New data provided to Axios spells out just how outsized a role immigrants play on the high- and low-skilled ends of the economy keeping Americans alive and fed during the coronavirus crisis, Axios’ Stef Kight reports.
By the numbers: Immigrants make up an estimated 17% of the overall U.S. workforce. But the analysis by New American Economy (NAE) shows they’re more than one in four doctors, nearly half the nation’s taxi drivers and chauffeurs and a clear majority of farm workers.
Reporting to work in hospitals, restaurant kitchens, cabs or the fields — for jobs deemed “essential” by the government — many documented and undocumented workers are putting themselves at higher risk of COVID-19 infections.
Be smart: The share of immigrants in some health care roles are higher in states that have been hit hardest by the virus.
More than a third of California nurses are immigrants, as well as 29% of nurses in New York and New Jersey, according to NAE data.
Between the lines: A large percentage of farm workers, who help maintain food supplies, are unauthorized immigrants, as the New York Times reported.
Immigrants make up a small percentage of delivery workers nationwide, but one-third of delivery workers in New York are unauthorized immigrants, NAE director of quantitative research Andrew Lim told Axios.
The $2 trillion aid package does not include assistance for unauthorized immigrants.
The shortage of hospital beds in the U.S. didn’t happen by accident. It’s a result of both market pressures and public policy.
Why it matters: The bed shortage is one of many factors complicating America’s response to the new coronavirus. But if we want to have more beds and critical equipment on hand for the next pandemic, the government will need to make it happen — and pay for it.
How it happened: Health care resources, including hospital beds, are allocated mainly by market dynamics, not public-health blueprints.
Over the last 50 years, a great deal of care has shifted away from inpatient hospital settings and into outpatient services.
The motivation was to help control costs and improve the quality of care, while making it more convenient for patients.
Government also worked to directly cut the number of U.S. hospital beds, believing in a rule called Roemer’s Law, which said that “a hospital bed built would be a hospital bed filled,” driving up costs.
The push to reduce beds was embodied in a 1974 law that set up a health planning system in every state. A central objective was to get the U.S. below three hospital beds per 1,000 people, the level many think is now too low today.
And though it was repealed under President Ronald Reagan, the broader push to reduce capacity continued in many states.
The bottom line: If we want to have surge capacity of hospital beds and equipment in place for the next crisis, and if we don’t want to push health care costs higher, hospitals will need to acquire extra beds and then leave that surge capacity largely unused until the next crisis.
That means Congress would have to dictate that capacity by law, decide which hospitals to put it in, and fund it, while increasing the strategic stockpile of equipment like ventilators, masks and other protective equipment at the same time.
As worried Americans pack supermarket aisles in anticipation of quarantines and shelter-in-place orders, grocery workers like Courtney Meadows are working at a frantic pace to keep Americans fed and alive, and risking their own health in the process.
Meadows, a cashier at Kroger in Beckley, W.Va., said her store is the busiest she has seen it in 10 years on the job. “I have worked through snow scares, a blizzard, two derechos, holidays, anything that can impact a grocery store,” she told me. “This is the absolute worst I have seen it. It is a sea of people everywhere.”
Over the last week, I traveled to supermarkets across the Washington, D.C. region and interviewed workers from Virginia, Maryland, West Virginia and the District to hear—in their words—how COVID-19 is impacting them. These crowded stores I visited had few visible safeguards or protections for workers.
“We aren’t staying six feet away from the customers,” said Michelle Lee, a Safeway cashier in Alexandria, Va. “When we ring them up, they are like two feet away from us. We check out 200 customers a day. A doctor can wear a mask and protective gear. We don’t have all of that.”
Amber Stevens, a cashier at Shoppers in Prince George’s County, Md., expressed concern over social distancing as well. “I do still have a job to go to, but it isn’t helping me with social distancing because I am hands-on with customers,” she told me. “That is the scary part. Dealing with money, having to be so close to people.”
More than their own health, the grocery store employees I interviewed expressed the most concern about the safety of those around them: their loved ones at home, their elderly customers, their colleagues with underlying health conditions, and their neighbors in crowded apartment buildings. Several workers welled up with emotion as they described how hard it is to be unable to care for older relatives during the pandemic.
“All of that worry plus the stress of double the number of customers we normally have,” said Lisa Harris, a cashier at Kroger in Richmond, Va. “This isn’t just for one day. It is for weeks.”
As grocery workers put their lives on the line—often for low wages and few benefits—it is imperative that employers, policymakers, and even customers act with urgency to protect, support, and compensate them.
EMPLOYERS MUST KEEP GROCERY WORKERS HEALTHY
Employers need to implement immediate steps to reduce grocery workers’ exposure to COVID-19. First, employers should expand access to personal protective equipment (PPE) such as masks and gloves and end any restrictions on workers wearing them. While supplies of protective masks and gloves are extremely limited across the country, employers and policymakers should prioritize PPE for grocery workers as they become available. Employers should provide adequate cleaning supplies and hand sanitizer, regular opportunities for workers to wash their hands, and frequent equipment cleaning.
Second, stores should shorten hours and limit the number of customers at any given time. While several stores—including Trader Joe’s, Walmart, and Safeway—have limited store hours and introduced “senior only” hours, most stores are not following the CDC’s guidance of limiting gatherings to 50 people. Even tighter restrictions may be needed to keep workers safe as the virus spreads; for instance, some stores in China arechecking customers’ temperatures before they enter the store.
Third, grocery stores should implement additional measures to protect workers and enforce safe spacing of customers. Albertsons, which owns Safeway and 19 other grocery chains, was the first major company to announce they will install plexiglass “sneeze-guard” barriers at checkouts in its 2,200 stores over the next two weeks. Walmart and Kroger have made similar commitments, and other grocery stores should follow.
Even in the absence of specific CDC guidelines for grocery workers, employers should act boldly and creatively to modify stores to keep workers safe, continuously adapt to evolving best practices, and respond to safety priorities identified by unions like the United Food and Commercial Workers International Union (UFCW), which represents over 1.2 million workers.
INCREASE COMPENSATION AND OFFER HAZARD PAY
The coronavirus pandemic has put a harsh spotlight on the low wages that grocery workers earn for their life-saving work. At Kroger, the country’s second-largest grocery chain with 453,000 workers, the average hourly wage of cashiers is just $9.94 per hour, according to estimates on Indeed.com.
Lisa Harris, a Kroger cashier, described the financial hardships she and her low-wage colleagues face: “I have coworkers who stand all day serving people, and then have to go pay for their own groceries with food stamps. I am very lucky that my boyfriend works in pizza because that is our survival food. If we can’t afford to buy food, he brings home a pizza.”
Even in “normal” times, grocery workers—like other service and low-wage workers—deserve better wages. In these extreme times, adequately compensating them is even more imperative. As grocery sales soar and their stock prices rise, employers should provide additional compensation and hazard pay to their workers on the front line.
“I think that some pay increase would be wonderful,” Kroger cashier Courtney Meadows told me. “I don’t think they understand the toll that comes through in our lives. They don’t see it. They don’t see the panic on people’s faces.”
In response to the pandemic, the two largest grocery employers, Kroger and Walmart, have offered workers one-time bonuses of $300. Responding to pressure from the UFCW, Safeway and Shoppers are now offering an additional $2 per hour of hazard pay, while Whole Foods and Target are also raising pay $2 per hour.
These pay increases are an important start, but they don’t go far enough. The raises should be permanent, and enough to provide a family-sustaining wage to workers.
ENSURE ACCESS TO HEALTH INSURANCE AND EXTEND PAID SICK LEAVE
Now more than ever, paid sick leave and health insurance are critical for grocery workers. Well before the COVID-19 pandemic, hundreds of thousands of grocery workers didn’t receive paid sick leave from their employers. Responding to public outrage and pressure from employees and unions, most large employers now have updated their sick leave policy to respond to COVID-19. However, their policies don’t go far enough: They are temporary, focus narrowly on COVID-19, and are insufficient to meet the needs of workers.
Companies including Safeway, Kroger, and Walmart are now offering 14 days paid sick leave for workers with a confirmed COVID-19 diagnosis. But COVID-19 tests are in extremely short supply and many workers with suspected cases will be unable to get tested. Employers should modify paid leave policies to allow flexibility for ill workers to access the benefits even without a confirmed test, at least until testing is more widely available.
Policies should cover paid leave for grocery workers to care for their immediate family members or people they live with if they become ill. Employers should also compensate workers for any coronavirus-related medical bills that are not covered by their health insurance.
Employers should provide extra support to grocery workers who are especially high-risk, such as older workers and the immunocompromised. The most vulnerable workers may need to simply stay home during the pandemic and not work for weeks or months. Employers should do their part to ensure those workers have extended paid leave or other forms of adequate compensation and benefits, including health insurance.
CUSTOMERS CAN HELP KEEP GROCERY WORKERS SAFE
A major concern for the workers I interviewed was the actions of individual customers that could jeopardize their health. Many workers noted that customers continue to come to their store even when they are sick.
“Some customers will come through the line and cough or sneeze in their hand,” said Safeway cashier Michelle Lee. “If you are sick, you should stay home or cough in their elbow.”
Customers should do their part by keeping a safe distance from workers at checkout and throughout the store, practicing proper hygiene when coughing or sneezing, and staying home when ill.
RIGHT NOW, GROCERY WORKERS ARE EMERGENCY PERSONNEL
Other states should follow the lead of Minnesota and Vermont and designate grocery workers as emergency personnel, granting them the same protections and benefits as first responders and health workers.
“If we had an opportunity to get free child care, people like me could go in,” Matt Milzman, a 29-year-old Safeway cashier in Washington, D.C. and father of two small children, told me. “They need all the people they can. I am low risk and healthy. I would much rather me work than someone who is older with a million health problems.”
Grocery workers are among the true heroes of the pandemic, providing basic necessities to keep Americans alive, but also human comfort for their customers during an anxious time.
“I choose to be happy and positive,” cashier Courtney Meadows told me. “If you can talk and make someone laugh, that might be the only positive thing in their life that day. That is what I choose to do.”
We owe them not only our gratitude, but the protection, support, and compensation they deserve.
Worry that ‘all hands’ responses may expose doctors and nurses to infection prompts debate about prioritizing the survival of the many over the one.
Hospitals on the front lines of the pandemic are engaged in a heated private debate over a calculation few have encountered in their lifetimes — how to weigh the “save at all costs” approach to resuscitating a dying patient against the real danger of exposing doctors and nurses to the contagion of coronavirus.
The conversations are driven by the realization that the risk to staff amid dwindling stores of protective equipment — such as masks, gowns and gloves — may be too great to justify the conventional response when a patient “codes,” and their heart or breathing stops.
Northwestern Memorial Hospital in Chicago has been discussing a do-not-resuscitate policy for infected patients, regardless of the wishes of the patient or their family members — a wrenching decision to prioritize the lives of the many over the one.
Richard Wunderink, one of Northwestern’s intensive-care medical directors, said hospital administrators would have to ask Illinois Gov. J.B. Pritzker for help in clarifying state law and whether it permits the policy shift.
“It’s a major concern for everyone,” he said. “This is something about which we have had lots of communication with families, and I think they are very aware of the grave circumstances.”
Officials at George Washington University Hospital in the District say they have had similar conversations, but for now will continue to resuscitate covid-19 patients using modified procedures, such as putting plastic sheeting over the patient to create a barrier. The University of Washington Medical Center in Seattle, one of the country’s major hot spots for infections, is dealing with the problem by severely limiting the number of responders to a contagious patient in cardiac or respiratory arrest.
Several large hospital systems — Atrium Health in the Carolinas, Geisinger in Pennsylvania and regional Kaiser Permanente networks — are looking at guidelines that would allow doctors to override the wishes of the coronavirus patient or family members on a case-by-case basis due to the risk to doctors and nurses, or a shortage of protective equipment, say ethicists and doctors involved in those conversations. But they would stop short of imposing a do-not-resuscitate order on every coronavirus patient. The companies declined to comment.
Lewis Kaplan, president of the Society of Critical Care Medicine and a University of Pennsylvania surgeon, described how colleagues at different institutions are sharing draft policies to address their changed reality.
“We are now on crisis footing,” he said. “What you take as first-come, first-served, no-holds-barred, everything-that-is-available-should-be-applied medicine is not where we are. We are now facing some difficult choices in how we apply medical resources — including staff.”
The new protocols are part of a larger rationing of lifesaving procedures and equipment — including ventilators — that is quickly becoming a reality here as in other parts of the world battling the virus. The concerns are not just about health-care workers getting sick but also about them potentially carrying the virus to other patients in the hospital.
R. Alta Charo, a University of Wisconsin-Madison bioethicist, said that while the idea of withholding treatments may be unsettling, especially in a country as wealthy as ours, it is pragmatic. “It doesn’t help anybody if our doctors and nurses are felled by this virus and not able to care for us,” she said. “The code process is one that puts them at an enhanced risk.”
Wunderink said all of the most critically ill patients in the 12 days since they had their first coronavirus case have experienced steady declines rather than a sudden crash. That allowed medical staff to talk with families about the risk to workers and how having to put on protective gear delays a response and decreases the chance of saving someone’s life.
A consequence of those conversations, he said, is that many family members are making the difficult choice to sign do-not-resuscitate orders.
Code blue
Health-care providers are bound by oath — and in some states, by law — to do everything they can within the bounds of modern technology to save a patient’s life, absent an order, such as a DNR, to do otherwise. But as cases mount amid a national shortage of personal protective equipment, or PPE, hospitals are beginning to implement emergency measures that will either minimize, modify or completely stop the use of certain procedures on patients with covid-19.
Some of the most anxiety-provoking minutes in a health-care worker’s day involve participating in procedures that send virus-laced droplets from a patient’s airways all over the room.
These include endoscopies, bronchoscopies and other procedures in which tubes or cameras are sent down the throat and are routine in ICUs to look for bleeds or examine the inside of the lungs.
Changing or eliminating those protocols is likely to decrease some patients’ chances for survival. But hospital administrators and doctors say the measures are necessary to save the most lives.
The most extreme of these situations is when a patient, in hospital lingo, “codes.”
When a code blue alarm is activated, it signals that a patient has gone into cardiopulmonary arrest and typically all available personnel — usually somewhere around eight but sometimes as many as 30 people — rush into the room to begin live-saving procedures without which the person would almost certainly perish.
“It’s extremely dangerous in terms of infection risk because it involves multiple bodily fluids,” explained one ICU physician in the Midwest, who did not want her name used because she was not authorized to speak by her hospital.
Fred Wyese, an ICU nurse in Muskegon, Mich., describes it like a storm:
A team of nurses and doctors, trading off every two minutes, begin the chest compressions that are part of cardiopulmonary resuscitation or CPR. Someone punctures the neck and arms to access blood vessels to put in new intravenous lines. Someone else grabs a “crash cart” stocked with a variety of lifesaving medications and equipment ranging from epinephrine injectors to a defibrillator to restart the heart.
As soon as possible, a breathing tube will be placed down the throat and the person will be hooked up to a mechanical ventilator. Even in the best of times, a patient who is coding presents an ethical maze; there’s often no clear cut answer for when there’s still hope and when it’s too late.
In the process, heaps of protective equipment is used — often many dozens of gloves, gowns, masks, and more.
Bruno Petinaux, chief medical officer at George Washington University Hospital, said the hospital has had a lot of discussion about how — and whether — to resuscitate covid-19 patients who are coding.
“From a safety perspective you can make the argument that the safest thing is to do nothing,” he said. “I don’t believe that is necessarily the right approach. So we have decided not to go in that direction. What we are doing is what can be done safely.”
However, he said, the decision comes down to a hospital’s resources and “every hospital has to assess and evaluate for themselves.” It’s still early in the outbreak in the Washington area, and GW still has sufficient equipment and manpower. Petinaux said he cannot rule out a change in protocol if things get worse.
GW’s procedure for responding to coronavirus patients who are coding includes using a machine called a Lucas device, which looks like a bumper, to deliver chest compressions. But the hospital has only two. If the Lucas devices are not readily accessible, doctors and nurses have been told to drape plastic sheeting — the 7-mil kind available at Home Depot or Lowe’s — over the patient’s body to minimize the spread of droplets and then proceed with chest compressions. Because the patient would presumably be on a ventilator, there is no risk of suffocation.
In Washington state which had the nation’s first covid-19 cases, UW Medicine’s chief medical officer, Tim Dellit, said the decision to send in fewer doctors and nurses to help a coding patient is about “minimizing use of PPE as we go into the surge.” He said the hospital is monitoring health-care workers’ health closely. So far, the percentage of infections among those tested is less than in the general population, which, he hopes, means their precautions are working.
‘It is a nightmare’
Bioethicist Scott Halpern at the University of Pennsylvania is the author of one widely circulated model guideline being considered by many hospitals. In an interview, he said a blanket stop to resuscitations for infected patients is too “draconian” and may end up sacrificing a young person who is otherwise in good health. However, health-care workers and limited protective equipment cannot be ignored.
“If we risk their well-being in service of one patient, we detract from the care of future patients, which is unfair,” he said.
Halpern’s document calls for two physicians, the one directly taking care of a patient and one who is not, to sign off on do-not-resuscitate orders. They must document the reason for the decision, and the family must be informed but does not have to agree.
Wyese, the Michigan ICU nurse, said his own hospital has been thinking about these issues for years but still is unprepared.
“They made us do all kinds of mandatory education and fittings and made it sound like they are prepared,” he said. “But when it hits the fan, they don’t have the supplies so the plans they had in place aren’t working.”
Over the weekend, Wyese said, a suspected covid-19 patient was rushed in and put into a negative pressure room to prevent the virus spread. In normal times, a nurse in full hazmat-type gear would sit with the patient to care for him, but there was little equipment to spare. So Wyese had to monitor him from the outside. Before he walked inside, he said, he would have to put on a face shield, N95 mask, and other equipment and slather antibacterial foam on his bald head as the hospital did not have any more head coverings. Only one powered air-purifying respirator or PAPR was available for the room and others nearby that could be used when performing an invasive procedure — but it was 150 feet away.
While he said his hospital’s policy still called for a full response to patients whose heart or breathing stopped, he worried any efforts would be challenging, if not futile.
“By the time you get all gowned up and double-gloved the patient is going to be dead,” he said. “We are going to be coding dead people. It is a nightmare.”
IN RECENT WEEKS, investment bankers have pressed health care companies on the front lines of fighting the novel coronavirus, including drug firms developing experimental treatments and medical supply firms, to consider ways that they can profit from the crisis.
The media has mostly focused on individuals who have taken advantage of the market for now-scarce medical and hygiene supplies to hoard masks and hand sanitizer and resell them at higher prices. But the largest voices in the health care industry stand to gain from billions of dollars in emergency spending on the pandemic, as do the bankers and investors who invest in health care companies.
Over the past few weeks, investment bankers have been candid on investor calls and during health care conferences about the opportunity to raise drug prices. In some cases, bankers received sharp rebukes from health care executives; in others, executives joked about using the attention on Covid-19 to dodge public pressure on the opioid crisis.
Gilead Sciences, the company producing remdesivir, the most promising drug to treat Covid-19 symptoms, is one such firm facing investor pressure.
Remdesivir is an antiviral that began development as a treatment for dengue, West Nile virus, and Zika, as well as MERS and SARS. The World Health Organization has said there is “only one drug right now that we think may have real efficacy in treating coronavirus symptoms” — namely, remdesivir.
The drug, though developed in partnership with the University of Alabama through a grant from the federal government’s National Institutes of Health, is patented by Gilead Sciences, a major pharmaceutical company based in California. The firm has faced sharp criticism in the past for its pricing practices. It previously charged $84,000 for a yearlong supply of its hepatitis C treatment, which was also developed with government research support. Remdesivir is estimated to produce a one-time revenue of $2.5 billion.
During an investor conference earlier this month, Phil Nadeau, managing director at investment bank Cowen & Co., quizzed Gilead Science executives over whether the firm had planned for a “commercial strategy for remdesivir” or could “create a business out of remdesivir.”
Johanna Mercier, executive vice president of Gilead, noted that the company is currently donating products and “manufacturing at risk and increasing our capacity” to do its best to find a solution to the pandemic. The company at the moment is focused, she said, primarily on “patient access” and “government access” for remdesivir.
“Commercial opportunity,” Mercier added, “might come if this becomes a seasonal disease or stockpiling comes into play, but that’s much later down the line.”
Steven Valiquette, a managing director at Barclays Investment Bank, last week peppered executives from Cardinal Health, a health care distributor of N95 masks, ventilators and pharmaceuticals, on whether the company would raise prices on a range of supplies.
Valiquette asked repeatedly about potential price increases on a variety of products. Could the company, he asked, “offset some of the risk of volume shortages” on the “pricing side”?
Michael Kaufmann, the chief executive of Cardinal Health, said that “so far, we’ve not seen any material price increases that I would say are related to the coronavirus yet.” Cardinal Health, Kaufman said, would weigh a variety of factors when making these decisions, and added that the company is “always going to fight aggressively to make sure that we’re getting after the lowest cost.”
“Are you able to raise the price on some of this to offset what could be some volume shortages such that it all kind of nets out to be fairly consistent as far as your overall profit matrix?” asked Valiquette.
Kaufman responded that price decisions would depend on contracts with providers, though the firm has greater flexibility over some drug sales. “As you have changes on the cost side, you’re able to make some adjustments,” he noted.
The discussion, over conference call, occurred during the Barclays Global Healthcare Conference on March 10. At one point, Valiquette joked that “one positive” about the coronavirus would be a “silver lining” that Cardinal Health may receive “less questions” about opioid-related lawsuits.
Cardinal Health is one of several firms accused of ignoring warnings and flooding pharmacies known as so-called pill mills with shipments of millions of highly addictive painkillers. Kaufmann noted that negotiations for a settlement are ongoing.
Owens & Minor, a health care logistics company that sources and manufactures surgical gowns, N95 masks, and other medical equipment, presented at the Barclays Global Healthcare Conference the following day.
Valiquette, citing the Covid-19 crisis, asked the company whether it could “increase prices on some of the products where there’s greater demand.” Valiquette then chuckled, adding that doing so “is probably not politically all that great in the sort of dynamic,” but said he was “curious to get some thoughts” on whether the firm would consider hiking prices.
The inquiry was sharply rebuked by Owens & Minor chief executive Edward Pesicka. “I think in a crisis like this, our mission is really around serving the customer. And from an integrity standpoint, we have pricing agreements,” Pesicka said. “So we are not going to go out and leverage this and try to ‘jam up’ customers and raise prices to have short-term benefit.”
AmerisourceBergen, another health care distributor that supplies similar products to Cardinal Health, which is also a defendant in the multistate opioid litigation, faced similar questions from Valiquette at the Barclays event.
Steve Collis, president and chief executive of AmerisourceBergen, noted that his company has been actively involved in efforts to push back against political demands to limit the price of pharmaceutical products.
Collis said that he was recently at a dinner with other pharmaceutical firms involved with developing “vaccines for the coronavirus” and was reminded that the U.S. firms, operating under limited drug price intervention, were among the industry leaders — a claim that has been disputed by experts who note that lack of regulation in the drug industry has led to few investments in viral treatments, which are seen as less lucrative. Leading firms developing a vaccine for Covid-19 are based in Germany, China, and Japan, countries with high levels of government influence in the pharmaceutical industry.
AmerisourceBergen, Collis continued, has been “very active with key stakeholders in D.C., and our priority is to educate policymakers about the impact of policy changes,” with a focus on “rational and responsible discussion about drug pricing.”
Later in the conversation, Valiquette asked AmerisourceBergen about the opioid litigation. The lawsuits could cost as much as $150 billion among the various pharmaceutical and drug distributor defendants. Purdue Pharma, one of the firms targeted with the opioid litigation, has already pursued bankruptcy protection in response to the lawsuit threat.
“We can’t say too much,” Collis responded. But the executive hinted that his company is using its crucial role in responding to the pandemic crisis as leverage in the settlement negotiations. “I would say that this crisis, the coronavirus crisis, actually highlights a lot of what we’ve been saying, how important it is for us to be very strong financial companies and to have strong cash flow ability to invest in our business and to continue to grow our business and our relationship with our customers,” Collis said.
The hope that the coronavirus will benefit firms involved in the opioid crisis has already materialized in some ways. New York Attorney General Letitia James announced last week that her lawsuit against opioid firms and distributors, including Cardinal Health and AmerisourceBergen, set to begin on March 20, would be delayed over coronavirus concerns.
MARKET PRESSURE has encouraged large health care firms to spend billions of dollars on stock buybacks and lobbying, rather than research and development. Barclays declined to comment, and Cowen & Co. did not respond to a request for comment.
The fallout over the coronavirus could pose potential risks for for-profit health care operators. In Spain, the government seized control of private health care providers, including privately run hospitals, to manage the demand for treatment for patients with Covid-19.
But pharmaceutical interests in the U.S. have a large degree of political power. Health and Human Services Secretary Alex Azar previously served as president of the U.S. division of drug giant Eli Lilly and on the board of the Biotechnology Innovation Organization, a drug lobby group.
During a congressional hearing last month, Azar rejected the notion that any vaccine or treatment for Covid-19 should be set at an affordable price. “We would want to ensure that we work to make it affordable, but we can’t control that price because we need the private sector to invest,” said Azar. “The priority is to get vaccines and therapeutics. Price controls won’t get us there.”
The initial $8.3 billion coronavirus spending bill passed in early March to provide financial support for research into vaccines and other drug treatments contained a provision that prevents the government from delaying the introduction of any new pharmaceutical to address the crisis over affordability concerns. The legislative text was shaped, according to reports, by industry lobbyists.
As The Intercept previously reported, Joe Grogan, a key White House domestic policy adviser now serving on Donald Trump’s Coronavirus Task Force, previously served as a lobbyist for Gilead Sciences.
“Notwithstanding the pressure they may feel from the markets, corporate CEOs have large amounts of discretion and in this case, they should be very mindful of price gouging, they’re going to be facing a lot more than reputational hits,” said Robert Weissman, president of public interest watchdog Public Citizen, in an interview with The Intercept.
“There will be a backlash that will both prevent their profiteering, but also may push to more structural limitations on their monopolies and authority moving forward,” Weissman said.
Weissman’s group supports an effort led by Rep. Andy Levin, D-Mich., who has called on the government to invoke the Defense Production Act to scale up domestic manufacturing of health care supplies.
There are other steps the government can take, Weissman added, to prevent price gouging.
“The Gilead product is patent-protected and monopoly-protected, but the government has a big claim over that product because of the investment it’s made,” said Weissman.
“The government has special authority to have generic competition for products it helped fund and prevent nonexclusive licensing for products it helped fund,” Weissman continued. “Even for products that have no connection to government funding, the government has the ability to force licensing for generic competition for its own acquisition and purchases.”
Drug companies often eschew vaccine development because of the limited profit potential for a one-time treatment. Testing kit companies and other medical supply firms have few market incentives for domestic production, especially scaling up an entire factory for short-term use. Instead, Levin and Weissman have argued, the government should take direct control of producing the necessary medical supplies and generic drug production.
Last Friday, Levin circulated a letter signed by other House Democrats that called for the government to take charge in producing ventilators, N95 respirators, and other critical supplies facing shortages.
The once inconceivable policy was endorsed on Wednesday when Trump unveiled a plan to invoke the Defense Production Act to compel private firms to produce needed supplies during the crisis. The law, notably, allows the president to set a price ceiling for critical goods used in an emergency.
At ground zero of America’s coronavirus outbreak, Seattle is overwhelmed by patients needing care. Social distancing and persistent hand washing is no longer enough. “The next step is to start thinking about alternate care systems.”
Amid the first signs that the novel coronavirus was spreading in the Seattle area, a senior officer at the University of Washington Medical Center sent an urgent note to staffers.
“We are currently exceptionally full and are experiencing some challenges with staffing,” Tom Staiger, UW Medical Center’s medical director, wrote on Feb. 29. He asked hospital staff to “expedite appropriate discharges asap,” reflecting the need for more beds.
That same day, health officials announced King County’s — and the nation’s — first death from the coronavirus. Now as cases of virus-stricken patients suffering from COVID-19 multiply, government and hospital officials are facing the real-life consequences of shortcomings they’ve documented on paper for years.
Medical supplies have run low. Administrators are searching for ways to expand hospital bed capacity. Health care workers are being asked to work extra shifts as their peers self-isolate.
And researchers this week made stark predictions for COVID-19’s impact on King and Snohomish counties, estimating 400 deaths and some 25,000 infections by April 7 without social-distancing measures.
“If you start doing that math in your head, based on every person who was infected infecting two other people, you can see every week you have a doubling in the number of new cases,” state health oficer Dr. Kathy Lofy said.
Hand-washing, staying home from work and other measures were no longer enough to sufficiently slow the virus, Lofy said.
Hospital administrators are rapidly changing protocols as the outbreak stresses the system, while frontline health care workers are beginning to feel the effects of disruptions to daily life. UW Medicine on Thursday told employees it would begin postponing elective procedures, beginning March 16.
“We’ve seen what has happened in other countries where they’ve had really rapid spread. The health care system has become overwhelmed,” Lofy said. “We want to do everything we can to prevent that from happening here.”
“We’re Always Full”
King and Snohomish counties offer some 4,900 staffed hospital beds, of which about 940 are used for critical care, according to the researchers — with the Institute for Disease Modeling, the Bill & Melinda Gates Foundation and the Fred Hutchinson Cancer Research Center — who modeled the outbreak’s potential growth. “… This capacity may quickly be filled,” they wrote.
Some of Seattle’s largest hospitals were already near capacity before the outbreak. Harborview Medical Center in downtown Seattle operated at 95 percent of its capacity in 2019, based on its licensed 413 beds and the days of patient care it reported to the Department of Health.
Of 81 hospitals that reported data for all of 2019, excluding psychiatric hospitals, the median hospital operated at 50 percent of its licensed capacity, according to a Seattle Times analysis. Many hospitals staff fewer beds than the maximum their license allows for, so the actual occupancy rate is likely higher.
Katharine Liang, a psychiatry resident physician who works rotations for Seattle-area hospitals, said requests for UW Medicine staffers to discharge patients in a timely fashion are not uncommon as administrators seek extra beds.
“The safety net hospitals, we’re always full,” Liang said, referring to medical centers that care for patients without insurance or means to pay.
Susan Gregg, a spokeswoman for UW Medicine, which operates UW Medical Center, Harborview Medical Center, Valley Medical Center and Northwest Hospital, said that each hospital had a surge-capacity plan being adapted for the outbreak.
“Our daily planning sessions monitor our available beds, supply usage and human resources,” Gregg said in a statement.
While Washington state has a robust system for detecting and monitoring infectious diseases, it has struggled to build the capacity to respond to emergencies like the coronavirus outbreak, according to a review of public data and interviews.
On a per-person basis, the state lags most others in nurses and hospital rooms designed to isolate patients with infectious, airborne diseases, according to a nationwide index of health-security measures.
The U.S. Centers for Disease Control and Prevention launched this initiative — called the National Health Security Preparedness Index — in 2013 to comprehensively evaluate the nation’s readiness for public health emergencies.
The state’s greatest strength, according to the index, is in its ability to detect public-health threats and contain them — scoring 8.5 points out of a possible 10, above the national average.
“It’s a leading state now in terms of how testing capabilities are playing out” for COVID-19, said Glen Mays, a professor at the Colorado School of Public Health who directs the index work.
With the scope of the outbreak becoming clear, the focus is turning to an area that is the state’s weakest on the index: providing access to medical care during emergencies.
When it comes to nurses per 100,000 people, Washington state ranked near the bottom — 46th among states and the District of Columbia — in 2018. It ranked 43rd nationally in the number of hospital isolation rooms — commonly referred to as “negative pressure” rooms, which draw in air to prevent an airborne disease from spreading — per 100,000 people and in neighboring states.
“It’s an area of concern,” Mays said of the state’s health care delivery capacity.
This vulnerability is well known to state policymakers. John Wiesman, Washington state’s health secretary, serves on the national advisory committee of the index and has championed its use as a tool for improvement, Mays said. He recalled Washington seeking lessons from other states that have been more successful and building a “medical reserve corps,” another area where the state has lagged.
The state scored 2.5 points for managing volunteers in an emergency in 2013. In 2018, it had improved to just 2.6.
Health Workers Strained
Less than a week after diagnosed cases of COVID-19 grew rapidly in the Seattle area, administrators at several area hospitals had to hunt for additional medical supplies and called for rationing. They also established fast-shifting isolation policies for sick or potentially exposed staffers.
“Hospitals are being very vigilant. If you have the slightest signs of illness, don’t come to work,” said Alexander Adami, a UW Medicine resident, on Monday.
On March 6, UW Medicine directed employees who tested positive for COVID-19, the illness caused by coronavirus, to remain isolated at home for a minimum of seven days after symptoms developed, according to internal UW documents. Hospital workers told workers with symptoms who hadn’t been tested to remain isolated until they were three days without symptoms. Those who tested negative, or had influenza, could return after 24 hours.
Quarantines for sick workers means others must backfill.
“Programs are having to pull residents in other blocks in other hospitals and other clinics to fill gaps,” Adami said. “There simply aren’t enough people.”
School closures further complicate staffing.
Liang, the resident physician who works rotations for several area hospitals, said she had been pulled into an expanded backup pool on short notice to cover shifts.
Liang is the mother of a 1-year-old. On Wednesday, her family’s day care closed, as it typically does when Seattle schools close. Gov. Jay Inslee has ordered all schools in King, Pierce and Snohomish counties to close until late April.
“I’m not really sure what we’re going to do going forward,” Liang said. “My demands at home are increasing, and now, at the same time because of the same problem, my demands at the hospital are increasing as well.”
Adami, a second-year internal medicine resident, said residents were used to taxing hours, and demands had not been much more excessive than usual, but he remained concerned for the future.
“I would be worried about: We eventually get to the point where there are so many health care workers who become sick we have to accept things like saying, All right: Do you have a fever? No? Take a mask and keep working, because there are people to care for,” he said.
One sign of demand: Some hospitals are asking workers at greater risk of COVID-19 to continue in their roles, even after public health officials encouraged people in these at-risk groups among the broader public to stay home.
Staff over the age of 60 “should continue to work per their regular schedules,” a UW Medicine policy statement said. People who are pregnant, immunocompromised or over 60 and with underlying health conditions were “invited to talk to their team leader or manager about any concerns,” noting that hospital workers’ personal protective equipment would minimize exposure risks.
A registered nurse at Swedish First Hill who is over 60 and who has a history of cardiac issues said she told a manager last week of her concern about working with potential or confirmed COVID-19 patients.
She said a manager adjusted her schedule for an initial shift, but couldn’t guarantee that she would be excused from caring for these patients.
Hours later, the nurse said she suffered a cardiac event and was later admitted to another hospital with a stress-induced cardiomyopathy. The nurse did not want to be named for fear of reprisal by Swedish.
“I’m afraid for my life to work in there,” the nurse said. “I don’t think we’re being adequately protected.”
The nurse is now on medical leave.
In a statement, Swedish said it could not comment on an individual caregiver’s specific circumstances, but that employees at a higher risk are able to request reassignment and if it can not be accommodated, they can take a leave of absence.
“Providing a safe environment for our caregivers and patients is always our top priority, but especially during the current COVID-19 outbreak,” according to the statement.
Anne Piazza, senior director of strategic initiatives for the the Washington State Nurses Association said she had heard from a “flood” of nurses with similar concerns.
Additionally, “we are seeing increased demand for nurse staffing and that we do have reports of nurses being required to work mandatory overtime.”
Wuhan was Overwhelmed
China might provide an example of what could happen to the U.S. hospital system if the pace of transmission escalates, according to unpublished work from researchers with Johns Hopkins University, Harvard University and other institutions.
In Wuhan, the people seeking care for COVID-19 symptoms quickly outpaced local hospitals’ ability to keep up, the researchers found. Even after the city went on lockdown in late January, the number of people needing care continued to rise.
Between Jan. 10 and the end of February, physicians served an average of 637 intensive-care unit patients and more than 3,450 patients in serious condition each day.
But by the epidemic’s peak, nearly 20,000 people were hospitalized on any given day. In response, two new hospitals were built to exclusively serve COVID-19 patients; in all, officials dedicated more than 26,000 beds at 48 hospitals for people with the virus. An additional 13,000 beds at quarantine centers were set aside for patients with mild symptoms.
The researchers analyzed what might happen if a Wuhan-like outbreak happened here.
“Our critical-care resources would be overwhelmed,” said Caitlin Rivers, an epidemiologist at Johns Hopkins Center for Health Security who helped lead the study.
“The lesson here, though, is we have an opportunity to learn from their experience and to intervene before it gets to that point.”
Preparing For The Worst
Hospital administrators are stretching to make the most of their staff, avoid burnout and find space for patients flooding into hospitals.
As of Thursday afternoon, there hadn’t been an unusual uptick in hospitals asking emergency responders to divert patients elsewhere, according to Beth Zborowski, a spokeswoman for the Washington State Hospital Association.
Zborowski said administrators are getting creative to deal with shortages of supplies, staff and space, such as potentially hiring temporary workers.
The state is trying to reduce regulations to help scale up staffing.
The state health department’s Nursing Commission said last Friday it would give “top priority” to reviewing applications for temporary practice permits for nurses to help during the COVID-19 crisis.
After the governor’s emergency proclamation, the Department of Health also said it was allowing volunteer out-of-state health practitioners who are licensed elsewhere to practice without a Washington license.
All the doctors with UW Medicine have been trained, or are being trained on how to care for patients via telemedicine. The number of people using the service has increased tenfold since public health officials urged patients to not visit emergency rooms or visit clinics for minor issues, said Dr. John Scott, director of digital health at UW Medicine.
Some hospitals are creating wards for COVID-19 patients. EvergreenHealth, in Kirkland, converted its 8th floor for the use of these patients.
King County officials last week purchased a motel, which could allow patients to recover outside a clinical setting and free up beds.
“These are places for people to recover and convalesce who are not at grave medical risk, and therefore do not need to be in a hospital,” said Alex Fryer, spokesperson for King County Executive Dow Constantine.
Supply problems are ongoing, even after the federal government fulfilled a first shipment that included tens of thousands of N95 respirator masks, surgical masks and disposable gowns from a federal stockpile.
Piazza said the nursing association continues to receive reports that members at area hospitals are being asked to reuse or share personal protective equipment, wear only one mask a shift or conserve masks for use exclusively with COVID-19 confirmed patients.
“We need to address the safety of frontline caregivers,” Piazza said.
State officials placed a second order for supplies last weekend.
Casey Katims, director of federal affairs for Inslee, said three trucks of medical supplies from the federal stockpile arrived Thursday morning, including 129,380 N-95 respirators; 308,206 surgical masks; 58,688 face shields; 47,850 surgical gowns; and 170,376 glove pairs.
If the measures taken now aren’t enough, state officials have contingency plans they’ve been working on “for a while now,” said Lofy, the state health officer.
“The next step is to start thinking about alternate care systems or alternate care facilities. These are facilities that could potentially be used outside the clinic or the health care system walls.”
An epidemiological threat such as the new coronavirus, which causes the disease COVID-19, can have disruptive effects on the economy. It can disrupt the global supply of goods, making it harder for U.S. firms to fill orders. It can also waylay workers in affected areas, reducing labor supply on one end and on the other slow the demand for U.S. products and services.
International Monetary Fund Managing Director Kristalina Georgieva says the outbreak is the world’s “most pressing uncertainty.” The economic disruptions caused by the virus and the increased uncertainty are being reflected in lower valuations and increased volatility in the financial markets. While the exact effect of the coronavirus on the U.S. economy is unknown and unknowable, it is clear that it poses tremendous risks.
Policymakers should therefore immediately undertake a number of steps to address any economic fallout from the virus. The burden of meeting this challenge falls squarely on Congress and the Trump administration. To its credit, the Federal Reserve has aggressively cut interest rates, but monetary policy will likely have a very limited effect since interest rates are already low and have been so for some time. To put the U.S. economy on steady footing, CAP recommends that Congress and the Trump administration engage in fiscal stimulus and embrace five key principles for economic policy action in response to the coronavirus:
Do no harm
Put more, not fewer, resources in public health efforts
Assure businesses that things will be fine if the virus hits their sector and remediate harm when necessary
Calm financial markets
Ease the risks for households and vulnerable populations
The risks to the economy from the spread of the virus can be contained—even if the virus cannot. Congress and the Trump administration, however, will need to act quickly and communicate their actions clearly to ensure that the U.S. economy faces a more certain future.
Assessing the economic impact of COVID-19
In order to assess the possible impact of the coronavirus on the economy, it is important not only to focus on the epidemiological profile of the virus but also on the ways that consumers, businesses, and governments may respond to it. COVID-19 will most directly shape economic losses through supply chains, demand, and financial markets, affecting business investment, household consumption, and international trade. And it will do so both in traditional, textbook supply-and-demand ways and through the introduction of potentially large levels of uncertainty.
Economists have been using the SARS epidemic to put the coronavirus outbreak in context. The 2003 SARS epidemic is estimated to have shaved 0.5 percent to 1 percent off of China’s growth that year and cost the global economy about $40 billion (or 0.1 percent of global GDP).The coronavirus epidemic, which like SARS originated in China, differs in a few key ways. China’s economy accounted for roughly 4 percent of the world’s GDP in 2003; it now commands 16.3 percent. If the coronavirus has a similar effect on China as SARS, the impact on global growth will be worse. Moreover, China’s growth is weaker than it was in 2003—after years of rapid economic development, China’s growth stands at 6 percent, the lowest it’s been since 1990. Its confidence had been shaken by the dual effects of general economic deceleration and the U.S.-China trade war escalation. Even before the epidemic, China’s Purchasing Managers’ Index was already showing signs of contraction. The February reading slowed from 50 to 35.7, a level in line with that of November 2008 during the global financial crisis. The economic fallout from the coronavirus could rattle China’s economy further and dampen global growth.
The coronavirus spreads more quickly than SARS, but, so far, seems to have a lower mortality rate. For its part, China responded more quickly to the coronavirus outbreak than it did with SARS, employing unprecedented confinement measures in areas such as Wuhan. These measures, while prudent, have created short-term economic pain on the supply-and-demand side.
Outside China, the outbreak has also affected global supply chains, as other governments have also taken immediate steps to slow the spread of the virus. The Harvard Business Reviewpredicts that the peak of the impact will occur in mid-March, “forcing thousands of companies to throttle down or temporarily shut assembly and manufacturing plants in the U.S. and Europe.” This again will disrupt global supply chains as well as demand for goods and services in the affected economies. These disruptions make it more difficult for companies in the U.S. and elsewhere to bring their goods to customers, and these companies will reduce exports from the U.S. to the rest of the world in the coming months.
Furthermore, households, companies, and governments alike are deeper in debt now than they were when SARS hit. For example, the U.S. nonfinancial corporate debt of large companies is currently around $10 trillion, up from around $4.8 trillion in 2003. Deutsche Bank released analysis showing the world’s major economies harboring the highest debt levels of the past 150 years, with World War II as an exception. They all still need to continue repaying that debt, even if jobs, customers, and tax revenues decline in a weakening economy. These fixed costs then will leave less money to spend on other things. Large amounts of debt often exacerbate an economic slowdown, especially if central banks can do little to ease that burden by cutting interest rates.
The world looks different from the last global virus outbreak in 2003. Global growth is already slow, and financial markets already have very low interest rates, which means that central banks in almost every major country have little ammunition with which to mitigate any potential economic fallout. This puts greater pressure on governments to use the power of their purse to counter the economic fallout from the coronavirus. While the fallout from the coronavirus will disrupt supply chains and global demand that could also affect the U.S. economy, the current situation also creates a lot of uncertainty over the longer term. Congress and the Trump administration can do a lot to counter the risks associated with the spread of the virus by engaging in fiscal policies (deficit spending) that will provide relief to affected populations and mitigate disruptions to U.S firms.
Supply chain disruptions make it difficult for U.S. firms to finish their products
Disruptions to global supply chains are one of the clearest effects of the coronavirus. Looking more closely at global supply chains, there have already been significant disruptions, with the list of manufacturers outside of China forced to decrease production in their plants growing longer every day.
As noted earlier, China has shut down factories in areas affected by the virus as a preventive measure, causing supply chain disruptions and affecting the mobility and near-term employment prospects of migrant workers.
These disruptions could further spread. As the virus has moved outside of China along with the efforts to contain it, it is possible that many workers around the world may not be able or willing to show up at work, further reducing economic activity. The viral outbreak in northern Italy, for instance, has shut down a firm that is the supplier of electronic parts to automakers across the European Union, meaning auto plants in several countries may need to close. This kind of widening of supply chain disruptions to suppliers of intermediate goods outside of China will make it increasingly difficult for U.S. firms to substitute products from other countries for the missing inputs from China.
How much this affects U.S. firms will depend on how tightly they manage their supply chains. Many firms manage the time between needing new supplies from China and putting them into their own production with very short lead times—often weeks and not months. These companies will feel the effect of factory shutdowns in China relatively quickly. These challenges affect not just traditional industries such as car manufacturing but also increasingly high-tech industries such as smart phones and computers. As a consequence of these supply chain disruptions, U.S. firms cannot finish their own production and thus cannot bring their products to customers. The result is reduced economic activity and growth.
Consumers are buying fewer things as they worry about the virus and its spread
The virus will not only affect supply, but some sectors of the U.S. economy may also experience declines in demand—and big reductions in revenue—because of the overall effects on the economy. There are two separate effects to consider. First, people will buy less of some goods and services because they are afraid of potential exposure to the virus. For example, they may be less willing to travel or go out to eat. The result is that air travel and hotels could feel a real pinch. Already lessened demand on food and beverage industries seems to be occurring. As Americans feel increasingly uneasy about the spread of the virus in the country, it is foreseeable that they will further cut back on some goods and increase their emergency savings instead.
Second, when firms are forced to close, workers likely will receive less money than they otherwise would have expected and, in some instances, will receive no pay. As a result, these workers will have less to spend, again cutting overall demand. A fall in demand that follows a supply shock constitutes a one-two punch that will further contract economic activity, although the size of these effects is largely unknown.
Mass flight cancellations to and from China—which has been designated as a “do not travel” destination in the United States—means almost no one is traveling to China and, more importantly for U.S. firms, Chinese tourists are not traveling overseas. A consulting firm estimates that the United States will lose 1.6 million visitors from mainland China, with an associated decrease in spending of $10.3 billion dollars. Multinational companies and luxury goods makers who rely on Chinese consumers have already suffered and had to close stores. As such effects proliferate around the world, U.S. exporters will find it harder to sell their wares around their globe, which will have negative repercussions for U.S. growth and jobs.
Meanwhile, the U.S. anticipates lower imports from China. The last quarter of 2019 saw low imports, exports, and international trade. There is a risk of a sizeable negative demand shock if the public overreacts to the coronavirus outbreak.
Uncertainty over the virus and its economic effects can damage the economy
As much as economists think about risk-taking as a key driver of the economy, an economy only works if risks are largely known. But unknown risks, or uncertainties, can have a larger, more paralyzing effect.
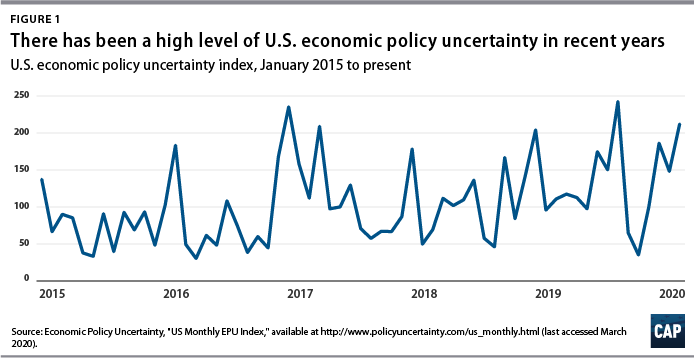
The current U.S. domestic economy—with its strong labor market and consumption levels but concerningly low inflation and investment—already exhibits a heightened sense of uncertainty. Political polarization and conflicting policies on regulation have led to firms thinking twice before investing or expanding. Both a global and U.S. economic uncertainty index, developed by economists from Northwestern, Stanford, and the University of Chicago note an all-time high in August 2019.
In addition to the already high level of policy uncertainty, the effects of the coronavirus outbreak have a commonality with the 2008 financial crisis, specifically, its unknown magnitude. There are uncertainties about the scale of the virus, contagion rate, mortality rates, risk of incidence, and more. On top of the usual online disinformation and swirl of conspiracy theories, there are questions about the accuracy of the health statistics coming from China, in part because of China’s history of providing less-than-credible numbers related to its economy. Federal Reserve Chairman Jerome Powell remarked that it’s “very hard” to understand China’s economy. That issue of credibility has only become more challenging during this crisis and it makes assessing the impact of the virus on the global economy that much more difficult.
How may a heightened sense of uncertainty affect the economy? It could affect businesses, households, and financial market participants. Businesses may hold off on investments because they don’t know what happens to supply chains as well as their domestic and international customers. Internationally, it is not known where and how far the virus will spread. This makes it hard or even impossible to assess the effects on supply chain and demand disruptions discussed above. But if these effects are difficult to evaluate, businesses will not know whether they should continue with planned or even new investments. Yet, any slowdown of business investment in the United States would come after investment spending by U.S. firms has already fallen from March to December 2019.
Businesses are not the only ones that could pull back amid uncertainty. Households, worried about contracting the virus, could cut spending on some items such as traveling and going out. Moreover, this health risk poses a real economic risk, as many households have inadequate health insurance, which could leave them with large doctors’ bills when they get sick. And, most Americans do not have paid sick leave, meaning if they get sick from the virus and need to stay home, they will not get paid. In light of the risks, many people will view it as good economic precaution to avoid activities that increase exposure to others. On an economywide scale, though, this means less spending and thus less growth.
Banks and other financial institutions may restrict and reprice credit because they cannot properly assess short-term risks to particular borrowers, sectors, or countries. Less credit availability could make it harder for businesses, especially smaller ones, to invest and grow. And, some potential home buyers could find it harder to get a mortgage. Credit market uncertainty could then exacerbate the demand fallout from the coronavirus.
There is also an international wrinkle to growing uncertainty. International financial investors could become worried about the unknown risks to the global economy from the coronavirus. They could look for the comfort of a safe investment. Traditionally, U.S. treasuries are seen as very safe investment. However, more money coming into the United States from abroad typically strengthens the U.S. dollar, and a stronger U.S. dollar will eventually make U.S. exports costlier, making it more difficult for U.S. firms to compete globally.
Supply chain disruptions, demand contractions, and global economic uncertainty happen against the backdrop of many firms and households straining under large amounts of debt. This debt has to be repaid even if the economy slows. This continued debt service then leaves less money for businesses and households to spend when their incomes drop. High debt levels will exacerbate the economic fallout from the virus.
Interest rates and stock price decline as economic uncertainty takes hold
U.S. interest rates have recently fallen to historic lows in a sign of increasing economic uncertainty. The 10-year Treasury yield fell from 1.69 percent to 1.50 percent in the last week of January after remaining steadily around 1.7 percent to 1.8 percent throughout 2019 and early 2020. The decline continued through February, and for the first time in 150 years, the yield rate dipped below 1 percent on March 3.
The abnormal decline has increased calls for action from Wall Street, demanding that the White House and Congress to do something. The 10-year yield rate—often looked to as a fear index of the economy—clearly reflects the uncertainty and instability caused by the coronavirus and lack of appropriate response.
Prices on bonds with a range of maturities reflect an increasing possibility of a recession. In technical parlance, the yield curve has become inverted. Shorter-term interest rates are now higher than longer-term interest rates—the opposite of what happens in normal economic times. Such inversions are typically taken as a sign that financial markets worry about the longer-term outlook for the economy. Financial markets now see a growing risk of a recession. In the same vein, lower long-term interest rates mean that financial markets expect the Fed to cut interest rates, which are already low, to reduce the risk of a recession.
Financial markets, however, clearly worry that Federal Reserve action on interest rates may not be enough. The federal funds rate—the main interest rate that the Federal Reserve seeks to influence—has already been low. Moreover, longer-term interest rates—such as mortgage rates that matter for economic activity, including people buying houses—have fallen even without the Fed cutting rates. In addition, households hold a lot of consumer debt—student debt, car loans, and credit cards—where interest rates do not appear to react much to what the Fed is doing. That said, the effect of Federal Reserve bank interest rate cuts will be limited.
All these factors worry the stock market as the future outlook for the economy—and thus the outlook for profits—becomes murkier. The Dow Jones Industrial Average, S&P 500, and the Nasdaq composite all fell into correction territory at the end of February, representing their worst weekly skids since 2008. Stock market conditions are expected to remain volatile as measured by the Volatility Index (VIX).
Data from the Federal Reserve Bank of St. Louis shows volatility spiking abnormally in mid-February, as global panic surrounding the outbreak starts to set in. The index jumped from around 15 to almost 40 within a month. Such volatility has led corporate borrowers, who were looking to take advantage of favorable credit conditions to refinance loans, to withdraw their loans from the market and wait for stabilization. According to the Harvard Business Review, volatility “has signaled the greatest strain” on the valuation of risk assets, setting up volatility levels on par with the most major economic disruptions of the last three decades—barring the 2008 financial crisis.
5 core economic principles to inform policy in response to the coronavirus
The coronavirus puts the spotlight on policymakers to counter the risks of the virus in a quick, constructive, and effective way. It is imperative for policymakers to keep cool heads and take steps to ensure that the disruptions to workers, individual businesses, and sectors—which will cascade through the economy because of interconnectedness—are minimized while not interfering with efforts to deal with the epidemic. To that end CAP recommends five principles for economic policy action.
Do no harm
The Trump administration must find one voice and stop adding to the confusion. Moreover, the administration must to stop attacking the very programs Americans need right now: paid leave, public health insurance, SNAP, and other social programs. In its early 2020 budget proposal, the Trump administration sought to cut Centers for Disease Control and Prevention (CDC) funding by 16 percent; cut $85 million from the Emerging and Zoonotic Infectious Diseases program; and had the U.S. Department of Health and Human Services (HHS) cut $25 million from the Office of Public Health Preparedness and Response along with another $18 million from the department’s Hospital Preparedness Program. The latest budget proposal, modified to address the coronavirus outbreak, asks for $1.25 billion in new emergency funds for preparation and response efforts and to divert another $1.25 billion from other federal programs. It is imperative to change the message from cutting funding for public health, planning, and preparedness and instead articulate clear and decisive support of public efforts to contain the outbreak, minimize harms, and ensure investments in public health and emergency preparedness.
Put more, not fewer, resources in public health efforts
Potentially massive externalities related to epidemics alter conventional economic thinking. For example, many medical services that providers would normally charge for should be highly subsidized and delivered free (or close to free) and at a minimum of inconvenience to users. The Trump administration should consider immediate efforts to subsidize detection, treatment, and eventually immunization. Reimbursements could be a way of accomplishing this. Specifically, in terms of lowering barriers to testing, the government should make it clear that testing will be free (or at least not too expensive) and that people should not fear hospitalization (as undocumented people sometimes do).
The federal government needs to identify crucial medical supplies to deal with the outbreak and make sure that production will meet demand. Production and stockpiling of facemasks and protective gear for medical workers, and saline bags to treat patients, must be organized with government financial support. In addition, since many of the active ingredients in generic pharmaceuticals are made throughout the world—in places such as India, China, and the Czech Republic—the federal government needs to coordinate with domestic drug manufacturers to make sure the supply of many lifesaving drugs is not disrupted.
Policymakers should consider providing relief to hospitals and health care providers. It is unrealistic to think that health care providers won’t face financial strain in the event of a major outbreak or pandemic. Moreover, pandemics affect everyone, and many of the patients in need of acute care may be uninsured. Failure to treat these patients would produce large, negative health and economic externalities. Thus, pandemic preparedness cannot be approached by relying on standard health care business models. The spending necessary to expand capacity during such a public health crisis should come from the federal government, principally through the U.S. Department of Homeland Security, and, ideally, informed by a robust interagency working group with HHS, CDC, and other relevant executive agencies.
Assure businesses that they will be fine if their sector is hit by the virus and remediate harm when necessary.
Beyond the health sector, other industries necessary for the well-being of U.S. citizens may also need direct federal support. For example, a common response to natural disasters is panic buying in food stores, reflecting fear that supplies may not last. If the effects of the outbreak on food processors and retailers are severe, that sort of heightened anxiety will reappear—and perhaps for good reason. The government needs to consult with major food retailers and their suppliers to plan for possible disruptions in deliveries all along the food supply network and provide direct financial support to ensure that food supply does not become a serious problem.
Congress and the administration should consider measures that would provide immediate and direct relief where it is needed most. For example, in areas where the local, state, or federal government has mandated quarantines, the federal government could provide low-interest loans to small businesses for their associated costs and loss of profits. This will ensure that small businesses stay in business and that they do not have to let employees go or cut their pay. If the Trump administration can do three rounds of farm bailouts due to the trade wars, the government can certainly offer some better-designed insurance program to sectors and firms affected by the fallout from the virus.
Targeted relief to sectors heavily affected in a direct way serves both to ensure minimum service levels, minimize supply chain disruptions, and avoid credit events that could spread across the economy.
Calm financial markets
The spread of COVID-19 has begun to affect financial markets, but it is uncertain how severely the coronavirus will strain the broader financial system moving forward. As financial markets become more volatile, and more economically vulnerable actors suffer increased difficulties to meet financial contracts, it will be important to act swiftly in order to avoid any disruptions in the chain of payments and too much risk-averse behavior.
The Federal Reserve cut its benchmark interest rate by half (.5) a percentage point on March 3 in a move that was widely seen as a reaction to the coronavirus. Other central banks have already lowered interest rates or are considering doing so. The Federal Reserve should adopt an accommodative monetary policy stance and should consider using all tools at its disposal, including its emergency lending authorities. But as interest rates are close to zero in many large markets, there is limited scope for further decreases, so more creative instruments such as quantitative easing may be warranted. Inflating financial asset prices (such as the stock market) should not be a main goal in this context.
The federal government and regulators should monitor financial markets closely and prepare for possible market stress; credit events; or sudden drops in credit supply or in liquidity in markets such as overnight repurchase agreements (repos) and intervene where it is sensible to do so.
Moreover, financial regulators should carefully monitor the ongoing impact of COVID-19 on broader financial stability. If, for example, community banks in hard hit areas are unable to meet commercially viable business loans because they are capital constrained, a program to temporarily purchase preferred stock in these banks would allow them to meet local needs and keep good businesses operating.
The Financial Stability Oversight Council (FSOC)—a postcrisis body of financial regulators—should immediately convene a meeting to discuss the risks COVID-19 may pose to the financial system. The FSOC should task its research arm—the Office of Financial Research (OFR)—to assist with this monitoring and analysis. If the COVID-19 outbreak leads to severe stress at financial institutions and markets, financial regulators should stand ready to use the emergency authorities under their respective jurisdictions. It is important to note that the officials currently leading the financial regulatory agencies were not in office during the 2007-2008 financial crisis and may not be intimately familiar with the mechanics and protocols associated with their respective emergency authorities. To that end, the FSOC could organize a wargaming exercise to ensure financial regulators are not caught off guard if the health of the financial system does deteriorate.
It is important to emphasize that financial regulators should refrain from relaxing critical regulatory and supervisory safeguards during this period. Weakening financial stability rules for large banking institutions would undermine the core resiliency of the financial system and increase risk to the real economy.
Finally, as the coronavirus advances, it will be optimal to aim for international cooperation on economic policy matters, including financial policy. Coordinated responses will lower the likelihood of beggar-thy-neighbor policies and accusations of currency manipulation. International cooperation and coordination should also help address supply chain issues, especially in crucial supplies such as medicines.
Ease the risks for households and vulnerable populations
It will be important to reduce the impact that this outbreak with have on the financial stability and prosperity of households, particularly those who are already vulnerable. Many workers do not have health insurance, and roughly 27 percent of private-sector workers did not have access to paid sick days in 2019. Given that this is unlikely to be the last health crisis Americans will experience, the United States should adopt a guaranteed paid sick leave policy as soon as possible, just as virtually every other developed country has done. In the event of a major health crisis that involves extended sick leave, the federal government could support employers with the cost of providing paid sick time or help workers by expanding benefits through the unemployment insurance system. This would ensure that employees can recover from COVID-19 or care for a sick family member without losing their job or pay while also benefitting the businesses where they are employed.
Being uninsured or underinsured, combined with limited or no paid sick time, makes people particularly financially vulnerable. For instance, lower-wage frontline workers who work in jobs where they interact with other people—such as health aides, personal care workers, cooks and servers, and retail sales people—were less likely to have health insurance and more likely to incur medical debt due to an unexpected health event than other workers in 2018. Almost one-fourth of these workers, 23.4 percent, did not have health insurance then, compared to 10.5 percent of other workers and 4.7 percent of health care workers, such as doctors, nurses, and technicians. (see Table 1) Even though the share of lower-wage frontline workers that had unexpected health expenses in 2018 was less than that of other groups of workers (see Table 1), more than half of those frontline workers with unexpected health expenses ended up with medical debt compared to only 23.1 percent for other health care workers and 38.7 percent of all other workers. (see Table 2) Health care emergencies can quickly translate into financial burdens when people lack health insurance and the ability to take time off. The 14 states that have yet to adopt the Affordable Care Act’s Medicaid expansion should do so immediately, which would result in more than 2 million low-income people gaining comprehensive health care coverage.
Congress and the administration should also mitigate the economic harm to households. This will also have the important effect of supporting consumption—the most important pillar of the economy.
Congress could take several steps to help vulnerable households. These would include ensuring free—or affordable to the patient—access to testing and treatment for the coronavirus and protecting patients from surprise bills. Other ideas for temporary assistance could include getting cash into the hands of average people. This could be done through a payroll tax holiday or through direct cash payments. Providing financial assistance to vulnerable individuals in times of hardship ensures that they can afford the basic everyday necessities; retain a measure of control over their own lives; and avoid the dire consequences of financial disaster. Putting cash in the pockets of households increases consumption and can motivate businesses to invest more. Increased consumption and business investment have a direct positive effect on economic activity and can ignite a virtuous circle of economic growth. Consumption and investment are the cornerstone of a full economic recovery.
Conclusion
With the spread of the coronavirus, the United States is facing a potential “black swan event”—an extremely rare and unpredictable incident that has potentially severe consequences. Therefore, it is important to act swiftly and in meaningful ways to minimize the fallout from this shock. Now is precisely the time for deficit spending: Low interest rates make it cheap and easy for the government to finance itself while limiting the potency of further monetary stimuli from the Federal Reserve. Therefore, it is incumbent upon the federal government to provide fiscal stimulus to ignite economic activity. In other words, the government needs to engage in sizeable spending and investment in key areas of the economy in order to increase economic activity; minimize disruption to the health and prosperity of the population; and to limit the effects on supply chains and the business sector. The five principles for economic policy action outlined in this report provide a roadmap for meaningful and decisive fiscal action that will help the economy regain its footing.
It is important to note a policy prescription that is clearly not included in the list of recommended actions outlined above: a broad-based tax cut that favors corporations and the wealthy. There is evidence that the Tax Cuts and Jobs Act (TCJA) constituted a large corporate-tax windfall that went mostly to already wealthy individuals with little evidence that it well to middle- and working-class families. It did not spur large levels of investment or growth and ballooned the fiscal deficit. The tax cuts recently proposed by the Trump administration will be very costly and will not directly or efficiently address the economic fallouts from a potential widespread coronavirus outbreak in the United States. Such proposals, including further cuts to the corporate income tax, would provide a windfall to many large and profitable corporations and other businesses—regardless of whether or not they have been meaningfully impacted. Most of these firms are already benefitting from enormous tax cuts enacted in the 2017 tax law. Redoubling this mistake will distract from other efforts and waste resources that are urgently needed for the purposes outlined in this report.
A potential sudden stop in activity, coupled with heightened uncertainty, may expose structural vulnerabilities in certain households and markets. A decisive and rational response along the lines of the five principles outlined here will minimize economic risks and contribute to a speedy recovery.
As the new coronavirus, called 2019-nCoV, spreads rapidly around the globe, the international community is scrambling to keep up. Scientists rush to develop a vaccine, policymakers debate the most effective containment methods, and health care systems strain to accommodate the growing number of sick and dying. Though it may sound like a scene from the 2011 movie “Contagion,” it is actually an unfolding reality.
In the midst of all of this, a potential crisis simmers in the shadows: The global dependence on China for the production of pharmaceuticals and medical equipment.
Today, about 80% of pharmaceuticals sold in the U.S. are produced in China. This number, while concerning, hides an even greater problem: China is the largest and sometimes only global supplier for the active ingredient of some vital medications. The active ingredients for medicines that treat breast cancer and lung cancer and the antibiotic Vancomycin, which is a last resort antibiotic for some types of antimicrobial resistant infections, are made almost exclusively in China. Additionally, China controls such a large market portion of heparin, a blood thinner used in open-heart surgery, kidney dialysis and blood transfusions that the U.S. government was left with no choice but to continue buying from China even after a contamination scandal in 2007.
China is not only the dominant global supplier of pharmaceuticals, but it is also the largest supplier of medical devices in the U.S. These include things like MRI equipment, surgical gowns, and equipment that measures oxygen levels in the blood. Supplies of these essential products have not yet been severely disrupted by the coronavirus, but if China is no longer will or able to supply them to the U.S., thousands of Americans could die.
More concerning still are the limited options available to the U.S. and the rest of the globe to make up the shortfall. It could take years to develop the necessary infrastructure to reestablish U.S. manufacturing capacities and obtain Food and Drug Administration licensure to overcome the loss of the Chinese supply.
When a disease reaches epidemic levels, the first obligation for leaders in any country is to protect their own people. As this current crisis progresses, there may come a point when political leaders in China will face decisions on whether to prohibit the export of pharmaceuticals, medical devices and other vital medical components in order to treat or protect their own people. Such acts would be the logical outcome of an escalating situation. For the 2009 H1N1 pandemic response, for example, the U.S. was pushed to the back of the queue for vaccine deliveries even though we had existing contracts with a major vaccine manufacturer located in another country. Those vaccine deliveries were delayed.
Disruption of global pharmaceuticals?
While a total loss of active ingredient imports from China might seem far-fetched, we believe the increasing scale of the outbreak moves it closer to the realm of possibility.
About six weeks into international recognition of the epidemic in China, there are already shortages of vital personal protective equipment in both China and the U.S. UPS has transported more than 2 million masks and 11,000 gowns to Wuhan to help alleviate the shortage. But what happens when everyone runs out of protective equipment?
Wuhan is a significant player in the biotechnology and pharmaceutical industry, with multiple pharmaceutical companies located in the city. How many of these factories have closed as a result of the pandemic, and when will those that have closed open back up? Global supply chains could reach a crisis point if they are compromised because Hubei province, where Wuhan is located, is in quarantine and factories are shut down.
Additionally, Wuhan is the location of China’s first Biosafety Level (BSL) 4 laboratory, which was opened in 2017 to research SARS and other emerging diseases. It is the only lab in China that can safely handle the world’s most dangerous pathogens that pose a significant risk of transmission. Infection, death and quarantine in Wuhan and the surrounding Hubei province is restricting the ability of all types of commerce in the region. Meanwhile, the virus is already creating a significant supply chain imbalance within China. That means those medical supply companies will be under pressure to keep any products produced within the country for protection of their own health care workers, laboratory personnel and the general public.
The regulatory apparatus to insure that the Chinese manufactured pharmaceuticals being exported meet the highest standards of safety and quality control are weak or nonexistent, according to a congressional report last year. The pressure placed on supply chains by the outbreak could further exacerbate existing quality control challenges. In doing so, the virus has highlighted our reliance on China as a U.S. national security issue due to outsourcing our manufacturing capabilities and inability to ensure quality control.
As with all pandemics, the complexity of this outbreak demands international collaboration and transparency. At the same time, U.S. public health officials must acknowledge the country’s vulnerability due to our dependence on Chinese production of pharmaceuticals and medical equipment. The U.S. must develop a response plan for the inevitable shortages in the near-term and take necessary actions to reclaim control of our medical supply chain. Continuing to overlook this long-known vulnerability will only lead to catastrophe.
The U.S. trade war with China threatens to hit hospitals and health systems as well as consumers in the form of higher prices and product shortages, the president of medical supply distributor DealMed told Yahoo Finance.
On Sept. 1, President Donald Trump imposed a 10 percent tariff on $300 billion in Chinese imports, tacking more medical supplies on the list. And the administration is threatening to hike the current 25 percent tariff on $250 billion in Chinese imports to a 30 percent tariff on Oct. 1.
The products affected by the tariffs are used daily in physician offices, hospitals, pharmacies and by consumers at home, according to DealMed President Michael Einhorn.
“Think of products like gauze that are in Band-Aids. Think of other products like medical gloves,” Mr. Einhorn told Yahoo Finance. “Those products will be somewhat affected, somewhere between 10 percent and 25 percent.
“When you throw tariffs into the mix, we’re talking about potential shortages, we’re talking about potential price increases — not only to hospitals and big healthcare systems, but also to the consumer at home,” Mr. Einhorn said.


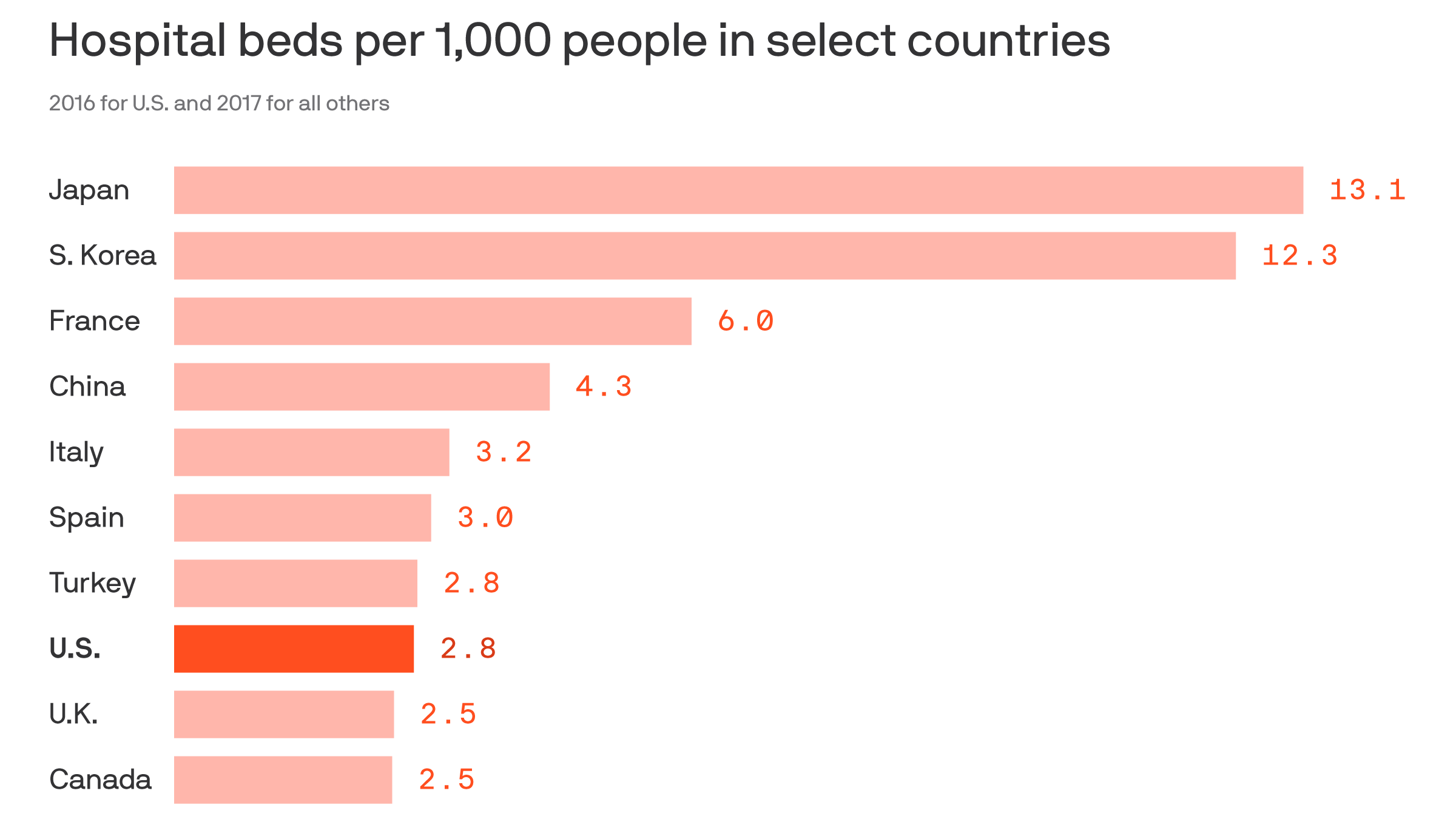

/posttv-thumbnails-prod.s3.amazonaws.com/03-24-2020/t_8a8c5e491d224704beec957580f758f3_name_032420_AmericanDoctors_Thumb_v02.png)