Cigna, my former employer, disclosed this morning that during the first seven months of this year, it spent $5 billion of the money it took from its health plan and pharmacy benefit customers to buy back shares of its own stock, a gimmick that rewards shareholders at the expense of those customers.
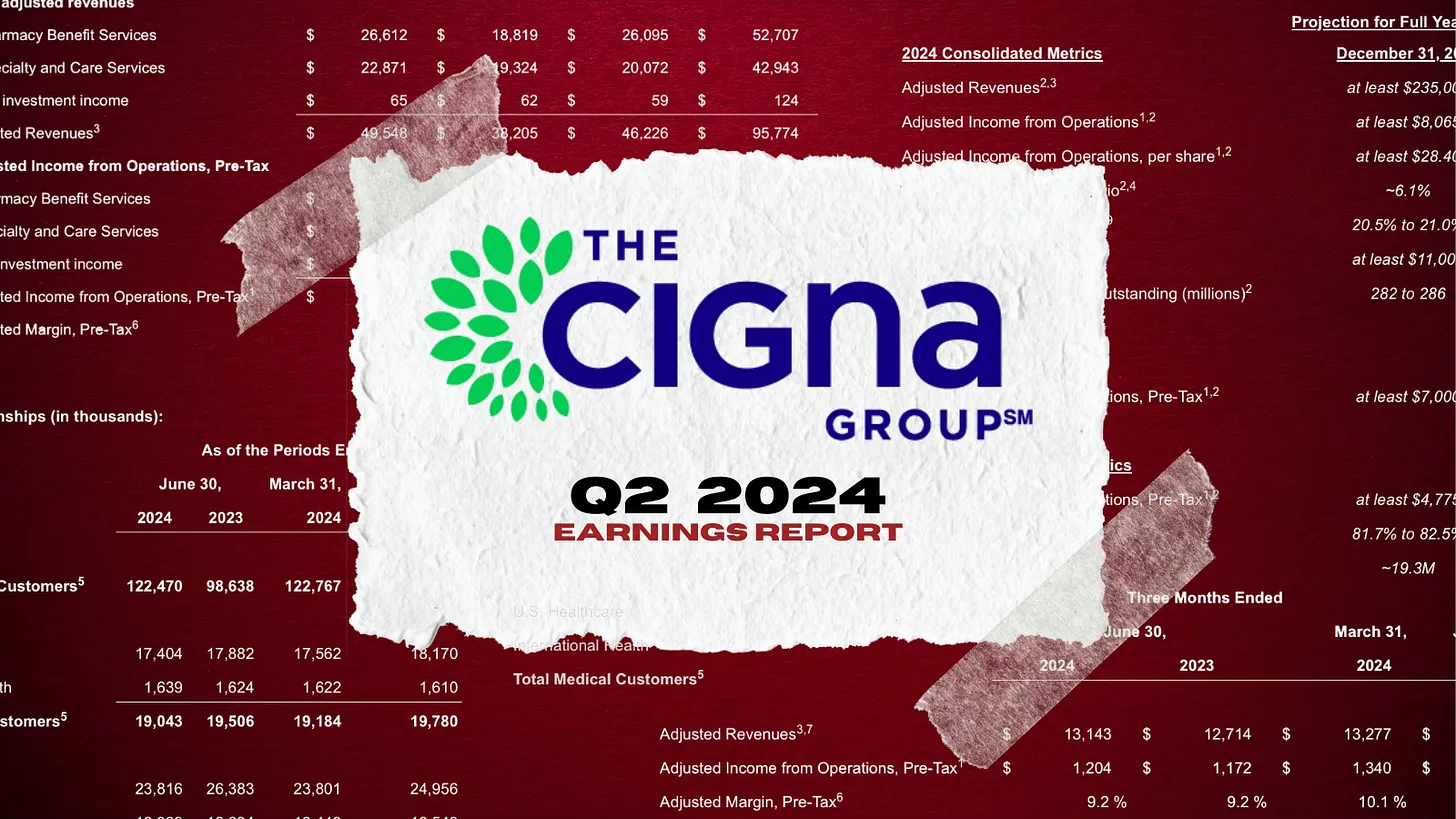
Cigna also disclosed that its revenues increased a stunning 25% – to $60.5 billion – during the second quarter of this year compared to the same period in 2023. Profits also grew, from $1.8 billion to $1.9 billion.
One of the ways Cigna made so much money was by purging health plan enrollees it decided were not profitable enough to meet Wall Street’s profit expectations.
Enrollment in its U.S. health plans fell by nearly half a million people – from 17.9 million to 17.4 million – over the past year. The company signaled to investors that it was more than OK with that decline, noting that it ran off those customers through “targeted pricing actions in certain geographies.” What that means is that Cigna increased premiums so much for those folks that they either found other insurers or joined the ranks of the uninsured.
It was an entirely different story in Cigna’s pharmacy benefit (PBM) business, which saw a 24% increase in total pharmacy customers. The vast majority of Cigna’s revenues now come from its role as one of the country’s largest middlemen in the pharmacy supply chain. Revenue from Cigna’s pharmacy operations totaled nearly $50 billion in the second quarter of this year, up from $38.2 billion last year. By contrast, revenue from its health plan business increased modestly, from $12.7 billion to $13.1 billion.
But by purging 478,000 men, women and children from its rolls, Cigna reported a profit margin of 9.2% for its health plan operations. That, folks, is exceedingly high in the health insurance business.
One way Cigna and the other industry giants can reward their shareholders so handsomely is by making their health plan and pharmacy customers pay more and more out of their own pockets before the insurers pay a dime.
The Affordable Care Act made it illegal for insurers to refuse to sell coverage to people with preexisting conditions or to set premiums based on someone’s health status.
But that law kept open a big back door that enables insurers like Cigna to make people with health problems pay huge sums of money for their care through deductibles and copayments. As a consequence, millions of Americans are walking away from the pharmacy counter without their medications, and many others who simply cannot live without their meds often wind up buried under a mountain of medical debt.
A growing number of bills have been or soon will be introduced by members of Congress to fulfill Biden’s pledge, but you can expect Cigna and other big insurers to insist that doing so will mean premiums will have to go up.
That’s bullshit.
It might mean that Cigna and the other giants might have to curtail their stock buyback programs and accept slimmer profit margins, but it does not mean premiums will have to go up.
Wall Street will howl if one of the tools insurers use to gouge their customers is taken away – just as investors are punishing Cigna today for the sin of not predicting even higher profits for the rest of the year –
but reducing out-of-pocket requirements would put a significant dent in the enormous and ongoing transfer of wealth by middlemen like Cigna from middle-class Americans, especially those struggling with health issues, to fat cat investors and corporate executives.
Over the weekend, President Biden called it quits and Democrats seemingly coalesced around Vice President Harris as the Party’s candidate for the White House. While speculation about her running mate swirls, the stakes for healthcare just got higher. Here’s why:
A GOP View of U.S. Healthcare
Republicans were mute on their plans for healthcare during last week’s nominating convention in Milwaukee. The RNC healthcare platform boils down to two aims: ‘protecting Medicare’ and ‘granting states oversight of abortion services. Promises to repeal and replace the Affordable Care Act, once the staple of GOP health policy, are long-gone as polls show the majority (even in Red states (like Texas and Florida) favor keeping it. The addition of Ohio Senator JD Vance to the ticket reinforces the party’s pro-capitalism, pro-competition, pro-states’ rights pitch.
To core Trump voters and right leaning Republicans, the healthcare industry is a juggernaut that’s over-regulated, wasteful and in need of discipline. Excesses in spending for illegal immigrant medical services ($8 billion in 2023), high priced drugs, lack of price transparency, increased out-of-pocket costs and insurer red tape stoke voter resentment. Healthcare, after all, is an industry that benefits from capitalism and market forces: its abuses and weaknesses should be corrected through private-sector innovation and pro-competition, pro-consumer policies.
A Dem View of Healthcare
By contrast, healthcare is more prominent in the Democrat’s platform as the party convenes for its convention in Chicago August 19. Women’s health and access to abortion, excess profitability by “corporate” drug manufacturers, hospitals and insurers, inadequate price transparency, uneven access and household affordability will be core themes in speeches and ads, with a promise to reverse the Dobb’s ruling by the Supreme Court punctuating every voter outreach.
Healthcare, to the Democratic-leaning voters is a right, not a privilege.
Its majority think it should be universally accessible, affordable, and comprehensive akin to Medicare. They believe the status quo isn’t working: the federal government should steward something better.
Here’s what we know for sure:
Foreign policy will be a secondary focus. The campaigns will credential their teams as world-savvy diplomats who seek peace and avoid conflicts. Nationalism vs. globalism will be key differentiator for the White House aspirants but domestic policies will be more important to most voters.
Healthcare reform will be a more significant theme in Campaign 2024 in races for the White House, U.S. Senate, U.S. House of Representatives and Governors. Dissatisfaction with the status quo and disappointment with its performance will be accentuated.
The White House campaigns will be hyper-negative and disinformation used widely (especially on healthcare issues). A prosecutorial tone is certain.
Given the consequence of the SCOTUS’ Chevron ruling limiting the role and scope of agency authority (HHS, CMS, FDA, CDC, et al), campaigns will feature proposed federal & state policy changes and potential Cabinet appointments in positioning their teams. Media speculation will swirl around ideologues mentioned as appointees while outside influencers will push for fresh faces and new ideas.
Consumer prices and inflation will be hot-button issues for pocketbook voters: the health industry, especially insurers, hospitals and drug companies, will be attacked for inattention to affordability.
Substantive changes in health policies and funding will be suspended until 2025 or later. Court decisions, Executive Orders from the White House/Governors, and appointments to Cabinet and health agency roles will be the stimuli for changes. Major legislative and regulatory policy shifts will become reality in 2026 and beyond. Temporary adjustments to physician pay, ‘blame and shame’ litigation and Congressional inquiries targeting high profile bad actors, excess executive compensation et al and state level referenda or executive actions (i.e. abortion coverage, price-containment councils, CON revisions et al) will increase.
Total healthcare spending, its role in the economy and a long-term vision for the entire system will not be discussed beneath platitudes and promises. Per the Congressional Budget Office, healthcare as a share of the U.S. GDP will increase from 17.6% today to 19.7% in 2032. Spending is forecast to increase 5.6% annually—higher than wages and overall inflation. But it’s too risky for most politicians to opine beyond acknowledgment that “they feel their pain.”
My take:
Regardless of the election outcome November 5, the U.S. healthcare industry will be under intense scrutiny in 2025 and beyond. It’s unavoidable.
Discontent is palpable. No sector in U.S. healthcare can afford complacency. And every stakeholder in the system faces threats that require new solutions and fresh voices.
In the Congressional Budget Office’ latest report on the status of health insurance coverage from the 2023 National Health Interview Survey released last week, a cautiously optimistic picture of coverage is presented:
“In 2023, 25.0 million people of all ages (7.6%) were uninsured at the time of interview. This was lower than, but not significantly different from 2022, when 27.6 million people of all ages (8.4%) were uninsured. Among adults ages 18 64, 10.9% were uninsured at the time of interview, 23.0% had public coverage, and 68.1% had private health insurance coverage.
The percentage of adults ages 18-64 who were uninsured in 2023 (10.9%) was lower than the percentage who were uninsured in 2022 (12.2%).
Among children ages 0–17 years, 3.9% were uninsured, 44.2% had public coverage, and 54.0% had private health insurance coverage.
The percentage of people younger than age 65 with exchange-based coverage increased from 3.7% in 2019 to 4.8% in 2023.”
That represents the highest level of coverage in modern history. Later, it adds important context: The percentage of adults ages 18–64 who were uninsured decreased between 2019 and 2023 for all family income groups shown except for adults in families with incomes greater than 400% FPL. Notably, a period in which the Covid-19 pandemic prompted federal government’s emergency funding so households and businesses could maintain their coverage.
“Among adults with incomes below 100% FPL, the percentage who were uninsured in 2023 (20.2%) was lower than, but not significantly different from, the percentage who were uninsured in 2022 (22.7%).
Among adults with incomes 100% to less than 200% FPL, the percentage who were uninsured decreased from 22.3% in 2022 to 19.1% in 2023.
Among adults with incomes 200% to 400% FPL, the percentage who were uninsured decreased from 14.2% in 2022 to 11.5% in 2023.
No significant difference was observed in the percentage of adults with incomes above 400% FPL who were uninsured between 2022 (4.1%) and 2023 (4.3%).”
In 2023, among adults ages 18–64, the percentage who were uninsured was highest among health insurance coverage of any type was higher for those with higher household income but decreased coverage in 2023 correlated to ethnicity, non-expansion of state Medicaid programs: From 2019 to 2023.”
And decreases in the ranks of the uninsured were noted across all ethnic groups:
Among Hispanic adults, from 29.7% to 24.8%
Among Black non-Hispanic adults, from 14.7% to 10.4% in 2023
Among White non-Hispanic adults, decreased from 10.5% to 6.8%
Among Asian non-Hispanic adults, from 8.8% to 4.4% in 2023.
The New York Times noted “The drops cut significantly into gaps between ethnic groups.The uninsured rate among Black Americans, for example, was almost 8% higher than for white Americans in 2010, and was only 4%higher in 2022. The data points to the broad effects of the Affordable Care Act, the landmark law President Barack Obama signed in 2010 that created new state and federal insurance marketplaces and expanded Medicaid to millions of adults. National uninsured rates have continued to drop in recent years, hitting a record low in early 2023.”
But the report also flags a reversal of the trend: “The uninsured share of the population will rise over the course of the next decade, before settling at 8.9% in 2034, largely as a result of the end of COVID-19 pandemic–related Medicaid policies, the expiration of enhanced subsidies available through the Affordable Care Act health insurance Marketplaces, and a surge in immigration that began in 2022. The largest increase in the uninsured population will be among adults ages 19–44. Employment-based coverage will be the predominant source of health insurance, and as the population ages, Medicare enrollment will grow significantly. After greater-than-expected enrollment in 2023, Marketplace enrollment is projected to reach an all-time high of twenty-three million people in 2025.”
My take:
A close reading of this report suggests its forecast might be overly optimistic. it paints a best-case picture of health insurance coverage that under-estimates the realities of household economics and marketplace trends and over-estimates the value proposition promoted by health insurers to their customers. My conclusion is based on four trends that suggest coverage might slip more than the report suggests:
The affordability of healthcare insurance is increasingly problematic to lower- and middle-income households who face inflationary prices for housing, food, energy and transportation. The CBO report verifies that household income is key to coverage and working age populations are most-at risk of losing its protections. Subsidies to fund premiums for those eligible, employer plans that expose workers to high deductibles and increased non-covered services are likely to push fewer to enroll as premiums become unaffordable to working age adults and unattractive to their employers. As outlined in a sobering KFF analysis, half of the adult population is worried about the affordability of their healthcare—and that includes 48% who have health insurance. And wages in the working age population are not keeping pace with prices for food, shelter and energy, leaving healthcare expenses including their insurance premiums and out-of-pocket obligations at greater risk.
The value proposition for health insurance coverage is eroding among employers, consumers and lawmakers. To large employers that provide employee insurance, medical costs are forcing benefits reduction or cessation altogether. Insurance has not negated their medical costs. To small employers, it’s an expensive bet to recruit and keep their workforce. To government sponsors (i.e. Medicare, Medicaid, VHA, et al), insurance is a necessary but increasingly expensive obligation with growing dependence on private insurers to administer their programs. State and federal regulators are keen to limit public spending and address disparities in their public insurance programs. All recognize that private insurers play a necessary role in the system and all recognize that confidence in health insurance protections is suspect. Thus, increased regulation of private insurers is likely though unwelcome by its members.
Public funding for government payers will be increasingly limited increasing insurer dependence on private capital for sustainability and growth. Funding for Medicare, Medicaid, Veterans and Military Health, Public Health et al are dependent on appropriations and tax collections. All are structured to invite private insurer participation: all are seeing corporate insurers seize market share from their weaker competitors. The issues are complex and controversial as evidenced by the ongoing debates about fairness in Medicare Advantage and administration of Medicaid expansion among others. And polls indicate widespread dissatisfaction with the system and lack of confidence in its insurers, hospitals, physicians or the government to fix it.
Access to private capital for private health insurers is shrinking enabling corporate insurers to play bigger roles in financing and delivering services. Private investments in healthcare services (i.e. hospitals, physicians, clinics) has slowed and momentum has shifted from sellers to buyers seeking less risk and higher returns. Capital deployment by corporate insurers i.e. UHG, HUM et al has resulted in vertically-integrated systems of health inclusive of physician services, drug distribution, ASCs and more. And funding for AI-investments that lower their admin costs and increase their contracting leverage with providers is a strategic advantage for corporate insurer that operate nationally at scale. Unless the federal government bridles their growth (which is unlikely), corporate insurers will control national coverage while others fail.
Thus, no one knows for sure what coverage will be in 2034 as presented in the CBO report. Its analysis appropriately considers medical inflation, population growth and an incremental shift to value-based purchasing in healthcare, but it fails to accommodate highly relevant changes in the capital markets, corporate insurer shareholder interests and voter sentiment.
P.S. This is an important week for healthcare: Today marks the two-year anniversary of the Supreme Court’s Dobbs decision that overturned Roe v. Wade, ending the constitutional right to an abortion that pushed reproductive rights to states.
And Thursday in Atlanta, President Joe Biden and former President Donald Trump will make history in the first presidential debate between an incumbent and a former president.
Reproductive rights will be a prominent theme along with immigration and border security as wedge issues for voters.
The economy and inflation are the issues of most consequence to most voters, so unless the campaigns directly link healthcare spending and out of pocket costs to voter angst about their household finances, not much will be said.
Notably, half of the U.S. population have unpaid medical bills and medical debt is directly related to their financial insecurity. Worth watching.
The proposal would attempt to stop credit reporting companies from sharing medical debts with lenders.
The Consumer Financial Protection Bureau (CFPB) has proposed a rule intended to remove medical bills from most credit reports, increase privacy protections, help to increase credit scores and loan approvals and prevent debt collectors from using the credit reporting system to coerce people to pay.
The proposal would attempt to stop credit reporting companies from sharing medical debts with lenders and prohibit lenders from making lending decisions based on medical information.
CFPB framed the proposed rule as part of its efforts to address the burden of medical debt and what it called manipulative credit reporting practices.
WHAT’S THE IMPACT?
In 2003, Congress restricted lenders from obtaining or using medical information, including information about debts, through the Fair and Accurate Credit Transactions Act. But federal agencies then issued a special regulatory exception to allow creditors to use medical debts in their credit decisions.
The CFPB is proposing to close the regulatory loophole it said has kept vast amounts of medical debt information in the credit reporting system. The proposed rule is intended to ensure that medical information does not unjustly damage credit scores, and would help keep debt collectors from coercing payments for inaccurate or false medical bills.
Internal research from CFPB shows that a medical bill on a person’s credit report is not a good predictor of whether they will repay a loan. In fact, the analysis shows that medical debts penalize consumers by making underwriting decisions less accurate and leading to thousands of denied applications on mortgages that consumers would repay.
Since these are loans people will repay, the CFPB expects lenders will also benefit from improved underwriting and increased volume of safe loan approvals. In terms of mortgages, the CFPB expects the proposed rule would lead to the approval of approximately 22,000 additional, safe mortgages every year.
In December 2014, the CFPB released a report showing that medical debts provide less predictive value to lenders than other debts on credit reports. Then in March 2022, it released a report estimating that medical bills made up $88 billion of reported debts on credit reports. In that report, the CFPB announced that it would assess whether credit reports should include data on unpaid medical bills.
Since the March 2022 report, the three nationwide credit reporting conglomerates – Equifax, Experian and TransUnion – announced they would take many of those bills off credit reports, and FICO and VantageScore, the two major credit scoring companies, have decreased the degree to which medical bills impact a consumer’s score.
Despite these voluntary industry changes, 15 million Americans still have $49 billion in outstanding medical bills in collections appearing in the credit reporting system.
The complex nature of medical billing, insurance coverage and reimbursement, and collections means that medical debts that continue to be reported are often inaccurate or inflated, CFPB said.
Additionally, the changes by FICO and VantageScore have not eliminated the credit score difference between people with and without medical debt on their credit reports. CFPB expects that Americans with medical debt on their credit reports will see their credit scores rise by 20 points, on average, if the proposed rule is finalized.
Specifically, the proposed rule would remove the exception that broadly permits lenders to obtain and use information about medical debt to make credit eligibility determinations. Lenders would continue to be able to consider medical information related to disability income and similar benefits, as well as medical information relevant to the purpose of the loan, so long as certain conditions are met.
The rule would also prohibit credit reporting companies from including medical debt on credit reports sent to creditors when creditors are prohibited from considering it. Additionally, it would prohibit lenders from taking medical devices as collateral for a loan, and bans lenders from repossessing medical devices, like wheelchairs or prosthetic limbs, if people are unable to repay the loan.
THE LARGER TREND
The CFPB began its rulemaking in September 2023 with the goals of ending coercive debt collection practices and limiting the role of medical debt in the credit-reporting system.
The CFPB also published in 2022 a report describing the effects of medical debt, along with a bulletin on the No Surprises Act to remind credit reporting companies and debt collectors of their legal responsibilities under that legislation.
As campaigns for November elections gear up for early voting and Congress considers bipartisan reforms to limit consolidation and enhance competition in U.S. healthcare, prospective voters are sending a cleat message to would-be office holders:
Healthcare Affordability must be addressed directly, transparently and now.
Polling by Gallup, Kaiser Family Foundation and Pew have consistently shown healthcare affordability among top concerns to voters alongside inflation, immigration and access to abortion. It is higher among Democratic-leaning voters but represents the majority in every socio-economic cohort–young and old, low and middle income and households with/without health insurance coverage., urban and rural and so on.
It’s understandable: household economic security is declining: per the Federal Reserve’s latest household finances report:
72% of US adults say they are doing well financially (down from 78% in 2021)
54% say they have emergency savings to cover 3 months expenses ($400)—down from high of 59% in 2015.
69% say their finances deteriorated in 2023. They’re paying more for groceries, fuel, insurance premiums and childcare.
Renters absorbed a 10% increase last year and mortgage interest spike has put home ownership beyond reach for 6 in 10 households
Thus, household financial security is the issue and healthcare expenses play a key role. Drug prices, hospital consolidation, price transparency and corporate greed will get frequent recognition in candidate rhetoric. “Reform” will be promised. And each sector in the industry will offer solutions that place the blame on others.
Granted, the U.S. health system lacks a uniform definition of healthcare affordability. It’s a flaw. In the Affordable Care Act, it was framed in the context of an individual’s eligibility for government-subsidized insurance coverage (8.39% adjusted gross income for households between 100% and 400% of the federal poverty level). But a broader application to the entire population was overlooked. Nonetheless, economists, regulators and consumers recognize the central role healthcare affordability plays in household financial security.
Handicapping the major players potential to win the hearts and minds of voters about healthcare affordability is tricky:
Each major sector has seen the ranks of its membership decrease and the influence (and visibility) of its bigger players increase. They’re easy targets for industry critics.
Each sector is seeing private equity and non-traditional players play bigger roles. The healthcare landscape is expanding beyond the traditional players.
Each sector is struggling to make their cases for incremental reforms while employers, legislators and consumers want more. Bipartisan support for anything is a rarity: an exception is antipathy toward healthcare consolidation and lack of price transparency.
All recognize that affordability is complicated. Unit cost and price increases for goods and services are the culprit: excess utilization is secondary.
Against this backdrop, here’s a scorecard on the current state of preparedness as each navigates affordability going into Campaign 2024:
Sector
Advantages
Disadvantages
Handicap Score1=Unprepared to5=Well Prepared
Hospitals
Community presence (employer, safety net) Economic impact Influence in Congress Scale: 30% of spending + direct employment of 52% of physicians Access to capital
Lack of costs & price transparency Unit costs inflation due to wage, supply chain & admin Shifting demand for core services. Low entry barriers for key services Regulator headwind (state, federal). Operating, governing culture Value proposition erosion with employers, pre-Medicare populations Consumer orientation
3
Physicians
Consumer trust Influence in Congress Shared savings (Medicare) Essentiality Specialization Access to technology
Care continuity Inadequacy of primary care Disorganization (fragmentation) Value of shared savings to general population (beyond Medicare) Culture: change-averse (education, licensing performance measurement, et al) Data: costs, outcomes
2
Drug Manufacturers
Increasing product demand Influence in Congress Public trust in drug efficacy Insurance structure that limits consumer price sensitivity to OOP Potential for AI -enabled discovery, market access Access to private capital Congress’ constraint on PBMs
Unit cost escalation Lack of price transparency Growing disaffection for FDA Long-term Basic Research Funding State Price Control Momentum Market access Restrictive Formulary Growth Transparency in Distributor-PBM business relationships Public perception of corporate greed
2
Health Insurers
Availability of claims, cost data Employer tax exemptions Growing government market Plan design: OOP, provider access Public association: coverage = financial security Access to private capital
Escalating premiums Declining group market Growing regulatory scrutiny (consolidation, data protection) Tension with health systems Value proposition erosion among government, employers, consumers
4
Retail Health
Non-incumbrance of restrictive regulatory framework Consumer acceptance Breadth of product opportunities Access to private capital Opportunity for care management (i.e. CVS- Epic) Operational orientation to consumers (convenience, pricing, et al) Potential with employers,
Lack of access, coordination with needed specialty care Threat of regulatory restraint on growth Risks associated with care management models
3
The biggest, investor-owned health insurers own the advantage today. As in other sectors, they’re growing faster than their smaller peers and enjoy advantages of scale and private capital access to fund their growth. A handful of big players in the other sectors stand-out, but their affordability solutions are, to date, not readily active.
In each sector above, there is consensus that a fundamental change in the structure, function and oversight of the U.S. health is eminent. In all, tribalism is an issue: publicly-owned, not for profits vs. investor-owned, independent vs. affiliated, big vs. small and so on.
Getting consensus to address affordability head on is hard, so not much is done by the sectors themselves. And none is approaching the solution in its necessary context—the financial security of a households facing unprecedented pressures to make ends meet. In all likelihood, the bigger, more prominent organizations in their ranks of these sectors will deliver affordability solutions well-above the lowest common denominators that are comfortable for most Thus, health care affordability will be associated with organizational brands and differentiated services, not the sectors from which their trace their origins. And it will be based on specified utilization, costs, outcome and spending guarantees to consumers and employers that are reasonable and transparent.
“Incrementalism.” The word is perceived as the enemy of hope for universal health care in the United States.
Those who advocate for single-payer, expanded Medicare for all tend to be on the left side of the political spectrum, and we have advanced the movement while pushing back on incremental change. But the profit-taking health industry giants in what’s been called the medical-industrial complex are pursuing their own incremental agenda, designed to sustain the outrageously expensive and unfair status quo.
In recent years, as the financial sector of the U.S. economy has joined that unholy alliance, scholars have begun writing about the “financialization” of health care.
It has morphed into the medical-financial-industrial complex (MFIC) so vast and deeply entrenched in our economy that a single piece of legislation to achieve our goal–even with growing support in Congress–remains far short of enough votes to enact.
If we are to see the day when all Americans can access care without significant financial barriers, policy changes that move us closer to that goal must be pursued as aggressively as we fight against the changes that push universal health care into the distant future. Labeling all positive steps toward universal health care as unacceptable “incrementalism” could have the effect of aiding and abetting the MFIC and increase the chances of a worst-case scenario: Medicare Advantage for all, a goal of the giants in the private insurance business. But words matter. Instead of “incremental,” let’s call the essential positive steps forward as “foundational” and not undermine them.
The pandemic crisis exposed the weaknesses of our health system. When millions of emergencies in the form of COVID-19 infections overtook the system, most providers were ill-prepared and understaffed. More than 1.1 million U.S. citizens died of COVID-19-related illness, according to the Centers for Disease Control.
For years, the MFIC had been advancing its agenda, even as the U.S. was losing ground in life expectancy and major measures of health outcomes. While health care profits soared in the years leading up to and during the pandemic, those of us in the single-payer movement demanded improved, expanded Medicare for all. And we were right to do so. Progress came through almost every effort. The number of advocates grew, and more newly elected leaders supported a single-payer plan. Bernie Sanders’ 2016 presidential bid proved that millions of Americans were fed up with having to delay or avoid care altogether because it simply cost too much or because insurance companies refused to cover needed tests, treatments and medications.
But as the demand for systemic overhaul grew, the health care industry was making strategic political contributions and finding ways to gain even more control of health policy and the political process itself.
Over the years, many in the universal health care movement have opposed foundational change for strategic reasons. Some movement leaders believed that backing small changes or tweaks to the current system at best deflected from our ultimate goal. And when the Patient Protection and Affordable Care Act was passed, many on the left viewed it as a Band-Aid if not an outright gift to the MFIC. While many physicians in our movement knew that the law’s Medicaid expansion and the provisions making it illegal for insurers to refuse coverage to people with preexisting conditions would save many thousands of lives, they worried that the ACA would further empower big insurance companies. Both positions were valid.
After the passage of the ACA, more of us had insurance cards in our wallets and access to needed care for the first time, although high premiums and out-of-pocket costs have become insurmountable barriers for many. Meanwhile, industry profits soared.
The industry expanded its turf. Hospitals grew larger, stand-alone urgent care clinics, often owned by corporate conglomerates, opened on street corners in cities across the country, private insurance rolls grew, disease management schemes proliferated, and hospital and drug prices continued the march upward. The money flowing into the campaign coffers of political candidates made industry-favored incremental changes an easier lift.
To change this “system” would require an overhaul of the whole economy. Single-payer advocates must consider that herculean task as they continue their work. We must understand that the true system of universal health care we envision would also disrupt the financial industry – banks, collection agencies, investors – an often-forgotten but extraordinarily powerful segment of the corporate-run complex.
Even if the research and data show that improved, expanded Medicare for all would save money and lives (and they do show that), that is not motivating for the finance folks, who fear that without unfettered control of health care, they might profit less. Eliminating medical bills and debt would be marvelous for patients but not for a large segment of the financial community, including bankruptcy attorneys.
Following the money in U.S. health care means understanding how deep and far the tentacles of profit reach, and how embedded they are now.
We know the MFIC positioned itself to continue growing profits and building more capacity. The industry made steady, incremental progress toward that goal. There is no illusion that better overall health for Americans is the mission of the stockholders who drive this industry. No matter what the marketers tell us, patients are not their priority. If too many of us get healthier, we might not use as much care and generate as much money for the owners and providers. Private insurers want enough premiums and government perks to keep flowing their way to keep the C-Suite and Wall Street happy.
More than health insurers
Health insurers are far from the only rapidly expanding component of the MFIC. A recent documentary, “American Hospitals: Healing a Broken System,” for example, explores a segment of the U.S. health industry that is often overlooked by policymakers and the media. Though they were unprepared for the national health crisis, hospitals endured the pandemic in this country largely because the dedicated doctors, nurses and ancillary staff risked their own lives to keep caring for COVID-19 patients while everything from masks, gowns and gloves to thermometers and respirators were in short supply. But make no mistake, many hospitals were still making money through the pandemic. In fact, some boosted their already high profits, and private insurance companies had practically found profit-making nirvana. Patients put off everything from colonoscopies to knee replacements, physical therapy to MRIs. Procedures not done meant claims not submitted, while monthly insurance premiums kept right on coming and right on increasing.
The pandemic was a time of turmoil for most businesses and families, yet the MFIC took its share of profits. It was pure gold for many hospitals until staffing pressures and supply issues grew more dire, COVID patients were still in need of care, and more general patient care needs started to reemerge.
We might be forgiven for thinking there wasn’t much regulating or legislating done around health care during the pandemic years. We’d be wrong. There was a flurry of legislation at the state level as some states took on the abuses of the private insurance industry and hospital billing practices.
And the movement to improve and expand traditional Medicare to cover all of us stayed active, though somewhat muted. The bills before Congress that expanded access to Medicaid during the pandemic through a continuous enrollment provision offered access to care for millions of people. Yet as that COVID-era expansion ended, many of those patients were left without coverage or access to care. This might have been a chance to raise the issue loudly, but the social justice movement did not sufficiently activate national support for maintaining continuous enrollment in Medicaid. Is that the kind of foundational change worth fighting for? I would argue it most certainly is.
As those previously covered by Medicaid enter this “unwinding” phase, many will be unable to secure equivalent or adequate health insurance coverage. The money folks began to worry as coverage waned. After all, sick people will show up needing care and they will not be able to pay for it. As of this writing, patient advocacy groups are largely on the sidelines.
But Allina Health took action. The hospital chain announced it would no longer treat patients with medical debt. After days of negative press, the company did an about-face.
Throughout the country, even as the pandemic loomed, the universal, single-payer movement focused on explaining to candidates and elected officials why improving and expanding Medicare to cover all of us not only is a moral imperative but also makes economic sense. In many ways, the movement has been tremendously effective: More than 130 city and county governing bodies have passed resolutions in support of Medicare for all, including in Seattle, Denver, Cincinnati, Washington, D.C., Tampa, Sacramento, Los Angeles, St. Louis, Atlanta, Duluth, Baltimore, and Cook County (Chicago).
The Medicare for All Act, sponsored by Rep Pramila Jayapal (D-Wash.) and Sanders (I-Vt.) has 113 co-sponsors in the House and 14 in the Senate. Another bill allowing states to establish their own universal health care programs has been introduced in the House and will be introduced soon in the Senate.
Moving us closer
The late Dr. Quentin Young was a young Barack Obama’s doctor in Chicago. Young spoke to his president-in-the-making patient about universal health care and Obama, then a state legislator, famously answered that he would support a single-payer plan if we were starting from scratch. Many in the Medicare–for-all movement dismissed that statement as accepting corporate control of health care.
But Young would steadfastly advocate for single-payer health care for years to come and as one of the founding forces behind Physicians for a National Health Program. Once Dr. Young was asked if the movement should support incremental changes. He answered, “If a measure makes it easier and moves us closer to achieving health care for all of us, we should support that wholeheartedly. And if a measure makes it harder to get to single-payer, we need to oppose it and work to defeat that measure.” Many people liked that response. Others were not persuaded.
But in recent years, PHNP has become a national leader in a broad-based effort to halt the privatization of Medicare through so-called Medicare Advantage plans and other means. A case can be made that those are incremental/foundational but essential steps to achieving the ultimate goal.
We must fight incrementally sometimes, for instance when traditional Medicare is threatened with further privatization. Bit by painful bit, a program that has served this nation so well for more than 50 years will be carved up and given over to the private insurance industry unless the foundational steps taken by the industry are met with resistance and facts at every turn. We can achieve our goal by playing the short game as well as the long game. Foundational change can be and has been powerful. It just has to be focused on the health and well-being of every person.
Today is the federal income Tax Day. In 43 states, it’s in addition to their own income tax requirements. Last year, the federal government took in $4.6 trillion and spent $6.2 trillion including $1.9 trillion for its health programs. Overall, 2023 federal revenue decreased 15.5% and spending was down 8.4% from 2022 and the deficit increased to $33.2 trillion. Healthcare spending exceeded social security ($1.351 trillion) and defense spending ($828 billion) and is the federal economy’s biggest expense.
Along with the fragile geopolitical landscape involving relationships with China, Russia and Middle East, federal spending and the economy frame the context for U.S. domestic policies which include its health system. That’s the big picture.
Today also marks the second day of the American Hospital Association annual meeting in DC. The backdrop for this year’s meeting is unusually harsh for its members:
Increased government oversight:
Five committees of Congress and three federal agencies (FTC, DOJ, HHS) are investigating competition and business practices in hospitals, with special attention to the roles of private equity ownership, debt collection policies, price transparency compliance, tax exemptions, workforce diversity, consumer prices and more.
Medicare payment shortfall:
CMS just issued (last week) its IPPS rate adjustment for 2025: a 2.6% bump that falls short of medical inflation and is certain to exacerbate wage pressures in the hospital workforce. Per a Bank of American analysis last week, “it appears healthcare payrolls remain below pre-pandemic trend” with hospitals and nursing homes lagging ambulatory sectors in recovering.”
Persistent negative media coverage:
The financial challenges for Mission (Asheville), Steward (Massachusetts) and others have been attributed to mismanagement and greed by their corporate owners and reports from independent watchdogs (Lown, West Health, Arnold Ventures, Patient Rights Advocate) about hospital tax exemptions, patient safety, community benefits, executive compensation and charity care have amplified unflattering media attention to hospitals.
Physicians discontent:
59% of physicians in the U.S. are employed by hospitals; 18% by private equity-backed investors and the rest are “independent”. All are worried about their income. All think hospitals are wasteful and inefficient. Most think hospital employment is the lesser of evils threatening the future of their profession. And those in private equity-backed settings hope regulators leave them alone so they can survive. As America’s Physician Group CEO Susan Dentzer observed: “we knew we’re always going to need hospitals; but they don’t have to look or operate the way they do now. And they don’t have to be predicated on a revenue model based on people getting more elective surgeries than they actually need. We don’t have to run the system that way; we do run the healthcare system that way currently.”
The Value Agenda in limbo:
Since the Affordable Care Act (2010), the CMS Center for Innovation has sponsored and ultimately disabled all but 6 of its 54+ alternative payment programs. As it turns out, those that have performed best were driven by physician organizations sans hospital control. Last week’s release of “Creating a Sustainable Future for Value-Based Care: A Playbook of Voluntary Best Practices for VBC Payment Arrangements.” By the American Medical Association, the National Association of ACOs (NAACOs) and AHIP, the trade group representing America’s health insurance payers is illustrative. Noticeably not included: the American Hospital Association because value-pursuers think for hospitals it’s all talk.
National insurers hostility:
Large, corporate insurers have intensified reimbursement pressure on hospitals while successfully strengthening their collective grip on the U.S. health insurance sector. 5 insurers control 50% of the U.S. health insurance market: 4 are investor owned. By contrast, the 5 largest hospital systems control 17% of the hospital market: 1 is investor-owned. And bumpy insurer earnings post-pandemic has prompted robust price increases: in 2022 (the last year for complete data and first year post pandemic), medical inflation was 4.0%, hospital prices went up 2.2% but insurer prices increased 5.9%.
Costly capital:
The U.S. economy is in a tricky place: inflation is stuck above 3%, consumer prices are stable and employment is strong. Thus, the Fed is not likely to drop interest rates making hospital debt more costly for hospitals—especially problematic for public, safety net and rural hospitals. The hospital business is capital intense: it needs $$ for technologies, facilities and clinical innovations that treat medical demand. For those dependent on federal funding (i.e. Medicare), it’s unrealistic to think its funding from taxpayers will be adequate. Ditto state and local governments. For those that are credit worthy, capital is accessible from private investors and lenders. For at least half, it’s problematic and for all it’s certain to be more expensive.
Campaign 2024 spotlight:
In Campaign 2024, healthcare affordability is an issue to likely voters. It is noticeably missing among the priorities in the hospital-backed Coalition to Strengthen America’s Healthcare advocacy platform though 8 states have already created “affordability” boards to enact policies to protect consumers from medical debts, surprise hospital bills and more.
Understandably, hospitals argue they’re victims. They depend on AHA, its state associations, and its alliances with FAH, CHA, AEH and other like-minded collaborators to fight against policies that erode their finances i.e. 340B program participation, site-neutral payments and others. They rightfully assert that their 7/24/365 availability is uniquely qualifying for the greater good, but it’s not enough. These battles are fought with energy and resolve, but they do not win the war facing hospitals.
AHA spent more than $30 million last year to influence federal legislation but it’s an uphill battle. 70% of the U.S. population think the health system is flawed and in need of transformative change. Hospitals are its biggest player (30% of total spending), among its most visible and vulnerable to market change.
Some think hospitals can hunker down and weather the storm of these 8 challenges; others think transformative change is needed and many aren’t sure. And all recognize that the future is not a repeat of the past.
For hospitals, including those in DC this week, playing victim is not a strategy. A vision about the future of the health system that’s accessible, affordable and effective and a comprehensive plan inclusive of structural changes and funding is needed. Hospitals should play a leading, but not exclusive, role in this urgently needed effort.
Lacking this, hospitals will be public utilities in a system of health designed and implemented by others.
Published this week in The Atlantic, this piece chronicles the increase in Americans using crowdfunding sites like GoFundMe to cover—or at least attempt to cover—their catastrophic medical expenses. Envisioned as a tool to fund “ideas and dreams,” the GoFundMe platform saw a 25-fold increase in the number of campaigns dedicated to medical care from 2011 to 2020.
Medical campaigns have garnered at least one third of all donations and raised $650M in contributions.
The article’s accounts of life-saving care leading to bankrupting medical bills are heartbreaking and familiar, and despite some success stories, the average GoFundMe medical campaign falls well short of its target donation goal.
The Gist:
Although unfortunately not surprising, these crowdfunding stats reflect ournation’s healthcare affordability crisis.
Online campaigns can alleviate real financial burdens for some people; however, they come at the costs of publicly exposing personal medical information, potentially offering false hope, and financially imposing on friends and family.
The majority of personal bankruptcies are caused by medical expenses, and recent changes like removingsome levels of medical debt from credit reports are only a small step toward reducing the personal financial effects of medical debt.
Absent larger-scale healthcare payment and coverage reform, healthcare industry leaders continue to be challenged with finding ways to decouple the provision of essential medical care from the risk of financial ruin for patients.
Nearly 50% of U.S. adults report struggling to keep up with the cost of healthcare, with four in ten ringing in the new year with medical debt. Medical debt is a major burden that often forces people to delay–and sometimes forgo–access to care. Not only do outstanding medical bills undermine health, but they also represent the most common type of collections, with estimates ranging anywhere from $81 to $140 billion.
With problematic hospital practices gaining national media attention – including rejecting appointments for patients with outstanding medical bills and going so far as to sue such patients – the issue of medical debt is front and center for many Americans.
A glimpse into the state of hospital billing practices
Hospital watchdogs have started collecting valuable data on hospital billing practices to inform patients about these practices and potentially put pressure on hospitals to improve.
In an effort to capture the varied nature of hospital billing and collection practices, the Lown Institute is building a database of financial assistance policies and billing and collection practices across 2,500 hospitals with the support of Arnold Ventures. Initial results are expected to be available in mid-2024 with a full report issued in 2025.
Also interested in evaluating the current state of hospital’s financial practices, in 2021, the Leapfrog Group added questions to their hospital survey around billing and collections. Researchers from the Leapfrog Group, Northwestern University Feinberg School of Medicine, and Johns Hopkins University School of Medicine published a recent analysis of this data in JAMAwhere they found that many hospitals are still falling short when it comes to billing ethics. Although the data set of 2,270 hospitals was not nationally representative, it provides an interesting glimpse into the billing practices of some U.S. hospitals.
Here are the key takeaways:
754 hospitals (33.2%) reported that they “take legal action against patients for late payment or insufficient payment of a medical bill.” Rural hospitals were 38% more likely than urban hospitals to take legal action against patients.
1,020 (44.9%) hospitals did not routinely send patients itemized bills within 30 days of final claims adjudication or date of service for patients without insurance.
125 (5.5%) hospitals did not provide access to billing representatives capable of investigating billing errors, offering price adjustment, and establishing payment plans.
Ultimately, only 38% of surveyed hospitals reported meeting all three proposed billing quality standards. Interestingly, hospitals with worse Leapfrog safety grades were less likely to meet all three billing standards compared to hospitals with better grades. It’s not clear what’s behind this pattern, but it could be an issue of capacity (hospitals with more resources and staff have an easier time abiding by safety protocol and billing standards), or potentially profiteering (hospitals more concerned with making money may be both understaffing hospitals and suing patients).
So, how can we encourage better billing practices and reduce harm caused by medical debt?
The JAMA study authors recommend standardizing measurement and reporting of hospital billing practices to “increase accountability, reduce variation in billing practices, and reduce barriers in access to care in the US.”
Some states are taking these recommendations to the policy-level, working to make healthcare more affordable for patients. To date, eight states limit medical debt interest and two states restrict credit reporting of medical debt. Current policy proposals on the docket include New York’s Senate Bill S5909B, which seeks to ban hospitals from suing patients making less than 400% of the federal poverty level (FPL).
This research is important to not only provide further insight into how hospitals financially support, or undermine, their patients, but also inform policy efforts to improve healthcare affordability and hospital accountability moving forward.