

Sign of the Times: High Deductible Health Care
https://mailchi.mp/e1b9f9c249d0/the-weekly-gist-september-15-2023?e=d1e747d2d8

Two of the nation’s largest nonprofit health systems, Salt Lake City, UT-based Intermountain Healthcare and Pittsburgh, PA-based UPMC, have recently announced plans to end their electronic health record (EHR) contracts with Oracle Cerner and transition, enterprise-wide, to Epic.
Intermountain, which operates 33 hospitals across seven states, plans to integrate Epic’s EHR into all of its facilities by 2025; its legacy SCL Health hospitals in Colorado and Montana already use Epic.
UPMC, which operates 40 hospitals in three states, has set mid-2026 as the target for consolidating its nine EHRs into a single platform with Epic. It has been using Oracle Cerner in inpatient settings and Epic for ambulatory care.
Both systems cited provider feedback and a desire to simplify patient record-keeping as key reasons behind their decisions to switch.
The Gist: With two more marquee health systems jumping ship for Epic, Oracle Cerner faces a steeper battle to maintain a foothold with health systems and may need to rethink its target market and value proposition.
Cerner initially appealed to large, progressive, value-oriented systems with highly customizable offerings, but over the years the resulting “Franken-Cerner” systems (as one CIO put it) became hard to maintain and scale.
Meanwhile, Epic continues to grow its lead in the domestic EHR market: it now covers roughly half of acute-care beds in the US and holds records on 78 percent of US patients.
Sitting on troves of health data, Epic is also well-positioned to become a leader in the rollout of next-generation healthcare AI, which it has already set in motion through its partnership with Microsoft.
https://mailchi.mp/e1b9f9c249d0/the-weekly-gist-september-15-2023?e=d1e747d2d8

Bloomberg reported this week that retail behemoth Walmart has engaged in talks to acquire a majority stake in ChenMed, a closely held value-based primary care company based in Miami, FL.
The deal would significantly expand Walmart’s primary care footprint and capabilities, adding to the 39 Walmart Health centers slated to be in operation by the end of this year.
ChenMed, which operates 120+ clinics across 15 states, delivers primary care to complex Medicare Advantage beneficiaries, taking risk for the total cost of care, and has grown its membership by 36 percent annually across the last decade. It has remained privately owned by the Chen family, but recently revamped its leadership structure and tapped UnitedHealth Group (UHG) veteran Steve Nelson to run operations. ChenMed has an expected value of several billion dollars, a price that could be driven upwards if other bidders express interest. Bloomberg’s sources emphasized that the deal could still be weeks away and that no terms have been finalized.
The Gist: Should this purchase go through, it might change Walmart’s status as a “sleeping giant” in healthcare.
ChenMed’s primary care model and strong foothold in the Southeast would dovetail with Walmart’s store clinic footprint and its 10-year partnership with UHG to drive value-based care adoption in that region.
With ChenMed competitors Oak Street, One Medical, and VillageMD now backed or owned by some of Walmart’s biggest competitors, Walmart may view ChenMed as its best opportunity to scale its primary care footprint through a large acquisition.
However, much of ChenMed’s success to date has been attributed to its strong culture and track record of physician recruitment and retention—something a large company like Walmart may have challenges preserving.
https://mailchi.mp/e1b9f9c249d0/the-weekly-gist-september-15-2023?e=d1e747d2d8

On Monday, the Food and Drug Administration authorized new COVID vaccines from Moderna and Pfizer-BioNTech, and the Centers for Disease Control and Prevention followed Tuesday by recommending the shots be given as a single dose for most people five years of age and older. Children older than six months but younger than five, as well as completely unvaccinated people of any age, may be eligible for multiple doses.
These vaccines were formulated to target the XBB.1.5. variant,
which was the dominant strain in January but has since receded, although initial results suggest they remain effective against all currently circulating variants. Pharmacies and healthcare providers are expected to have the updated vaccines available by early next week.
The Gist: Due to the end of the COVID public health emergency in May, this COVID vaccination campaign will be the first not directly bankrolled by the federal government.
While insurers are still required to cover vaccinations without cost-sharing, the uninsured may find free shots, which the Biden administration says it will still provide at certain locations, harder to access.
Unlike past COVID boosters, reframing this shot as an annual vaccine that patients receive along with their flu shots should help with the rollout, as around 50 percent of Americans got a flu shot in 2022 while only 17 percent received the bivalent COVID booster.
With COVID cases and hospitalizations currently rising, promoting widespread uptake is critical to dampening a likely winter COVID spike.
However, public health officials will have to overcome many Americans’ wearied indifference toward COVID to motivate them to get vaccinated.
https://mailchi.mp/e1b9f9c249d0/the-weekly-gist-september-15-2023?e=d1e747d2d8
We had an interesting exchange with a health system CEO this week, which started as a discussion about what to tell his board about the rapidly changing AI landscape, but drifted into a larger conversation about how human-dependent healthcare is. His system has invested heavily in virtual care and has begun to make strides in applying automation and artificial intelligence to both clinical care delivery and key operational processes. He’s glimpsed the potential for process automation—AI’s less sexy sibling, now that “generative AI” has burst onto the scene—to radically reduce staffing costs in areas like revenue cycle management.
And that’s making him wonder about the larger implications for workforce development—both inside his organization and in the economy as a whole. Like many health systems, his organization not only provides care to the community, but also employment opportunities and job growth.
What happens when large swaths of healthcare delivery become more automated—how will the system look to retrain those workers for other roles?
One clear area of workforce need over the coming decades will be hands-on caregiving for an older, sicker population that wants to age in place. Health aides, home health workers, community social workers and so forth—will those roles ultimately be filled by workers from other parts of healthcare (and the economy beyond) who find themselves displaced by AI and robotics?
Will the Amazon warehouse worker of today become the home care worker of tomorrow?
The conversation was fascinating and made us realize that we’ve paid too little attention to two key issues.
First, the tension between healthcare as a cost problem and healthcare as a source of job growth.
And second, the redistribution of workers into roles that will require hands-on, human presence (like caregiving) in the coming wave of AI and robotics.
https://mailchi.mp/e1b9f9c249d0/the-weekly-gist-september-15-2023?e=d1e747d2d8
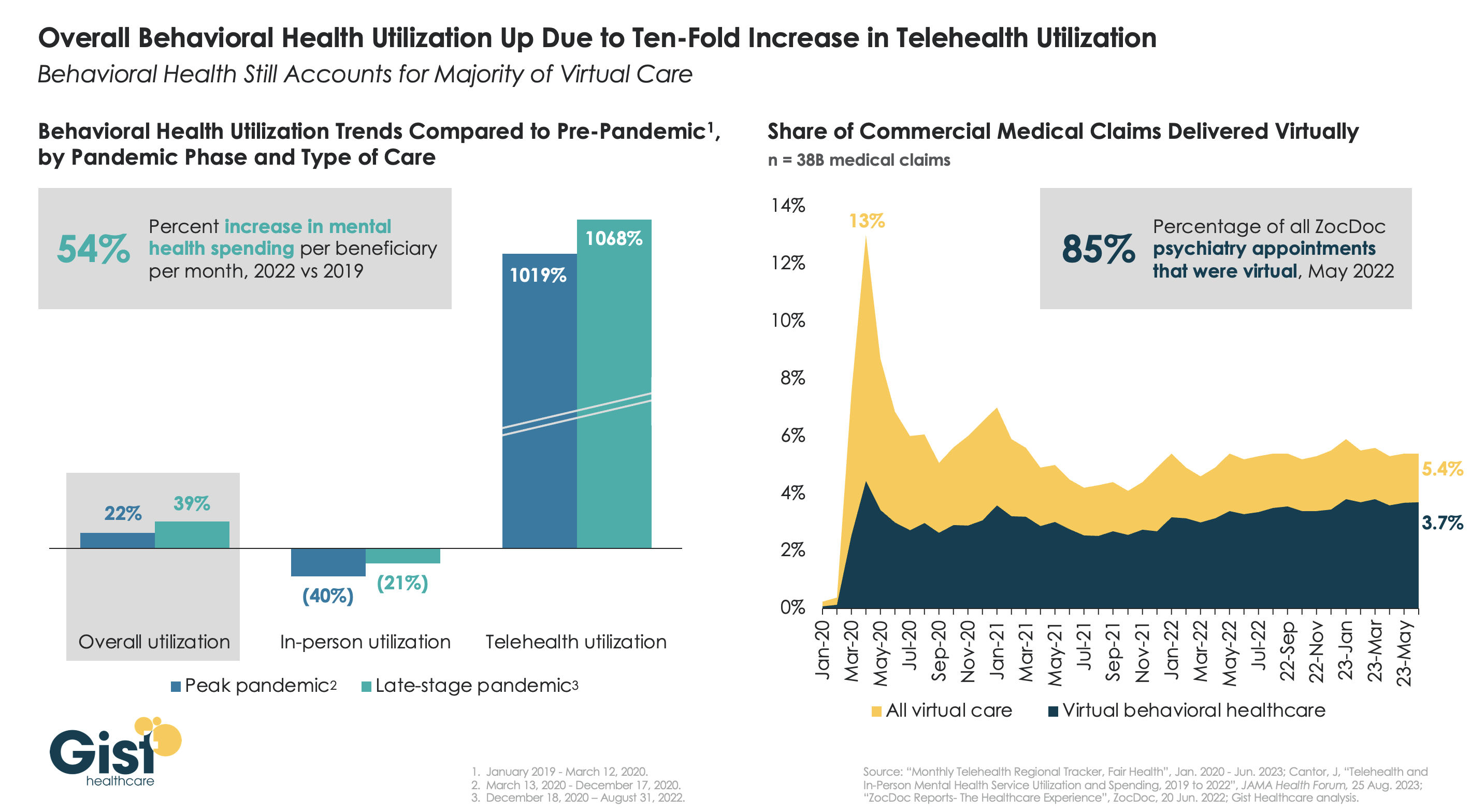
The pandemic worsened the existing mental health crisis in the United States, greatly increasing demand for care. In this week’s graphic, we highlight new data from JAMA Health Forum on mental healthcare trends from 2019 to 2022.
Overall behavioral health utilization increased in 2022 compared to pre-pandemic and peak-pandemic levels, fueled by a ten-fold increase in telehealth usage.
In-person behavioral health utilization decreased early in the pandemic and declines continued in 2022, compared to pre-pandemic levels. Behavioral health still accounts for more than two-thirds of all telehealth visits, a trend that has remained largely unchanged since 2021.
While many consumers and mental health providers continue to embrace telehealth as a means to expand access and increase affordability, a recent Morning Consult survey found that most Americans actually favor in-person visits for quality and efficiency—that is, if they can access it.
Additionally, the future of some types of virtual behavioral healthcare remains murky as the Drug Enforcement Agency (DEA) has yet to establish rules for prescribing controlled substances via telehealth beyond November 2024.
https://mailchi.mp/e1b9f9c249d0/the-weekly-gist-september-15-2023?e=d1e747d2d8

An article published this week in Stat documents private equity’s move into the cardiovascular space. There’s reason to suspect private equity ownership could exacerbate cardiology’s overuse problem, according to several cardiologists and researchers. Studies has found private equity acquisition results in more patients, more visits per patient, and higher charges.
Outpatient atherectomies have become a poster child for overutilization, with the volume billed to Medicare more than doubling from 2011-2021.
The Gist: Fueled by the growing number of states allowing outpatient cardiac catheterization, all signs point to cardiovascular practices being the next specialty courted for PE rollups.
However, the service line brings more complexities to deal structure and future returns than recent targets like dermatology and orthopedics. Heart and vascular groups are more heterogeneous, and less profitable medical management of conditions like congestive heart failure accounts for a greater portion of patient volume. Much more of the medical group business is intertwined with inpatient care, and, unlike other proceduralists, around 80 percent of cardiologists are already employed by health systems. While that doesn’t mean health systems are safe from cardiologists seceding for the promise of PE windfalls,
the closer PE firms get to the “heart” of medicine, the more they’ll find their standard playbook at odds with the broad spectrum of care that cardiovascular specialists provide—and the more they’ll find that partnering with local hospitals will be non-negotiable to maintain the book of business.
Politicians, economists, auto industry analysts and main street business owners are closely watching the UAW strike that began at midnight last Thursday. Healthcare should also pay attention, especially hospitals. medical groups and facility operators where workforce issues are mounting.
Auto manufacturing accounts for 3% of America’s GDP and employs 2.2 million including 923,000 in frontline production. It’s high-profile sector industry in the U.S. with its most prominent operators aka “the Big Three” operating globally. Some stats:
By comparison, the healthcare services industry in the U.S.—those that operate facilities and services serving patients—employs 9 times more workers, is 29 times bigger ($104 Billion vs. $2.99 trillion/65% of total spend) and 6 times more integral in the overall economy (3% vs. 18.3% of GDP).
Surprisingly, average hourly wages are similar ($31.07 in auto manufacturing vs. $33.12 in healthcare per BLS) though the range is wider in healthcare since it encompasses licensed professionals to unskilled support roles. There are other similarities:
Ironically, the genesis of the UAW dispute is not about wages; it is about job security as electric-powered vehicles that require fewer parts and fewer laborers become the mainstay of the sector. CEO compensation and the corporate profits of the Big Three are talking points used by union leaders to galvanize sympathizer antipathy of “corporate greed” and unfair treatment of frontline workers.
But the real issue is uncertainty about the future: will auto workers have jobs and health benefits in their new normal?
In healthcare services sectors—hospitals, medical groups, post-acute care facilities, home-care et al—the scenario is similar: workers face an uncertain future but significantly more complicated. Corporate greed, CEO compensation and workforce discontent are popular targets in healthcare services media coverage but the prominence of not-for-profit organizations in healthcare services obfuscates direct comparisons to for-profit organizations which represents less than a third of the services economy. For example, CEO compensation in NFPs—a prominent target of worker attention—is accounted differently for CEOs in investor-owned operations in which stock ownership is not treated as income until in options are exercised or shares sold. Annual 990 filings by NFPs tell an incomplete story nonetheless fodder for misinformation.
The competitive landscape and regulatory scrutiny for healthcare services are also more complicated for healthcare services. Unlike auto manufacturing where electric vehicles are forcing incumbents to change, there’s no consensus about what the new normal in U.S. healthcare services will be nor a meaningful industry-wide effort to define it. Each sector is defining its own “future state” based on questionable assumptions about competitors, demand, affordability, workforce requirements and more. Imagine an environmental scan in automakers strategy that’s mute on Tesla, or mass transit, Zoom, pandemic lock-downs or energy costs?
While the outlook for U.S. automakers is guardedly favorable, per Moody’s and Fitch, for not-for-profit health services operators it’s “unsustainable” and “deteriorating.”
Nonetheless, the parallels between the current state of worker sentiment in the U.S. auto manufacturing and healthcare services sectors are instructive. Auto and healthcare workers want job security and higher pay, believing their company executives and boards but corporate profit above their interests and all else. And polls suggest the public’s increasingly sympathetic to worker issues and strikes like the UAW more frequent.
Ultimately, the UAW dispute with the Big Three will be settled. Ultimately, both sides will make concessions. Ultimately, the automakers will pass on their concession costs to their customers while continuing their transitions to electric vehicles.
In health services, operators are unable to pass thru concession costs due to reimbursement constraints that, along with supply chain cost inflation, wipe out earnings and heighten labor tension.
So, the immediate imperatives for healthcare services organizations seem clear as labor issues mount and economics erode:
Stay tuned to the UAW strike and consider fresh approaches to labor issues. It’s not a matter of if, but when.
PS: I drive an electric car—my step into the auto industry future state. It took me 9 hours last Thursday to drive 275 miles to my son’s wedding because the infrastructure to support timely battery charges in route was non-existent. Ironically, after one of three self-charges for which I paid more than equivalent gas, I was prompted to “add a tip”. So, the transition to electric vehicles seems certain, but it will be bumpy and workers will be impacted.
The future state for healthcare is equally frought with inadequate charging stations aka “systemness” but it’s inevitable those issues will be settled. And worker job security and labor costs will be significantly impacted in the process.

