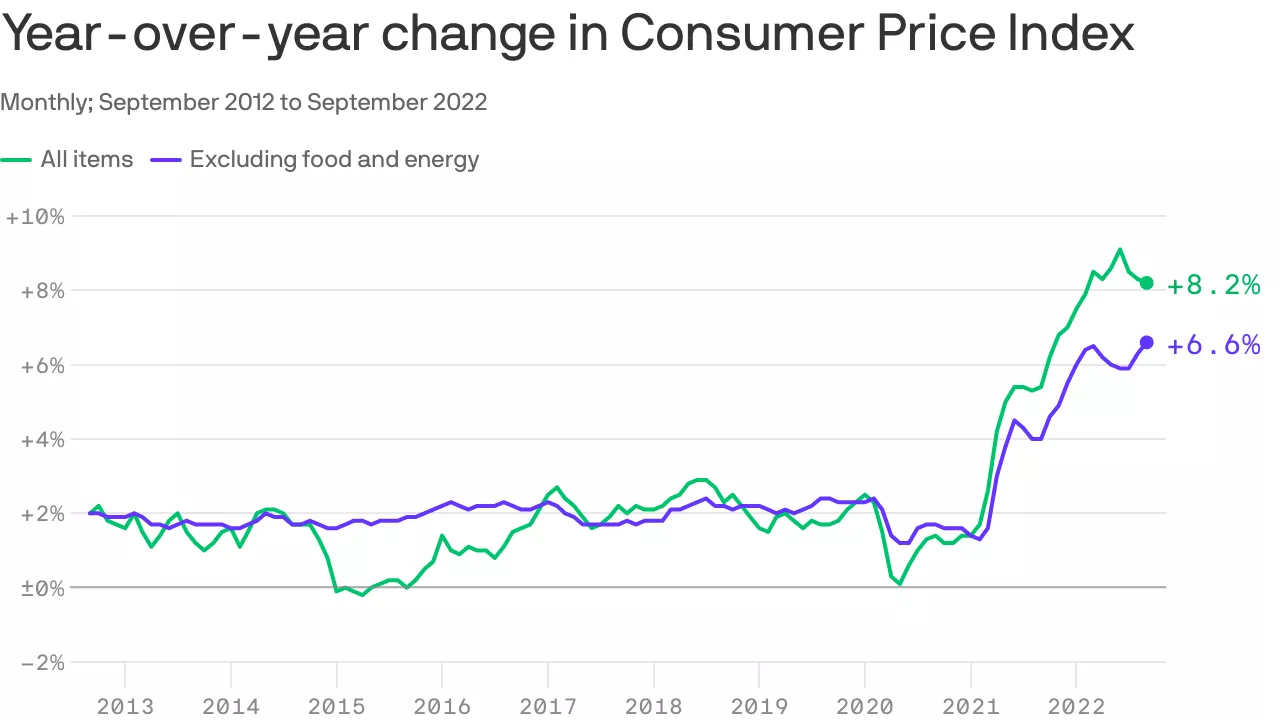
Following a cooler-than-expected inflation reading in October, consumer price gains slowed even further last month: the Consumer Price Index rose 7.1% in the year ending in November, down from 7.7% the prior month, the Labor Department said on Tuesday.
Why it matters: Inflation is still way too high, but the data offers some hope that it can ease alongside a still-healthy economy.
By the numbers: On a monthly basis, CPI rose 0.1%, slower than the 0.4% in October.
Core CPI, which strips out volatile food and energy costs, also continued to ease. On a monthly basis, it rose 0.2% — up 6% over the 12 months ending in November.
In October, those figures were 0.3% and 6.3%, respectively.
Where it stands: The Federal Reserve has raced to try to get inflation under control, raising interest rates at a historic clip — moves that risk throwing the economy into a recession.
Officials will likely raise rates by a smaller (but still historically huge) amount following a two-day policy meeting that concludes on Wednesday.
That will come after surprisingly cooler inflation readings, though officials have warned that its war on inflation is far from over.
Charlotte, NC-based Atrium Health and Downers Grove, IL- and Milwaukee, WI-based Advocate Aurora Health have formally combined to become the nation’s fifth-largest nonprofit health system. Taking the name Advocate Health, the $27B system will control 67 hospitals across six states in the Midwest and Southeast. The merger, announced in May of this year, unites the systems on even footing, with equal representation on a new board of directors, and a co-CEO arrangement for the first 18 months. The Atrium, Advocate, and Aurora brands will continue to be used in their respective local markets.
The Gist: Structuring Advocate Health as a joint operating agreement, and creating a new superstructure atop the two legacy systems, should allow the combined entity more flexibility in local decision-making, while still potentially generating cost savings from back-office efficiencies.
While we expect these kinds of mega-mergers between large regional systems to continue, it remains to be seen whether the newly combined systems can successfully create value by building larger “platforms” of care to win consumer loyalty, deploying digital capabilities, attracting talent, and becoming more desirable partners for nontraditional players.
Even before the pandemic, healthcare workers accounted for nearly three quarters of non-fatal injuries from violence in the workplace. Given the level of emotion and stress experienced in hospitals, that’s not surprising. But during the pandemic, once-sporadic violent outbursts became routine, leaving many healthcare workers fearful for their safety.
According to several health systems we’ve recently spoken with, violent events haven’t waned as the number of COVID admissions has fallen. One hospital CEO recently told us, “I never would’ve imagined that security would consume so much of my time. We keep looking for a great solution, but despite a ton of effort and a lot of money, it’s barely made a dent.” The cost of additional security—more personnel, metal detectors, restricted access—can run into millions annually for the average hospital.
Another CEO shared, “We want the hospital to be a healing environment, not feel like a prison, so we were looking for less-threatening alternatives. But those were even more expensive. Placing a canine team in the ED would run over $1M per year!” And violent episodes are not limited to hospitals, with systems reporting an increase in incidents at outpatient and clinic sites where it’s not feasible to place onsite security, given the number of smaller-scale locations.
Human resource leaders report that experiencing workplace violence, either personally or through a colleague, has been a tipping point for those considering leaving the field. According to one CHRO, workers experiencing repeat violence has been increasingly common: “We recognized the importance of having someone very senior—CEO, COO, or CMO—personally reach out to staff who have been assaulted in the workplace. But there are people who we’ve now had to call two or even three times. It’s hard to even know what to say in those situations.”
In addition to visible security and constant staff communication, providers must lobby state and federal lawmakers for legislation that requires tracking and reporting of healthcare workplace violence, and increases penalties. The Workplace Violence Prevention for Health Care and Social Service Workers Act was passed by the US House of Representatives in 2021, and was recently introduced into the Senate, so it’s time to contact your representatives and urge them to move this bill forward.
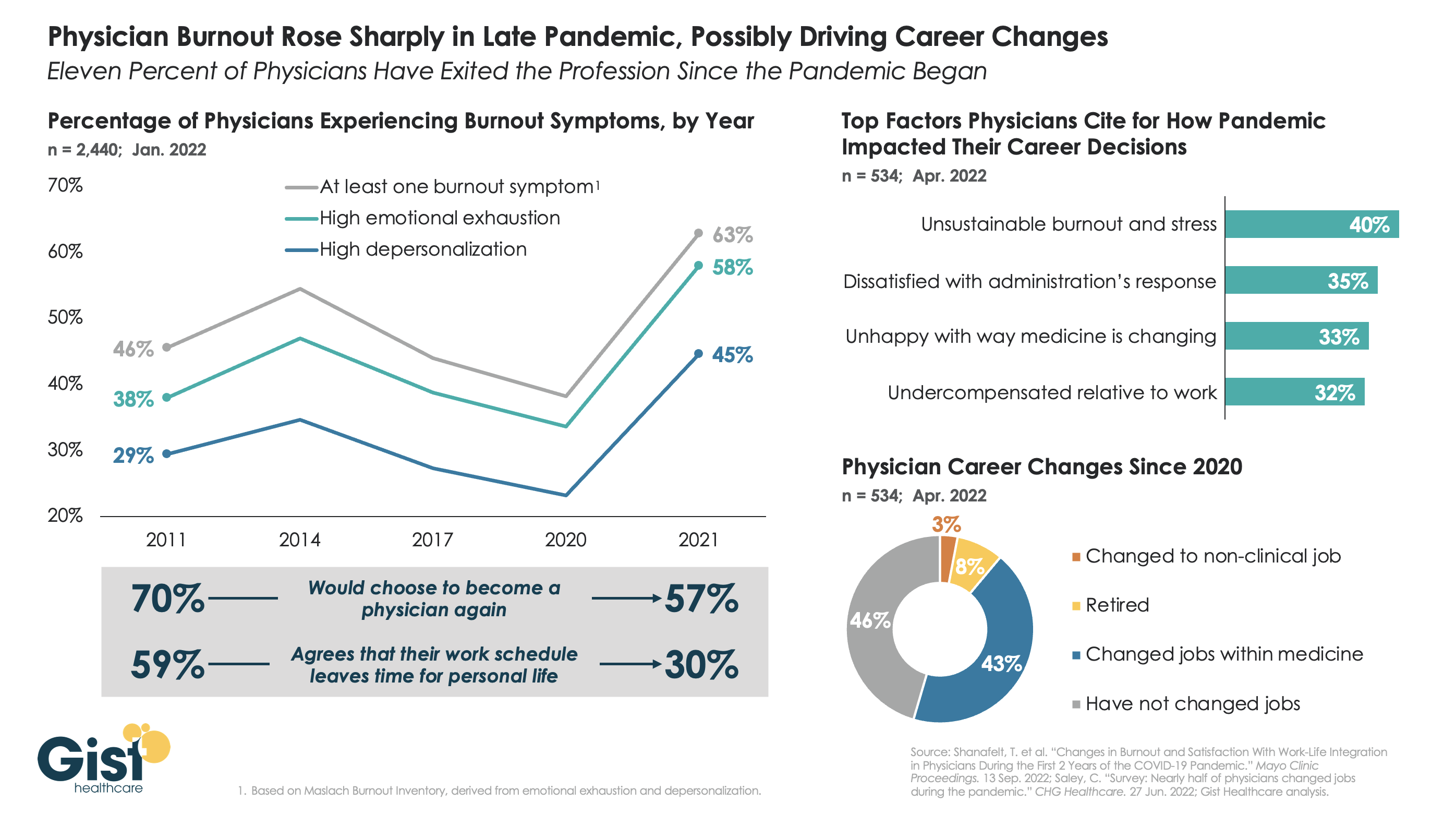
The long hours, stressful conditions, and labor shortages brought on by the pandemic have done serious harm to the physician workforce. The graphic above tracks physician burnout, a combination of emotional exhaustion, loss of agency, and depersonalization that has become the primary measure of the pandemic’s toll on workers, to reveal that physicians are demoralized like never before.
Physician burnout levels had been decreasing since 2014, in part due to practice consolidation and the expansion of team-based care models. Burnout reached its lowest levels in 2020—perhaps explained by a pandemic-induced sense of purpose—but 2021 then saw a dramatic spike in every measure of physician dissatisfaction, as the heroic glow of the early pandemic faded, and an overtaxed and understaffed delivery system became the new norm.
In explaining how the pandemic has impacted their career decisions, surveyed physicians list unsustainable burnout and stress as their top concern, and 11 percent say they have exited the profession, either for retirement or a non-clinical job, in the past two years.Four in ten surveyed physicians report changing jobs since 2020, mainly within similar or different practice settings, citing a desire for better work-life balance as their primary motivation. (It should be caveated that these data are from a smaller survey of 534 physicians, 40 percent of whom identified as “early career”.)
While the solutions here aren’t new, they are challenging: we must continue to implement team-based care models that provide physicians top-of-license practice and improved work-life balance, remove administrative tasks wherever possible, and ensure that we are communicating and engaging physicians—employed and independent alike—in organizational strategy and decision-making.
An enlightening piece published this week in Stat News lays out exactly how UnitedHealth Group (UHG) is using its vast network of physicians to generate new streams of profit, a playbook being followed by most other major payers. Already familiar to close observers of the post-Affordable Care Act healthcare landscape, the article highlights how UHG can use “intercompany eliminations”—payments from its UnitedHealthcare payer arm to its Optum provider and pharmacy arms—to achieve profits above the 15 to 20 percent cap placed on health insurance companies.
So far in 2022, 38 percent of UHG’s insurance revenue has flowed into its provider groups, up from 23 percent in 2017. And UHG expects next year’s intercompany eliminations to grow by 20 percent to a total of $130B, which would make up over half of its total projected revenue.
The Gist:
The profit motive behind payer-provider vertical integration is as clear as it is concerning for the state of competition in healthcare.
UHG now employs or affiliates with 70K physicians—10K more than last year—seven percent of the US physician workforce, and the largest of any entity.
Given the weak antitrust framework for regulating vertical integration, the federal government has proven unable to stop the acquisition of providers by payers. Eventually, profit growth for these vertically integrated payers will have to come from tightening provider networks, and not just acquiring more assets. That could prompt regulatory action or consumer backlash, if the government or enrollees determine that access to care is being unfairly restricted.
Until then, the march of consolidation is likely to continue.
On Tuesday, the Centers for Medicare and Medicaid Services (CMS) announced a proposed rule that aims to streamline the prior authorization process by requiring certain payers to establish a method for electronic transmission, shorten response time for physician requests, and provide a reason for denials. This rule replaces one proposed in December 2020 that was never finalized.
In addition to applying to Medicaid and Affordable Care Act exchange plans, the new rule would also apply to Medicare Advantage plans, which the previous rule did not. If finalized, it will take effect in 2026.
The Gist: Managing prior authorization requests is one of providers’ greatest sources of frustration, with over 80 percent of physicians rating it as “very or extremely burdensome” in a recent Medical Group Management Association survey.
Not only would patients would benefit from faster turnarounds, but even major payers agree that the status quo is suboptimal, and payer advocacy organization AHIP has signaled support for transmitting prior authorization requests electronically.
The challenge for regulators will be to strike a balance that satisfies the competing interests of payers and providers—turnaround time is likely to be a sticking point—but the one good thing about a system that no one likes is that there’s plenty of room for improvement.
Open enrollment is upon us. While many are focused on which health insurance company has the best deal, health care sharing ministries (HCSMs) are quietly offering cheaper and less regulated alternatives to traditional coverage. Despite being an inadequate substitute, for some, they’re a welcome one.
What are HCSMs?
HCSMs are not health insurance; they are cost-sharing organizations. The idea is that members help each other directly cover medical costs. Members pay monthly contributions, similar to premiums, but can also make additional donations to cover specific bills from other members.
HCSMs are allowed to exclude pre-existing conditions from eligibility, exclude various health care services altogether, such as maternity care or contraception, and cap the lifetime financial assistance for which a member is eligible. They also do not guarantee claims will be reimbursed. (One review of HCSMs in Massachusetts found that only half of submitted claims were eligible for reimbursement.)
They are often, if not always, religiously affiliated. Members commit to a code of conduct, which may include abstaining from tobacco use and holding a traditional view of sex and marriage.
HCSMs and the Affordable Care Act
Because they are not insurance and because they are religiously affiliated, HCSMs are not regulated by the Affordable Care Act (ACA). They are not subject to minimal coverage guidelines and members are not subject to the individual mandate.
HCSMs are a notable exemption to the ACA. Supporters lobbied for the exemption based on a few reasons, including former President Obama’s promise that Americans could keep their coverage if they liked it. But the main motive was religious freedom. They argued that sharing health care costs was a “religious right and a privilege.” Congress agreed to the carveout to minimize religious opposition, and advocates lauded the decision as “Obamacare’s Silver Lining.”
The appeal of HCSMs
Some see HCSMs as a viable alternative to traditional health insurance and research suggests there may be a few reasons why.
Perhaps the most significant reason is freedom: freedom of religious expression and freedom from government oversight. The Bible encourages Christians to “bear one another’s burdens,” and HCSM members see their approach to health care costs as a fulfillment of that command. Additionally, many religious individuals oppose abortion and other medical services. As such, they may see HCSMs as a way to pay for their own health care needs without funding religiously prohibited services even indirectly.
HCSMs promote a sense of freedom beyond religion, including provider choice and less government interference. For example, members essentially pay out of pocket for health care, getting reimbursed later, so they can choose any provider that accepts self-paying patients. HCSMs also allow members to bypass “the system,” staying out of the carousel that is the heavily regulated health insurance industry.
A more tangible reason why some prefer HCSMs to traditional health insurance is thrift. Monthly contributions are typically less than monthly insurance premiums. This makes sense; HCSMs are set up to cover health care expenses after they’re accrued so upfront costs can be lower. Plus, the list of reimbursable services is often limited in exchange for even lower costs.
For healthy individuals, especially those who don’t use much health care, this kind of “low cost up front” arrangement can be enticing. But, if a member has an emergency or an extended hospital stay, or develops a chronic condition, they may be stuck with significant medical bills. Monthly contributions can also increase due to changes in health status, even common ones like weight gain.
While freedom and thrift are conscious reasons to prefer HCSMs, others may choose them due to inadequate health insurance literacy. Individuals less familiar with terms like coinsurance and deductibles may have difficulty choosing from a set of ACA-compliant health insurance plans. This difficulty likely extends to evaluating the relative costs and benefits of HCSMs.
Challenges differentiating between insurance and HCSMs may also increase when small businesses list HCSMs as a potential source of coverage for health care costs. Deceptive advertising by HCSMs and insurance brokers adds further confusion.
While HCSMs are an unregulated, risky alternative to traditional insurance coverage, some find the freedom and cost savings they provide attractive. Others don’t know of a better option and join an HCSM without understanding the potential consequences. Given that inadequate insurance coverage is associated with greater medical debt and delays in seeking necessary care, it’s important that consumers have clear, accurate information to facilitate coverage decisions.
Private equity has piled into healthcare in recent years, but one company’s recent moves have some questioning whether it belongs in the industry.
Los Angeles-based Prospect Medical Holdings has come under fire for shuttering hospitals and service lines across multiple states after paying itself and shareholders $457 million from a $1.1 billion loan in 2018, CBS News reported Dec. 6. The company paid the loan by selling assets to a healthcare real estate trust.
Prospect Medical then turned around and leased the same assets from the trust, resulting in $35 million in annual rent charges.
The company began cutting services earlier in 2022 at the 168-bed Upper Darby, Pa.-based Delaware County Memorial, the report said. The hospital’s emergency department closed in November.
“What they’ve done is extremely evil, in my words,” emergency nurse Angela Neopolitano, who worked at Delaware County Memorial for 41 years, told CBS News. “To gain a dollar, you maybe destroyed lives, maybe even ended lives, because they can’t get the help they need.”
Paramedics in the hospital’s system at one point found that the credit cards used to refuel their ambulances had been disabled because Prospect Medical “didn’t pay their bill,” Ms. Neopolitano told CBS News.
Delaware County officials said Prospect Medical told them labor costs, inflation and strain from the pandemic all fed into its decision to cut services, the report said.
“I had the sense they were not giving us all the information,” county official Monica Taylor told CBS News.
The Pennsylvania Office of the Attorney General has filed a petition seeking to have Prospect Medical held in contempt and fined $100,000 per day for violating a court order prohibiting the hospital’s closure pending further order by the court.
Prospect Medical has said it plans to convert Delaware County Memorial into a 100-bed behavioral health facility, the report said.
Durham, N.C.-based Duke University Health System was downgraded to an “AA-” credit rating amid concern over its planned integration of the Private Diagnostic Clinic, a for-profit medical group with over 1,800 physicians, Fitch Ratings said Dec. 8.
The rating, declining from “AA,” applies both to specific bonds the group holds and to its overall Issuer Default Rating. In addition to the integration of the PDC, Fitch also cited concern over macro issues such as labor and inflationary pressures, which have helped to drag down operating results for the health group.
“While the transition of the PDC into the Duke Health Integrated Practice will only be effective in July 2023, the uncertainty of the proposed change had already caused some disruption to PDC’s ability to recruit physicians and may have had a negative impact on volumes,” Fitch said.
But while such integration will likely lead to an “extended period of lower operating results,” Duke Health is expected to gradually return to much stronger performance given its robust fundamentals, the ratings group added. Historically, the hospital system had pre-pandemic operating EBITDA margins of over 10 percent, compared with a fiscal year 2022 figure of just 2.1 percent.
The health system, which reported $4.5 billion of total operating revenues in 2022, said its CEO, A. Eugene Washington, MD, will step down in June 2023.