Using data from Kaufman Hall’s latest National Hospital Flash Report and publicly available investor reports for some of the nation’s largest health systems, the graphic below takes stock of the state of health system margins.
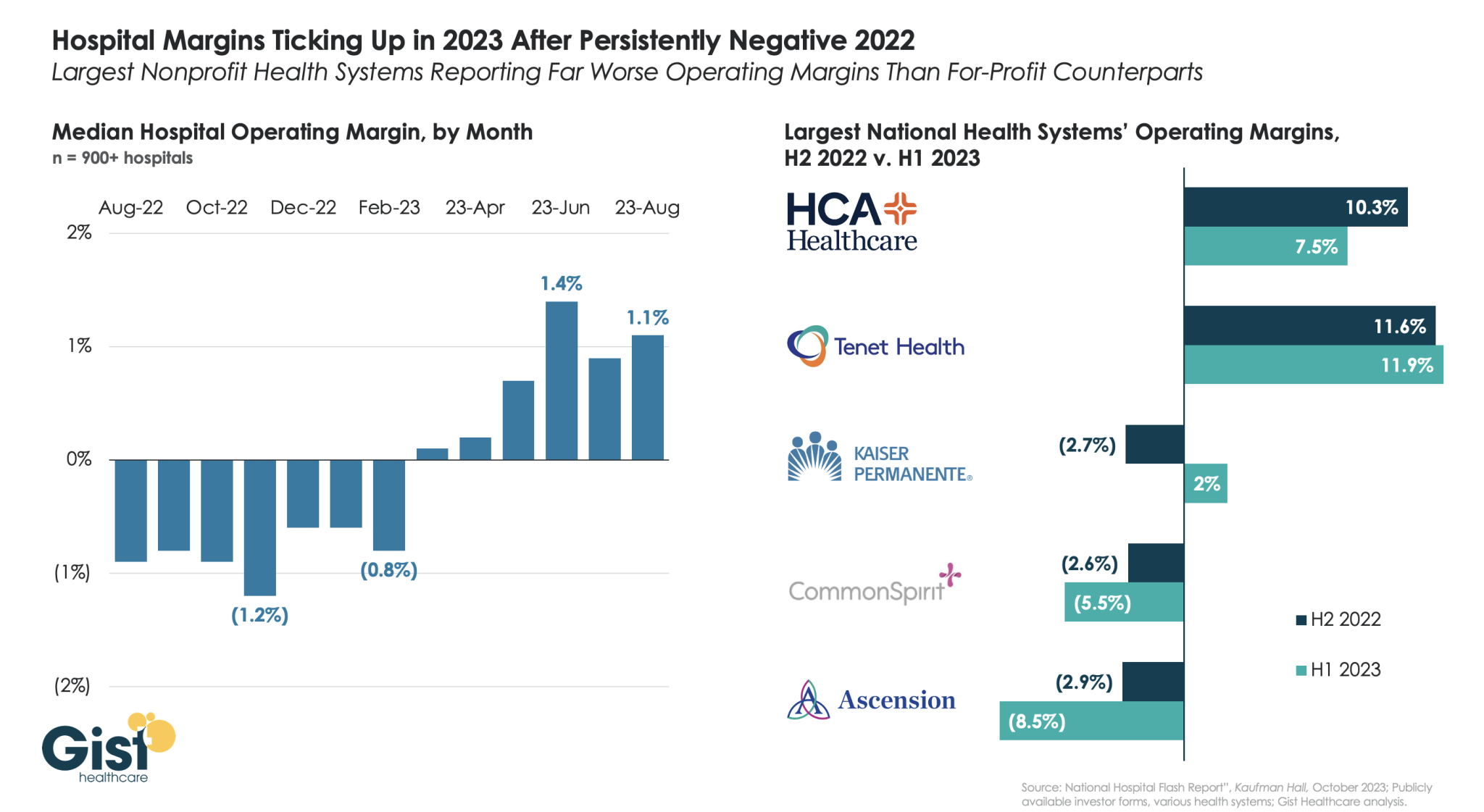
After the median hospital delivered negative operating margins for twelve-straight months, 2023 has made for a positive but slim year so far, with margins hovering around one percent. Amid this breakeven environment, fortunes have diverged between nonprofit and for-profit health systems.
The largest for-profit systems, HCA Healthcare and Tenet Healthcare, posted operating margins of around 10 percent between July 2022 and June 2023, while the three largest nonprofit systems, Kaiser Permanente, CommonSpirit Health, and Ascension, suffered net losses.
Although Kaiser Permanente’s margin bounced back in the first half of this year, CommonSpirit and Ascension’s margins continued to decline, more than doubling the operating losses of the prior six months.
One key to the recent success of the largest for-profit systems is their diversification away from inpatient care.
Case in point: almost half of Tenet’s profits in 2023 have come from its ambulatory division, driven by its United Surgical Partners International (USPI) ambulatory surgery center network, which has posted 40 percent margins over the past several quarters.
Nurses who work for staffing agencies are much more satisfied than their counterparts who serve hospitals, health systems, home healthcare providers and senior living facilities, according to an Oct. 18 report from MIT Sloan Management Review.
Researchers identified 200 of the largest healthcare employers in the U.S., and calculated how highly nurses rate the organization and senior leadership on Glassdoor from the beginning of COVID-19 through June 2023 (view their ranking here).
The five highest-ranked employers in the sample were staffing agencies, according to the report — and higher compensation only accounts for part of nurses’ satisfaction. Researchers analyzed the free text on Glassdoor to determine how positively nurses spoke about 200 topics, and found that nurses spoke more highly of staffing agencies on issues other than pay.
Overall, 75% of nurses’ comments about staffing agencies were positive, compared with 23% of nurses’ comments about health systems.
Staffing agencies have other healthcare employers beat in problem resolution, the researchers found. Seventy-three percent of nurses said staffing agencies resolved problems efficiently, compared to 31% of nurses employed by hospitals and health systems. The difference was even greater when it came to resolving problems effectively — 55% of nurses say staffing agencies do this, compared to 9% of nurses at hospitals and health systems.
Nurses also rated staffing agencies more highly on several measures related to honesty, according to the report. Three-quarters of nurses employed by staffing agencies spoke highly of their organizations’ speed in replying to inquiries; less than one-quarter of nurses employed by hospitals and health systems praised their organization on timely replies. Staffing agencies scored 41 percentage points higher on transparency, 36 points higher on trust and 46 points higher on honesty than their hospital and health system counterparts.
Although nurses employed by staffing agencies also ranked their compensation and work-related stress levels significantly better than nurses employed by hospitals and health systems, the latter took the lead in some metrics. Nurses prefer hospitals and health systems for health and retirement benefits, learning and development opportunities, and connection with colleagues: all “important aspects of organizational life,” according to the report.
“Healthcare systems can learn from staffing agencies, but they can also leverage their own distinctive advantages to attract and retain nurses,” the report says. “Healthcare systems should invest in their comparative advantages and emphasize them when communicating their value proposition to potential and current employees.”
Health systems are increasingly focused on their regional structures, reorganizing leadership to provide oversight most effectively. On Oct. 23, those changes hit the corner office.
Providence is phasing out the CEO role at two of its California hospitals, the Renton, Wash.-based system confirmed to Becker’s. One year ago, Providence’s Northern and Southern California regions came together to create a sole South Division. Now, a single chief executive — Garry Olney, DNP, RN — will oversee operations in the Northern California service area, replacing the CEOs of Napa-based Queen of the Valley Medical Center and Santa Rosa (Calif.) Memorial Hospital.
“This was part of a systemwide restructuring to streamline executive roles so we could preserve more resources for front-line caregivers and become nimbler and more responsive to the times,” the system said in a statement.
Providence isn’t alone in its desire to streamline leadership. Corewell Health East — part of Corewell Health, which has dual headquarters in Grand Rapids and Southfield, Mich. — made seven executive changes within the region, the system confirmed to Becker’s on Oct. 23. The senior vice president of medical group operations was let go, along with two hospital presidents. The region’s COO of acute and post-acute care, Nancy Susick, RN, will take over one hospital in addition to her current duties; the second hospital will be overseen in a dual capacity by Derk Pronger, who already helms another hospital in the region.
The word “streamline” was also used by Chicago-based CommonSpirit, which recently shared plans to lighten its regional load.
“We are also making further changes to streamline the organization, including the consolidation of our operating divisions into five regions from eight, clearly define our market-based focus and strategies and continue to refine our operating model,” CFO Dan Morissette said on an Oct. 12 investor call.
Regional revamps don’t always lead to cuts or “consolidation.” In some cases, they lead to the creation of new roles. Atlanta-based Emory Healthcare recently split its 10 hospitals into two divisions — one for regional hospitals, one for university hospitals — and tapped a president to helm each. Plus, Tampa (Fla.) General Hospital named eight new executives in a C-suite overhaul following the adoption of three Bravera Health hospitals into TGH North.
If the healthcare leaders plan to confront looming challenges, they need to be comfortable with “innovating and disrupting [themselves],” John Couris, president and CEO of Tampa General, told Becker’s.
“The way I would describe this is the last five years was all about foundational work,” Mr. Couris said. “The next five years and beyond is all about transformational work. So we’re shifting from the foundational activity to the transformational activity, and we need an organizational structure and a leadership team that reflects that journey. That’s why we made the changes.”
Hospitals and health systems are seeing some signs of stabilization in 2023 following an extremely difficult year in 2022. Workforce-related challenges persist, however, keeping costs high and contributing to issues with patient access to care. The percentage of respondents who report that they have run at less than full capacity at some time over the past year because of staffing shortages, for example, remains at 66%, unchanged from last year’s State of Healthcare Performance Improvement report. A solid majority of respondents (63%) are struggling to meet demand within their physician enterprise, with patient concerns or complaints about access to physician clinics increasing at approximately one-third (32%) of respondent organizations.
Most organizations are pursuing multiple strategies to recruit and retain staff. They recognize, however, that this is an issue that will take years to resolve—especially with respect to nursing staff—as an older generation of talent moves toward retirement and current educational pipelines fail to generate an adequate flow of new talent. One bright spot is utilization of contract labor, which is decreasing at almost two-thirds (60%) of respondent organizations.
Many of the organizations we interviewed have recovered from a year of negative or breakeven operating margins. But most foresee a slow climb back to the 3% to 4% operating margins that help ensure long-term sustainability, with adequate resources to make needed investments for the future. Difficulties with financial performance are reflected in the relatively high percentage of respondents (24%) who report that their organization has faced challenges with respect to debt covenants over the past year, and the even higher percentage (34%) who foresee challenges over the coming year. Interviews confirmed that some of these challenges were “near misses,” not an actual breach of covenants, but hitting key metrics such as days cash on hand and debt service coverage ratios remains a concern.
As in last year’s survey, an increased rate of claims denials has had the most significant impact on revenue cycle over the past year. Interviewees confirm that this is an issue across health plans, but it seems particularly acute in markets with a higher penetration of Medicare Advantage plans. A significant percentage of respondents also report a lower percentage of commercially insured patients (52%), an increase in bad debt and uncompensated care (50%), and a higher percentage of Medicaid patients (47%).
Supply chain issues are concentrated largely in distribution delays and raw product and sourcing availability. These issues are sometimes connected when difficulties sourcing raw materials result in distribution delays. The most common measures organizations are taking to mitigate these issues are defining approved vendor product substitutes (82%) and increasing inventory levels (57%). Also, as care delivery continues to migrate to outpatient settings, organizations are working to standardize supplies across their non-acute settings and align acute and non-acute ordering to the extent possible to secure volume discounts.
Survey Highlights
98% of respondents are pursuing one or more recruitment and retention strategies
90%have raised starting salaries or the minimum wage
73%report an increased rate of claims denials
71% are encountering distribution delays in their supply chain
70%are boarding patients in the emergency department or post-anesthesia care unit because of a lack of staffing or bed capacity
66% report that staffing shortages have required their organization to run at less than full capacity at some time over the past year
63% are struggling to meet demand for patient access to their physician enterprise
60% see decreasing utilization of contract labor at their organization
44%report that inpatient volumes remain below pre-pandemic levels
32% say that patients concerns or complaints about access to their physician enterprise are increasing
24%have encountered debt covenant challenges during the past 12 months
None of our respondents believe that their organization has fully optimized its use of the automation technologies in which it has already invested
The law, which was heavily backed by healthcare unions, is expected to affect approximately 469,000 healthcare workers and will be phased in over the next several years.
Dive Brief:
California Gov. Gavin Newsom on Friday signed a law raising the minimum wage for thousands of healthcare workers in the state from $15.50 an hour to $25 per hour.
State lawmakers argued in the law’s text that competitive wages are necessary to attract and retain healthcare workers who provide critical services, noting that “even before the COVID pandemic, California was facing an urgent and immediate shortage of healthcare workers, adversely impacting the health and well-being of Californians.”
Although wage increases will begin rolling out next year, the timeline for implementation depends on facility type. Large health systems with more than 10,000 workers and dialysis clinics must implement the law fully by 2026, while rural independent hospitals and those with a high mix of Medi-Cal and Medicare patients have until 2033 to implement the new wage minimums.
Dive Insight:
The law, backed by California healthcare unions, broadly defines healthcare workers as full-time or contract employees of a healthcare facility, including those in roles supporting the provision of healthcare, such as janitors, clerical workers, food service workers and medical billing personnel.
The wage increase is projected to impact approximately 469,000 employees, many of whom are currently living on the margins, according to an analysis from the University of California, Berkeley’s Labor Center.
Newsom signed the bill into law on the same day that Kaiser Permanente unions announced they had secured a tentative $25 per hour minimum wage for over 60,000 California-based Kaiser employees, pending ratification from members. California healthcare workers were represented by SEIU-United Healthcare Workers West president Dave Regan during Kaiser bargaining.
In Senate analyses of the minimum wage bill conducted in May and September, lawmakers said thatSEIU-UHW’s organizing elsewhere in the state had motivated the state-level analysis of pay. The unionspearheaded several similar local ordinances last year, including inLos Angeles and San Diego.
SEIU California, which sponsored the bill, released a statement on Friday saying that raising healthcare workers’ wages is a matter of equity. Three out of four workers who will see increases in wages thanks to the new law are women, and 76% are workers of color, according to SEIU California. Almost half of all healthcare workers affected are Latino, the union said.
“Governor Newsom signed SB 525 into law because he heard our call for change to a status quo that has left us exhausted and struggling to pay our bills,” Dr. Kelley Butler, resident physician at San Francisco General Hospital and member of SEIU California, said in a statement. “I’m proud of our collective advocacy as a union and proud of our Governor for doing right by the California healthcare workforce and the patients it serves.”
The law went through several edits since the beginning of the legislative session to make it more palatable to healthcare facilities, which largely opposed its passage earlier this year. An earlier version of the bill, debated in May, tasked all healthcare providers with instituting the new minimum by June 2025.
The final version of the law has a phase-in approach that grants some workers the new minimum by 2026 and leaves others waiting ten years to reap the full sum. Healthcare facilities that are in financial distress can also apply for a waiver program to temporarily delay payroll hikes. Tribal clinics are excluded from the new pay requirements entirely.
The California Hospital Association, a lobbying organization, ultimately supported the law, saying in a statement that it provided “stability and predictability for hospitals” by providing more reasonable phase-in requirements and “preempting city and county minimum wage measures for 10 years and local compensation measures for six years.”
The dialysis industry also got on board after lawmakers added an amendment which prevents SEIU from pushing for ballot measures targeting dialysis centers. The union’s unsuccessful lobbying for changes in the dialysis industry has cost the healthcare industry over 100 million dollars in recent years, according to reporting from CalMatters.
Last week, Kaiser Family Foundation (KFF) released its Annual Employer Health Benefits Survey which included a surprise:
The average annual single premium and the average annual family premium each increased by 7% over the last year.
In 2022 as post-pandemic recovery was the focus for employers, the average single premium grew by 2% and the average family premium increased by 1%. Health costs and insurance premiums were not top of mind concerns to employers struggling to keep employees paid and door open. But 7% is an eye-opener.
The rest of the findings in the 2023 KFF Report are unremarkable: they reflect employer willingness to maintain benefits at/near pre-pandemic levels and slight inclination toward expanded benefits beyond mental health:
“The average annual premium for employer-sponsored health insurance in 2023 is $8,435 for single coverage and $23,968 for family coverage. Comparatively, there was an increase of 5.2% in workers’ wages and inflation of 5.8%2. The average single and family premiums increased faster this year than last year (2% vs. 7% and 1% vs. 7% respectively).
Over the last five years, the average premium for family coverage has increased by 22% compared to an 27% increase in workers’ wages and 21% inflation.
For single coverage, the average premium for covered workers is higher at small firms than at large firms ($8,722 vs. $8,321). The average premiums for family coverage are comparable for covered workers in small and large firms ($23,621 vs. $24,104) …
Most covered workers contribute to the cost of the premium for their coverage. On average, covered workers contribute 17% of the premium for single coverage and 29% of the premium for family coverage, similar to the percentages contributed in 2022…
90% of workers with single coverage have a general annual deductible that must be met before most services are paid for by the plan, similar to the percentage last year (88%).
The average deductible amount in 2023 for workers with single coverage and a general annual deductible is $1,735, similar to last year…
In 2023, among workers with single coverage, 47% of workers at small firms and 25% of workers at large firms have a general annual deductible of $2,000 or more. Over the last five years, the percentage of covered workers with a general annual deductible of $2,000 or more for single coverage has grown from 26% to 31%.
While nearly all large firms (firms with 200 or more workers) offer health benefits to at least some workers, small firms (3-199 workers) are significantly less likely to do so. In 2023, 53% of all firms offered some health benefits, similar to the percentage last year (51%).”
My take:
These findings show that employers are not prone to drastic changes in health benefits for their employees despite recognition it is expensive and unaffordable to small companies and for many of their own employees. But many large self-insured employers (except those in government, education and healthcare) are poised to make significant changes next year. They recognize themselves as the primary source of profits enjoyed by insurers, hospitals, physicians, drug companies and others.
They’re developing multi-year at risk direct contracts, value-based purchasing arrangements, primary care gatekeeping, narrow networks, restricted formularies, alternative care models and more to that leverage their clout. They’re going on offense.
The KFF Benefits Survey is a snapshot of where employer benefits are today, but it’s likely not the same next year. It appears employers are ready to engage the health industry head on.
PS Last week, the feud between Senate Health, Education, Labor and Pensions (HELP) Committee Chair Bernie Sanders and Not-for-Profit Health Systems heated up. On Oct. 10, he released a Majority Staff Report that said NFP hospitals do not deserve their tax exemptions as they spend “paltry amounts” on charity care. “Hospitals have gladly accepted the tax benefits that come with nonprofit status but have failed to provide the required community benefits. Non-profit hospitals spent only an estimated $16 billion on charity care in 2020, or about 57% of the value of their tax breaks in the same year.”
The same day, the American Hospital Association (AHA) released its analysis of hospital Schedule H filings concluding that tax-exempt hospitals provided $130 billion in community benefits in 2020 and called the HELP report “just plain wrong”.
In response to the AHA report, Sanders noted that AHA had not included CEO Compensation for NFPs in its analysis though featured prominently in his Majority Staff Report: “In 2021, the most recent year for which data is available for all of the 16 hospital chains, those companies’ CEOs averaged more than $8 million in compensation and collectively made over $140 million…
The disparities between the paltry amounts these hospitals are spending on charity care and their massive revenues and excessive executive compensation demonstrates that they are failing to live up to their end of the non-profit bargain.”
This tit for tat between the Committee Chairman and AHA is notable for 2 reasons: it draws attention to the Schedule H information goldmine about how not-for-profit hospitals operate since they’re now required to attach their S-10 Medicare cost report worksheets. Quantifying charity care in Exhibit 3B (for which there’s no expectation of payment) and the myriad of claimed community benefits including bad debt in Schedule 3C will likely intensify scrutiny of NFPs even more. Second, it draws attention to Executive Pay in hospitals: in this regard the Majority Staff Report commentary on CEO pay is misleading: by combining Column B (wages, bonuses) with Columns C (Deferred compensation) and D (non-taxable benefits), the total is significantly higher than one-year’s actual take-home pay for the CEOs. But it makes headlines!
If not-for-profit systems wish to lead transformational change in U.S. healthcare, not-for-profit system boards and their trade associations must be prepared to address the storm clouds gathering above. The skirmish between the Senate HELP Chair and AHA mirrors an increasingly skeptical public who, with Congress, believe the system is being gamed.
Vancouver, Wash.-based PeaceHealth has notified state officials about layoffs associated with the closure of its Sacred Heart Medical Center University District hospital campus in Eugene, Ore.
“PeaceHealth will begin consolidating services at the [Sacred Heart Medical Center] RiverBend campus in Springfield, [Ore.], and will experience a reduction in our workforce through this process that will occur throughout the next few months,” Justin Thomas, senior director for human resources in the PeaceHealth Oregon network, wrote in a WARN notice filed Oct. 19 with the Oregon Higher Education Coordinating Commission’s Office of Community Colleges and Workforce Development. “We expect some aspects of that campus to be completely closed by Feb. 1, 2024.”
PeaceHealth told state officials there are currently 463 caregivers on the University District hospital campus, and the health system is looking to have opportunities for roughly 325 caregivers, displacing 129.
“However, some of those individuals may not choose to come work at the RiverBend hospital. We do have a severance policy in place for those that will be affected by this layoff,” Mr. Thomas said.
PeaceHealth also told state officials in the notice that it notified staff in August of these changes and recently received notice from Oregon officials that it can close the first department, the emergency department, on Dec. 1. The health system noted that most of these caregivers will have positions available at the RiverBend hospital.
“However, per the request from the [Service Employees International Union], we are considering this a lay off for those caregivers and not a reorganization, so I will be providing them notice, knowing that a large portion will still be coming to the RiverBend hospital,” said Mr. Thomas.
In August, PeaceHealth shared plans to close the “underutilized” University District campus and shift services to the RiverBend campus. The plans also include relocating an urgent care to a medical office building on the University District campus to maintain access to care for those who live in the area.
In Las Vegas this week, 10,000 healthcare entrepreneurs, investors, purchasers and industry onlookers are gathered to celebrate the business of U.S. healthcare. It follows the inaugural Nashville Healthcare Sessions last month that drew a crowd to Music City touting “the premier healthcare conference set in the most relevant, exciting, and welcoming city in the south.“
Besides their locations and exceptional marketing, three notable themes are prominent that speak volumes about where this industry is:
1- The focus is systemness—integrated, connected, data-driven and scalable. Traditional divides that separate health and social services, hospitals and insurers, biotherapeutics and companion diagnostics are obsolete and access to private capital and swift execution vitals. And embedded in systemness is an expanded role of human resources that create workforces that are right-sized, diverse, AI-enabled and productive. 2-Technologies focused on end user value are gaining traction. Solutions that enable better, quicker, more accurate and affordable transactions with consumers are prominent. While traditional providers—hospitals, physicians, long-term care providers and public health programs– see HIT and AI investments as ways to make their work more efficient and satisfying, disruptors are focused on the untapped consumer market that’s dissatisfied with the status quo. 3-Access to smart capital is key. The venture capital and private equity markets in healthcare services are weathering corrections that have deflated returns and forced many to pullback or exit. The possibility of regulatory reforms involving greater transparency, carried interest restrictions and minimum hold periods means stronger funds with experienced operating partners and stable LP funding will be advantaged. In Vegas, they’ll be working the hallways to find tuck-ins for their platform bets and courting not-for-profit hospitals needing non-operating income to fund their growth and diversification efforts.
Those attending recognize the U.S. health industry faces unprecedented challenges:
Growing employer activism against lack of price transparency and inexplicably high unit costs for hospital care, prescription drugs, insurer overhead and mal-effect of consolidation in each sector.
Medical inflation that’s persistent but disproportionately absorbed by fewer and fewer employers and individuals who lack bargaining power.
Value-based purchasing activities that have failed to achieve desired cost containment goals.
Public dissatisfaction with the “system” and growing receptivity to alternatives.
Growing hostility in media coverage about hospitals, especially large not-for-profit hospitals, deemed to be profitable and wasteful.
Increased tension between providers (hospitals, medical groups) and insurers.
Increased regulation in states and court rulings that change (or have the potential to alter) how care is defined, provided, funded and legally authorized.
HLTH and Session attendees recognize the uncertainties of the political, economic and global markets in which healthcare operates. Israel will be front of mind to all as the fast-paced HLTH proceedings continue this week.
The root causes of the system’s poor performance are understood and considered: they’re daunting. But that does not impede the willingness of private investors to make bets presuming the future of the U.S. healthcare is not a repeat of its past.
Contrary to pop culture, what happens in Vegas this week will not stay in Vegas: that’s the point. The health system is not working well. While some HLTH and Sessions attendees are no doubt focused on incremental innovations to improve the performance of their legacy organizations, others are looking beyond. And, if industries akin to healthcare like financial services and higher education are instructive, the latter are better prepared to respond than the former.
PS: Nearly 50 years to the day after the Yom Kippur War in 1973, Israel was again taken by surprise by a sudden attack. Unlike the series of clashes with Palestinian forces in Gaza over the past few years, this appears to be a full-scale conflict mounted by Hamas and its allies including Iran.
Thousands are dead, more are injured and the health systems in both will be overwhelmed by the need. Health systems matter!
There is a local urgent care chain that we frequented regularly when my kids were young and cycling through rounds of ear infections and strep throat. The experience was always solid, driven by online scheduling, efficient operations, and good customer service.
A few years ago, the clinics were bought by a local health system. We recently visited one for the first time post-acquisition, when my now teenage son needed to rule out a broken bone from a sports injury. This experience at the same urgent care left a very different impression.
In contrast to the “easy in, easy out” experience I expected, we sat in an exam room for hours, even though the place was not crowded. While this could be due to the staffing challenges pervasive across the industry, other elements of the acquisition left a different impression.
Gone was the advertised cash pricing (and I’m anticipating a higher bill once we get one). The new patient self-registration system was overly complex, built for a hospital, not an immediate care setting.
The only signs of “systemness”? Multiple prompts to sign up for the health system’s MyChart patient portal (not interested, they have few facilities close by), and a printed referral to an employed orthopedic surgeon a forty-minute drive from home (with no guidance as to whether or when we should seek it, given that no bones were broken).
A few days ago, a scheduler from the system called to book the appointment. With no inquiry as to whether my son’s pain had improved, the interaction felt like a business transaction, not clinical follow-up. I declined.
Just because a care site is acquired by a health system, that doesn’t mean that patients will feel any value from its being part of a system.
Right or wrong, my impression was that health system ownership has made for a worse experience: inefficient, more complicated, and possibly more expensive.
Nothing about the visit gave me confidence that there was a benefit to following up with an affiliated provider. The health system had failed to earn our referral.
Systems buy assets like urgent care to create entry points that will generate downstream demand and hopefully build loyalty to the brand. But capturing that must start with delivering an excellent experience in every encounter, not merely changing the name on the building.
On Wednesday, 75K Kaiser Permanente (KP) healthcare workers in five states and Washington, DC walked off the job as part of the largest healthcare strike in US history.
The striking workers are a diverse group, based mostly in California, that includes support staff, X-ray technicians, medical assistants, and pharmacy workers. They will continue their work stoppage until Saturday morning, though union leadership is threatening an even larger strike in November if a new contract agreement is not reached by then.
Their employment contract expired on September 30th, and while negotiations have progressed on issues like shift-payment differentials and employee training investments, union leaders and KP executives remain at odds over key wage increase demands, with the unions asking for a $25 national minimum wage, and KP proposing $21.
The company has sought to minimize disruptions to patient care during the strike, bringing in temporary labor to keep critical infrastructure open, but has told its members to expect some non-urgent procedures to be rescheduled, some clinic and pharmacy operating hours to be reduced, and call center wait times to be lengthy.
The Gist: Kaiser Permanente has enjoyed solid relations with its unions for decades, making this strike a significant break from precedent,fueled by post-pandemic burnout and staffing shortages.
While KP is keeping all essential services open, care disruptions are inevitable with around one third of its total workforce on strike.
The stakes of these labor negotiations extend far beyond just KP and its employees, as union success could inspire other unionized healthcare workers to adopt similar tactics and demands. (Case in point: Employees at eleven Tenet Healthcare facilities in California represented by SEIU-UHW, one of the unions representing striking KP workers, just voted to authorize their own strike.)
While happening alongside high-profile strikes in other industries, labor unrest is a troubling trend for health systems, whose margins remain well below historical levels amid persistently high labor and supply expenses.