been identified there.
But the state prison system has conducted mass testing at only a handful of institutions where infections have been found, according to state data. In one of those facilities, the California Institution for Men in Chino, nearly 875 people have tested positive and 13 inmates have died.
Instead, California has employed surveillance testing, which involves testing a limited number of inmates at each state prison regardless of the known infection rate.
That method, Mr. Kelso said, had led officials to conclude that the vast majority of its prisons are free of the virus.
“We’re not 100 percent confident because we’re not testing everyone,” he said. “As we learn every single day from what we’re doing, we may suddenly decide, ‘No, we actually have to test all of them.’ We’re not at that point yet.”
In interviews, California prison inmates say prison staff have sometimes refused to test them, even after they complained about symptoms similar to the coronavirus. Several prisoners said they had been too weak to move for weeks at a time, but were never permitted to see a nurse and had never been tested.
“I had chest pains. I couldn’t breathe,” said Althea Housley, 43, an inmate at Folsom State Prison, where no inmates have tested positive, according to state data. “They told us it was the flu going around, but I ain’t never had a flu like that.”
Mr. Kelso did not dispute the prisoners’ accounts.
In Texas, mass testing has found that nearly 8,000 inmates and guards have been infected. Sixty-two people have died, including some who had not exhibited symptoms.
Dr. Murray, the physician who oversees much of Texas’ prison health care system, said the disparate approaches taken by prison authorities might actually be beneficial as officials compare notes.
“I’m glad we’ve got 50 states and everyone is trying to do something a little different — whether that’s by intent or not — because it’s really the only basis that we’re going to have for comparison later on,” he said.
But Baleegh Brown, 31, an inmate at a California prison, said he was displeased about being part of what he considered a science experiment. His prison has had more than 170 infections.
He said that he and his cellmate are confined to a 6-by-9-foot space for about 22 hours each day as the prison tries to prevent the virus from spreading further. Mr. Brown said he had a weakened immune system after a case of non-Hodgkin’s lymphoma, making him particularly vulnerable to illness.
“We need more testing here so everyone knows for sure,” he said. “And for me, my body has been compromised, so I don’t know how it is going to react. That makes all you don’t know even scarier.”
About half of all facilities have yet to be inspected for procedures to stop the spread of coronavirus.
Thousands of nursing homes across the country have not been checked to see if staff are following proper procedures to prevent coronavirus transmission, a form of community spread that is responsible for more than a quarter of the nation’s Covid-19 fatalities.
Only a little more than half of the nation’s nursing homes had received inspections, according to data released earlier this month, which prompted a fresh mandate from Medicare and Medicaid chief Seema Verma that states complete the checks by July 31 or risk losing federal recovery funds.
A POLITICO survey of state officials, however, suggests that the lack of oversight of nursing homes has many roots. Many states that were hit hard by the virus say they chose to provide protective gear to frontline health workers rather than inspectors, delaying in-person checks for weeks if not months. Some states chose to assess facilities remotely, conducting interviews over the phone and analyzing documentation, a process many experts consider inadequate.
In places where state officials claimed that in-person inspections have taken place, the reports found no issues in the overwhelming majority of cases, even as Covid-19 claimed more than 31,000 deaths in nursing homes.Less than 3 percent of the more than 5,700 inspection surveys the federal government released this month had any infection control deficiencies, according to a report on Thursday by the Center for Medicare Advocacy, a nonprofit patient activist group.
“It is not possible or believable that the infection control surveys accurately portray the extent of infection control deficiencies in U.S. nursing facilities,” the report states.
Noting the vast and unprecedented danger that the coronavirus presents to the elderly and people with disabilities, patient advocates described the lack of inspections as a shocking oversight.
“If you’re not going in, you’re essentially taking the providers’ word that they’re doing a good job,” said Richard Mollot, the executive director of the Long Term Care Community Coalition.
In March, the Trump administration paused routine nursing home inspections, which typically occur about once a year. Instead, the Centers for Medicare and Medicaid Services asked that state agencies focus on inspecting facilities for their infection control practices, such as whether staff wash their hands or properly wear protective clothing before tending to multiple patients.
But for more than two months, state inspectors failed to enter half the country’s homes — a revelation that prompted CMS to crack down.
“We are saying you need to be doing more inspections,” Verma told reporters, explaining her message to states. “We called on states in early March to go into every single nursing home and to do a focused inspection around infection control.”
In some hard-hit states, inspectors conducted remote surveys rather than going into nursing homes, a process that involved speaking to staff by phone and reviewing records. In Pennsylvania, for example, inspectors conducted interviews and reviewed documents for 657 facilities from March 13 to May 15 — most of which was done remotely.
But critics say the failure to make in-person checks prevented states from identifying lapses at a crucial time. The fact that family members were blocked from visiting their relatives — a policy intended to prevent the virus from entering the facility — removed another source of accountability in homes, some of which ended up having more than halfof their residents stricken with the coronavirus.
Keeping relatives out of nursing homes — a policy that continues— has made it more difficult to advocate on behalf of residents in the state, said Karen Buck, executive director of the Pennsylvania-based SeniorLAW Center. More than 4,000residents ofnursing homes and other personal care facilities have died of coronavirus in the Keystone State.
“The inspections are vital,” said Buck. “I think access to residents is essential, and we are very concerned that Pennsylvanians are behind where we should be. We recognize these are very difficult times for our leaders, but we can’t continue to wait.”
Pennsylvania officials maintained that the remote inspections were beneficial, and said they went into the facilities when they felt there was significant concern over residents’ health.
“We can conduct the same interviews, review the same documentation and do all the same actions we could in person, except for the ability to be on-site,”health department spokesperson Nate Wardle wrote in an email, adding that Verma’s office approved the remote procedures earlier this spring.
Nonetheless, many public health experts say they believe states have erred in choosing not to prioritize nursing home inspectors when handing out protective equipment. While it makes sense to direct resources to front-line workers, nursing home inspectors were only a tiny number of people compared to the hundreds of thousands of hospital employees — and experts contend that the situation in nursing facilities was dire enough to require immediate action.
David Grabowski, an expert in aging and long-term care at Harvard Medical School, said he understands inspectors were put in a tough position in the early days of the pandemic, but that inspections needed to be ramped up within a few weeks.
“I think after those first few weeks we should have had personal protective equipment in place for the inspectors and doing these inspections remotely is really second best,” he said.
And yet state after state waited on inspections or performed them remotely.
In Utah, only a small portion of the state’s nearly 100 facilities received inspections over the first three months of the pandemic. Only now is the state health department ramping up on-site inspections, with the goal of hitting all of its nursing homes by the second week of July. It conducted 14 last week, and received some help from federal inspectors with another four.
The state survey agency said it made a conscious determination not to request protective equipment for state inspectors in the initial phase of the pandemic, fearing they would take supplies away from frontline health providers, said Greg Bateman, the head of long-term care surveys. Instead, the department conducted 43 remote reviews and talked to nursing homes at least twice a week.
In Idaho,state inspectors have only recently received the N95 masks, face shields and gowns necessary to perform inspections.
“The reason we had difficulty is because Idaho, like many other states, was challenged to secure adequate PPE to meet the needs of the various health care entities,” health department spokesperson Niki Forbing-Orr wrote in an email. “The state surveyors had concerns about potentially using PPE that other entities could use that provide direct medical services and care to Idaho residents.”
In New Jersey, which has seen roughly 6,000 deaths in nursing homes and other communal settings, the health department also first chose sending supplies to frontline workers in nursing homes and hospitals.The state began making in-person checks when it received PPE April 16, said Dawn Thomas, a New Jersey health department spokesperson.
But New Jersey still has a long way to go. The state has completed inspections in only about 115 out of more than 360 nursing homes as of June 3, according to Thomas.
While Pennsylvania, Idaho, New Jersey and other states complained of a lack of PPE, other states battling major outbreaks of coronavirus in nursing homes have completed nearly all of their inspections, calling into question the explanations for why others have struggled.
Washington state, where the Life Care Center of Kirkland became an early epicenter of the coronavirus outbreak, has completed 99 percent of its inspections, the state reported this spring to CMS. And Michigan, which has had nearly 2,000 deaths in nursing homes, has completed nearly 85 percent of its inspections.
By contrast, states such as West Virginia and Maryland, with only 11.4 and 16.4 percent of facilities inspected as of the end of May, lagged way behind.
A nursing home in Maryland’s Carroll County served as an early example of just how quickly the coronavirus can ravage nursing homes. On March 26, a resident at a Carroll County, Md., facility tested positive for the coronavirus. Two weeks later, the number of confirmed cases was up to 77 out of 95 residents, along with 24 staff members. At least 28 residents have died.
A Maryland health department spokesperson says the state took “early and aggressive measures” to address the virus in nursing homes, noting that Maryland created the country’s first strike teams — composed of state and local health officials, medical professionals and National Guard members — to help triage seniors and scrutinize facilities.
Nonetheless, state inspectors didn’t have personal protective equipment until late April, according to the health department.
“In April, PPE acquisition was challenging across the nation and in Maryland due to the rapidly evolving Covid-19 pandemic,” the spokesperson wrote in an email, adding that the department sought N95 masks, gowns and other items from “the national stockpile, FEMA and national and international supply chains.”
With many facilities still closed to visitors, the slow pace of inspections lost a key window into the nursing homes during the pandemic.
“I think having more eyes on what’s happening is really important,” Grabowski said.
Last month, the Health and Human Services’ watchdog agency announced plans to review the pace of inspections in nursing homes and barriers to completing them — referring to such checks as a “fundamental safeguard to ensure that nursing home residents are safe and receive high-quality care.”
“There is no substitute for boots on the ground — for going into a facility to assess whether a facility is abiding by long-standing infection control practices,” Verma told reporters this month.
• Since April, the numbers of new cases and deaths from the coronavirus have been falling nationally, although the number of cases ticked slightly upward in the first week of June, a few weeks after many states ended their stay-at-home orders.
• The spread of the virus has varied significantly from state to state. Some states, especially those with longer-lasting stay-at-home orders, have seen cases fall since April. Others, including many that ended their closures earlier, have seen increases.
• Scientists expect to see a rise in coronavirus cases in the coming weeks due to continued reopenings and the racial justice protests. However, it’s unclear how large those increases will be.
With most states reopening for business after shutting down for the novel coronavirus, some states are seeing an increase in infections. And with protest marches bringing together large numbers of people, some scientists worry that infections could rise further.
However, scientists say that there’s lots of uncertainty about whether, and how much, the coronavirus will spread following the lifting of stay-at-home orders and the emergence of protest marches for racial justice.
We looked at the most recent data and interviewed several researchers to explain what we’re seeing already, and what might happen in the future.
What are the overall trends for coronavirus cases and deaths?
Nationally, both cases and deaths have generally been falling since April, although cases saw a small uptick in early June.
Here’s a chart showing the number of new coronavirus cases confirmed each day since the outbreak began in late February. The blue bars show the number of new cases per day, while the orange line shows the seven-day rolling average, which smooths out technical differences in the daily reporting.
The pattern for coronavirus deaths has been similar, with a fairly consistent decline since mid-April.
Researchers said the spring stay-at-home orders are likely the main reason for the declining trend.
“The social distancing that resulted from the closures slowed cases,” said Tara C. Smith, a professor of epidemiology at Kent State University.
Smith cited a recent study that estimated that the shutdowns prevented an additional 4.8 million confirmed coronavirus cases in the U.S., and about 60 million infections in all. (The 60 million figure includes people who didn’t know they were infected and did not confirm their infection with a test.) So far, there have been roughly 2 million confirmed coronavirus cases.
The decline in cases has been driven by significant improvements in the hardest-hit area: the tri-state region of New York, New Jersey and Connecticut. Each of those states has seen the number of new cases decline consistently since April, as can be seen in this chart:
How has the timing of reopenings affected new-case patterns?
The national numbers mask considerable differences among the states in new caseloads.
Beyond New York, New Jersey and Connecticut, several other largestates have seen declining caseloads over time.
Here’s a chart showing the patterns for Pennsylvania, Illinois, Ohio, Michigan and Virginia, all of which have seen declines in new cases in recent weeks:
But other states have seen increases in recent weeks. Here’s a look at the upward trends in California, Texas, Florida, Georgia, North Carolina and Arizona:
Almost every state in our chart that’s seeing rising numbers of new cases reopened between April 30 and May 22. (The one exception is California, which is a mystery to the experts we asked.)
By contrast, the states in our charts with falling numbers of new cases opened no earlier than May 28.
Experts said there are too many variables to conclude that reopening will inevitably produce rising new case counts. For instance, the virus’ spread may be proceeding differently in urban areas than in the rest of the state, something that the state-level data wouldn’t capture.
Also, the data we used are not adjusted for the number of tests being conducted. The more tests that are done, the more positive cases will be found, everything else being equal.
That said, if there is a connection between reopening and a rise in new cases, the states that delayed their openings may see their new case loads rise in the coming weeks.
“Until we have a vaccine for prevention, our ‘people’ interventions are what stand between us and the virus spreading,” said Nicole Gatto, an associate professor in the School of Community and Global Health at Claremont Graduate University. “Reopening efforts and mixing of people again will reintroduce the potential for viral transmission.”
What impact could the recent protest marches have on the virus’ spread?
For now, the impact of the protests on new caseloads is not showing up in the data. Any impact would become evident only in the next few weeks, as participants get tested and the results are tabulated.
Some aspects of the protests could promote the spread, experts said.
“The protests have ingredients which we have been making efforts to avoid these last three months: large gatherings of people in close proximity to each other not always wearing protective face coverings,” Gatto said. “Add in tear gas, and the recipe becomes worse.”
People who were arrested at protests and had to spend time in jail could also be at higher risk for infection, scientists said.
The best-case scenario, scientists said, is that the marches’ outdoor locations and the precautions taken by participants will cut down on the spread.
“Outdoor gatherings may present less transmission risk, especially when everyone is wearing a mask,” said Forrest W. Crawford, a biostatistician at Yale University.
While emphasizing the uncertainties, Smith said she was surprised by the relatively modest impact of the state reopenings on the virus’ spread so far. So there may be reason for cautious optimism.
“I’m expecting cases to grow over the next two weeks, but it’s really tough to say if it will be a spike or a less dramatic increase,” she said.