A new COVID calamity is hammering China, with a surge in infections prompting a return of lockdowns, including in some manufacturing areas that supply the West.
China reported a record number of infections this week, amid lockdowns and mass testing that are fueling unrest and darkening the country’s economic outlook. Schools in Beijing returned to online teaching.
Why it matters: In addition to the human misery for the world’s most populous country, the effects will be felt around the globe, Axios China author Bethany Allen-Ebrahimian reports from Taipei.
Supply chains are likely to be disrupted, causing prices to rise in an already rocky global economy.
Rare protests broke out today in China’s far western Xinjiang region. Crowds shouted at hazmat-suited guards after a deadly fire triggered anger by prolonged COVID lockdowns, Reuters reports.
“End the lockdown!” shouted protesters in the Xinjiang capital Urumqi, where an apartment fire killed 10.
What’s happening: The moment of truth for China’s zero-COVID policy has finally come.
Either party leaders will need to plunge much of the country into draconian lockdowns, as we saw at the beginning of the pandemic — or they’ll decide it’s time to learn to live with COVID.
Reality check: China’s doctors have warned Xi Jinping that the healthcare system isn’t prepared for the huge outbreak likely to follow the easing of strict anti-COVID measures, the Financial Times reports.
Chinese-made vaccines, which don’t use the mRNA technology employed by many produced by the West, aren’t as effective compared to those made in the U.S. And China has worrisomely low vaccination rates among older people.
But the number of cases in China is actually still very low for anywhere but China.
The big picture: “Zero COVID” restrictions have damaged the economy and undermined people’s trust in government.
That’s a stark about-face from the height of the pandemic. Then, many Chinese people felt the tight central control had protected them better than any other governance model in the world.
But it’s that very model that has plunged China into its current predicament. Xi tied his reputation, and the party’s legitimacy, to the success of “zero COVID.”
Between the lines: Chinese leaders made a huge, politically motivated mistake. They resisted the import of Western-made mRNA vaccines (including Pfizer and Moderna) for its citizens. These vaccines were only recently made available to foreigners.
That’s likely because of Beijing’s big vaccine diplomacy push: Chinese officials touted their own vaccines as the best and safest.
It was politically unpalatable to admit “defeat,” and allow Chinese people to get more effective — but Western-made — jabs.
China is facing an increasingly precarious situation as new COVID cases soar and the population seems to be hitting a breaking point with the government’s stringent zero-tolerance policies.
Why it matters: The world’s most populous nation has massive vulnerabilities heading into this winter, starting with the fact the vast majority of its population has yet to be exposed to the virus and has little ‘natural immunity.’
China’s vaccines didn’t work well compared to those distributed in the West, and the government refused to approve foreign vaccines and doesn’t have a version to combat Omicron.
Vaccine uptake was particularly low among the elderly.
And now, public outrage over new COVID lockdown restrictions has fueled rare protests, Axios’ Herb Scribner writes, with residents demanding the government to lift restrictions quickly and some calling for President Xi Jinping’s resignation.
State of play: Overall, China’s number of reported COVID cases and COVID deaths are far lower than other nations, but there have been recent reported spikes in overall numbers of cases and some new deaths.
It came after the Chinese government announced some easing of its zero-COVID policy, such as reducing mass testing and quarantine requirements, earlier this month.
Reality check: China’s doctors have warned that the health care system isn’t prepared for the huge outbreak likely to follow any easing of public health measures, Axios’ Bethany Allen-Ebrahimian writes.
That includes worries the nation doesn’t have enough ICU bed capacity to handle such outbreaks, according to the Financial Times.
Between the lines: Another concern is the potential evolution of a new, more dangerous variant if there’s a huge surge of infections, Christian Drosten, Germany’s most prominent virologist, told Bloomberg.
“Xi Jinping knows very well that he can’t simply let the virus loose,” Drosten said. “The Chinese population first needs to be as well vaccinated as we are.”
Be smart: China’s officials are scrambling to address the vaccine problem.
For instance, they are launching more aggressive vaccine drives and limiting movement among at-risk groups, including the elderly, the Washington Post reports.
But they have yet to open up the availability of mRNA vaccines from Pfizer-BioNTech and Moderna, opting to focus on their own, per the Post.
The bottom line: China’s zero-COVID policy has kept cases in China relatively low compared to the rest of the world.
But even as the societal and economic consequences of shutdowns become apparent, it faces a very difficult path ahead in unwinding strict public health policies.
Most experts agree that updated bivalent Covid-19 boosters provide additional protection against serious illness and death among vulnerable populations—but evidence suggests that increased booster uptake may not prevent a “wave of Covid” infections this winter, Apoorva Mandavilli writes for the New York Times.
Can bivalent boosters prevent another surge of infections?
While the Biden administration’s plan to prevent another surge of Covid-19 infections relies on increasing Americans’ uptake of the updated booster doses of the Pfizer–BioNTech and Moderna vaccines, some experts doubt the strategy.
According to John Moore, a virologist at Weill Cornell Medicine, boosters provide additional protection to vulnerable populations—including older adults, immunocompromised individuals, and pregnant people—who should get boosted to prevent severe illness and death.
However, the benefit is not as clear for healthy, younger Americans who “are rarely at risk of severe illness or death from Covid, and at this point most have built immunity through multiple vaccine doses, infections or both,” Mandavilli writes.
“If you’re at medical risk, you should get boosted, or if you’re at psychological risk and worrying yourself to death, go and get boosted,” Moore said. “But don’t believe that will give you some kind of amazing protection against infection, and then go out and party like there’s no tomorrow.”
Separately, Peter Marks, FDA‘s top vaccine regulator, noted the limited data available data for the updated boosters.
“It’s true, we’re not sure how well these vaccines will do yet against preventing symptomatic disease,” he said, especially as the newer variants spread.
However, Marks added, “even modest improvements in vaccine response to the bivalent boosters could have important positive consequences on public health. Given the downside is pretty low here, I think the answer is we really advocate people going out and consider getting that booster.”
How much additional protection do updated shots provide?
While Pfizer-BioNTech and Moderna recently reported that their bivalent boosters produced antibody levels that were four to six times higher than the original vaccine, their results were based on BA.4 and BA.5 antibodies, instead of the more prevalent BQ.1 and BQ.1.1 variants.
According to Mandavilli, “[a] spate of preliminary research suggests that the updated boosters, introduced in September, are only marginally better than the original vaccines at protecting against the newer variants — if at all.”
These small studies have not been reviewed for publication in a journal—but they all came to similar conclusions.
“It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection,” said Dan Barouch, head of Beth Israel Deaconess‘ Center for Virology and Vaccine Research, who helped develop Johnson & Johnson‘s vaccine.
Notably, Barouch’s team recently discovered that BQ.1.1 is around seven times more resistant to the body’s immune defenses than BA.5, and 175 times more resistant than the original strain of the coronavirus. “It has the most striking immune escape, and it’s also growing the most rapidly,” he said. BQ.1 will likely follow a similar pattern.
“By now, most Americans have some degree of immunity to the coronavirus, and it does not surprise scientists that the variant that best evades the body’s immune response is likely to outrun its rivals,” Mandavilli writes.
The new vaccine increases antibodies, but the fact it is bivalent may not be significant. In August, a study by Australian immunologists suggested that any kind of booster would offer extra protection. In addition, the study noted that a variant-specific booster would likely not be more effective than the original vaccine.
“The bulk of the benefit is from the provision of a booster dose, irrespective of whether it is a monovalent or bivalent vaccine,” according to the World Health Organization.
Florian Krammer, an immunologist at the Icahn School of Medicine at Mount Sinai, noted that despite recent research, which evaluated immune response soon after vaccination, immune response may improve over time.
“We will see with larger studies and studies at a later time point if there is a good or a significant benefit, but I think it’s certainly not worse,” he added. “I don’t see much risk when you get the vaccine, so you might as well get the benefit.”
“What we need to do right now to get us through the next few months when I think we are in yet another wave of incipient wave of Covid,” Marks added. “And then we need to look forward, and lean into how we’re going to do things differently moving forward.”
Will we see an increase in vaccine uptake?
Currently, FDA allows the booster dose at least two months after a Covid-19 infection or previous does. However, some studies suggest boosting too early could have negative consequences. “Lengthening the interval between boosts to five or six months may be more effective, giving the immune system more time to refine its response,” Mandavilli writes.
Still, “adding yet another shot to the regimen seems unlikely to motivate Americans to opt for the immunization,” no matter the schedule, she adds.
“Each new booster we roll out is going to have a lower and lower uptake, and we’re already pretty close to the floor,” said Gretchen Chapman, an expert in health behavior at Carnegie Mellon University.
Ultimately, “[w]e should not spend a lot of political capital trying to get people to get this bivalent booster, because the benefits are limited,” Chapman added. “It’s more important to get folks who never got the initial vaccine series vaccinated than to get people like me to get their fifth shot.”
The Department of Health and Human Services (HHS) appears set to extend the federal COVID PHE past its current expiration date of January 11, 2023, as HHS had promised to give stakeholders at least 60 days’ notice before ending it, and that deadline came and went on November 11th. Days later the Senate voted to end the PHE, a bill which Biden has promised to veto should it reach his desk. Measures set to expire with the PHE, or on a several month delay after it ends, include Medicare telehealth flexibilities, continuous enrollment guarantees in Medicaid, and boosted payments to hospitals treating COVID patients.
The Gist: Despite growing calls to end the PHE declaration, and even as White House COVID coordinator Dr. Ashish Jha has said another severe COVID surge this winter is unlikely, the White House is likely trying to buy time to resolve the complicated issues tied to the PHE, some of which must be dealt with legislatively.
And with a divided Congress ahead, it remains to be seen how these issues, especially Medicare telehealth flexibilities—a topic of bipartisan agreement—are sorted out. Meanwhile the continuation of the PHE prevents states from beginning Medicaid re-determinations, allowing millions of Americans to avoid being disenrolled.
Even as new omicron strains take over, Covid is no longer driving a majority of patients into the hospital. Still, doctors worry the virus could re-emerge as immunity wanes.
As the flu and RSV (respiratory syncytial virus) have spread rapidly this fall — inundating and overwhelming hospitals and their staff across the country — Covid has not.
In fact, Covid-related deaths and hospitalizations have fallen in recent months,despite the emergence of new omicron subvariants that evade immunity from previous infections and vaccination.
According to NBC News data, Covid deaths have fallen consistently since Aug. 31, when the seven-day average of daily Covid deaths was at 571. A month later, on Sept. 30, the number fell to 475. By Halloween, 365 were dying per day, on average, from Covid.
As of Nov. 14, the number had fallen to 316.
This week, the Centers for Disease Control and Prevention is expected to release new data on Covid-related mortality, finding that death rates began to decline in March 2022.
The overall hopeful sign of declining deaths could indicate yet another new Covid phase, doctors suggest. Fewer people sick enough to be hospitalized with Covid means that fewer people are dying of the illness.
The average number of Covid hospitalizations per day has decreased by 27.9% since Aug. 28, according to NBC News data.
Even better, Covid, it seems, is no longer sending a majority of patients into intensive care units.
“There has not been an increase in patients admitted to the hospital specific for Covid-related disease,” said Dr. Hugh Cassiere, director of critical care services at Sandra Atlas Bass Heart Hospital at North Shore University Hospital, part of Northwell Health in New York City.
Patients in his ICU with Covid were admitted with unrelated medical issues, and were subsequently found to be Covid-positive, Cassiere said.
“Not to say that it’s gone, but Covid has become a coincidental disease,” he said.
Dr. Vin Gupta, a pulmonologist and an affiliate faculty member at the University of Washington in Seattle, attributes the decline in deaths and severe Covid cases to a level of “baked-in immunity,” including vaccination, prior infection or a combination of the two.
While Covid-related hospitalizations are not currently increasing, Gupta warns that they could during the winter as immunity, especially from previous infection, diminishes.
“If you had Covid, say six to four months ago, you’re going to have less protection against hospitalization than if you were vaccinated,” Gupta said. “The duration and the robustness of protection wanes a lot more quickly if all you rely on is natural immunity.”
With that in mind, data from the Institute for Health Metrics and Evaluation, a research center within the University of Washington, suggest that Covid hospitalizations and deaths could tick up again in “mid-January at the earliest,” said Gupta, a medical analyst for NBC News and MSNBC.
Despite the encouraging decline in Covid deaths, another school of thought suggests that Covid has simply morphed into a new kind of fatal illness.
“Before everyone was vaccinated or had been infected, 80 or 90% of Covid looked exactly same. They had terrible pneumonia. They were in the ICU on respiratory support,” said Dr. Jeremy Faust, an emergency medicine physician at Brigham and Women’s Hospital and an instructor at Harvard Medical School in Boston.
Now, he said, “Covid deaths don’t all look the same.” While “baked-in immunity” may keep the most severe cases at a minimum, it is clear that Covid can wreak havoc on the body long after the infection has cleared.
“Somebody could have Covid and have a heart attack, and the primary cause of death is listed as a heart attack because that’s what really brought them to the hospital,” Faust said.
But, he added, “we’ll never know to what degree Covid triggered that heart attack.”
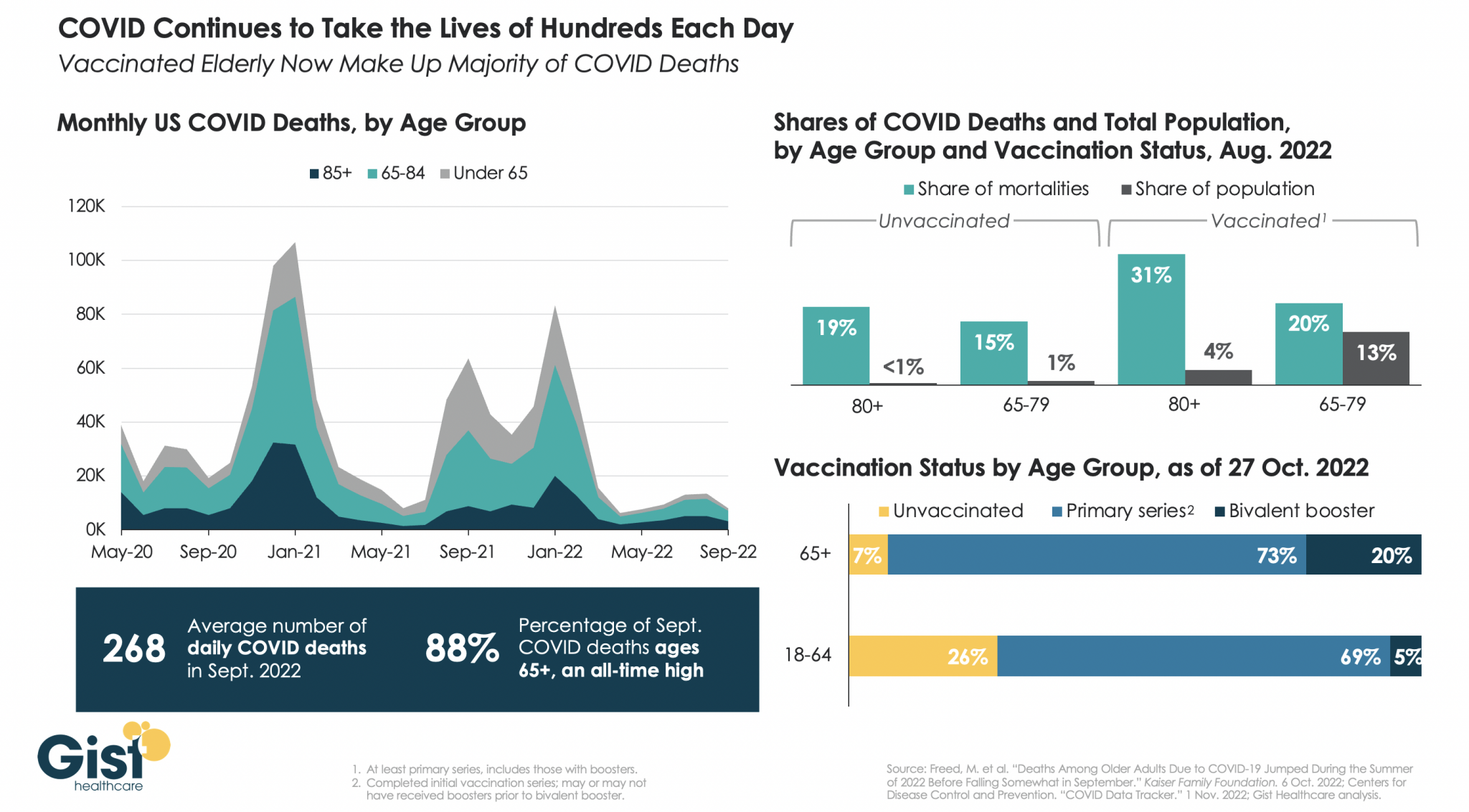
While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
Respiratory syncytial virus, more commonly known as RSV, sends thousands of children to the hospital every year in the U.S. But during September and October 2022, health professionals across the country have watched an unprecedented spike in the number of cases of this usually mild, but occasionally dangerous, respiratory infection in children.Jennifer Girotto is a pharmacist who studies pediatric infectious diseases. She explains how RSV infects the human body, who is most at risk and what might be causing this year’s outbreak to be worse than normal.
1. What is respiratory syncytial virus?
RSV is a common, RNA respiratory virus that affects about 2 million children under 5 years old annually nationwide. Researchers think that most children have been infected by age 2. Like the flu, in most areas of the U.S., RSV usually circulates from November through March and then mostly disappears during the summer months, with only sporadic cases being seen.
For most people, especially those who have had an RSV infection in the past, the virus only causes mild symptoms like cough, runny nose and fever, with instances of wheezing and decreased appetite more common in young children.
But young infants, especially those under 6 months old, born prematurely or with congenital heart, lung or other health issues are at increased risk for more severe symptoms. The U.S. Centers for Disease Control and Prevention estimates that 1% to 2% of infants younger than 6 months who get infected with RSV require hospitalization. In an average year, around 250 children die from the disease.
The main reason RSV sends babies and young children to the hospital is because the virus infects and kills surface cells within small sacs of the lungs. The body responds by increasing the production of mucus and fluid in these areas. But the extra mucus can plug up and obstruct these parts of the lung and make it so that an infant doesn’t get enough oxygen.
A second common cause for hospitalization due to RSV is pneumonia, where a person’s lungs fill up with fluid. The pneumonia can either be triggered by the virus itself or by a secondary, bacterial infection. Finally, some infants get so sick that they struggle to eat and are unable to take in sufficient nutrients, eventually landing them in the hospital.
Health officials aren’t yet sure why the outbreak is so bad this year, but the COVID-19 pandemic may have something to do with it. Some research has shown that seasonality of RSV has shifted. In 2021, RSV infections started much earlier than normal, and over the summer of 2022, they never quite went away. One theory as to why RSV season is starting earlier and hitting harder is that, due to social distancing measures since 2020, an unusually high number of infants and children are experiencing their first exposures and infections at once.
5. How can you protect against catching RSV?
Like colds and the flu, RSV infections spread when people touch dirty surfaces or from respiratory droplets, when an infected person coughs or sneezes.
If someone is sick with symptoms that look like a cold, it may be best to avoid close contact until they feel better, especially if you have young children or high-risk people around.
COVID-19 hospitalizations increased slightly this week after nearly two months of decline, while omicron subvariants BQ.1 and BQ.1.1 — dubbed ‘escape variants’ for their immune evasiveness — continued to gain prevalence nationwide, according to the CDC’s COVID-19 data tracker weekly review published Oct. 28.
Ten findings:
Hospitalizations
1. The seven-day hospitalization average for Oct. 19-25 was 3,249, a 1 percent increase from the previous week’s average. New hospital admissions had been falling since early August, CDC data shows.
Cases
2. As of Oct. 26, the nation’s seven-day case average was 37,683, a 25.1 percent decrease from the previous week’s average. This marks the 14th week of decline and the lowest daily case rate seen since late April, CDC data shows.
Variants
3. Based on projections for the week ending Oct. 29, the CDC estimates that BQ.1 accounts for 14 percent of cases, while BQ.1.1 accounts for 13.1 percent.
4. BA. 5 remains the nation’s dominant strain, accounting for 49.6 percent of infections. BF.7, another omicron subvariant experts are closely monitoring, makes up 7.5 percent of cases. Other omicron subvariants make up the rest.
Community levels
5. As of Oct. 27, 2.3 percent of counties, districts or territories had high COVID-19 community levels, 21.9 percent had medium community levels and 75.8 percent had low community levels.
Deaths
6. The current seven-day death average is 373, down 13.7 percent from the previous week’s average. Some historical deaths have been excluded from these counts, the CDC said.
Vaccinations
7. As of Oct. 26, about 266 million people — 80.1 percent of the U.S. population — have received at least one dose of the COVID-19 vaccine, and more than 226.9 million people, or 68.4 percent of the population, have received both doses.
8. About 111.8 million people have received a booster dose, and more than 22.9 million people have received an updated omicron booster. However, 49.3 percent of people eligible for a booster dose have not yet gotten one, the CDC said.
Wastewater surveillance
9. About 34 percent of the U.S. is reporting moderate to high virus levels in wastewater. Of these surveillance sites, 10 percent are seeing some of the highest levels since Dec. 1, 2021.
10. About 50 percent of sites are reporting an increase in virus levels, and 44 percent of sites are seeing a decrease.
Early into flu season, nationwide flu activity is ten times higher than at the same point last year. Meanwhile, cases of respiratory syncytial virus (RSV), a virus most severe in young children and the elderly, have tripled in the past two months, with some children’s hospitals reporting “unprecedented” admissions for the virus. And most experts expect at least some winter COVID surge, possibly involving several different variants. The combined threat of these viruses circulating together has been labeled a potential “tripledemic.”
The Gist: Across the past two winters, the widespread adoption of COVID prevention measures, including masking and social distancing, kept the spread of other viruses at bay. But with return to normal life for most Americans, other viruses have returned to circulation—and with a vengeance, as population immunity toward flu and RSV has weakened.
While it’s hard to predict when and where local surges will occur, hospitals struggling with staffing shortages may be forced to hire more contract labor to care for an influx of patients—making this a potentially challenging winter for already stretched facilities.
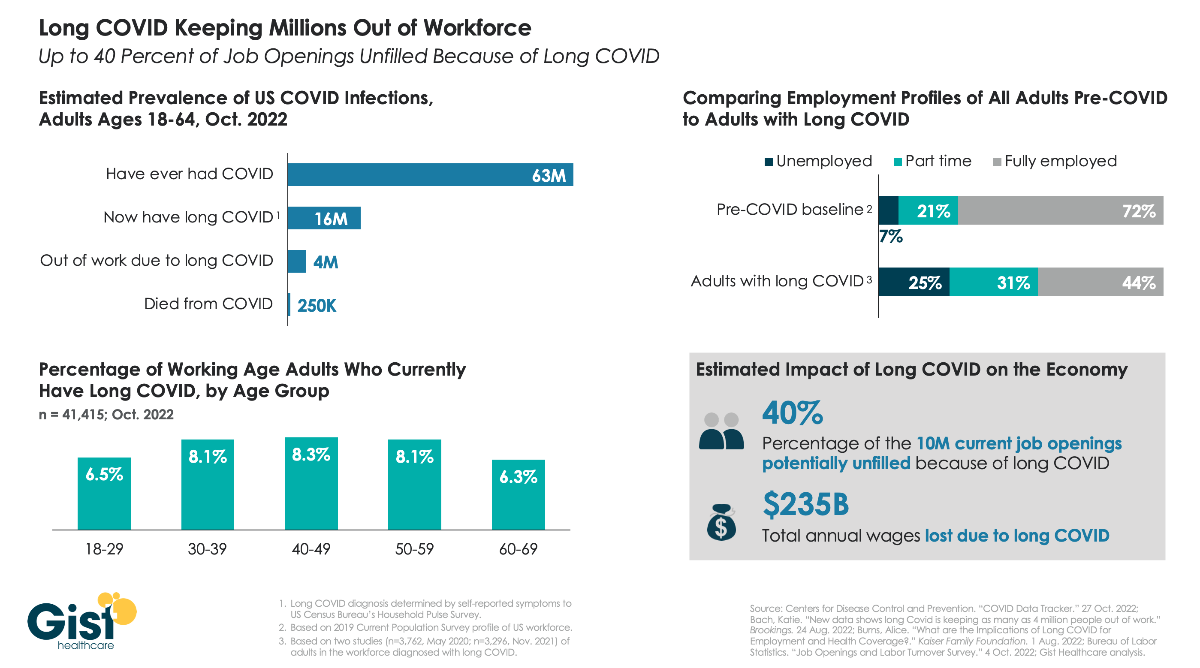
As the nation continues to grapple with the fallout from COVID, one of the greatest unknowns is “long COVID”, the broad range of health problems experienced by a significant number of individuals after contracting the virus. The Centers for Disease Control and Prevention defines long COVID as any post-COVID condition lasting three months or longer.
In the graphic above, we aim to quantify the prevalence of long COVID and its ongoing impact on the US workforce. While estimates for thesenumbers vary, data compiled by Brookings show that COVID infections in roughly one in four working age adults have resulted in long COVID, and up to one in four individuals with long COVID are unable to work due to their lingering health problems. Long COVID is also more prevalent in middle-aged adults, who are often at the peak of their working years. Dealing with symptoms like chronic fatigue and brain fog, long COVID patients are more likely to be unemployed or working reduced hours, compared to a pre-COVID baseline of the general adult population.
While it’s difficult to assess the precise impact on the nation’s current labor shortage, the estimate that 4M working age adults are no longer working because of long COVID equals about 40 percent of the 10M total job openings in August of this year, undoubtedly exacerbating ongoing economic challenges.









_(33114415716).jpg#/media/File:Human_Respiratory_Syncytial_Virus_(RSV)_(33114415716).jpg){kind=link}