Lown Institute berates greedy pricing, ethical lapses, wallet biopsies, and avoidable shortages.
Greedy corporations, uncaring hospitals, individual miscreants, and a task force led by Jared Kushner were dinged Tuesday in the Lown Institute‘s annual Shkreli awards, a list of the top 10 worst offenders for 2020.
Named after Martin Shkreli, the entrepreneur who unapologetically raised the price of an anti-parasitic drug by a factor of 56 in 2015 (now serving a federal prison term for unrelated crimes), the list of shame calls out what Vikas Saini, the institute’s CEO, called “pandemic profiteers.” (Lown bills itself as “a nonpartisan think tank advocating bold ideas for a just and caring system for health.”)
Topping the listwas the federal government itself and Jared Kushner, President’s Trump’s son-in-law, who led a personal protective equipment (PPE) procurement task force. The effort, called Project Airbridge, was to “airlift PPE from overseas and bring it to the U.S. quickly,” which it did.
“But rather than distribute the PPE to the states, FEMA gave these supplies to six private medical supply companies to sell to the highest bidder, creating a bidding war among the states,” Saini said. Though these supplies were supposed to go to designated pandemic hotspots, “no officials from the 10 hardest hit counties” said they received PPE from Project Airbridge. In fact, federal agencies outbid states or seized supplies that states had purchased, “making it much harder and more expensive” for states to get supplies, he said.
Number twoon the institute’s list: vaccine maker Moderna, which received nearly $1 billion in federal funds to develop its mRNA COVID-19 preventive. It set a price of between $32 and $37 per dose, more than the U.S. agreed to pay for other COVID vaccines. “Although the U.S. has placed an order for $1.5 billion worth of doses at a discount, a price of $15 per dose, given the upfront investment by the U.S. government, we are essentially paying for the vaccine twice,” said Lown Institute Senior Vice President Shannon Brownlee.
Webcast panelist Don Berwick, MD, former acting administrator for the Centers for Medicare & Medicaid Services, noted that a lot of work went into producing the vaccine at an impressive pace, “and if there’s not an immune breakout, we’re going to be very grateful that this happened.” But, he added, “I mean, how much money is enough? Maybe there needs to be some real sense of discipline and public spirit here that goes way beyond what any of these companies are doing.”
In third place: four California hospital systems that refused to take COVID-19 patients or delayed transfers from hospitals that were out of beds.A Wall Street Journal investigation found that these refusals or delays were based on the patients’ ability to pay; many were on Medicaid or were uninsured.
“In the midst of such a pandemic, to continue that sort of behavior is mind boggling,” said Saini. “This is more than the proverbial wallet biopsy.”
The remaining seven offenders:
4. Poor nursing homes decisions, especially one by Soldiers’ Home for Veterans in western Massachusetts, that worsened an already terrible situation. At Soldiers’ Home, management decided to combine the COVID-19 unit with a dementia unit because they were low on staff, said Brownlee. That allowed the virus to spread rapidly, killing 76 residents and staff as of November. Roughly one-third of all COVID-19 deaths in the U.S. have been in long-term care facilities.
5. Pharmaceutical giants AstraZeneca, GlaxoSmithKline, Pfizer, and Johnson & Johnson,which refused to share intellectual property on COVID-19, instead deciding to “compete for their profits instead,” Saini said. The envisioned technology access pool would have made participants’ discoveries openly available “to more easily develop and distribute coronavirus treatments, vaccines, and diagnostics.”
Saini added that he was was most struck by such an attitude of “historical blindness or tone deafness” at a time when the pandemic is roiling every single country.
Berwick asked rhetorically, “What would it be like if we were a world in which a company like Pfizer or Moderna, or the next company that develops a really great breakthrough, says on behalf of the well-being of the human race, we will make this intellectual property available to anyone who wants it?”
6. Elizabeth Nabel, MD, CEO of Brigham and Women’s Hospital in Boston, because she defended high drug prices as a necessity for innovation in an op-ed, without disclosing that she sat on Moderna’s board. In that capacity, she received $487,500 in stock options and other payments in 2019. The value of those options quadrupled on the news of Moderna’s successful vaccine. She sold $8.5 million worth of stock last year, after its value nearly quadrupled. She resigned from Moderna’s board in July and, it was announced Tuesday, is leaving her CEO position to join a biotech company founded by her husband.
7. Hospitals that punished clinicians for “scaring the public,” suspending or firing them, because they “insisted on wearing N95 masks and other protective equipment in the hospital,” said Saini. Hospitals also fired or threatened to fire clinicians for speaking out on COVID-19 safety issues, such as the lack of PPE and long test turnaround times.
Webcast panelist Mona Hanna-Attisha, MD, the Flint, Michigan, pediatrician who exposed the city’s water contamination, said that healthcare workers “have really been abandoned in this administration” and that the federal Occupational Safety and Health Administration “has pretty much fallen asleep at the wheel.” She added that workers in many industries such as meatpacking and poultry processing “have suffered tremendously from not having the protections or regulations in place to protect [them].”
8. Connecticut internist Steven Murphy, MD, who ran COVID-19 testing sites for several towns, but conducted allegedly unnecessary add-ons such as screening for 20 other respiratory pathogens. He also charged insurers $480 to provide results over the phone, leading to total bills of up to $2,000 per person.
“As far as I know, having an MD is not a license to steal, and this guy seemed to think that it was,” said Brownlee.
9. Those “pandemic profiteers”who hawked fake and potentially harmful COVID-19 cures. Among them: televangelist Jim Bakker sold “Silver Solution,” containing colloidal silver, and the “MyPillow Guy,” Mike Lindell, for his boostering for oleandrin.
“Colloidal silver has no known health benefits and can cause seizures and organ damage. Oleandrin is a biological extract from the oleander plant and known for its toxicity and ingesting it can be deadly,” said Saini.
Others named by the Lown Institute include Jennings Ryan Staley, MD — now under indictment — who ran the “Skinny Beach Med Spa” in San Diego which sold so-called COVID treatment packs containing hydroxychloroquine, antibiotics, Xanax, and Viagra, all for $4,000.
Berwick commented that such schemes indicate a crisis of confidence in science, adding that without facts and science to guide care, “patients get hurt, costs rise without any benefit, and confusion reigns, and COVID has made that worse right now.”
Brownlee mentioned the “huge play” that hydroxychloroquine received and the FDA’s recent record as examples of why confidence in science has eroded.
10. Two private equity-owned companies that provide physician staffing for hospitals, Team Health and Envision, that cut doctors’ pay during the first COVID-19 wave while simultaneously spending millions on political ads to protect surprise billing practices. And the same companies also received millions in COVID relief funds under the CARES Act.
Berwick said surprise billing by itself should receive a deputy Shkreli award, “as out-of-pocket costs to patients have risen dramatically and even worse during the COVID pandemic… and Congress has failed to act. It’s time to fix this one.”
Additional evidence continued to suggest blood type may not only play a role in COVID-19 susceptibility, but also severity of infection, according to two retrospective studies.
In Denmark, blood type O was associated with reduced risk of developing COVID-19 (RR 0.87, 95% CI 0.83-0.91), based on the proportion of those with type O blood who tested positive for SARS-CoV-2 compared with a reference population, reported Torben Barington, MD, of Odense University Hospital, and colleagues.
However, there was no increased risk for COVID-19 hospitalization or death associated with blood type, the authors wrote in Blood Advances.
Limitations to the data include that ABO blood group information was only available for 62% of individuals, and that the sex of the testing population was skewed, with women accounting for 71% who tested negative and 67% who tested positive.
They pointed to the recent research that blood type plays a role in infection, noting the lower than expected prevalence of blood group O individuals among COVID-19 patients. Researchers also observed how blood groups are “increasingly recognized to influence susceptibility to certain viruses,” among them SARS-CoV-1 and norovirus, adding that individuals with A, B, and AB blood types may be at “increased risk for thrombosis and cardiovascular diseases,” which are important comorbidities among patients hospitalized with COVID-19.
ABO and RhD blood group information was available for 473,654 individuals who were tested for SARS-CoV-2 from February 27 to July 30, as well as for 2,204,742 individuals not tested for SARS-CoV-2 as a reference.
Of the individuals tested, 7,422 tested positive for SARS-CoV-2. About a third of both those who tested positive and negative were men, and those with positive tests were slightly older (52 vs 50, respectively).
Among individuals testing positive for SARS-CoV-2, about 38% (95% CI 37.5-39.5%) belonged to blood group O versus about 42% of those in the reference population. There were significantly more group A and AB individuals in the positive testing group versus the reference population, though the difference was non-significant for group B. When group O individuals were removed, there was no difference between the remaining groups.
Blood Type Linked to COVID-19 Severity?
Meanwhile, a second, smaller study in Blood Advances did report a connection between blood type and COVID-19 severity.
Blood types A or AB in COVID-19 patients were associated with increased risk for mechanical ventilation, continuous renal replacement therapy, and prolonged ICU admission versus patients with blood type O or B, according to Mypinder Sekhon, MD, of the University of British Columbia in Vancouver, and colleagues. Inflammatory cytokines did not differ between groups, however.
These authors also cited research that found that blood groups were linked to virus susceptibility, but that the relationship between SARS-CoV-2 infection severity and blood groups remains “unresolved.” However, COVID-19 appears to be a multisystem disease with renal and hepatic manifestations.
“If ABO blood groups play a role in determining disease severity, these differences would be expected to manifest within multiple organ systems and hold relevance for multiple resource-intensive treatments, such as mechanical ventilation and continuous renal replacement therapy,” Sekhon and colleagues wrote.
They collected data from six metropolitan Vancouver hospitals from Feb. 21 to April 28, identifying 95 COVID-19 patients admitted to an ICU with known ABO blood type.
Among these patients, 57 were group O or B, while 38 were group A or AB. A significantly higher proportion of A/AB patients required mechanical ventilation versus O/B patients (84% vs 61%, respectively, P=0.02). Similar figures were seen for patients requiring continuous renal replacement therapy (32% vs 9%, P=0.04). Median ICU stay length was also longer for A or AB patients compared with O or B patients (13.5 days vs 9 days, P=0.03).
There was no difference in probability of ICU discharge, and eight patients died in the O/B group versus nine patients in the A/AB group. Not surprisingly, biomarkers of renal and hepatic dysfunction were higher in the A/AB group, as well.
“The unique part of our study is our focus on the severity effect of blood type on COVID-19. We observed this lung and kidney damage, and in future studies, we will want to tease out the effect of blood group and COVID-19 on other vital organs,” Sekhon said in a statement.
About 25% of patients were missing data on blood group, and the nature of the study makes it impossible to infer causality, the authors acknowledged. Ethnic ancestry and outcomes in patients with COVID-19 could be an unaddressed confounder. Additionally, anti-A antibody titers may affect COVID-19 severity, and these were not measured.
The first month of the pandemic was also supposed to be the month I got pregnant, but my clinic closed and plans changed. Doctors and nurses needed personal protective equipment to tend to patients with covid-19, not women with recurrent miscarriages.
When the clinic reopened several months later, it turned out my husband and I had only been delaying yet another loss: In late August, he obeyed the medical center’s strict coronavirus protocols by waiting anxiously in the car while I trudged inside, masked and hand-sanitized, to receive a miscarriage diagnosis alone. I searched the ultrasound screen for the rhythmic beat of a heart, and then accepted that whatever had once been there was now gone.
But that was 2020 for you, consistent only in its utter crappiness. For every inspiring video of neighbors applauding a shift change at the hospital, another video of a bone-tired nurse begging viewers to believe covid was real, it wasn’t a hoax, wear a mask.
For every protest organized by activists who understood racism is also a long-term crisis, an appearance by the Proud Boys; for every GoFundMe successfully raising money for a beloved teacher’s hospital bills, a bitter acknowledgment that online panhandling is our country’s version of a safety net.
Millions of citizens stood in line for hours to vote for the next president and then endured weeks of legal petitions arguing that their votes should be negated. The basis for these legal actions were conspiracy theories too wild to be believed, except that millions of other citizens believed them.
And that was 2020 for you, too: accepting the increasingly obvious reality that the country was in peril, built on iffy foundations that now buckled under pressure. My loved ones who worked as waiters or bartenders or physical therapists were choosing between health and paychecks, and even from the lucky safety of my work-from-home job, each day began to feel like watching America itself arrive at a hospital in bad shape, praying that doctors or clergy could find something they were able to save.
Is there a heartbeat?
You want the answer to be yes, but even so, it was hard to imagine how we would come back from this.
What kind of delusional person would even try to get pregnant in this world? In my case it would never be a happy accident; it would always be a herculean effort. And so it seemed I should have some answers.
How do you explain to a future child: Sorry, we can’t fix climate change; we can’t even get people to agree that we should wear masks in grocery stores? How do you explain the frustration of seeing brokenness, and then the wearying choice of trying to fix it instead of abandoning it? How do you say, Love it anyway. You’re inheriting an absolute mess, but love it anyway?
I found myself asking a lot of things like this in 2020, but really they were all variations of the same question: What does it mean to have hope?
But in the middle of this, scientists worked quietly in labs all over the world. They applied the scientific method with extraordinary discipline and speed. A vaccine was developed. Tens of thousands of volunteers rolled up their sleeves and said, Try it out on me.
It was approved, and a nurse from Long Island was the first American televised receiving it. Her name was Sandra Lindsay, an immigrant from Jamaica who had come to the United States 30 years ago and who had spent the last year overseeing critical care teams in back-to-back shifts. She said she had agreed to go first to show communities of color, long abused, brushed-off or condescended to by the medical system, that the vaccine was safe.
Here was hope. And more than that, here was hope from a woman who had more reason than most to be embittered: an exhausted health-care worker who knew too well America’s hideous racial past and present, who nonetheless also knew there was only one way out of the tunnel. Here she was, rolling up her own sleeve, and there were the lines of hospital employees ready to go after her, and there were the truck drivers ferrying shipments of syringes.
I can’t have been the only person to watch the video of those early inoculations, feeling elated and tired, and to then burst into tears. I can’t have been the only person to realize that even as 2020 revealed brokenness, it also contained such astounding undercurrents of good.
The scientific method works whether you accept it or not. Doctors try to save you whether you respected public-health guidelines or not. Voter turnout was astronomical because individual citizens realized they were all, every one of them, necessary pieces in a puzzle, even if they couldn’t see what the final picture was supposed to look like.
The way to believe in America is to believe those things are passed down, too.
Sometime in October, a couple of months after my last miscarriage — when the country was riding up on eight months of lonely and stoic birthdays, graduations, deaths and weddings — I went into the bathroom and saw a faint second line on a First Response pregnancy test. It was far from my first rodeo, so I knew better than to get excited. I mentioned it to my husband with studied nonchalance, I told him that I’d test again in a few days but that we should assume the worst would happen.
Two weeks after that, I had a doctor’s appointment, and then another a week later, each time assuming the worst, but each time scheduling another appointment anyway, until eventually I was further along than I’d ever gotten before — by one day, then three days, then thirty.
I am not a superstitious person. I don’t believe that good things always come to those who deserve them. I believe that stories regularly have sad endings and that it’s often nobody’s fault when they do, and that we should tell more stories with sad endings so that people who experience them know that they’re not alone.
But 2020 has taught me that I am, for better or worse, someone who wants to hope for things. To believe in the people who developed vaccines. In the people who administered them. In Sandra Lindsay. In the people who delivered groceries, who sewed masks, who have long cursed America’s imperfect systems and long fought to change them, who still donate $10 to a sick teacher’s GoFundMe.
At my most recent appointment, the doctor’s office was backed up in a holiday logjam. I sat in the exam room for nearly three hours while my husband again waited anxiously in the car. I texted him sporadic updates and tried to put hope in a process that so far had not seemed to warrant my hope.
It all felt precarious. The current reality always feels precarious.
And yet there we all are together, searching for signs of life, hoping that whatever we emerge to can be better than what we had before, and that whatever we build will become our new legacy. The sonographer finally arrived and turned on the machine.
A Florida taxi driver and his wife had seen enough conspiracy theories online to believe the virus was overblown, maybe even a hoax. So no masks for them. Then they got sick. She died. A college lecturer had trouble refilling her lupus drug after the president promoted it as a treatment for the new disease. A hospital nurse broke down when an ICU patient insisted his illness was nothing worse than the flu, oblivious to the silence in beds next door.
Lies infected America in 2020. The very worst were not just damaging, but deadly.
President Donald J. Trump fueled confusion and conspiracies from the earliest days of the coronavirus pandemic. He embraced theories that COVID-19 accounted for only a small fraction of the thousands upon thousands of deaths. He undermined public health guidance for wearing masks and cast Dr. Anthony Fauci as an unreliable flip-flopper.
But the infodemic was not the work of a single person.
Anonymous bad actors offered up junk science. Online skeptics made bogus accusations that hospitals padded their coronavirus case numbers to generate bonus payments. Influential TV and radio opinion hosts told millions of viewers that social distancing was a joke and that states had all of the personal protective equipment they needed (when they didn’t).
It was a symphony of counter narrative, and Trump was the conductor, if not the composer. The message: The threat to your health was overhyped to hurt the political fortunes of the president.
Every year, PolitiFact editors review the year’s most inaccurate statements to elevate one as the Lie of the Year. The “award” goes to a statement, or a collection of claims, that prove to be of substantive consequence in undermining reality.
It has become harder and harder to choose when cynical pundits and politicians don’t pay much of a price for saying things that aren’t true. For the past month, unproven claims of massive election fraud have tested democratic institutions and certainly qualify as historic and dangerously bald-faced. Fortunately, the constitutional foundations that undergird American democracy are holding.
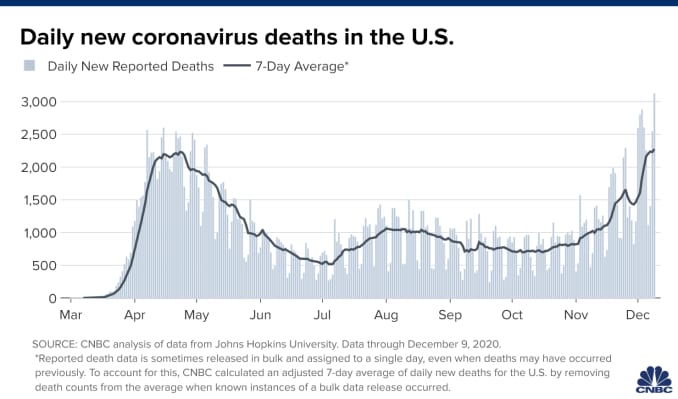
Meanwhile, the coronavirus has killed more than 300,000 in the United States, a crisis exacerbated by the reckless spread of falsehoods.
PolitiFact’s 2020 Lie of the Year: claims that deny, downplay or disinform about COVID-19.
‘I always wanted to play it down’
On Feb. 7, Trump leveled with book author Bob Woodward about the dangers of the new virus that was spreading across the world, originating in central China. He told the legendary reporter that the virus was airborne, tricky and “more deadly than even your strenuous flus.”
Trump told the public something else. OnFeb. 26, the president appeared with his coronavirus task force in the crowded White House briefing room. A reporter asked if he was telling healthy Americans not to change their behavior.
“Wash your hands, stay clean. You don’t have to necessarily grab every handrail unless you have to,” he said, the room chuckling. “I mean, view this the same as the flu.”
Three weeks later, March 19, he acknowledged to Woodward: “To be honest with you, I wanted to always play it down. I still like playing it down. Because I don’t want to create a panic.”
His acolytes in politics and the media were on the same page. Rush Limbaugh told his audience of about 15 million on Feb. 24 that coronavirus was being weaponized against Trump when it was just “the common cold, folks.” That’s wrong — even in the early weeks, it was clear the virus had a higher fatality rate than the common cold, with worse potential side effects, too.
As the virus was spreading, so was the message to downplay it.
“There are lots of sources of misinformation, and there are lots of elected officials besides Trump that have not taken the virus seriously or promoted misinformation,” said Brendan Nyhan, a government professor at Dartmouth College. “It’s not solely a Trump story — and it’s important to not take everyone else’s role out of the narrative.”
The skeptics cited Centers for Disease Control and Prevention data to claim that only 6% of COVID-19 deaths could actually be attributed to the virus. On Aug. 24, BlazeTV host Steve Deace amplified it on Facebook.
“Here’s the percentage of people who died OF or FROM Covid with no underlying comorbidity,” he said to his 120,000 followers. “According to CDC, that is just 6% of the deaths WITH Covid so far.”
That misrepresented the reality of coronavirus deaths. The CDC had always said people with underlying health problems — comorbidities — were most vulnerable if they caught COVID-19. The report was noting that 6% died even without being at obvious risk.
But for those skeptical of COVID-19, the narrative confirmed their beliefs. Facebook users copied and pasted language from influencers like Amiri King, who had 2.2 million Facebook followers before he was banned. The Gateway Pundit called it a “SHOCK REPORT.”
“I saw a statistic come out the other day, talking about only 6% of the people actually died from COVID, which is very interesting — that they died from other reasons,” Trump told Fox News host Laura Ingraham on Sept. 1.
Fauci, director of the National Institute of Allergy and Infectious Diseases, addressed the claim on “Good Morning America” the same day.
“The point that the CDC was trying to make was that a certain percentage of them had nothing else but just COVID,” he said. “That does not mean that someone who has hypertension or diabetes who dies of COVID didn’t die of COVID-19 — they did.”
Trump retweeted the message from an account that sported the slogans and symbols of QAnon, a conspiracy movement that claims Democrats and Hollywood elites are members of an underground pedophilia ring.
False information moved between social media, Trump and TV, creating its own feedback loop.
“It’s an echo effect of sorts, where Donald Trump is certainly looking for information that resonates with his audiences and that supports his political objectives. And his audiences are looking to be amplified, so they’re incentivized to get him their information,” said Kate Starbird, an associate professor and misinformation expert at the University of Washington.Weakening the armor: misleading on masks
At the start of the pandemic, the CDC told healthy people not to wear masks, saying they were needed for health care providers on the frontlines. But on April 3 the agency changed its guidelines, saying every American should wear non-medical cloth masks in public.
Trump announced the CDC’s guidance, then gutted it.
“So it’s voluntary. You don’t have to do it. They suggested for a period of time, but this is voluntary,” Trump said at a press briefing. “I don’t think I’m going to be doing it.”
Rather than an advance in best practices on coronavirus prevention, face masks turned into a dividing line between Trump’s political calculations and his decision-making as president. Americans didn’t see Trump wearing a mask until a July visit to Walter Reed National Military Medical Center.
In September, the CDC reported a correlation between people who went to bars and restaurants, where masks can’t consistently be worn, and positive COVID-19 test results. Bloggers and skeptical news outlets countered with a misleading report about masks.
On Oct. 13, the story landed on Fox News’ flagship show, “Tucker Carlson Tonight.” During the show, Carlson claimed “almost everyone — 85% — who got the coronavirus in July was wearing a mask.”
“So clearly (wearing a mask) doesn’t work the way they tell us it works,” Carlson said.
That’s wrong, and it misrepresented a small sample of people who tested positive. Public health officials and infectious disease experts have been consistent since April in saying that face masks are among the best ways to prevent the spread of COVID-19.
But two days later, Trump repeated the 85% stat during a rally and at a town hall with NBC’s Savannah Guthrie.
“I tell people, wear masks,” he said at the town hall. “But just the other day, they came out with a statement that 85% of the people that wear masks catch it.”
The assault on hospitals
On March 24, registered nurse Melissa Steiner worked her first shift in the new COVID-19 ICU of her southeast Michigan hospital. After her 13-hour day caring for two critically ill patients on ventilators, she posted a tearful video.
“Honestly, guys, it felt like I was working in a war zone,” Steiner said. “(I was) completely isolated from my team members, limited resources, limited supplies, limited responses from physicians because they’re just as overwhelmed.”
“I’m already breaking, so for f—’s sake, people, please take this seriously. This is so bad.”
Steiner’s post was one of manyemotionalpleas offered by overwhelmed hospital workers last spring urging people to take the threat seriously. The denialists mounted a counter offensive.
On March 28, Todd Starnes, a conservative radio host and commentator, tweeted a video from outside Brooklyn Hospital Center. There were few people or cars in sight.
“This is the ‘war zone’ outside the hospital in my Brooklyn neighborhood,” Starnes said sarcastically. The video racked up more than 1.5 million views.
Starnes’ video was one of the first examples of #FilmYourHospital, a conspiratorial social media trend that pushed back on the idea that hospitals had been strained by a rapid influx of coronavirus patients.
Several internet personalities asked people to go out and shoot their own videos. The result: a series of user-generated clips taken outside hospitals, where the response to the pandemic was not easily seen. Over the course of a week, #FilmYourHospital videos were uploaded to YouTube and posted tens of thousands of times on Twitter and Facebook.
Nearly two weeks and more than 10,000 deaths later, Fox News featured a guest who opened a new misinformation assault on hospitals.
Dr. Scott Jensen, a Minnesota physician and Republican state senator, told Ingraham that, because hospitals were receiving more money for COVID-19 patients on Medicare — a result of a coronavirus stimulus bill — they were overcounting COVID-19 cases. He had no proof of fraud, but the cynical story took off.
Trump used the false report on the campaign trail to continue to minimize the death toll.
“Our doctors get more money if somebody dies from COVID,” Trump told supporters at a rally in Waterford, Mich., Oct. 30. “You know that, right? I mean, our doctors are very smart people. So what they do is they say, ‘I’m sorry, but, you know, everybody dies of COVID.’”
The real fake news: The Plandemic
The most viral disinformation of the pandemic was styled to look like it had the blessing of people Americans trust: scientists and doctors.
In a 26-minute video called “Plandemic: The Hidden Agenda Behind COVID-19,” a former scientist at the National Cancer Institute claimed that the virus was manipulated in a lab, hydroxychloroquine is effective against coronaviruses, and face masks make people sick.
Judy Mikovits’ conspiracies received more than 8 million views in May thanks in part to the online outrage machine — anti-vaccine activists, anti-lockdown groups and QAnon supporters — that push disinformation into the mainstream. The video was circulated in a coordinated effort to promote Mikovits’ book release.
A couple of months later, a similar effort propelled another video of fact-averse doctors to millions of people in only a few hours.
On July 27, Breitbart publisheda clipof a press conference hosted by a group called America’s Frontline Doctors in front of the U.S. Supreme Court. Looking authoritative in white lab coats, these doctors discouraged mask wearing and falsely said there was already a cure in hydroxychloroquine, a drug used to treat rheumatoid arthritis and lupus.
Trump, who had been talking up the drug since March and claimed to be taking it himself as a preventive measure in May, retweeted clips of the event before Twitter removed them as misinformation about COVID-19. He defended the “very respected doctors” in a July 28 press conference.
When Olga Lucia Torres, a lecturer at Columbia University, heard Trump touting the drug in March, she knew it didn’t bode well for her own prescription. Sure enough, the misinformation led to a run on hydroxychloroquine, creating a shortage for Americans like her who needed the drug for chronic conditions.
A lupus patient, she went to her local pharmacy to request a 90-day supply of the medication. But she was told they were only granting partial refills. It took her three weeks to get her medication through the mail.
“What about all the people who were silenced and just lost access to their staple medication because people ran to their doctors and begged to take it?” Torres said.No sickbed conversion
On Sept. 26, Trump hosted a Rose Garden ceremony to announce his nominee to replace the late Ruth Bader Ginsburg on the U.S. Supreme Court. More than 150 people attended the event introducing Amy Coney Barrett. Few wore masks, and the chairs weren’t spaced out.
In the weeks after, more than two dozen people close to Trump and the White House became infected with COVID-19. Early Oct. 2, Trump announced his positive test.
Those hoping the experience and Trump’s successful treatment at Walter Reed might inform his view of the coronavirus were disappointed.
Trump snapped back into minimizing the threat during his first moments back at the White House. He yanked off his mask and recorded a video.
“Don’t let it dominate you. Don’t be afraid of it,” he said, describing experimental and out-of-reach therapies he received. “You’re going to beat it.”
In Trump’s telling, his hospitalization was not the product of poor judgment about large gatherings like the Rose Garden event, but the consequence of leading with bravery. Plus, now, he claimed, he was immune from the virus.
On the morning after he returned from Walter Reed, Trump tweeted a seasonal flu death count of 100,000 lives and added that COVID-19 was “far less lethal” for most populations. More false claims at odds with data — the U.S. average for flu deaths over the past decade is 36,000, and experts said COVID-19 is more deadly for each age group over 30.
When Trump left the hospital, the U.S. death toll from COVID-19 was more than 200,000. Today it is more than 300,000. Meanwhile, this month the president has gone ahead with a series of indoor holiday parties.
The vaccine war
The vaccine disinformation campaign started in the spring but is still underway.
In April, blogs and social media users falsely claimed Democrats and powerful figures like Bill Gates wanted to use microchips to track which Americans had been vaccinated for the coronavirus. Now, false claims are taking aim at vaccines developed by Pfizer and BioNTech and other companies.
A blogger claimed Pfizer’s head of research said the coronavirus vaccine could cause female infertility. That’s false.
An alternative health website wrote that the vaccine could cause an array of life-threatening side effects, and that the FDA knew about it. The list included all possible — not confirmed— side effects.
Social media users speculated that the federal government would force Americans to receive the vaccine. Neither Trump nor President-elect Joe Biden has advocated for that, and the federal government doesn’t have the power to mandate vaccines, anyway.
As is often the case with disinformation, the strategy is to deliver it with a charade of certainty.
“People are anxious and scared right now,” said Dr. Seema Yasmin, director of research and education programs at the Stanford Health Communication Initiative. “They’re looking for a whole picture.”
Most polls have shown far from universal acceptance of vaccines, with only 50% to 70% of respondents willing to take the vaccine. Black and Hispanic Americans are even less likely to take it so far.
Meanwhile, the future course of the coronavirus in the U.S. depends on whether Americans take public health guidance to heart. The Institute for Health Metrics and Evaluation projected that, without mask mandates or a rapid vaccine rollout, the death toll could rise to more than 500,000 by April 2021.
“How can we come to terms with all that when people are living in separate informational realities?” Starbird said.
On Monday, at Long Island Jewish Medical Center in New York City, critical care nurse Sandra Lindsay rolled up her sleeve andbecame the first American to receive Pfizer and BioNTech’s newly approved COVID vaccine, opening a new front in the nation’s battle with the coronavirus pandemic.
By Friday, nearly 50,000 doses of the vaccine had been administered nationwide, with millions more expected before year’s end. Amid a complex rollout that has already raised questions about the timely distribution of doses, the Food and Drug Administration (FDA) confirmed that it was safe to use every last drop of the Pfizer vaccine, including the excess amount used to fill the five-dose vials of the precious medicine—meaning many vials may have enough to immunize a sixth person.
Based on Thursday’s recommendation from a key panel of experts, the FDA is expected to approve a similar vaccine from Moderna as soon as Friday evening, with doses of that vaccine beginning to be administered by next week. The Moderna vaccine comes in smaller packages with less-demanding storage requirements, making it suitable for a wider distribution across smaller settings and remote areas.
Pharmacy chains CVS and Walgreens were set to begin administering shots to nursing home residents in Ohio, Connecticut, and Florida on Friday, as part of an agreement with the US government to vaccinate staff and residents in 75,000 long-term care facilities nationwide.
In an interview this week, Secretary of Health and Human Services (HHS) Alex Azar said that the vaccine could be widely available to the general public as soon as late February or early March. While it’s surely tempting to fixate on every setback, second guess every decision about prioritization and distribution, and fret over every isolated report of an adverse vaccine reaction, it will be important in the coming weeks to keep the big picture in mind: we are on the way to beating back the coronavirus. The end is nigh.
Britain’s medicine regulator said anyone with a history of anaphylaxis to a medicine or food should not get the Pfizer-BioNTech COVID-19 vaccine, giving fuller guidance on an earlier allergy warning about the shot.
Starting with the elderly and frontline workers, Britain began mass vaccinating its population on Tuesday, part of a global drive that poses one of the biggest logistical challenges in peacetime history.
The Medicines and Healthcare Products Regulatory Agency (MHRA) said there had been two reports of anaphylaxis and one report of a possible allergic reaction since rollout began.
“Any person with a history of anaphylaxis to a vaccine, medicine or food should not receive the Pfizer BioNTech vaccine,” MHRA Chief Executive June Raine said in a statement.
“Most people will not get anaphylaxis and the benefits in protecting people against COVID-19 outweigh the risks… You can be completely confident that this vaccine has met the MHRA’s robust standards of safety, quality and effectiveness.”
Anaphylaxis is an overreaction of the body’s immune system, which the National Health Service describes as severe and sometimes life-threatening.
The fuller guidance, clarifying that the main risk was from anaphylaxis specifically, was issued after consulting experts on allergies. The MHRA had initially advised anyone with a history of a “significant allergic reaction” not to take the shot.
Pfizer and BioNTech said they were supporting the MHRA’s investigation.
Last week, Britain’s MHRA became the first in the world to approve the vaccine, developed by Germany’s BioNTech and Pfizer, while the U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) continue to assess the data.
A top U.S. official said on Wednesday that Americans with known severe allergic reactions may not be candidates for Pfizer’s COVID-19 vaccine until more was understood about what had happened.
Canada’s health ministry said it would look at the reported adverse reactions in Britain, but said adverse events were to be expected and would not necessarily change the risk/benefit of the shot, after the country approved the vaccine.
ALLERGIC REACTION
MHRA chief Raine told lawmakers such allergic reactions had not been a feature of the Pfizer’s clinical trials.
Pfizer has said people with a history of severe adverse allergic reactions to vaccines or the candidate’s ingredients were excluded from their late stage trials, which is reflected in the MHRA’s emergency approval protocol.
However, the allergic reactions may have been caused by a component of Pfizer’s vaccine called polyethylene glycol, or PEG, which helps stabilise the shot and is not in other types of vaccines.
Imperial College London’s Paul Turner, an expert in allergy and immunology, who has been advising the MHRA on their revised guidance, told Reuters: “As we’ve had more information through, the initial concern that maybe it affects everyone with allergies is not true.”
“The ingredients like PEG which we think might be responsible for the reactions are not related to things which can cause food allergy. Likewise, people with a known allergy to just one medicine should not be at risk,” Turner told Reuters.
The EMA said in an email that all quality, safety and efficacy data would be taken into account in assessing the vaccine, including data generated outside the EU.
In the United States, the FDA released documents on Tuesday in preparation for an advisory committee meeting on Thursday, saying the Pfizer vaccine’s efficacy and safety data met its expectations for authorization.
The briefing documents said 0.63% of people in the vaccine group and 0.51% in the placebo group reported possible allergic reactions in trials, which Peter Openshaw, professor of experimental medicine at Imperial College London, said was a very small number.
“The fact that we know so soon about these two allergic reactions and that the regulator has acted on this to issue precautionary advice shows that this monitoring system is working well,” he said.
However, Gregory Poland, a virologist and vaccine researcher with the Mayo Clinic in Rochester, Minnesota, said that the MHRA and NHS had overreacted initially.
“I would not have broadened to the degree they did,” he said.
“It’s reasonable to let the world know about this, and to be aware of it in terms of people who have had reactions like this to vaccines. I think to say medicines, foods or any other allergies is past the boundary of science.”
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the anti-vaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, director of the division of medical ethics at New York University School of Medicine.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups — from those representing home-based health workers and community health centers to patients with kidney disease — were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Offit, who sits on the FDA advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the U.S. and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Dr. Allison Kempe, a professor of pediatrics at the University of Colorado School of Medicine and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when and to whom next doses should be distributed, said Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” — a broad and ill-defined category — as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” said Caplan of NYU.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus or subway,” Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Limaye said.
“We’re all seeing this now,” said Kempe. “Even deniers are beginning to see what this illness can do.”
Trump administration officials deny there will be availability issues, but others say problems are possible in the second quarter.
Pfizer has told the Trump administration it cannot provide substantial additional doses of its coronavirus vaccine until late June or July because other countries have rushed to buy up most of its supply, according to multiple individuals familiar with the situation.
That means the U.S. government may not be able to ramp up as rapidly as it had expected from the 100 million doses of the Pfizer vaccine that it purchased earlier this year, raising questions about whether it can keep to its aggressive schedule to vaccinate most Americans by late spring or early summer.
Trump administration officials denied there would be availability issues in the second quarter, citing other vaccines in the pipeline — most immediately, Moderna’s, also expected to be approved in coming weeks. Both vaccines are two-dose regimens, so the 100 million doses purchased of each would cover 50 million people each.
“I’m not concerned about our ability to buy vaccines to offer to all of the American public,” Gen. Paul Ostrowski, who oversees logistics for Operation Warp Speed, the government’s initiative to expedite vaccine development, said in an interview Monday. “It’s clear that Pfizer made plans with other countries. Many have been announced. We understand those pieces.”
But several officials knowledgeable about the contracts said that supplies from other companies may be insufficient to fill the gap.
Last summer, Pfizer officials had urged Operation Warp Speed to purchase 200 million doses, or enough of the two-shot regimen for 100 million people, according to people knowledgeable about the issue who spoke on the condition of anonymity because they weren’t authorized to discuss the situation. But the Warp Speed officials declined, opting instead for 100 million doses, they said. The New York Times first reported that federal officials passed on the opportunity when Pfizer offered to sell more doses.
“Anyone who wanted to sell us … without an [FDA] approval, hundreds of millions of doses back in July and August, was just not going to get the government’s money,” said a senior administration official.
It was only last weekend, with a Food and Drug Administration clearance expected any day, that federal officials reached back out to the company asking to buy another 100 million doses. By then, Pfizer said it had committed the supply elsewhere and suggested elevating the conversation to “a high level discussion,” said a person familiar with the talks.
Pfizer said the company might be able to provide 50 million doses at the end of the second quarter, and another 50 million doses in the third quarter, the individuals said.
The government had a different type of contract with Pfizer than with other companies involved with Operation Warp Speed. Pfizer was the only company that did not take government money for research and development, which meant U.S. officials have had less insight into its decisions than it does with the other companies, said a senior administration official familiar with the matter who spoke on the condition of anonymity.
The contract between the government and Pfizer stipulated that if Pfizer’s vaccine was successful and received authorization from the FDA, the U.S. government would purchase 100 million doses at a set price.
Pfizer spokeswoman Amy Rose declined to confirm any information about the company’s discussions with the government, and said that beyond the first 100 million doses the U.S. has already secured, a separate agreement would have to be negotiated.
President Trump is expected to sign an executive order Tuesday that would prioritize vaccinating Americans before providing doses to other countries, according to a senior administration official who requested anonymity because he was not authorized to speak about the plans. Fox News first reported the executive order. It is not clear whether the order is related to the Pfizer supply issue, or whether the president can prevent an American company from fulfilling lawful contracts with other countries.
“The executive order reaffirms to the American people that we are going to put America first,” said a senior administration official, who spoke on the condition of anonymity because he was not authorized to discuss the issue publicly.
The order will be announced as part of a White House “vaccine summit” designed to highlight the administration’s accomplishments on vaccines.
The vaccine by Pfizer and German biotech firm BioNTech is expected to receive emergency authorization from the FDA in the next several days, and Moderna is lined up for likely clearance shortly after that. Shipments of the vaccines will begin within 24 hours of the approvals, federal officials have said.
Warp Speed officials hope that other companies with promising vaccine candidates will supplement the supply in the near future, but some are still conducting late-stage clinical trials, while others haven’t begun them.
That means it could be several weeks to months before they are ready to apply to the FDA for clearance. One of the companies, AztraZeneca recently reported encouraging vaccine data, but experts raised questions about it and what it meant about the efficacy of the vaccine.
Moncef Slaoui, chief science adviser to Warp Speed, said in an interview Monday that the U.S. government strategy was to spread its risk widely over many different types of vaccines from different manufacturers. He declined to comment on negotiations with any company, but said he did not believe there would be any kind of vaccine “cliff,” where the available doses would fall off sharply.
Slaoui said that Johnson & Johnson was likely to report trial results in early January and be ready to ship doses in February, if its vaccine is authorized. He predicted that AstraZeneca’s trial would report results in late January or early February and potentially begin providing doses later that month.
“We could have all of them,” Slaoui said. “And for this reason, we feel confident we could cover the needs without a specific cliff … We have planned things in such a way as we would indeed avoid a cliff.”
The contract that Pfizer signed with the government in July was to deliver 100 million vaccine doses, and contained an option to contract to buy an additional 500 million doses.
“Pfizer shall inform the Government of appropriate lead times based on purchase of raw materials, capacity reservation and other factors, and Pfizer and the Government shall mutually agree on an appropriate estimated delivery schedule,” the contract states.
“Recognizing the urgency of the need, our manufacturing teams have been working around-the-clock so we can bring the vaccine to the world as quickly, efficiently and equitably as possible,” Rose said.
Additional doses would be “subject to a separate and mutually acceptable agreement” she said.
No agreements with Moderna beyond its initial contract for 100 million have been announced, but the U.S. has the option to purchase 400 million additional doses. Moderna is expected to deliver 20 million doses by year’s end and another tranche in the first quarter of 2021.
President-elect Joe Biden’s front-runner for secretary of Health and Human Services is New Mexico Governor Michelle Lujan Grisham, and he may announce several of his administration’s health leaders as soon as next week, according to people familiar with the matter.
The position of HHS secretary is down to two possibilities, the people said, between Lujan Grisham and former Surgeon General Vivek Murthy, a co-chair of the coronavirus advisory board Biden appointed shortly after he was elected.
Biden’s health team will assume office with the U.S. still suffering from the pandemic, as virus cases and hospitalizations soared over the past month. His health secretary is expected to have input on filling other top health posts, such as FDA commissioner and the administrator of the Centers for Medicare and Medicaid Services, the people said, so those appointments may not be announced until later.
The Health and Human Services secretary will have the tough task of rebuilding Obamacare, which Biden has promised to expand. That will be a difficult undertaking with a Republican-led Senate.
Murthy or Jeff Zients, who led the Obama administration effort to repair healthcare.gov, the faulty Obamacare website, may be named to a leadership role on the pandemic, according to the people familiar with the matter — a “Covid-19 czar.”
Mandy Cohen, the North Carolina state health secretary, is a favorite for CMS, the people said. Biden’s choices to lead the Food and Drug Administration appear narrowed down to David Kessler, a former commissioner of the agency who is another co-chair of his coronavirus advisory board, and Joshua Sharfstein, a former FDA official who is a vice dean at Johns Hopkins University’s Bloomberg School of Public Health.
Biden announced his economic team on Tuesday, a group led by Treasury Secretary-designate Janet Yellen whose top priority will be restoring jobs eliminated by the pandemic. An announcement on some of his health team could come as soon as Monday, the people said.
The people familiar with the matter asked not to be identified because talks are still ongoing and no final decision has been made. It’s not clear how many people will be announced at once, or which positions would later be filled by the health secretary once the Biden administration is in place.
Biden’s transition team did not immediately respond to a request for comment.
The U.S. recorded 158,000 new coronavirus infections on Monday and a record 205,000 cases three days earlier. Biden will take office as distribution of coronavirus vaccines ramps up, and he has warned that any delay in the transition to his administration could slow or complicate that endeavor.
Lujan Grisham is seen as having an easier path to confirmation than Murthy, who has spoken out against gun violence as a public health threat and may draw strong opposition from Senate Republicans as a result, the people familiar with the matter said.
If he isn’t nominated to lead HHS, Murthy is under consideration as Covid-19 czar or another role, including a second stint as surgeon general, the people said. Murthy talks to Biden almost every day as co-chair of his advisory board and is seen as having influential supporters.
Murthy and Zients have also represented Biden’s transition team on calls with current HHS officials, two of the people said.
Biden’s team is still discussing what the White House coronavirus task force and Operation Warp Speed — the Trump administration’s effort to fast-track vaccines — will look like under the new administration.
If Biden announces his health team next week, he may be just days ahead of the first emergency FDA approval of a coronavirus vaccine. President Donald Trump is planning a vaccine summit next week at the White House, while an FDA advisory panel is scheduled to meet on Dec. 10 to discuss the shots.
AstraZeneca on Monday became the third pharmaceutical company to announce remarkable results from late-stage trials of a coronavirus vaccine, saying that its candidate, developed by Oxford University, is up to 90 percent effective.
This is the third straight week to begin with buoyant scientific news that suggests, even as coronavirus cases surge to devastating levels in many countries, an end to the pandemic is in sight.
Pfizer and its German partner BioNTech and Moderna have each reported vaccines that are 95 percent effective in clinical trials. A direct comparison to the Oxford-AstraZeneca vaccine is complicated, due to the trial design, but the vaccine may be a more realistic option for much of the world, as it is likely to be cheaper and does not need to be stored at subzero temperatures.
Peter Piot, director of the London School of Hygiene & Tropical Medicine, who was instrumental in the battle against AIDS, said the positive results from three vaccine candidates cannot be overestimated.
“2020 will be remembered for the many lives lost from covid-19, lockdowns and the U.S. election. Science should now be added to this list,” said Piot, adding, “the only way to stop covid-19 in its tracks is having multiple effective and safe vaccines that can be deployed all around the world and in vast quantities.”
“I’m totally delighted,” said Hildegund C.J. Ertl, a vaccine expert at the Wistar Institute in Philadelphia. Adding to the results from Pfizer and Moderna, “what it tells me is this virus can be beaten quite easily: 90 to 95 percent efficacy is something we’d dream about for influenza virus, and we’d never get it.”
The Oxford-AstraZeneca team said in a video conference with journalists that its candidate offered 90 percent protection against the virus when a subject received a half-dose, followed with a full dose one month later. Efficacy was lower — 62 percent — when subjects received two full doses a month apart. The interim results, therefore, averaged to 70 percent efficacy.
Andrew Pollard, chief investigator of the Oxford trial, said the findings showed the vaccine would save many lives.
“Excitingly, we’ve found that one of our dosing regimens may be around 90 percent effective, and if this dosing regimen is used, more people could be vaccinated with planned vaccine supply,” he said.
Britain has preordered 100 million doses — which at a dose and a half per person would cover most of its population. The United States has ordered 300 million.
The results have yet to be peer-reviewed or published, and will be scrutinized by regulators. Many questions remain, including whether the vaccine can reduce transmission of the virus by people without symptoms, which would have repercussions for how soon people could stop wearing masks. It is also unclear how long the immunity from the vaccine lasts — a crucial question.
Sarah Gilbert, a lead Oxford researcher, cautioned that the dose-and-a-half regimen would have to be more closely studied to be fully understood. But she said the first half-dose might be priming a person’s immune system just enough, and that the second booster then encourages the body to produce a robust defense against sickness and infection.
AstraZeneca and Oxford have been conducting Phase 3 clinical trials worldwide, with the most recent data coming from an interim analysis based on 131 coronavirus infections in Britain and Brazil among 10,000 volunteers, with half getting the vaccine and half getting a placebo.
The company said it would present the results to Britain’s health-care products regulators immediately and would seek approval to fine-tune its clinical trials in the United States, to further assess the half-dose shot followed by a booster.
Because the vaccine is already in production, if approved, the first 4 million doses could be ready in December, and 40 million could be delivered in the first quarter of 2021, company executives said. By the spring, the company and its global partners in India, Brazil, Russia and the United States could be cranking out 100 million to 200 million doses a month.
British Health Secretary Matt Hancock said “should all that go well, the bulk of the rollout will be in the new year.”
In a statement to Parliament, Prime Minister Boris Johnson said that vaccines were “edging ever closer to liberating us from the virus, demonstrating emphatically that this is not a pandemic without end. We can take great heart from today’s news, which has the makings of a wonderful British scientific achievement.”
World markets have rallied on optimistic vaccine news, though shares in AstraZeneca were down Monday on the London stock exchange.
No participants who received the vaccine developed severe cases or required hospitalization, AstraZeneca said Monday. The drugmaker also said that no “serious safety events” were reported in connection with the vaccine, which was typically “well tolerated” by participants regardless of their dosing levels or ages.
The vaccine uses a harmless cold virus that typically infects chimpanzees to deliver to the body’s cells the genetic code of the spike protein that dots the outside of the coronavirus. That teaches the body’s immune system to recognize and block the real virus.
Although the reason the regimen with an initial half-dose worked better remains to be teased out, Ertl said that it could be related to the fact that the body’s immune system can develop a defense system to block the harmless virus that’s used to deliver the spike protein’s code. Giving a smaller initial dose may lessen those defenses, and make the vaccine more effective.
Several other vaccines in late-stage development use a similar technology, harnessing a harmless virus to deliver a payload that will teach the immune system how to fight off the real thing — including the Johnson & Johnson vaccine, the Russian vaccine being developed by the Gamaleya Research Institute and the vaccine made by CanSino Biologics in China.
While the results released by AstraZeneca indicate somewhat lower efficacy than Pfizer and Moderna, the vaccine can be stored and transported at normal refrigerated conditions for up to six months. That could make it significantly easier to roll out than Pfizer’s vaccine, which has to be stored at minus-70 degrees Celsius, or Moderna’s, which is stable in refrigerated conditions for only 30 days and must be frozen at minus-20 degrees Celsius after that.
The Oxford-AstraZeneca vaccine was first developed in a small laboratory running on a shoestring budget by Gilbert at Oxford and her team. The university kicked in 1 million pounds ($1.3 million) and then sought a manufacturing partner, before settling on AstraZeneca.
“We wanted to ensure there wouldn’t be any profiteering off the pandemic,” said Louise Richardson, the university’s vice chancellor, so that their vaccine would be widely distributed “and wouldn’t just be for the wealthy and the first world.”
The scientists said that although it appeared to be a race, or a competition, among the front-running vaccine developers, no one company could produce by itself the millions of doses needed to end the pandemic.
“We don’t have enough supply for the whole planet,” Pollard said, adding that the important message is that today there are at least three highly effective, safe vaccines, that also appear to work well among the elderly, and that they are produced using different technologies, ensuring the quickest route to manufacture the billions of doses that will be necessary.
Pollard said it is “unclear why” the different vaccines were producing different results, and he said he and the scientific community awaited full data sets from all the clinical trials to fully understand what is going on. He said different studies were also using different end points to describe efficacy.
“At this moment we can’t fully explain the differences,” Pollard said. “It’s critical to understand what everyone is measuring.”