Providence is investing $220 million to fill open positions and give bonuses to current employees, the Renton, Wash.-based system announced Sept. 3.
The health system is giving a $1,000 bonus to every caregiver who has been with the organization for at least 90 days. The bonuses, which will be given to workers up to and including the director level, will be paid in two installments in September and December.
Providence is also making investments to rapidly fill 17,000 job openings. The system said it is offering sign-on bonuses to front-line workers with the goal of filling positions quickly and alleviating the stress and burnout many clinicians are experiencing. Current employees are eligible for referral bonuses of between $1,000 and $7,500.
“Our caregivers are the core of who we are, and we have been committed to supporting their health and well-being throughout the pandemic,” Providence President and CEO Rod Hochman, MD, said in a news release. “Now, as we enter month 21 of our COVID-19 response, it’s even more imperative to continue to care for and bolster those who make our mission possible.”
For much of August, the U.S. South showed up fire-engine red on our map of COVID-19’s spread in the U.S., meaning case counts were shooting up. But now, Florida, Louisiana, Mississippi, Arkansas and Missouri show up in shades of green, meaning cases—while still high—are trending down.
Does that mean the Delta surge is nearing its end?
If covering the pandemic for 18 months has taught me anything, it’s that confident predictions often come back to bite you. But there is reason for cautious optimism. Past U.S. surges have played out in short, intense bursts, and some experts have predicted, based on Delta’s behavior in other countries, that U.S. infections could peak in late August or early September. Covidestim, a modeling project from researchers at Yale, Harvard and Stanford, points to another promising sign: In more than half of states, a person infected with COVID-19 would currently be expected to transmit the virus to less than one other person, in what is perhaps a sign of waning community transmission and/or better population immunity.
Still, we shouldn’t get ahead of ourselves. The U.S. is recording an average of about 150,000 new diagnoses per day, a number not seen since this past winter’s pre-vaccination spike. And in many states, like South Dakota and West Virginia, the trends are going in the wrong direction—and fast. That suggests Delta may be moving to new states, rather than fading away completely.
The situation may become even messier as the school year gets underway. Far more kids have gotten seriously ill during this wave compared to previous ones, in part because of Delta’s contagiousness and in part because children younger than 12 cannot be vaccinated, whereas older Americans are better protected from infection. In a worst-case scenario, pediatric ICUs nationwide may be heading for a repeat of what the South has seen this summer.
While the virus behaves in mysterious ways, people in the U.S. are not powerless. The Delta variant is indeed extra contagious, but the summer surge also coincided with relaxed mask guidelines and, for many people, a return to indoor activities. In South Dakota, one of the states currently seeing the largest increases in cases, the spike seems to be related to large-scale gatherings at the Sturgis Motorcycle Rally. That suggests our behavior matters just as much as the virus’. Getting vaccinated, wearing masks indoors and avoiding large crowds can all help the Delta surge come to an end.
TODAY’S CORONAVIRUS OUTLOOK
About 445.6 million doses of the COVID-19 vaccine have been shipped to various U.S. states as of this afternoon, of which some 372.1 million doses have been administered thus far, according to TIME’s vaccine tracker. About 52.7% of Americans have been completely vaccinated.
More than 219 million people around the world had been diagnosed with COVID-19 as of this afternoon, and more than 4.5 million people have died. On September 2, there were 631,605 new cases globally.
Here’s how the world as a whole is currently trending:
Here’s where daily cases have risen or fallen over the last 14 days, shown in confirmed cases per 100,000 residents:
And here’s every country that has reported over 4 million cases:
The U.S. had recorded more than 39.5 million coronavirus cases as of this afternoon. More than 643,000 people have died. On September 2, there were 153,143 new cases and 1,588 new deaths confirmed in the U.S.
Here’s how the country as a whole is currently trending:
Here’s where daily cases have risen or fallen over the last 14 days, shown in confirmed cases per 100,000 residents:
All numbers unless otherwise specified are from the Johns Hopkins University Center for Systems Science and Engineering, and are accurate as of Sept. 3 1 a.m. E.T. To see larger, interactive versions of these maps and charts, click here.
WHAT ELSE YOU SHOULD KNOW
The U.S. economy gained only 235,000 jobs in August, according to new data from the U.S. Bureau of Labor Statistics—far below this year’s average of 586,000 per month and economists’ expectations of more than 700,000 in August. The retail and dining sectors lost jobs in August, which suggests the Delta-related surge is again putting the squeeze on customer-facing businesses.
South Africa will no longer export Johnson & Johnson vaccines to Europe, under a deal struck by leaders from South Africa, France and the European Commission. The shots will instead be distributed among people on the African continent, where only about 3% of the population is fully vaccinated against COVID-19, compared to nearly 60% in the European Union. The European Commission will also return shots already shipped to Europe from South Africa to help aid the continent’s vaccination campaign, CNN reports.
The U.S. government will invest $3 billion in the vaccine supply chain, in an effort to help manufacturers churn out more shots and supplies for both the U.S. and the rest of the world. Federal officials have not publicly announced which companies will receive that money, but White House COVID-19 adviser Jeff Zients said yesterday that funding will be channeled toward firms that make materials needed for vaccine production and administration, as well as facilities that fill vaccine vials and those that make personal protective equipment.
Employers and private businesses around the world have begun to mandate COVID-19 vaccination. Now, Italian officials are mulling a population-wide vaccine requirement for anyone old enough to receive a shot, according to Reuters. Such a policy wouldn’t happen until the European Medicines Agency gives the shots full approval, but it would still likely be unpopular in a country with a significant vaccine-hesitant population. At present, about 70% of Italians 12 and older are fully vaccinated.
On the other end of the spectrum, U.K. regulators reportedly may not recommend vaccines for healthy children ages 12 to 15. While shots are recommended for children with underlying conditions that put them at risk of severe disease, U.K. authorities are still assessing whether immunization is necessary for healthy kids, given their relatively low risk of hospitalization or death. The country’s regulators are, however, analyzing whether universal pediatric vaccination may be necessary to maintain safe schools.
Dr. Anthony Fauci, the top U.S. expert on COVID-19, added to the back-and-forth on booster shots yesterday, noting that a three-shot regimen will probably become standard for COVID-19 vaccines. He said a three-dose system would likely ensure more “durable” protection against the virus than a two-shot schedule, CNN reports. Ultimately, though, that decision isn’t up to Fauci. It will be decided by regulators at the U.S. Food and Drug Administration, who are set to discuss booster shots at a meeting later this month.
Many people are seeking definitive answers about what they can and can’t do after being vaccinated against Covid-19. Is it OK to travel? Should I go to a big wedding? Does the Delta variant make spending time with my vaccinated grandmother more risky?
But there’s no one-size-fits-all answer to those questions because risk changes from one individual to the next, depending on a person’s overall health, where they live and those they spend time with.
The bottom line is that vaccines are highly protective against serious illness, and, with some precautions, will allow people to return to more normal lives, experts say.A recent study in Los Angeles County showed that while breakthrough infections can happen, the unvaccinated are 29 times as likely to end up hospitalized from Covid-19 as a vaccinated person.
Experts say anxiety about breakthrough infections remains pervasive, fueled in part by frightening headlines and unrealistic expectations about the role of vaccines.
“There’s been a lot of miscommunication about what the risks really are to vaccinated people, and how vaccinated people should be thinking about their lives,” said Dr. Ashish K. Jha, dean of the Brown University School of Public Health. “There are people who think we are back to square one, but we are in a much, much better place.”
While the Delta variant is causing a surge in infections in various hot spots around the country, including Florida and Louisiana, there will eventually be an end to the pandemic. Getting there will require ongoing precautions in the coming months, but vaccinated people will have more freedom to enjoy life than they did during the early lockdowns. Here are answers to some common questions about the road ahead.
What’s my risk of getting Covid if I’m vaccinated?
To understand why there is no simple answer to this question, think about another common risk: driving in a snowstorm. While we know that tens of thousands of people are injured or killed each year on icy roads, your individual risk depends on local conditions, the speed at which you travel, whether you’re wearing a seatbelt, the safety features on your car and whether you encounter a reckless driver on the road.
Your individual risk for Covid after vaccination also depends on local conditions, your overall health, the precautions you take and how often you are exposed to unvaccinated people who could be infected.
“People want to be told what to do — is it safe if I do this?” said Dr. Sharon Balter, director of the division of communicable disease control and prevention at the Los Angeles County Department of Public Health. “What we can say is, ‘These are the things that are more risky, and these are the things that are less risky.’”
Dr. Balter’s team has recently collected surveillance data that give us a clearer picture of the difference in risk to the vaccinated and unvaccinated as the Delta variant surged from May 1 through July 25. They studied infections in 10,895 fully vaccinated people and 30,801 unvaccinated people.The data showed that:
The rate of infection in unvaccinated people is five times the rate of infection in vaccinated people. By the end of the study period, the age-adjusted incidence of Covid-19 among unvaccinated persons was 315.1 per 100,000 people over a seven-day period compared to 63.8 per 100,000 incidence rate among fully vaccinated people. (Age adjustment is a statistical method used so the data are representative of the general population.)
The rate of hospitalization among the vaccinated was 1 per 100,000 people. The age-adjusted hospitalization rate in unvaccinated persons was 29.4 per 100,000.
Older vaccinated people were most vulnerable to serious illness after a breakthrough infection. The median age of vaccinated people who were hospitalized for Covid was 64 years. Among unvaccinated people who were hospitalized, the median age was 49.
The Delta variant appears to have increased the risk of breakthrough infections to vaccinated people. At the start of the study, before Delta was dominant, unvaccinated people became infected 10 times as often as vaccinated people did. By the end of study period, when Delta accounted for almost 90 percent of infections, unvaccinated people were five times as likely to get infected as vaccinated people.
What’s the chance of a vaccinated person spreading Covid-19?
While unvaccinated people are by far at highest risk for catching and spreading Covid-19, it’s also possible for a vaccinated person to become infected and transmit the illness to others. A recent outbreak in Provincetown, Mass., where thousands of people gathered in bars and restaurants, showed that vaccinated people can sometimes spread the virus.
Editors’ Picks
Even so, many experts believe the risk of getting infected from a vaccinated person is still relatively low. Dr. Jha noted that after an outbreak among vaccinated and unvaccinated workers at the Singapore airport, tracking studies suggested that most of the spread by vaccinated people happened when they had symptoms.
“When we’ve seen outbreaks, like those among the Yankees earlier in the year and other cases, almost always people are symptomatic when they’re spreading,” Dr. Jha said. “The asymptomatic, pre-symptomatic spread could happen, but we haven’t seen it among vaccinated people with any frequency.”
Another study from Singapore looked at vaccinated and unvaccinated people infected with the Delta variant. The researchers found that while viral loads in vaccinated and unvaccinated workers are similar at the onset of illness, the amount of virus declines more rapidly in the vaccinated after the first week, suggesting vaccinated people are infectious for a shorter period of time.
Is it still safe to gather unmasked with vaccinated people?
In many cases it will be safe, but the answer depends on a number of variables. The risk is lower with a few close family members and friends than a large group of people you don’t know. Outdoor gatherings are safer than indoor gatherings. What’s the community transmission rate? What’s the ventilation in the room? Do you have underlying health issues that would make you vulnerable to complications from Covid-19? Do any of the vaccinated people have a fever, sniffles or a cough?
“The big question is can five people sit around a table unmasked if we know they’re all vaccinated,” Dr. Jha said. “I think the answer is yes. The chances of anybody spreading the virus in that context is exceedingly low. And if someone does spread the virus, the other people are not going to get super sick from it. I certainly think most of us should not fear breakthrough infections to the point where we won’t tolerate doing things we really value in life.”
For larger gatherings or even small gatherings with a highly vulnerable person, rapid antigen testing using home testing kits can lower risk. Asking people to use a test a few days before the event, and then the day of the event, adds another layer of protection. Opening windows and doors or adding a HEPA air cleaner can also help.
How can unvaccinated children go to school safely?
Children under 12 probably will not be eligible for vaccination until the end of the year. As a result, the best way to protect them is to make sure all the adults and older kids around them are vaccinated.A recent report from the C.D.C. found that an unvaccinated elementary schoolteacher who didn’t wear a mask spread the virus to half of the students in a classroom.
Studies show that schools have not been a major cause of Covid-spreading events, particularly when a number of prevention measures are in place. A combination of precautions — masking indoors, keeping students at least three feet apart in classrooms, keeping students in separate cohorts or “pods,” encouraging hand washing and regular testing, and quarantining — have been effective. While many of those studies occurred before the Delta variant became dominant, they also happened when most teachers, staff and parents were unvaccinated, so public health experts are hopeful that the same precautions will work well this fall.
Dr. Balter noted that masking in schools, regular testing and improving ventilation will keep children safer, and that parents should be reassured by the data.
“The level of illness in children is much less than adults,” she said. “You do weigh all these things, but there are also a lot of consequences to not sending children to school.”
Can a vaccinated person visit with an elderly vaccinated person indoors without a mask?
In many cases it will be relatively safe for vaccinated people to spend time, unmasked, with an older relative. But the risk depends on local conditions and the precautions the visitor has taken in the days leading up to the visit. In areas where community vaccination rates are low and overall infection rates are high, meeting outdoors or wearing a mask may be advised.
If you’re vaccinated but have been going to restaurants, large gatherings or spending time with unvaccinated people, it’s a good idea to practice more social distancing in the days leading up to your visit with an older or vulnerable person. Home testing a few days before the visit and the day of the visit will add another layer of protection.
Gregg Gonsalves, an assistant professor of epidemiology at the Yale School of Public Health, said he recently visited his 87-year-old mother and did not wear a mask. But that is because both of them are vaccinated and he still works mostly from home, lives in a highly vaccinated area and has low risk for exposure. He is also investing in home testing kits for reassurance that he is not infectious.
“If I just came back from a big crowded gathering, and I had to go see my mom, I would put on a mask,” he said.
Is it safe to work in an office?
The answer depends on the precautions your workplace has taken. Does the company require proof of vaccination to come into the office? Are unvaccinated people tested regularly? What percentage of people in the office are unvaccinated? What steps did your company take to improve indoor air quality? (Upgrading the filters in ventilation systems and adding stand-alone HEPA air cleaners are two simple steps that can reduce viral particles in the air.)
Offices that mandate vaccination will be safer, but vaccination rates need to exceed 90 percent. Even an 85-percent vaccination rate is not enough, Dr. Jha said. “It’s not going to work because one of those 15-percent unvaccinated is going to cause an outbreak for every single person in that room,” he said. “You do not want a bunch of unvaccinated people running around your offices.”
Should I get a booster shot, and will it help protect me against Delta?
The people who have the most to gain from booster shots are older people, transplant patients, people with compromised immune systems or those with underlying conditions that put them at high risk for complications from Covid. People who received the single-dose Johnson & Johnson vaccine may also be good candidates for a second dose.
But many experts say healthy people with normal immune systems who received a two-dose mRNA vaccine from Pfizer or Moderna won’t get much benefit right now from a third shot because their vaccine antibodies still offer strong protection against severe illness. That said, the Biden administration appears to be moving ahead with offering booster shots to the general public starting as soon as the week of Sept. 20.
Economy adds just 235K jobs in August as delta hammers growth
The U.S. added 235,000 jobs in August and the unemployment rate fell to 5.2 percent as the economy appeared to falter under surging coronavirus cases, according to data released Friday by the Labor Department.
Economists had expected employment growth to slow slightly in August to a gain of roughly 750,000 jobs, according to consensus forecasts, amid falling consumer confidence and disruptive school closures.
Declines in restaurant reservations, air travel and other key drivers of the recovery also raised red flags about the August jobs haul.
“Today’s report has the delta variant written all over it. It is clear that the recent surge in COVID-19 cases is a strong headwind to the labor market,” wrote Nick Bunker, economic research director at Indeed. I break it down here.
Delta homes in on pandemic-sensitive industries: The August jobs report showed setbacks in sectors of the economy hit hardest by the pandemic and crucial to the comeback from its economic blow.
The leisure and hospitality sector did not add any net jobs in August as a 42,000-job decline in restaurants and bars wiped out a 36,000-job gain in arts and entertainment.
Employment in retail, another hard-hit sector, also fell by 29,000 thanks to steep losses at grocery stores and building material and garden supply stores.
“The industry breakdown in employment growth shows clear signs that the increased COVID-19 spread is behind this relatively weak number,” Bunker wrote. “Yet, the labor market is still recovering.”
Signs of resilience:While job growth slowed significantly in August, the first full month since the delta surge picked up in mid-July, the labor market still showed signs of holding strong.
Labor force participation stayed even at 61.7 percent in August and the employment to population ratio — a broader gauge of job market strength — ticked up 0.1 percentage points to 58.5 percent.
The number of Americans who have been jobless for 27 weeks or longer, known as the “long-term unemployed,” also dropped from 3.4 million to roughly 3.2 million. Those who suffer long-term unemployment often struggle to return to work and are hired at lower rates than those without long periods of joblessness.
Stronger days…behind? Upward revisions to June and July’s blockbuster jobs gains were another positive sign for the economy. June’s job haul was revised up from 938,000 to 962,000, and July’s was revised up from 943,000 to 1,053,000 — the first seven-digit job gain since August 2020.
“The underlying momentum is still there. We just have to see if we can keep up the pace until this surge is behind us,” Bunker said.
Contrary to what health care executives advertise, hospital mergers and acquisitions aren’t good for patients. They rarely improve access to health care or its quality, and they don’t reduce prices. But the system in place to stop them is often more bark than bite.
During 2019 and 2020, hospitals acquired an additional 3,200 medical practices and 18,600 physicians. By January 2021, almost half of all U.S. physicians were employed by a hospital or health system.
In 2018, the last year for which complete data are available, 72% of hospitals and more than 90% of hospital beds were affiliated with a health care system. Mergers and acquisitions are increasing the number of health care systems while decreasing the number of independently operated hospitals.
When hospitals buy provider practices, it leads to more unnecessary care and more expensive care, which increases overall spending. The same thing happens when hospitals merge or acquire other hospitals. These deals often increase prices and they don’t improve care quality; patients simply pay more for the same or worse care.
Mergers and acquisitions can negatively affect clinician morale as well. Some argue they lead to providers’ loss of autonomy and increase the emphasis on financial targets rather than patient care. They can also contribute to burnout and feeling unsupported.
Considerable machinery is in place at both the federal and state levels to stop “anticompetitive” mergers before they happen. But that machinery is limited by a lack of follow through.
The Federal Trade Commission (FTC) and the U.S. Department of Justice have always had broad authority over mergers. By law, one or both of these entities must review for any antitrust concerns proposed deals of a certain size before the deals are finalized. After a preliminary review, if no competition issues are identified, the merger or acquisition is allowed to proceed. This is what happens in most cases. If concerns are raised, however, the involved parties must submit additional information and undergo a second evaluation.
Some health care organizations seem willing to challenge this process. Leaders involved in a pending merger between Lifespan and Care New England in Rhode Island — which would leave 80% of the state’s inpatient market under one company’s umbrella — are preparing to move forward even if the FTC deems the deal anticompetitive. The companies will simply ask the state to approve the merger despite the FTC’s concerns.
The reality is that the FTC’s reach is limited when it comes to nonprofits, which most hospitals are. While the FTC can oppose anticompetitive mergers involving nonprofits, it cannot enforce action against them for anticompetitive behavior. So if a merger goes through, the FTC has limited authority to ensure the new entity plays fairly.
What’s more, the FTC has acknowledged it can’t keep up with its workload this year. It modified its antitrust review process to accommodate an increasing number of requests and its stagnant capacity. In July, the Biden administration issued an executive order about economic competition that explicitly acknowledges the negative impact of health care consolidation on U.S. communities. This is encouraging, signaling that the government is taking mergers seriously. Yet it’s unclear if the executive order will give the FTC more capacity, which is essential if it is to actually enforce antitrust laws.
At the state level, most of the antitrust power lies with the attorney general, who ultimately approves or challenges all mergers. Despite this authority, questionable mergers still go through.
In 2018, for example, two competing hospital systems in rural Tennessee merged to become Ballad Health and the only source of care for about 1.2 million residents. The deal was opposed by the FTC, which deemed it to be a monopoly. Despite the concerns, the state attorney general and Department of Health overrode the FTC’s ruling and approved the merger. (This is the same mechanism the Rhode Island hospitals hope to employ should the FTC oppose their merger.) As expected, Ballad Health then consolidated the services offered at its facilities and increased the fees on patient bills.
It’s clear that mechanisms exist to curb potentially harmful mergers and promote industry competition. It’s also clear they aren’t being used to the fullest extent. Unless these checks and balances lead to mergers being denied, their power over the market is limited.
Experts have been raising the alarm on health care consolidation for years. Mergers rarely lead to better care quality, access, or prices. Proposed mergers must be assessed and approved based on evidence, not industry pressure. If nothing changes, the consequences will be felt for years to come.
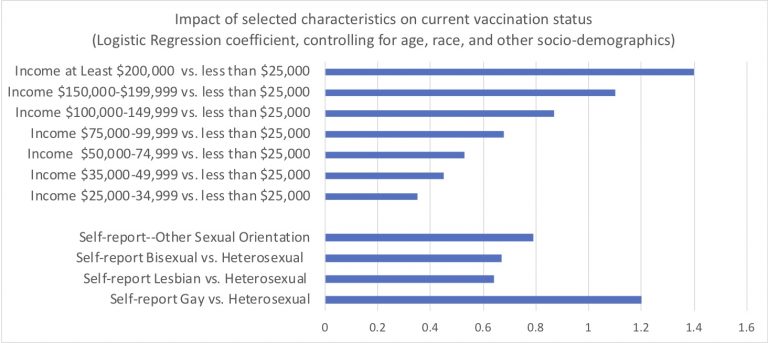
Last night I downloaded the latest Census Bureau July-August week 34 PULSE data. Over two cups of coffee, I ran the obvious multivariable logistic regressions to examine who is now fully vaccinated against COVID. See the above of this post for the full set of resulting Logit coefficients.
I’m sure Reviewer 2 would order due refinements to my quick analysis, were it immediately submitted for peer-review publication. My capacious study limitations section would note the inherent challenges of population surveys to gauge contentious questions like this. These data surely include response biases and likely overstate the true prevalence of COVID vaccination.
The overall patterns and disparities remain clear enough. Of course, we see huge disparities across regions, by education and by income. A bit more surprising: One group appears especially vulnerable and requires specific outreach…Yup. We must formulate culturally competent public health messaging for heterosexual non-Hispanic white Americans. This group conspicuously lags in vaccination status.
Among self-identified male respondents, heterosexual men were almost four times as likely to report not to be fully vaccinated (19%) as were gay men (5%)–an absolute different quite similar to the gradient observed between men with incomes less than $25,000 and those with incomes between $75,000 and $100,000.
I know that there daunting obstacles to reaching this disparity-population of heterosexual American men. We can’t let these barriers deter us. I’m joking–sort of. OK not really.
Winston Churchill loved paraprosdokians, figures of speech in which the latter part of a sentence or phrase is surprising or unexpected.
1. Where there’s a will, I want to be in it. 2. The last thing I want to do is hurt you, but it’s still on my list. 3. Since light travels faster than sound, some people appear bright until you hear them speak. 4. If I agreed with you, we’d both be wrong. 5. War does not determine who is right – only who is left. 6. Knowledge is knowing a tomato is a fruit. Wisdom is not putting it in a fruit salad. 7. They begin the evening news with ‘Good Evening,’ then proceed to tell you why it isn’t. 8. To steal ideas from one person is plagiarism. To steal from many is research. 9. I thought I wanted a career. Turns out, I just wanted pay checks. 10. In filling out an application, where it says, ‘In case of emergency, notify:’ I put “DOCTOR.” 11. I didn’t say it was your fault, I said I was blaming you. 12. Women will never be equal to men until they can walk down the street…with a bald head and a beer gut, and still think they are sexy. 13. Behind every successful man is his woman. Behind the fall of a successful man is usually another woman. 14. A clear conscience is the sign of a fuzzy memory. 15. You do not need a parachute to skydive. You only need a parachute to skydive twice. 16. Money can’t buy happiness, but it sure makes misery easier to live with. 17. There’s a fine line between cuddling and…holding someone down so they can’t get away. 18. I used to be indecisive. Now I’m not so sure. 19. You’re never too old to learn something stupid. 20. To be sure of hitting the target, shoot first and call whatever you hit the target. 21. Nostalgia isn’t what it used to be. 22. Change is inevitable, except from a vending machine. 23. Going to church doesn’t make you a Christian any more than standing in a garage makes you a car. 24. I’m supposed to respect my elders, but now it’s getting harder and harder for me to find one.