The coronavirus pandemic has caused national health care spending to go down this year — the first time that’s ever happened.
The big picture:Any big recession depresses the use of health services because people have less money to spend. But this pandemic has also directly attacked the health system, causing people to defer or skip care for fear of becoming infected.
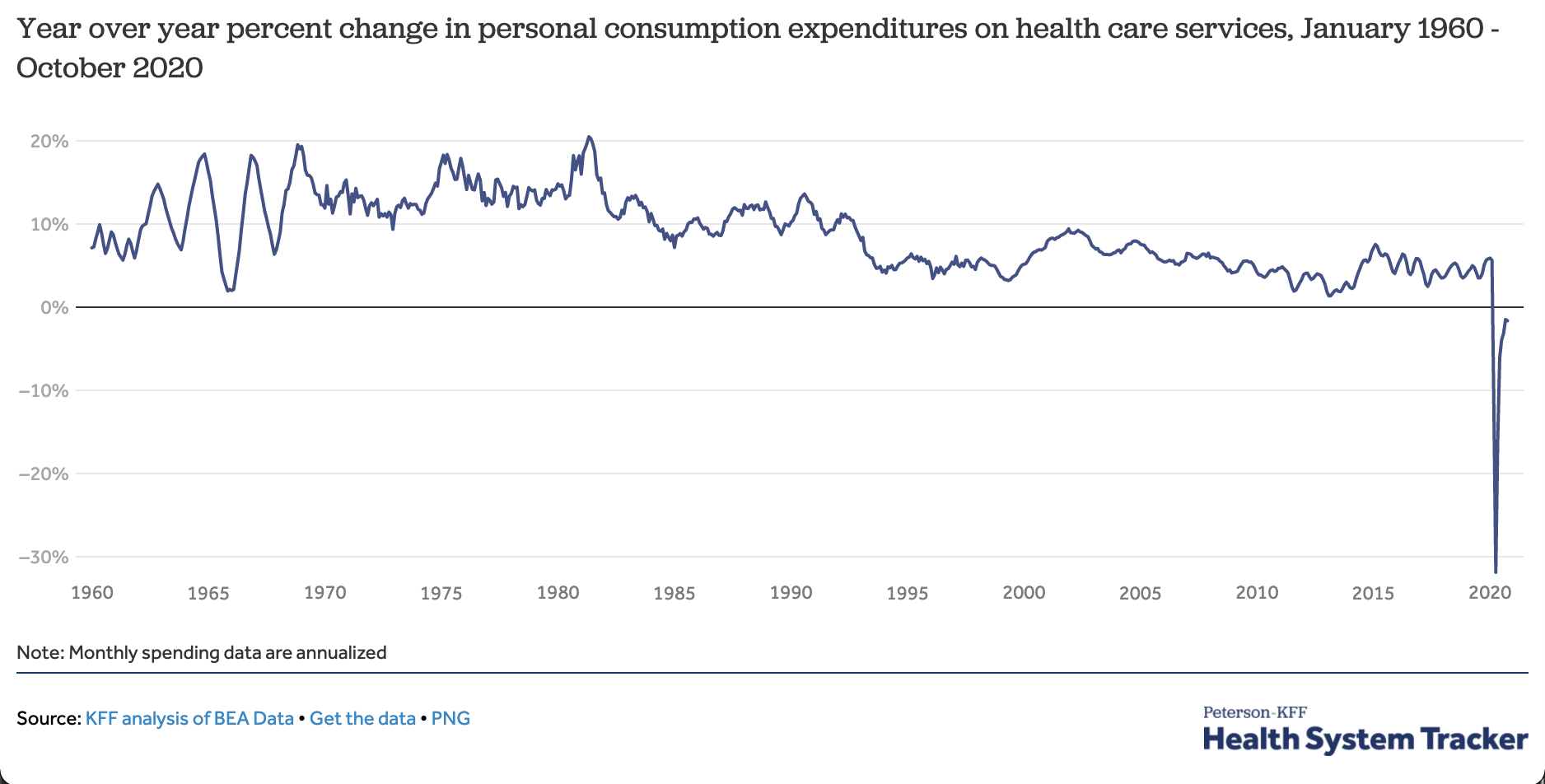
By the numbers: Year-to-date spending on health services is down about 2% from last year. Health spending for the calendar year may end up lower than it was in 2019.
In April, when the pandemic forced many facilities to temporarily close, spending on health services had fallen an eye-popping 32% on an annualized basis.
The largest drop-offs were in outpatient care. Telehealth visits increased dramatically but did not make up all of the difference.
Context: This is the first time expenditures for patient care have fallen year-over-year since data became available in the 1960s.
What’s next: Spending and utilization have been recovering, but could fall again if the current spike in cases prompts either hospitals or patients to again hold off on elective care.
There has been a decline in cancer screenings and visits to manage chronic conditions, but it will take more research before we know precisely how this has affected outcomes.
Many of the state’s hospitals have maintained lower numbers of beds in part to limit the length of patient stays and lower costs. But that approach is now being tested.
For all its size and economic might, California has long had few hospital beds relative to its population, a shortfall that state officials now say may prove catastrophic.
California is experiencing its largest surge in coronavirus cases with an average of nearly 15,000 new cases a day, an increase of 50 percent from the previous record over the summer.
So even though the state has some of the country’s most restrictive measures to prevent the spread of the virus, an influx of people with severe cases of Covid-19 may force overwhelmed hospitals to turn patients away by Christmas, Gov. Gavin Newsom warned this week.
A dearth of hospital beds has been a worldwide problem throughout the pandemic, but California, with a population of 40 million, has a particularly acute shortage. The wealthiest state in the wealthiest country has 1.8 hospital beds per 1,000 people, a level that exceeds only two states, Washington and Oregon, according to 2018 data compiled by the Kaiser Family Foundation. California has one-third the number of beds per capita as Poland.
Many hospitals in California have maintained lower numbers of beds in part to limit the length of patient stays and lower costs. But that approach is now being tested.
In addition to beds, a shortage of nursing staff will make handling the surge of virus cases “extraordinarily difficult for us in California,” said Carmela Coyle, the head of the California Hospital Association, which represents 400 hospitals across the state.
“This pandemic is a story of shortage, whether it is shortages of personal protective equipment, shortages of testing supplies, shortages of the trained staff needed to deal with these patients,” Ms. Coyle said. “It’s what has made this pandemic unique and different from other disasters.”
Also unlike other catastrophes, California will not be able to rely on other states for assistance. Mutual aid has been a cornerstone in its planning for disasters, requesting, for example, thousands of firefighters from neighboring states to help in dousing the mega-fires of recent years.
But with so many parts of the country struggling with the coronavirus at the same time, there are few traveling nurses available or nearby hospital beds to spare.
“You have to think of this as a natural disaster, like an earthquake — there’s a lot of need for hospitalization,” said Dr. George Rutherford, a professor of epidemiology at the University of California, San Francisco. “But the difference here is that it’s happening across the country. We can’t send people to Reno, Phoenix or Tucson. We’re stuck.”
The state government says it has 11 surge facilities, or alternative setups, including mothballed medical buildings and at least one sports arena, ready if hospitals become overloaded.
Beyond California, hospitals have been scrambling in recent weeks to handle a new rush of patients, particularly in parts of the Sun Belt and New England that had largely avoided coronavirus spikes in the spring and summer. The country is likely to hit a record 100,000 hospitalizations this week.CALIFORNIA TODAY: The news and stories that matter to Californians (and anyone else interested in the state).Sign Up
As hospitals exceed or get close to exceeding their capacity for coronavirus patients, state and local officials have been opening hospitals in parking lots or unoccupied buildings.
In Rhode Island, where infections have rapidly increased in recent weeks, a field hospital opened on Monday in the state’s second-largest city, Cranston. At a cost of $8 million, a former call center for Citizens Bank was converted into a 335-bed field hospital. In New Mexico, a vacant medical center in Albuquerque was being used for recovering coronavirus patients. “We are seeing the worst rates that we’ve seen since the pandemic hit,” Mayor Tim Keller said in a recent interview.
Nancy Foster, the American Hospital Association’s vice president for quality and patient safety policy, said hospital systems that are busy during the pandemic have not yet fully examined how they could have been better prepared. But she said the lack of hospital beds in many states reflected pre-Covid times.
“In an era when you’re focused on reducing the cost of health care, having excess capacity — that you’re heating and lighting and cleaning and all of that stuff — is just antithetical to your efforts to be as lean as possible, to be as cost-efficient as possible,” Ms. Foster said. “So we’re going to have some critical thinking around what’s that right balance between keeping costs low and being prepared in case a disaster happens.”
The number of hospital beds in California has declined over time partly because of a trend toward more outpatient care, said Kristof Stremikis, an expert on the state’s hospital system at the California Health Care Foundation. But more acute than the shortage of beds, Mr. Stremikis says, are staffing shortages, especially in regions with high concentrations of Black, Latino and Native American patients.
“The system is blinking red when it comes to the work force,” Mr. Stremikis said. “It’s nurses, doctors, allied health professionals — we don’t have enough of many different types of clinicians in California and they’re not in the right places. It’s a huge issue.”
Mr. Newsom has said California would draw from a registry of retired or nonpracticing health care workers and deploy them to hospitals.
But Ms. Coyle, the head of the California Hospital Association, says she does not think volunteers can bridge the gap.
“We are down to a very, very small fraction who are willing to serve,” she said. “Those volunteers were not trained at a level to be as helpful in a hospital setting.”
At the county level, health officers are counting down the days until their hospitals are full. On Sunday, California became the first state to record more than 100,000 cases in a week, according to a New York Times database. The state government estimates that about 12 percent of cases end up in a hospital.
Dr. Sara Cody, the chief health officer for Santa Clara County, which includes a large slice of Silicon Valley, projects that hospitals in the county will reach capacity by mid-December.
“This is the most difficult phase of the pandemic so far,” Dr. Cody said. “Everyone is tired.”
She is expecting a spike in cases from Thanksgiving gatherings, which could accelerate the timeline, she said.
Few states have been as aggressive in combating the pandemic as California, which now has a stockpile of a half-billion face masks. Los Angeles last week announced a ban on gatherings with other households. In Santa Clara County, hotels are now only reserved for essential travel and a ban on contact sports is forcing the San Francisco 49ers to play home games in Arizona.
“We have done everything that we can do as local leaders and health officials,” said Dr. Cody, who led the effort in March to put in place the country’s first shelter-in-place order. “We have worked as hard as we can work. We have tried everything that we know how to do. But without bold action at the state or federal level we are not going to be able to slow this down. We are not an island.”
Across California a weary populace wondered about the effectiveness of the state’s measures.
In Los Angeles, local officials were under fire after hundreds of tests scheduled for Tuesday at Union Station were canceled because of a film shoot, a remake of the 1990s romantic comedy “She’s All That.” People who had scheduled tests were informed of the cancellation on Monday afternoon, and it was not until after midnight that Mayor Eric Garcetti announced the tests were back on.
The filming was still taking place on Tuesday morning as Wendy Ambriz swabbed her mouth at the station’s testing kiosk.
Ms. Ambriz did not think the county’s restriction of outdoor dining, which went into effect last week, was necessary, noting that kitchen staffs are fastidious about cleanliness. But she did not blame government officials for the coronavirus spiraling out of control in Southern California.
“People don’t really follow directions,” she said.
That assessment appears to hold true for some of the state’s officials.
Sheila Kuehl, who sits on the county board of supervisors, was spotted at an Italian restaurant in Santa Monica hours after publicly calling outdoor dining “a most dangerous situation” and voting to ban it. In a statement on Monday, Ms. Kuehl’s office noted that the ban had not yet gone into effect when the dinner occurred. Her meal recalled another moment of apparent hypocrisy, a meal attended by Mr. Newsom and a gaggle of lobbyists at the luxurious French Laundry restaurant in Napa Valley just as the governor was advising residents to avoid meeting with large groups.
Outside the Broad Street Oyster Company in Malibu last week, picnic tables were cordoned off and the restaurant was not seating customers. But that did not stop people from eating there — they just ducked under the tape.
In mid-November, as the United States set records for newly diagnosed COVID-19 cases day after day, the hospital situation in one hard-hit state, Wisconsin, looked concerning but not yet urgent by one crucial measure. The main pandemic data tracking system run by the Department of Health and Human Services (HHS), dubbed HHS Protect, reported that on 16 November, 71% of the state’s hospital beds were filled. Wisconsin officials who rely on the data to support and advise their increasingly strained hospitals might have concluded they had some margin left.
Yet a different federal COVID-19 data system painted a much more dire picture for the same day, reporting 91% of Wisconsin’s hospital beds were filled. That day was no outlier. A Science examination of HHS Protect and confidential federal documents found the HHS data for three important values in Wisconsin hospitals—beds filled, intensive care unit (ICU) beds filled, and inpatients with COVID-19—often diverge dramatically from those collected by the other federal source, from state-supplied data, and from the apparent reality on the ground.
“Our hospitals are struggling,” says Jeffrey Pothof, a physician and chief quality officer for the health system of the University of Wisconsin (UW), Madison. During recent weeks, patients filled the system’s COVID-19 ward and ICU. The university’s main hospital converted other ICUs to treat the pandemic disease and may soon have to turn away patients referred to the hospital for specialized care. Inpatient beds—including those in ICUs—are nearly full across the state. “That’s the reality staring us down,” Pothof says, adding: The HHS Protect numbers “are not real.”
HHS Protect’s problems are a national issue, an internal analysis completed this month by the Centers for Disease Control and Prevention (CDC) shows. That analysis, other federal reports, and emails obtained by Science suggest HHS Protect’s data do not correspond with alternative hospital data sources in many states (see tables, below). “The HHS Protect data are poor quality, inconsistent with state reports, and the analysis is slipshod,” says one CDC source who had read the agency’s analysis and requested anonymity because of fear of retaliation from the Trump administration. “And the pressure on hospitals [from COVID-19] is through the roof.”
Both federal and state officials use HHS Protect’s data to assess the burden of disease across the country and allocate scarce resources, from limited stocks of COVID-19 medicines to personal protective equipment (PPE). Untrustworthy numbers could lead to supply and support problems in the months ahead, as U.S. cases continue to rise during an expected winter surge, according to current and former CDC officials. HHS Protect leaders vigorously defend the system and blame some disparities on inconsistent state and federal definitions of COVID-19 hospitalization. “We have made drastic improvements in the consistency of our data … even from September to now,” says one senior HHS official. (Three officials from the department spoke with Science on the condition that they not be named.)
CDC had a long-running, if imperfect, hospital data tracking system in place when the pandemic started, but the Trump administration and White House Coronavirus Task Force Coordinator Deborah Birx angered many in the agency when they shifted much of the responsibility for COVID-19 hospital data in July to private contractors.TeleTracking Technologies Inc., a small Pittsburgh-based company, now collects most of the data, while Palantir, based in Denver, helps manage the database. At the time, hundreds of public health organizations and experts warned the change could gravely disrupt the government’s ability to understand the pandemic and mount a response.
The feared data chaos now seems a reality, evident when recent HHS Protect figures are compared with public information from states or data documented by another hospital tracking system run by the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR). ASPR manages the Strategic National Stockpile of medicines, PPE—in perilously short supply in many areas—and other pandemic necessities. ASPR collects data nationwide, although it is more limited than what HHS Protect compiles, to help states and hospitals respond to the pandemic.
In Alabama, HHS Protect figures differ by 15% to 30% from daily state COVID-19 inpatient totals. Karen Landers, assistant state health officer, said nearly all of the state’s hospitals report data to HHS via the Alabama Department of Public Health. Although reporting delays sometimes prevent the systems from syncing precisely, Landers says, she cannot account for the sharp differences.
Many state health officials contacted by Science were reluctant to directly criticize HHS Protect or attribute supply or support problems to its data. Landers notes that Alabama relies on its own collected data, rather than HHS Protect’s, for its COVID-19 response. “We are very confident in our data,” she says, because the state reporting system was developed over several years and required little adjustment to add COVID-19. HHS, she adds, has generally been responsive to state requests for medicines and supplies, although Alabama has not always gotten all the PPE it has requested.
Other states, however, say they do rely on HHS Protect. A spokesperson for the Wisconsin Department of Health Services wrote in a response to questions, “When making decisions at the state level we use the HHS Protect data,” but declined to comment about its accuracy. HHS informed Wisconsin officials it distributes scarce supplies based on need indicated by HHS Protect data, the spokesperson wrote.
Pothof says UW’s hospital system has its own sophisticated data dashboard that draws on state, local, and internal sources to plan and cooperate on pandemic response with other hospitals. But small hospitals in Wisconsin—now experiencing shortages of some medicines, PPE, and other supplies—are more dependent on federal support largely based on HHS Protect data. Help might not arrive, Pothof says, if the data show “things look better than they are.”
If the HHS Protect data are suspect, “that’s a very large problem,” says Nancy Cox, former director of CDC’s influenza division and now an affiliated retiree of the agency. If HHS officials use bad data, they will not distribute medicines and supplies equitably, Cox notes, adding: “Undercounting in the hardest hit states means a lower level of care and will result in more severe infections and ultimately in more deaths.”
Birx and the other managers of HHS Protect “really had no idea what they were doing,” says Tom Frieden, CDC director under former President Barack Obama. (Birx declined to comment for this article.) Frieden cautions that ASPR data might also be erroneous—pointing to the need for an authoritative and clear federal source of hospital data. The original CDC system, called the National Healthcare Safety Network (NHSN), should be improved, he said, but it handles nursing home COVID-19 data skillfully and could do the same with hospitals. NHSN is “not just a computer program. It’s a public health program” built over 15 years and based on relationships with individual health facilities, Frieden says. (CDC insiders say HHS officials recently interfered with publication of an analysis showing that NHSN performed well early in the pandemic [see sidebar, below]).
An HHS official says HHS Protect’s data are complex and the department can’t verify any findings in the reports reviewed by Science without conducting its own analysis, which it did not do. But the official says HHS Protect has improved dramatically in the past 2 months and provides consistent and reliable results.
As for the difference between state and HHS Protect data, an HHS official contends state numbers “are always going to be lower” by up to 20%. That’s because hospitals could lose Medicare funding if they do not report to HHS, the official says, but face no penalty for failing to report to the state. So rather than expect identical numbers, HHS looks for state and federal data to reflect the same trajectory—which they do in all cases for COVID-19 inpatient data, according to another confidential CDC analysis of HHS Protect, covering all 50 states.
Yet the same analysis found 27 states recently alternated between showing more or fewer COVID-19 inpatients than HHS Protect—not always just fewer, as HHS says should be the case. Thirty states also showed differences between state and HHS Protect figures that were frequently well above the 20% threshold cited by HHS, and HHS Protect data fluctuated erratically in 21 states (see chart, below).
“Hospital capacity metrics can and should be a national bellwether,” the CDC data expert says. “One important question raised by the discordant data reported by HHS Protect and the states is whether HHS Protect is systematically checking data validity.” HHS has not provided its methodology for HHS Protect data estimates for review by independent experts. But an HHS official says a team of data troubleshooters, including CDC and ASPR field staff, work to resolve anomalies and respond to spikes in cases in a state or hospital.
Out of sync
Tracking hospital inpatients who have COVID-19 has become a crucial measure of the pandemic’s severity. Department of Health and Human Services (HHS) data from the HHS Protect system often diverge sharply from state-supplied data. This chart, drawn from a data analysis from the Centers for Disease Control and Prevention, summarizes some of the similarities and differences for COVID-19 inpatient totals over the past 2 months.
Along with improving trust in its data, HHS Protect needs to make it more accessible, CDC data scientists say. The publicly accessible HHS Protect data are far less complete than the figures in its password-protected database. This effectively hides from public view key pandemic information, such as local supplies of protective equipment.
The site also does not provide graphics highlighting patterns and trends. This might explain, in part, why most media organizations—as well as President-elect Joe Biden’s transition team—instead have relied on state or county websites that vary widely in completeness and quality, or on aggregations such as The Atlantic magazine’s COVID Tracking Project, which collects, organizes, and standardizes state data. (In comparing state and federal data, CDC also used the COVID Tracking Project.)
Frieden and other public health specialists call reliable, clear federal data essential for an effective pandemic response. “The big picture is that we’re coming up to 100,000 hospitalizations within the next few weeks. Hospital systems all over the country are going to be stressed,” Frieden says. “There’s not going to be any cavalry coming over the hill from somewhere else in the country, because most of the country is going to be overwhelmed. We’re heading into a very hard time with not very accurate information systems. And the government basically undermined the existing system.”
Dressed in blue scrubs and carrying a stethoscope around her neck, an oncology nurse in Salem, Ore., looked to the Grinch as inspiration while suggesting that she ignored coronavirus guidelines outside of work.
In a TikTok video posted Friday, she lip-dubbed a scene from “How the Grinch Stole Christmas” to get her point across to her unaware colleagues: She does not wear a mask in public when she’s not working at Salem Hospital.
“When my co-workers find out I still travel, don’t wear a mask when I’m out and let my kids have play dates,” the nurse wrote in a caption accompanying the video, which has since been deleted.
Following swift online backlash from critics, her employer, Salem Health, announced Saturday that the nurse had been placed on administrative leave. In a statement, the hospital said the nurse, who has not been publicly identified by her employer, “displayed cavalier disregard for the seriousness of this pandemic and her indifference towards physical distancing and masking out of work.”
“We also want to assure you that this one careless statement does not reflect the position of Salem Health or the hardworking and dedicated caregivers who work here,” said the hospital, adding that an investigation is underway.
Salem Health did not respond to The Washington Post’s request for comment as of early Monday.
The nurse’s video offers a startling and rare glimpse of a front-line health-care worker blatantly playing down a virus that has killed at least 266,000 Americans. It also has been seen in some coronavirus patients, some on their deathbeds, who still refuse to believe the pandemic is real.
The incident comes at a time when Oregon has continued to see a spike in new coronavirus cases and virus-related hospitalizations. Just last week, the state’s daily reported deaths and hospitalizations rose by 33.3 and 24.2 percent respectively, according to The Post’s coronavirus tracker. At least 74,120 Oregonians have been infected with the virus since late February; 905 of them have died.
The clip posted to TikTok on Friday shows the nurse mocking the health guidelines while using audio from a scene in which the Grinch reveals his true identity to Cindy Lou Who.
Although the original video was removed, TikTok users have shared a “duet” video posted by another user critical of the nurse, which had more than 274,000 reactions as of early Monday.
Soon after she posted the clip, hundreds took to social media and the hospital’s Facebook page to report the nurse’s video and demand an official response from her employer. Some requested that the nurse be removed from her position and that her license be revoked.
Hospital officials told the Salem Statesman Journal that the investigation is aiming to figure out which other staff members and patients have come in contact with the nurse, who works in the oncology department.
But for some, the hospital’s apologies and actions were not enough.
“The video supplied should be evidence enough,” one Facebook user commented. “She needs to be FIRED. Not on PAID leave. As someone fighting cancer, I can only imagine how her patients feel after seeing this news.”
The hospital thanked those who alerted them of the incident, emphasizing that its staff, patients and visitors must adhere to the Centers for Disease Control and Prevention guidelines.
“These policies are strictly enforced among staff from the moment they leave their cars at work to the moment they start driving home,” hospital officials told the Statesman Journal.
At a rural health system in Wisconsin, officials and medical experts began drawing up protocols for the once unthinkable practice of deciding which patients should get care. The chief quality officer of a major New York hospital network double- and triple-checked his system’s stockpile of emergency equipment, grimly recalling the last time he had to count how many ventilators he had left. In Arizona, a battle-weary doctor watched in horror as people flooded airports and flocked to stores for Black Friday sales, knowing it was only a matter of time before some of them wound up in his emergency room.
Days after millions of Americans ignored health guidance to avoid travel and large Thanksgiving gatherings, it’s still too soon to tell how many people became infected with the coronavirus over the course of the holiday weekend. But as travelers head home to communities already hit hard by the disease, hospitals and health officials across the country are bracing for what scientist Dave O’Connor called “a surge on top of a surge.”
“It is painful to watch,” said O’Connor, a virologist at the University of Wisconsin at Madison. “Like seeing two trains in the distance and knowing they’re about to crash, but you can’t do anything to stop it.”
“Because of the decisions and rationalizations people made to celebrate,” the scientist added, “we’re in for a very dark December.”
The holiday, which is typically one of the busiest travel periods of the year, fell at a particularly dire time in the pandemic. Some 4 million Americans have been diagnosed with the coronavirus in November — twice the previous record, which was set last month. More than 2,000 people are dying every day. Despite that, over a million people passed through U.S. airports the day before Thanksgiving — the highest number of travelers seen since the start of the outbreak.
Many states did not report new case counts over the holiday, and it typically takes about a week for official records to catch up after reporting delays, said Caitlin Rivers, an epidemiologist at the Johns Hopkins Center for Health Security.
But in two to three weeks, she said, “I fully expect on a national level we will see those trends continue of new highs in case counts and hospitalizations and deaths.”
The nation has already notched several bleak milestones over the holiday weekend. On Thanksgiving Day, hospitalizations in the United States exceeded 90,000 people for the first time. The following day, the country hit 13 million cases. At least nine states have seen 1 in every 1,000 residents die of the coronavirus.
Mark Jarret, the chief quality officer for New York’s Northwell Health system, said he understood that many people are tiring of constant vigilance after nine months of isolation and Zoom gatherings and waving at people from six feet away.
“But we’re so close to getting some control,” he said, noting that federal officials are on the verge of authorizing one or more vaccines against the virus next month. “This is not the time to let up. This is the time to put on the best defense we can to prevent further spread, further death.”
Officials urged people who traveled or spent time with people outside their household to stay at home for 14 days to avoid further spread of the virus. Some jurisdictions are moving toward lockdown measures not seen since the spring. Los Angeles County on Friday issued a three-week “safer at home” order, limiting business capacity and prohibiting gatherings other than religious services and protests.
Meanwhile, the December holidays are looming.
“Hopefully people will try to minimize their risks around Christmas, especially if there’s data that show Thanksgiving was really harmful,” O’Connor said.
To Cleavon Gilman, a Navy veteran and emergency room doctor in Yuma, Ariz., the wave of holiday travel was “a slap in the face.”
“It’s as if there’s not a pandemic happening,” he said. “We’re in a war right now, and half the country isn’t on board.”
On Friday, members of the University of Arizona coronavirus modeling team issued an urgent warning to state health officials, projecting that the state will exceed ICU capacity by the beginning of December.
“If action is not immediately taken, then it risks a catastrophe on a scale of the worst natural disaster the state has ever experienced,” the team wrote in a letter to Steven Bailey, chief of the Bureau of Public Health Statistics. “It would be akin to facing a major forest fire without evacuation orders.”
Arizona has no statewide mask mandate, and businesses in many parts of the state, including indoor dining at restaurants, remain open.
Gilman said the intensive care unit at his hospital is full and there’s nowhere to transfer new patients. When he’s home, his mind echoes with the sound of people gasping for breath. He and his colleagues are exhausted, and with cases spiking across the country, he worries there is no way they can handle the surge that will probably follow Thanksgiving celebrations.
In La Crosse, Wis., Gundersen Health System chief executive Scott Rathgaber echoed that fear. “We’ve had to tell our hard-working staff, ‘There’s no one out there to come rescue us,’” he said.
Like many in his college town, Rathgaber is anxious about what will happen when students who spent the holiday with their families return to campus. Though the University of Wisconsin and other schools shifted classes online for the remainder of the semester, he anticipates students who have jobs and apartments in La Crosse will return to town.
“We had trouble the first time the students came back,” Rathgaber said, noting that the start of college classes in September preceded outbreaks in nursing homes and a spike in deaths in La Crosse County. “I will continue to implore, to beg people to take this seriously.”
Gundersen has already more than tripled the size of the covid-19 ward at its main hospital, and even before this week it was almost entirely full. Physicians from the system’s rural clinics have been reassigned to La Crosse to help in the ICU. Staff who may have been exposed to the virus are being called back before completing their 14-day quarantine. And Rathgaber now attends regular meetings with ethicists and end-of-life caregivers to figure out Gundersen’s triage protocol if the hospital becomes overwhelmed.
“We’re not at a breaking point, but we are getting there,” Rathgaber said. “I’m concerned about what the next two weeks will bring.”
Becker’s Hospital Review compiled 40 large health systems by number of hospitals and 60 large hospitals by bed count.
This list was developed based on information as of September 2020.
Largest Health Systems
HCA Healthcare (Nashville, Tenn.): 186 hospitals. HCA Healthcare has more than 46,000 active and affiliated physicians and 98,000 registered nurses worldwide. In 2019, the health system reported approximately 35 million patient encounters and 9.2 million emergency room visits. HCA Healthcare ranks No. 65 on the Fortune 500 list and was named among the Ethisphere Institute’s “World’s Most Ethical Companies” list in 2019 for the 10th consecutive year.
Veteran’s Health Administration: 170 hospitals. The VA has 1,255 health care facilities that serve veterans and their families, including 170 medical centers. The health system has 1,074 outpatient sites as well. The VA serves around 9 million veterans per year.
Ascension (St. Louis): 151 hospitals. Ascension is a nonprofit Catholic health system with around 160,000 associates and 40,000 aligned providers. Systemwide, Ascension offers 2,700 care sites in 20 states and Washington, D.C. The health system provides around 25 million outpatient visits per year and 3.1 million ER visits.
CommonSpirit Health (Chicago): 137 hospitals. CommonSpirit Health was created in February 2019 as a combination of Englewood, Colo.-based Catholic Health Initiatives and San Francisco-based Dignity Health. When it launched, the health system included 150,000 employees and 25,000 physicians. The faith-based health system operates hospitals and care centers in 21 states.
Community Health Systems (Franklin, Tenn.): 93 hospitals. CHS has more than 30 years of history, acquiring individual community and small hospitals. It spun off of Brentwood, Tenn.-based Quorum Health as a 38-hospital health system in April 2016 and now includes 93 hospitals in 16 states. The publicly traded health system has 15,000 licensed beds across all facilities.
Trinity Health (Livonia, Mich.): 92 hospitals. Trinity Health is a Catholic health system with 92 hospitals and 106 continuing care locations. It employs around 119,000 individuals, including 7,500 physicians and clinicians. The health system has locations in 22 states and serves communities that include about 30 million people nationwide.
LifePoint Health (Brentwood, Tenn.): 88 hospitals. The National Rural Health Association recognized two of the health system’s hospitals — Riverview Regional Medical Center in Carthage, Tenn., and Trousdale Medical Center in Hartsville, Tenn. — among the top 20 critical access hospitals in the nation in 2019. LifePoint Health is home to more than 55,000 employees.
Tenet Healthcare (Dallas): 65 hospitals. In addition to its 65 acute care hospitals, Tenet Healthcare operates approximately 510 healthcare facilities, including ambulatory surgery centers, outpatient centers, urgent care centers and imaging centers. The health system was ranked No. 172 on the Fortune 500 rankings for 2020 and has around 112,000 employees.
Vibra Healthcare (Mechanicsburg, Pa.): 45 hospitals. Founded in 2004, Vibra Healthcare and its affiliates have grown significantly over the past 15 years to employ more than 6,000 individuals and operate 45 specialty acute care hospitals, transitional care units and facilities, and outpatient physical therapy centers. The health system operates facilities in 14 states.
Providence (Renton, Wash.): 51 hospitals. Providence supports 51 hospitals, 1,085 clinics and more than 120,000 employees across eight states. It was formed in 2016 by the combination of Providence Health & Services and St. Joseph Health, and now includes a single health plan with 2.1 million covered lives.
Atrium Health (Charlotte, N.C.): 36 hospitals. In 2018, Carolinas HealthCare System rebranded as Atrium Health, a health system with history dating back to 1940, when its flagship hospital opened its doors. Now, the health system includes nearly 40 hospitals and hundreds of care locations that include physician offices, behavioral health centers and nursing homes. The health system is home to more than 55,000 employees and has earned HIMSS Analytics Stage 7 certification in both the acute care and ambulatory environments.
AdventHealth (Altamonte Springs, Fla.): 49 hospitals. AdventHealth is a faith-based health system with nearly 50 hospitals in nine states, serving approximately 6 million patients annually. More than 80,000 team members in physician practices, hospitals, outpatient clinics, skilled nursing facilities, home health agencies and hospice centers provide individualized, whole-person care.
Baylor Scott & White Health (Dallas): 52 hospitals. Baylor Scott & White was formed in 2013 as a combination of Baylor Health Care System and Scott & White Healthcare. The system has more than 1,100 care sites and 7,300 active physicians. The health system also includes a health plan and supports more than 49,000 employees and more than 7.5 million patient encounters per year. In 2020-21, 17 Baylor Scott & White hospitals appeared on the U.S. News & World Report list of America’s Best Hospitals.
Bon Secours Mercy Health (Cincinnati): 50 hospitals. Bon Secours Mercy Health has more than 60,000 team members and 2,600 providers. The nonprofit Catholic health system has a presence in seven U.S. states and Ireland, and supports a research team focused on innovation to change the healthcare landscape.
Prime Healthcare (Ontario, Calif.): 46 hospitals. Since its founding in 2001, Prime Healthcare has grown to employ 40,000 people and operate hospitals and outpatient facilities across 14 states. The for-profit health system, which includes for-profit and nonprofit hospitals, hasn’t sold or closed any hospitals since its inception and has invested $1.7 billion in capital improvements since 2005.
Sanford Health (Sioux Falls, S.D.): 46 hospitals. Sanford Health is an integrated health system that includes more than 200 senior living facilities and more than 200 clinics. The health system also supports a 200,000-member health plan and 47,757 employees. More than 1,400 physicians and 8,502 registered nurses deliver care at the health system’s locations across 26 states and 10 countries.
UPMC (Pittsburgh): 40 hospitals. UPMC reports 40 academic, community and specialty hospitals, 700 physician offices and outpatient sites, and 90,000 employees. It also has rehabilitation, retirement and long-term care facilities, as well as a 3.9 million-member health plan. The health system has programs in four continents outside of North America and has a commercial arm, UPMC Enterprises, that aims to support innovation and efforts to lower the cost of care with data-focused digital solutions.
Mercy (St. Louis): 39 hospitals. The Sisters of Mercy founded this health system in 1986. The health system has 39 acute care, managed and specialty hospitals, as well as more than 900 physician practices and 2,400 Mercy Clinic physicians. Mercy also supports an IT division, supply chain organization and Mercy Virtual, which serves providers and patients nationwide.
Kaiser Permanente (Oakland, Calif.): 39 hospitals. Kaiser Permanente is a 39-hospital system with 715 medical offices and nearly 23,300 physicians. The health system supports more than 63,306 nurses and 217,828 employees across eight states and Washington, D.C. Kaiser also includes a nonprofit health plan serving 12.4 million members.
Avera Health (Sioux Falls, S.D.): 37 hospitals. Avera Health has 315 locations across 100 communities, covering a patient population of 1 million people. The faith-based health system has 19,700 employees and healthcare experts in 60 medical specialties. It also provides management and consultation services and group purchasing for rural healthcare facilities.
Steward Health Care (Dallas): 36 hospitals. Steward Health Care is the largest private, physician-owned and led healthcare network in the country. Steward serves more than 800 communities with hospitals, urgent care centers and preferred skilled nursing facilities across nine states. The health system has more than 37,000 employees and 7,000 beds systemwide. The Steward Health Care Network reports around 12 million patient encounters per year.
Christus Health (Irving, Texas): 35 hospitals. Christus Health is a nonprofit health system with more than 600 healthcare-related centers. The system has around 45,000 team members, including 15,000 physicians that provide care in North America and South America. The faith-based health system has an ACO that participates in the Medicare Shared Savings Program.
Ardent Health Services (Nashville, Tenn.): 30 hospitals. Ardent has invested more than $1.5 billion in new hospitals as well as expanding services at existing facilities since 2001. The health system encompasses 4,384 licensed beds, 26,000 employees, approximately 180 clinic locations and more than 1,350 employed providers. It continues to focus on acquisitions of both in-market and new market opportunities.
Great Plains Health Alliance (Wichita, Kan.): 29 hospitals. Great Plains Health Alliance is a nonprofit organization that leases, manages and affiliates with hospitals in Kansas and Nebraska. Dating back to 1950, the health system has served rural communities and now works with team members to develop innovative solutions to overcome the challenges community hospitals face through consolidation in the healthcare space.
Banner Health (Phoenix): 28 hospitals. Banner Health is a large nonprofit health system that serves both rural and urban areas. The health system merged with the Tucson-based University of Arizona Health Network in 2015 to form Banner-University Medicine. It has more than 50,000 employees and is the largest employer in the Arizona region.
Community Hospital Corp. (Plano, Texas): 27 hospitals. CHC was founded in 1996 as a company to help community hospitals succeed. The health system has expanded since then to include hospitals across the nation and to provide supply chain, consulting, management and strategic support services.
Texas Health Resources (Arlington): 27 hospitals. In 1997, Texas Health Resources was formed through assets of Harris Methodist Health System in Fort Worth, Texas, and Presbyterian Healthcare Resources in Dallas. Since then, the health system has grown to include 27 hospitals and more than 4,000 licensed beds. Texas Health employs more than 23,000 individuals and has about 6,200 physicians with staff privileges.
Advocate Aurora Health (Oak Lawn, Ill.): 26 hospitals. Advocate Aurora Health reports 3 million unique patient visits per year at its 26 hospitals and 500 outpatient locations. It also has 63 Walgreens clinics and more than half a million users of its LiveWell app, which allows consumers to access personalized wellness information and virtual health tools across the health system. Formed in 2018 as a merger of Advocate Health Care and Aurora Health, Advocate Aurora Health has 5,500 employed physicians and advanced practice clinicians, 22,000 nurses and 75,000 team members.
Universal Health Services (King of Prussia, Pa.): 26 hospitals. UHS has more than 400 hospitals, behavioral health facilities and ASCs in its system, which spans the U.S., U.K., and Puerto Rico. The health system ranked No. 281 among Fortune 500 companies in revenue for 2019; it has been ranked on the list for 17 years. The health system has more than 90,000 employees.
MercyOne (Clive, Iowa): 25 hospitals. MercyOne was founded in 1998 as a collaboration between Englewood, Colo.-based Catholic Health Initiatives and Livonia, Mich.-based Trinity Health, and the two Catholic health systems continue to support MercyOne. The health system has grown to 420 locations, including 25 affiliated hospitals and 18 owned or joint-venture medical centers.
Indian Health Service (Rockville, Md.): 24 IHS-operated and 22 tribally operated hospitals. The Indian Health Service is an agency within the HHS that provides healthcare services to about 2.6 million American Indians and Alaska natives belonging to 574 federally recognized tribes in 37 states. The health system includes CMS-designated critical access hospitals in rural areas and other locations.
Intermountain Healthcare (Salt Lake City): 24 hospitals. Intermountain Healthcare is a nonprofit health system with 24 hospitals (one is virtual), 215 clinics and 40,000 employees. The system also has a 2,500-physician medical group and a health plan. In 2017, the health system won the Hearst Health prize for its mental health integration program.
Sutter Health (Sacramento, Calif.): 24 hospitals. Sutter is a nonprofit health system that has more than 14,000 physician partners who care for more than 3.5 million patients. In addition to its hospitals, Sutter has about 36 ASCs and 4,259 licensed general acute care beds. The health system has appeared on IBM Watson Health’s Top 15 Health Systems list.
Mayo Clinic Health System (Rochester, Minn.): 23 hospitals. Mayo Clinic Health System has three major campuses in Minnesota, Arizona and Florida. The organization also serves more than 70 communities in Minnesota and Iowa through the Mayo Clinic Health System. More than 3,800 physicians and scientists and 63,100 allied health staff work at Mayo Clinic. Collectively, these sites care for about 1.2 million people annually from all 50 states and more than 135 countries.
Northwell Health (New Hyde Park, N.Y.): 23 hospitals. In addition to its 23 hospitals, Northwell Health has more than 800 outpatient facilities and 14,200 affiliated physicians providing care for New York residents. The health system has about 70,000 team members, including 18,500 nurses and 4,500 employed physicians, along with a 1,900-plus medical resident and fellows program. More than 2 million patients receive treatment at Northwell facilities per year, including 865,260 emergency visits and 221,580 ambulatory surgeries.
SSM Health (St. Louis): 23 hospitals. SSM Health has about 40,000 employees and 11,000 care providers. The faith-based nonprofit health system provides care in Illinois, Missouri, Oklahoma and Wisconsin. As of May 2019, the health system reported more than 2 million outpatient visits and 185,112 inpatient admissions per year.
Baptist (Memphis, Tenn.): 22 hospitals. Baptist has 22 hospitals and 3,561 licensed beds. The health system supports more than 19,000 team members and 5,000 affiliated physicians who perform nearly more than 70,000 surgical procedures per year. The health system has several specialty centers and partnered with Semmes Murphey Clinic in 2015 to form the Brain & Spine Network.
Quorum Health Corp. (Brentwood, Tenn.): 22 hospitals. Quorum Health has 22 affiliated hospitals in rural and mid-sized markets in 13 states. The health system has an aggregate of 1,817 licensed beds and also operates outpatient services providers. Quorum Health’s subsidiary, Quorum Health Resources, provides management and consulting services to more than 150 hospitals.
UnityPoint Health (West Des Moines, Iowa): 21 hospitals. UnityPoint Health has 400 physician clinics, 21 regional and 19 community network hospitals, seven community mental health centers, four accredited colleges and home care services in Iowa, Illinois and Wisconsin. It has more than 30,000 team members in rural and metropolitan communities. The health system reports about 7.9 million patient visits per year and has an ACO, as well as coordinated care programs.
Ballad Health (Johnson City, Tenn.): 21 hospitals. Ballad Health is a 21-hospital health system that includes about 3,000 clinicians who care for patients in 29 counties covering areas of Tennessee, Virginia, North Carolina and Kentucky. The system includes a children’s hospital as well as several community hospitals, long-term care facilities and retail pharmacies.
Largest Hospitals
Barnes-Jewish Hospital (St. Louis): 1,638 beds. Barnes-Jewish Hospital is a teaching hospital affiliated with Washington University School of Medicine in St. Louis. The hospital is among the top 20 hospitals named to U.S. News &World Report’s 2020-21 Best Hospitals Honor Roll. Barnes-Jewish is a member of BJC HealthCare, which provides a full range of health care services through its 15 hospitals and more than 100 healthcare sites in Missouri and Illinois.
Yale New Haven (Conn.) Hospital: 1,541 beds. Yale New Haven Hospital, part of Yale New Haven Health, serves as the primary teaching hospital for the Yale School of Medicine. Founded as the fourth voluntary hospital in the U.S. in 1826, today, it has two New Haven-based campuses, and also includes Yale New Haven Children’s Hospital, Yale New Haven Psychiatric Hospital and Smilow Cancer Hospital. Yale New Haven Hospital has a combined medical staff of about 4,500 university and community physicians practicing in more than 100 specialties.
Ohio State University Wexner Medical Center (Columbus): 1,509 beds. In August 2019, Ohio State University Wexner Medical Center recorded a milestone: performing more than 10,000 transplant surgeries. The hospital has nearly 30,000 employees and 1,813 physicians. lIt reported 62,352 patient admissions and 121,915 emergency room visits for the 2020 fiscal year. Wexner Medical Center also promotes research and reports more than 2,000 active studies and clinical trials.
Jackson Memorial Hospital (Miami): 1,500 beds. Jackson Memorial Hospital is the flagship hospital for Jackson Health System and is home to the level 1 Ryder Trauma Center. The hospital also houses the Miami Transplant Institute, Miami Burn Center and the Schatzi and Stanley Kassal Project, a level 3 neonatal intensive care units with 126 beds.
AdventHealth Orlando (Fla.): 1,364 beds. AdventHealth Orlando has an international reputation for providing cutting-edge treatment and research to advance care delivery. The hospital is the flagship of AdventHealth, a faith-based health system with nearly 50 hospitals in nine states. U.S. News & World Report named AdventHealth Orlando the No. 3 hospital in Florida in 2020-21.
Cleveland Clinic: 1,285 beds. The Cleveland Clinic is a nonprofit health system integrating hospital care, research and education. The main campus ranks among the U.S. News & World Report‘s Honor Roll of the top 20 hospitals in the nation. As of Sept. 15, the health system reported 4,520 physicians and scientists and 17,000 registered nurses and advanced practice providers.
Mayo Clinic Hospital-Saint Marys Campus (Rochester, Minn.): 1,265 beds. Saint Marys is part of Mayo Clinic Hospital-Rochester, which comprises Saint Marys and the 794-bed Methodist campus. Founded in 1889 as a faith-based hospital, St Marys has grown to include a children’s hospital, psychiatric treatment center and general clinical research center.
Atrium Health Carolinas Medical Center (Charlotte, N.C.): 1,211 beds. Atrium Health’s Carolinas Medical Center is the flagship hospital for Charlotte-based Atrium Health and has two locations less than 2 miles apart. The hospital has more than 1,100 physicians and care providers and is the region’s only level 1 trauma center. The hospital provides training for more than 360 physicians, dentists and pharmacists in 40 specialties and subspecialties.
Memorial Hermann-Texas Medical Center (Houston): 1,182 beds. Founded in 1925, Memorial Hermann-Texas Medical Center, which includes Children’s Memorial Hermann Hospital, is one of two level 1 adult trauma centers in Houston and the only level 1 trauma center for both adult and pediatric patients in Houston. Together with the hospital’s academic partners at McGovern Medical School at The University of Texas Health Science Center at Houston, which provides access to more than 1,800 physicians, Memorial Hermann-TMC serves more than 90,000 adult and pediatric patients per year in its 24/7 emergency and trauma center.
The Johns Hopkins Hospital (Baltimore): 1,162 beds. Johns Hopkins features 33 operating rooms, with 14 dedicated to general and neurosurgery, as well as the Sheik Zayed Tower with 355 inpatient rooms for adult care. The hospital’s Bloomberg Children’s Hospital has 205 private inpatient rooms and level 1 pediatric trauma services. U.S. News & World Report ranked the hospital No. 3 in the nation in 2020-21.
UAB Hospital (Birmingham, Ala.): 1,157 beds. UAB Hospital has more than 1,500 physicians and 17,642 employees. The academic medical center reports nearly 92,000 discharges annually and more than 1.6 million outpatient clinic visits. The hospital’s facilities include a 430,000- square-foot clinic, women and infant center, an eye hospital and a rehabilitation center. Healthgrades honored the hospital with the Outstanding Patient Experience Award from 2017 to 2019, and it was named one of America’s best hospitals in 2020.
Mount Sinai Hospital (New York City): 1,134 beds. Mount Sinai Hospital is the flagship hospital of an eight-hospital health system which includes 7,480 physicians. The hospital was designated with the highest recognition in the 2020-21 “Best Hospitals” issue of U.S. News & World Report, and the hospital is nationally ranked in six specialties including geriatrics, cardiology/heart surgery, gastroenterology/GI surgery, diabetes/endocrinology, nephrology, and neurology/neurosurgery.
Beaumont Hospital–Royal Oak (Mich.): 1,131 beds. Opened in 1955 as a 238-bed hospital, Beaumont has grown into a major academic and referral center that includes 7,930 employees and 2,110 physicians. The hospital is a level 1 adult trauma center and level 2 pediatric trauma center with 55 residency and fellowship programs. Beaumont is the exclusive clinical partner of the Oakland University William Beaumont School of Medicine, with more than 1,400 Beaumont doctors on faculty.
Saint Francis Hospital (Tulsa, Okla.): 1,112 beds. Saint Francis is a nonprofit Catholic health system that includes a 1,112-bed tertiary care center with a children’s hospital and level 4 neonatal intensive care unit. The health system has more than 1,000 physicians, 10,000 employees and 700 volunteers.
Miami Valley Hospital (Dayton, Ohio): 1,101 beds. Miami Valley Hospital opened in 1890 and has grown into a three-hospital system with a level 1 trauma center. U.S. News & World Report ranked Miami Valley Hospital No. 6 in Ohio for 2019-20. The hospital also earned recognition from Healthgrades among the America’s 100 Best Hospitals for three consecutive years.
UF Health Shands Hospital (Gainesville, Fla.): 1,095 beds. UF Health Shands Hospital has 1,209 physicians and more than 9,000 skilled nursing and support staff members. The hospital reported 56,557 admissions in 2019 and 10,922 employees. U.S. News & World Report’s 2020-21 Best Hospitals survey ranked it as the No. 1 hospital in Florida, with nine medical specialties in the nation’s Top 50, more than any other hospital in the state.
OhioHealth Riverside Methodist Hospital (Columbus): 1,095 beds. Serving patients since 1891, OhioHealth Riverside Methodist Hospital in Columbs is a teaching hosptial and the largest hospital in OhioHealth’s system. Riverside Methodist is recognized locally, regionally and nationally for quality healthcare and ranked among the nation’s best hospitals.
Baylor University Medical Center (Dallas): 1,042 beds. In the 2019 fiscal year, Baylor University Medical Center recorded 39,217 admissions, 101,080 emergency room visits and 122,255 outpatient visits. The hospital has 1,057 physicians and 4,943 employees. The hospital also has more than 20 specialty centers and offers patients access to more than 150 national clinical trials.
Massachusetts General Hospital (Boston): 1,042 beds. Massachusetts General Hospital was ranked No. 2 in the nation by U.S. News & World Report in 2019-20. Founded in 1811, the hospital now treats more than 50,434 inpatients and 1.8 million outpatients annually. The hospital also records more than 111,524 ER visits annually and its surgeons perform more than 42,000 procedures.
Tampa (Fla.) General Hospital: 1,006 beds. Tampa General Hospital serves a population of 4 million people in West Central Florida. The nonprofit hospital has more than 8,000 employees, is the primary teaching hospital for USF Health Morsani College of Medicine and has 400 residents and fellows assigned to it. It is a level 1 trauma center and its organ transplant center surgeons have performed more than 10,000 adult solid organ transplants.
Vanderbilt University Hospital (Nashville, Tenn.): 1,000 beds. Vanderbilt University Hospital serves around 65,000 inpatients per year. Physicians in the department of medicine clinics see more than 718,000 outpatient visits annually.
Vidant Medical Center (Greenville, N.C.): 974 beds. Vidant Medical Center provides medical services to more than 1.4 million patients annually across 29 counties. The hospital is a level 1 trauma center and the flagship teaching hospital for Brody School of Medicine at East Carolina University. The hospital received the Mission: Lifeline Gold STEMI Receiving Center Quality Achievement Award and NSTEMI Gold Quality Achievement Award from the American Heart Association in August.
Huntsville (Ala.) Hospital: 971 beds. Huntsville Hospital is a regional referral center for northern Alabama and southern Tennessee. It is the flagship facility for Huntsville Hospital Health System, which includes additional hospitals across Tennessee. Systemwide, Huntsville has 2,200 patient beds and 15,000 employees.
Duke University Hospital (Durham, N.C.): 957 beds. Duke University Hospital has 51 operating rooms and a nine-OR ASC. The nonprofit hospital has earned the Healthcare Equality Index Leader recognition from the Human Rights Campaign in 2020 and a Hospital Safety Grade of A from 2012 to 2020. U.S. News & World Report also named the hospital among the top 20 hospitals in the nation for 2019-20.
Houston Methodist Hospital: 952 beds. Houston Methodist Hospital is a nonprofit, faith-based academic medical center that is the flagship location for one of Houston’s largest healthcare systems. The hospital had more than 45,500 emergency room visits, 381,585 outpatient visits and nearly 42,000 admissions in 2019.
Orlando (Fla.) Regional Medical Center: 941 beds. Orlando Regional Medical Center (ORMC) is the flagship hospital for Orlando Health, providing medical care, rehabilitation and a brain injury rehab program. ORMC is also a level 1 trauma center, serving more than 425,000 inpatients and outpatients per year. In the winter 2019 hospital safety grades released by the patient-safety advocates at The Leapfrog Group, ORMC had back-to-back As, its fifth from the last six grading periods. Grades are based on a point system that calculates numerical scores for nearly 30 healthcare measures, including infections, practices to prevent errors, safety problems and communication between clinicians and patients.
Inova Fairfax Hospital (Falls Church, Va.): 923 beds. The Inova Fairfax Hospital campus includes a children’s hospital and is the flagship location of the Inova Heart and Vascular Institute. The hospital is a level 1 trauma center and teaching facility for Virginia Commonwealth University in Richmond and Georgetown in Washington, D.C., among others. The hospital also has partnerships with seven schools of pharmacy along the East Coast and in the Midwest.
MedStar Washington Hospital Center: 912 beds. MedStar Washington Hospital Center is a nonprofit, teaching and research hospital that recorded nearly 444,000 inpatient and outpatient visits last year. The hospital has a medical, dental and surgical staff with around 1,685 team members and is the founding site for the MedStar Heart & Vascular Institute. In 2020-21, U.S. News & World Report honored the hospital with a national ranking for its cardiology and heart surgery program.
Thomas Jefferson University Hospital (Philadelphia): 908 beds. Thomas Jefferson University Hospital is the flagship facility of Jefferson Health. As of June 2019, the hospital reported 39,122 inpatient visits and 1.3 million outpatient visits annually. The hospital has around 2,741 physicians and practitioners and 9,604 employees.
Christiana Hospital (Newark, Del.): 906 beds. ChristianaCare’s Christiana Hospital is a 1.3 million-square-foot hospital that serves as a level 1 trauma center. The teaching hospital has more than 1,400 physicians and surgeons as active members of the medical staff. Its Center for Heart & Vascular Health hosts nearly 1,000 open heart surgeries per year and includes about 50 clinical trials annually.
Medical City Dallas: 899 beds. Medical City Dallas includes more than 100 specialties and 1,463 active physicians. Medical City Dallas treats adult and pediatric patients who travel from more than 75 countries for treatment. The hospital was ranked No. 7 by U.S. News & World Report 2020-21 among hospitals in Dallas-Fort Worth.
Northwestern Memorial Hospital (Chicago): 894 beds. Northwestern Memorial Hospital is the primary teaching affiliate of the Feinberg School of Medicine. The hospital is the flagship facility of Northwestern Medicine, which includes more than 4,400 aligned physicians and hundreds of locations in the Chicago area. In 2019-20, U.S. News & World Report ranked Northwestern Memorial Hospital among the top 10 hospitals in the nation.
Cedars-Sinai Medical Center (Los Angeles): 886 beds. Founded in 1902 as a 12-bed hospital, Cedars-Sinai has expanded into a health system with more than 40 locations around Los Angeles and more than 4,500 physicians and nurses. The hospital reports 50,646 admissions and 802,354 outpatient visits per year. It also supports 14,121 full-time employees and a 2,112-member medical staff. Research is also prioritized at Cedars-Sinai, with 2,145 research projects systemwide.
Wake Forest Baptist Medical Center (Winston-Salem, N.C.): 885 beds. The Wake Forest Baptist Medical Center, part of Wake Forest Baptist Health, is an academic medical center that serves residents of 24 counties in North Carolina and southwest Virginia. It was founded in 1902 as a medical school for Wake Forest College and grew to a five-hospital health system with more than 19,220 employees, 2,100 physicians and more than 300 primary care and specialty clinics.
Parkland Health and Hospital System (Dallas): 882 beds. Opened in 1894, Parkland Health and Hospital System has grown into an organization with 20 community-based clinics and is the primary teaching hospital for the University of Texas Southwestern Medical Center. The public hospital reports more than 1 million outpatient visits every year and is a level 1 trauma center.
Hartford (Conn.) Hospital: 867 beds. Hartford Hospital is a regional referral center that includes a 114-bed mental health facility and a 104-bed long-term care facility. The hospital has more than 1,280 physicians and dentists on its medical staff and more than 7,000 nurses and staff members.
Lakeland (Fla.) Regional Health Medical Center: 864 beds. Lakeland Regional Health Medical Center is part of a health system that includes a 600-member medical staff and more than 25 specialties. The hospital reports around 209,650 emergency department visits per year and more than 1,300 trauma visits annually. U.S. News & World Report named Lakeland Regional Health Medical Center among the top 25 hospitals in Florida for 2019-20.
NewYork-Presbyterian/Weill Cornell Medical Center (New York City): 862 beds. NewYork-Presbyterian/Weill Cornell Medical Center is an academic medical center and part of NewYork-Presbyterian, an integrated academic healthcare system with 10 hospital campuses and more than 200 primary and specialty care clinics and medical groups.
Mercy Hospital St. Louis: 859 beds. Mercy Hospital is a level 1 trauma center and level 3 neonatal intensive care unit. The hospital has earned a spot on the IBM Watson Health 100 Top Hospitals list and a CMS 5-Star Hospital rating. Mercy Hospital St. Louis has 317 locations and had 1 million outpatient visits and 89,054 emergency visits during fiscal year 2018.
Novant Health Forsyth Medical Center (Winston-Salem, N.C.): 859 beds. Forsyth Medical Center, along with Novant Health Medical Park Hospital, hosts around 40,000 surgical procedures per year. The hospital was founded in 1887 and has grown into an award-winning institution. It has earned the Clinical Excellence Award from VHA and the Quality Gold Plus Achievement Award from the American Heart Association.
Aurora St. Luke’s Medical Center of Aurora Health Care (Milwaukee): 854 beds. St. Luke’s Medical Center partnered with Samaritan Medical Center in 1984 to form Aurora Health Care, which has grown to include more than 15 hospitals and 150 clinics. The system merged with Advocate Health Care in 2018.
Texas Heart Institute at Baylor St. Luke’s Medical Center (Houston): 850 beds. Texas Heart Institute at Baylor St. Luke’s Medical Center has recorded more than 250,000 cardiac catheterizations, 115,000 open heart surgeries and 1,450 heart transplants since its inception. Its specialists treat patients from more than 75 countries.
NYU Langone Hospitals (New York City): 844 beds. NYU Langone treats patients from around the world. The hospital in Manhattan includes 96 operating rooms and an advanced critical care unit. The hospital’s labor and delivery unit reports 5,500 deliveries over the last year.
Baptist Health – Little Rock (Ark.): 843 beds. Baptist Health – Little Rock is a faith-based hospital with a heart, orthopedic and women’s health center. It is part of the Arkansas-based Baptist Health system.
Montefiore Hospital – Moses Campus (Bronx, N.Y.): 816 beds. Montefiore Hospital – Moses Campus is part of Montefiore Medical Center, with more than 100 years of history. The health system has 10 hospitals as well as over 215 locations and is the academic medical center and University Hospital for Albert Einstein College of Medicine.
Methodist Hospital (San Antonio): 811 beds. Opened in 1963, Methodist Hospital provides an array of services including cardiology, oncology, emergency medicine, neurosciences, maternity care, gynecology and orthopedics. Methodist earned a Hospital Safety Grade of A from The Leapfrog Group. The hospital is part of Methodist Healthcare, a private health system.
University of Maryland Medical Center (Baltimore): 806 beds. The University of Maryland Medical Center is the flagship hospital of the University of Maryland Medical System in Baltimore. It has more than 10,000 employees and 1,000 faculty physicians. In 2019, the hospital reported more than 442,000 outpatient visits and more than 33,000 admissions at both its downtown and midtown campuses. UMMC has earned the Beacon Award for Excellence, a national award for critical care.
UNC Medical Center (Chapel Hill, N.C.): 803 beds. UNC Medical Center has a staff of more than 7,100 employees, including a 1,100-person medical staff, and treats more than 37,000 patients each year. The hospital serves all 100 North Carolina counties and its satellite locations provide care to more than 800,000 patients each year. The hospital also includes the Lineberger Comprehensive Cancer Center, a National Cancer Institute-designated facility.
Ochsner Medical Center (New Orleans): 775 beds. Ochsner Medical Center is a member of Ochsner Health System, a 40-hospital health system that has more than 4,500 employed and affiliated physicians as well as 26,000 employees. The nonprofit academic medical center recently expanded its campus increasing capacity to offer more specialty care services, such as cardiology, neuroscience, transplant and surgery services.
The University of Kansas Hospital (Kansas City): 750 beds. University of Kansas Hospital is an academic medical center with 23 accredited residency programs and more than 30 research institutes and centers. It serves as a level 1 trauma center and has 40 operating rooms.
Mayo Clinic Hospital – Methodist Campus (Rochester, Minn.): 794 beds. Mayo Clinic Hospital – Methodist Campus is an integrated medical center that includes a transplant program as well as several specialists. The hospital has 37 operating rooms as well as a women’s cancer program and vascular center.
ProMedica Toledo (Ohio) Hospital: 794 beds. ProMedica Toledo Hospital serves a 27-county area in northwest Ohio and southeast Michigan. The hospital has more than 4,800 employed healthcare professionals as well as 1,000 affiliated physicians. Healthgrades honored the hospital as one of the 50 Best Hospitals in the nation from 2018 to 2019.
Brigham and Women’s Hospital (Boston): 793 beds. Brigham and Women’s Hospital is the flagship institution for Brigham Health, which has more than 1,000 inpatient beds and 1,200 physicians providing care at its locations. Brigham and Women’s Hospital is also a teaching affiliate of Boston-based Harvard Medical School, and the health system has nearly 5,000 scientists and physician investigators.
Lehigh Valley Hospital – Cedar Crest (Allentown, Pa.): 780 beds. Lehigh Valley Hospital-Cedar Crest is the flagship hospital of Lehigh Valley Health Network. It is a level 1 trauma center and has a children’s ER, certified for level 2 pediatric trauma. The hospital is a member of the Memorial Sloan Kettering Cancer Alliance.
UMass Memorial Medical Center – Memorial Campus (Worcester, Mass.): 773 beds. UMass Memorial Medical Center is part of a three-hospital health system that has 1,392 physicians on the active medical staff and 9,573 total employees.
Hackensack University Medical Center: 771 beds. Hackensack Meridian Health’s Hackensack University Medical Center is a nonprofit teaching hospital that was founded in 1888. During the COVID-19 pandemic, the hospital grew to around 950 beds to accommodate patients with respiratory illness.
Albany (N.Y.) Medical Center: 766 beds. Albany Medical Center is part of Albany Med, a four-hospital system with more than 450 physicians. The health system serves more than 2 million people in a 25-county area.
NewYork-Presbyterian/Columbia University Irving Medical Center (New York City): 738 beds. NewYork-Presbyterian/Columbia University Irving Medical Center is an academic medical center and part of NewYork-Presbyterian, an integrated academic healthcare system with 10 hospital campuses and more than 200 primary and specialty care clinics and medical groups. The health system has around 47,000 employees and affiliated physicians.
North Shore University Hospital (Manhasset, N.Y.): 738 beds. North Shore University Hospital has more than 4,000 physicians delivering a wide range of specialty and general healthcare. The hospital, part of New Hyde Park, N.Y.-based Northwell Health, has a level 1 trauma center in an emergency department that serves 90,000 patients per year. The hospital has earned the Silver Beacon Award for Excellence from the American Association of Critical-Care Nurses and earned recognition from U.S. News & World Report among the 50 best hospitals in the nation for cardiac care in 2018-19.
Broward Health Medical Center (Fort Lauderdale, Fla.): 716 beds. Broward Health Medical Center is a nonprofit hospital and level 1 trauma center. The hospital has 800 physicians delivering care.
Reading Hospital (West Reading, Pa.): 714 beds. Reading Hospital is the flagship facility of Tower Health. It includes the Reading HealthPlex, McGlinn Cancer Institute and Miller Regional Heart Center. The hospital has more than 1,000 physicians and 49 locations.
University Hospital (Ann Arbor, Mich.): 695 beds. University Hospital opened its doors in 1986 and has grown into a 695-bed institution. It is a member of the Michigan Medicine health system and the campus’s 1.7 million square feet house clinical laboratories, operating rooms and inpatient care.
Hospitals across the U.S. are beginning to suspend elective procedures to respond to an uptick in hospitalized COVID-19 patients.
Below is a breakdown of 66 hospitals postponing or canceling the procedures to free up space, ensure proper staffing or enough protective gear to care for COVID-19 patients:
1. Mercy Health Youngstown (Ohio) will indefinitely suspend elective procedures that require an inpatient admission starting Nov. 26, according to the Tribune Chronicle.
2. Prescot, Ariz.-based Yavapai Regional Medical Center, which recently joined Dignity Health, will limit elective procedures effective Nov. 26 to Dec. 4, according to The Daily Courier.
3. South Bend, Ind.-based Beacon Health System is suspending nonemergency surgeries to free up bed space and staff to care for a surge in COVID-19 cases, according to WSBT. The surgeries affected include those that require an inpatient stay.
4. Citing a spike in COVID-19 cases, Goshen (Ind.) Health is suspending nonurgent surgeries, according to WSBT.
5. Stormont Vail Health in Topeka, Kan., is rescheduling some elective surgeries that require overnight stays to free up bed space, according to local news station WIBW.
6. UW Medicine in Seattle will suspend nonemergency surgeries that require an inpatient hospital stay, effective Nov. 23 through Feb. 1.
7. Mercy Hospital South in St. Louis plans to delay some nonurgent procedures that require longer hospital stays amid a spike in COVID-19 hospitalizations, according to the St. Louis Post-Dispatch.
8. Metro Health-University of Michigan Health in Wyoming, Mich., has delayed some surgeries that require an inpatient stay, according to MiBiz.
9. Albuquerque, N.M.-based Presbyterian Healthcare Services is canceling nonurgent surgeries that require hospitalization, according to local news station KBOB. The health system said it will postpone those surgeries that can be delayed for six weeks or longer safely.
10. HSHS Sacred Heart Hospital in Eau Claire, Wis., is postponing electives on a case-by-case basis amid a surge in COVID-19 cases, according to The Leader-Telegram.
11. IU Health Methodist Hospital in Indianapolis has started to reduce the amount of elective procedures it will perform, while still trying to catch up on those that were postponed during the initial surge, according to MedPageToday.
12. Carson Tahoe Hospital in Carson City, Nev., has delayed non-time sensitive surgeries for a few weeks to free up space and staff to care for a surge in COVID-19 hospitalizations, according to local station News 4.
13. The 267-bed Mercy Health Muskegon (Mich.) has begun to delay elective surgeries as needed amid an influx of COVID-19 cases, according to MiBiz.
14. Buffalo, N.Y.-based Catholic Health will halt all inpatient elective surgeries that require an overnight stay for two weeks amid a COVID-19 hospitalization surge, according to Buffalo News. The healthcare system will start rescheduling procedures Nov. 21, and reevaluate if an extension is needed Dec. 5.
15. Chicago-based Northwestern Medicine will reduce the number of nonemergency surgeries it performs to help preserve bed capacity and staff to help care for a surge in COVID-19 cases, according to the Northwest Herald.
16. Morris (Ill.) Hospital and Healthcare Centers postponed some inpatient surgeries requiring overnight stays the week of Nov. 16 due to a bed shortage exacerbated by the rise in COVID-19 cases, according to NBC Chicago.
17. Memorial Community Hospital and Health System in Blair, Neb., is limiting elective surgeries requiring an overnight hospital stay for several weeks to preserve bed capacity and ensure proper staffing levels to care for the influx of COVID-19 cases, according to the Pilot-Tribune & Enterprise.
18. Spectrum Health in Grand Rapids, Mich., is deferring elective surgeries requiring an overnight hospital stay, according to Michigan Radio. The deferral rate is about 10 percent, according to the report.
19. Avera St. Mary’s Hospital in Pierre, S.D., is postponing nonemergency procedures so staff can care for the influx of COVID-19 cases and respond to emergent needs, according to DRGNews.
20. Salt Lake City-based Intermountain Healthcarewill postpone some surgeries that require an inpatient admission to free up beds, preserve supplies and free up providers amid a surge in COVID-19 hospitalizations. The hospital system will only delay those that can be safely postponed.
21. Froedtert Health in Wauwatosa, Wis., will delay non-urgent surgeries that require an inpatient admission post-surgery in an effort to free up staff and beds amid the coronavirus case surge in Wisconsin, according to local news stationTMJ4. The hospitals are located in Wauwatosa, Menomonee Falls and West Bend.
22. Memorial Hospital in Aurora, Neb., has suspended elective surgeries that take place at its Wortman Surgery Center to dedicate staff to inpatient and emergency care.
23. Minneapolis-based Allina Health is delaying some non-urgent procedures at three of its hospitals until at least Nov. 27, according to The Star Tribune. The delays will affect non-urgent procedures that require an overnight hospital stay.
24. Bloomington, Minn.-based HealthPartners has started postponing some total joint surgeries, including hip or knee replacements, at three Minnesota hospitals, according to The Twin Cities Business Journal. The affected hospitals are Methodist Hospital in St. Louis Park, Regions Hospital in St. Paul and Lakeview Hospital in Stillwater.
25. Southern Illinois Healthcare, a two-hospital system based in Carbondale, will reduce its elective surgery volume by about 50 percent as more people seek inpatient care for COVID-19, according to The Southern Illinoisan.The surgeries affected by the delay include those that require an overnight hospital stay.
26. University of Cincinnati Health activated surge operations Nov. 16, requiring a 50 percent reduction in elective inpatient surgeries and procedures across the health system, according to local news station WLWT.
27. Rochester, Minn.-based Mayo Clinic has started scaling back elective care to ensure it can care for patients with emergent needs and a high influx of COVID-19 patients, according to The Post Bulletin.
28. Citing a 1,500 percent increase in COVID-19 hospitalizations between Nov. 1 and Nov. 17, Lake Health in Concord Township, Ohio, is pausing elective surgeries that require an overnight stay, according to The News-Herald.The pause will continue through Nov. 20, but the system will reevaluate if the pause needs to be extended on a weekly basis.
29. Cook County Health, the public hospital system based in Chicago, is suspending elective surgeries requiring inpatient stays, according to WBEZ.The decision was made to ensure adequate staffing to care for an influx in COVID-19 cases.
30. Urbana, Ill.-based Carle Foundation Hospital has canceled some elective procedures that require an overnight hospital stay in an effort to free up beds and staff to care for COVID-19 patients, according to The News Gazette.
31. Elkhart (Ind.) General Hospital stopped all elective surgeries Nov. 17 after more than 200 patients were admitted to its 144-bed hospital, according to The New York Times. Of those patients 90 were being treated with COVID-19. The hospital also diverted ambulances during this time.
32. Advocate Aurora Health, with dual headquarters in Milwaukee and Downers Grove, Ill., has started reducing elective procedures by 50 percent at some of its facilities, according to a Nov. 16 media briefing. The health system said that more hospitals will look into the option to postpone elective procedures later the week of Nov. 16.
33. The University of Kansas Health System in Kansas City started postponing some elective surgeries to free up inpatient beds Nov. 12.
34. St. Luke’s Health System in Boise, Idaho, will stop scheduling certain elective surgeries and procedures through Dec. 25, according to a company news release. The temporary delay starts Nov. 16. St. Luke’s medical centers in Boise, Meridian, Magic Valley and Nampa will also cancel elective cases requiring an overnight stay scheduled for the week of Nov. 16, according to the news release.
35. Citing an increased demand for inpatient beds, Ascension Genesys Hospital in Grand Blanc, Mich., will not schedule any new inpatient elective surgeries until at least Nov. 30. The hospital said it has asked surgeons to “thoughtfully examine” already scheduled cases requiring extended recovery through Nov. 30.
36. SSM Health St. Mary’s Hospital in Madison began rescheduling nonemergent surgeries to free up intensive care unit bed space, according to local news station NBC 15.
37. Cedar Rapids, Iowa-based Mercy Medical Center will reduce elective surgery cases through Nov. 20. It also temporarily stopped scheduling new elective procedures.
38. Columbia Memorial Hospital in Astoria, Ore., will reduce some elective procedures due to an increase in COVID-19 cases, according to the Cannon Beach Gazette.
39. St. Louis-based BJC HealthCarewill postpone some elective surgery cases at all 15 of its hospitals and ambulatory care settings starting Nov. 16. The surgery postponement will last eight weeks. The announcement comes just one week after the health system started rescheduling nonemergency surgeries at four of its hospitals.
40. Citing a significant increase in COVID-19 hospitalizations, Cleveland Clinic said it will postpone some nonemergency surgeries. Cleveland Clinic said it will reschedule nonessential surgical cases that require an inpatient stay at its hospitals in Ohio through Nov. 20. It will reassess its scheduled surgical cases daily to determine if more cases need to be delayed.
41. Baxter County Regional Medical Center in Mountain Home, Ark., said Nov. 11 it will begin postponing nonemergency surgeries. The hospital will only defer procedures requiring an overnight hospital stay in order to free up beds for COVID-19 patients.
42. Portland, Ore.-based Legacy Healthwill reduce the number of elective procedures requiring an overnight hospital stay by 25 percent.
“We will monitor the situation and adjust as needed,” Trent Green, Legacy Health COO, wrote in an email to staff. “If the number of hospitalized patients continues to grow, we may cancel more surgeries. As hospital volumes lower, we will add back elective surgeries.”
43. Kaiser Permanente Northwest, which has hospitals in Oregon and southwest Washington state, is implementing a “scheduling pause” at some of its Oregon medical centers through Dec. 31.
44. Portland-based Oregon Health & Sciences Universityis implementing voluntary elective surgery deferrals. The hospital system will evaluate surgical cases daily to ensure it has the appropriate capacity to care for all patients.
45. Aurora, Colo.-based UCHealthbegan postponing some nonemergency surgeries due to a surge in COVID-19 hospitalizations. The health system will defer nonemergent surgeries that require inpatient admission. The health system began postponing some of those surgeries the week of Nov. 2.
46. As of Nov. 11, Grand Rapids, Mich.-based Spectrum Health has 14 hospitals nearing capacity amid a surge of COVID-19 cases. As a result it is starting to delay inpatient surgeries that require overnight stays.
47. Community Memorial Hospital in Cloquet, Minn., has halted some elective surgeries to free up beds amid a surge in hospitalizations.
48. Sarah Bush Lincoln, a 145-bed hospital in Mattoon, Ill., is postponing most inpatient elective surgeries due to bed capacity constraints. The hospital said it will make the decision on whether to postpone a surgery on a case-by-case basis.
49. Memorial Health System in Springfield, Ill., will begin delaying some nonurgent surgeries Nov. 16.
50. Evanston, Ill.-based NorthShore University HealthSystem, has started evaluating elective surgeries on a case-by-case basis and delaying those that can be postponed safely.
51. UnityPoint Health Meriter in Madison, Wis., is rescheduling nonemergent surgeries that require overnight stays to save beds for COVID-19 patients. The hospital has seen a “significant” uptick in COVID-19-related hospitalizations, with about one-third of UnityPoint Meriter’s beds occupied by patients with the virus.
52. St. Luke’s, a two-hospital system in Duluth, Minn., is postponing nonemergency surgeries amid a surge in COVID-19 patients. The health system said it will only delay surgeries that require an overnight stay and can be rescheduled safely.
53. Omaha, Neb.-based Methodist Health Systembegan postponing elective surgeries at its flagship hospital Oct. 29, president and CEO Steve Goeser told Becker’s. It is reviewing the surgery schedule to determine which ones can be postponed safely.
54. Omaha-based Nebraska Medicineis limiting nonurgent procedures due to a rise in COVID-19 hospitalizations. The health system said that it has enough beds, but high-level intensive care unit providers “aren’t an infinite resource.”
55. CHI Health in Omaha, Neb., said that some nonurgent procedures will be postponed amid the COVID-19 resurgence. By postponing some surgeries, CHI Health said it aims to free up beds and capacity for patients.
56. Sanford Health, a 46-hospital system based in Sioux Falls, S.D., will begin rescheduling some nonemergency inpatient surgeries that require an overnight hospital stay due to an influx of COVID-19 patients.
57. Bryan Health, based in Lincoln, Neb., will begin scaling back elective surgeries requiring an overnight hospitalization due to a rise in COVID-19 cases. The system said it will decrease elective surgeries requiring overnight stay by 10 percent for the week of Nov. 2 to ensure it is able to care for COVID-19 patients and perform essential surgeries.
58. Mayo Clinic Health Systembegan deferring elective procedures at its hospitals in Northwest Wisconsin Oct. 31 amid an escalation of COVID-19 cases. The health system did not say when elective procedures will restart. The Mayo Clinic Health System has clinics, hospitals and other facilities across Iowa, Minnesota and Wisconsin.
59. Madison, Wis.-based UW Health is postponing a small number of elective procedures to free up bed capacity to care for COVID-19 patients, according to WKOW. Jeff Pothof, MD, UW Health’s chief quality officer, said that patients may be asked to push back a non-emergency procedure by about a week.
60. Saint Vincent Hospital in Erie, Pa., will postpone a small number of elective procedures after some patients and caregivers tested positive for COVID-19. The hospital did not specify the number of patients and staff who tested positive.
61. Johnson City, Tenn.-based Ballad Healthwill begin deferring elective procedures at three of its Tennessee hospitals due to a spike in COVID-19 hospitalizations. On Oct. 26, Ballad began rescheduling up to 25 percent of elective services at Holston Valley Medical Center in Kingsport, Tenn. Procedures are also expected to begin being deferred at Bristol Regional Medical Center and Johnson City Medical Center.
62. Maury Regional Medical Center in Columbia, Tenn., will suspend elective procedures requiring an overnight stay for two weeks. Hospital leadership will re-evaluate the feasibility of elective surgeries by Nov. 9.
63. Cookeville (Tenn.) Regional Medical Center said Oct. 26 it suspended elective procedures requiring an overnight stay after it was caring for a record high of 71 COVID-19 patients, according to WKRN.
64. Salt Lake City-based University of Utah Hospitalcanceled elective procedures after its intensive care unit hit capacity on Oct. 16. The hospital said it needed to postpone the elective care to allocate staff to care for critically ill patients.
65. Sanford Health in Sioux Falls, S.D., will stop scheduling new elective surgery cases requiring an overnight stay, according to system CMO Mike Wilde, MD. New elective cases requiring an overnight stay were not scheduled for Oct. 19-23, but previously scheduled elective surgeries were performed.
66. Billings (Mont.) Clinic began evaluating each surgical case for urgency in late September. It is postponing those it says can wait, according to The Wall Street Journal.
CMS is giving hospitals facing a surge of COVID-19 patients expanded flexibility to care for Medicare patients in their homes, the department announced Nov. 25.
The new Acute Hospital Care At Home program will require in-person screening protocols to assess both medical and non-medical factors, including working utilities, before care can begin at home. Medicare patients will be admitted into the program from emergency departments and inpatient hospital beds.
Once at-home care begins, a registered nurse will evaluate each patient every day either in person or remotely, and either registered nurses or mobile integrated health paramedics will have two in-person visits daily based on the patient’s nursing plan and hospital policies.
CMS approved the following six health systems with extensive experience providing acute hospital care at home to immediately participate in the program:
Chinese investor Tianqiao Chen and his group of companies have a 14.96 percent stake in Franklin, Tenn.-based Community Health Systems after recently selling nearly 4.6 million shares of the company, according to a Securities and Exchange Commission filing.
Mr. Chen and his Shanda Group company affiliates sold the shares Nov. 23 for between $8.66 and $9.08 per share, bringing in a total of $39.8 million. The move comes after he sold 5 million shares of CHS from Nov. 10-12 for $41.46 million.
Mr. Chen, a pioneer in China’s online gaming industry, began buying up shares of CHS in 2016. The last public comment the investor made about CHS was in 2018, when Shanda Group said it had a “good relationship” with CHS and supported the company’s strategy and management team.
On her day off not long ago, emergency room nurse Jane Sandoval sat with her husband and watched her favorite NFL team, the San Francisco 49ers. She’s off every other Sunday, and even during the coronavirus pandemic, this is something of a ritual. Jane and Carlos watch, cheer, yell — just one couple’s method of escape.
“It makes people feel normal,” she says.
For Sandoval, though, it has become more and more difficult to enjoy as the season — and the pandemic — wears on. Early in the season, the 49ers’ Kyle Shanahan was one of five coaches fined for violating the league’s requirement that all sideline personnel wear face coverings. Jane noticed, even as coronavirus cases surged again in California and across the United States, that Levi’s Stadium was considering admitting fans to watch games.
But the hardest thing to ignore, Sandoval says, is that when it comes to coronavirus testing, this is a nation of haves and have-nots.
Among the haves are professional and college athletes, in particular those who play football. From Nov. 8 to 14, the NFL administered 43,148 tests to 7,856 players, coaches and employees. Major college football programs supply dozens of tests each day, an attempt — futile as it has been — to maintain health and prevent schedule interruptions. Major League Soccer administered nearly 5,000 tests last week, and Major League Baseball conducted some 170,000 tests during its truncated season.
Sandoval, meanwhile, is a 58-year-old front-line worker who regularly treats patients either suspected or confirmed to have been infected by the coronavirus. In eight months, she has never been tested. She says her employer, California Pacific Medical Center, refuses to provide testing for its medical staff even after possible exposure.
Watching sports, then, no longer represents an escape from reality for Sandoval. Instead, she says, it’s a signal of what the nation prioritizes.
“There’s an endless supply in the sports world,” she says of coronavirus tests. “You’re throwing your arms up. I like sports as much as the next person. But the disparity between who gets tested and who doesn’t, it doesn’t make any sense.”
This month, registered nurses gathered in Los Angeles to protest the fact that UCLA’s athletic department conducted 1,248 tests in a single week while health-care workers at UCLA hospitals were denied testing. Last week National Nurses United, the country’s largest nursing union, released the results of a survey of more than 15,000 members. About two-thirds reported they had never been tested.
Since August, when NFL training camps opened, the nation’s most popular and powerful sports league — one that generates more than $15 billion in annual revenue — has conducted roughly 645,000 coronavirus tests.
“These athletes and teams have a stockpile of covid testing, enough to test them at will,” says Michelle Gutierrez Vo, another registered nurse and sports fan in California. “And it’s painful to watch. It seemed like nobody else mattered or their lives are more important than ours.”
Months into the pandemic, and with vaccines nearing distribution, testing in the United States remains something of a luxury. Testing sites are crowded, and some patients still report waiting days for results. Sandoval said nurses who suspect they’ve been exposed are expected to seek out a testing site on their own, at their expense, and take unpaid time while they wait for results — in effect choosing between their paycheck and their health and potentially that of others.
“The current [presidential] administration did not focus on tests and instead focused on the vaccine,” says Mara Aspinall, a professor of biomedical diagnostics at Arizona State University. “We should have focused with the same kind of ‘warp speed’ on testing. Would we still have needed a vaccine? Yes, but we would’ve saved more lives in that process and given more confidence to people to go to work.”
After a four-month shutdown amid the pandemic’s opening wave, professional sports returned in July. More than just a contest on television, it was, in a most unusual year, a symbol of comfort and routine. But as the sports calendar has advanced and dramatic adjustments have been made, it has become nearly impossible to ignore how different everything looks, sounds and feels.
Stadiums are empty, or mostly empty, while some sports have bubbles and others just pretend their spheres are impermeable. Coaches stand on the sideline with fogged-up face shields; rosters and schedules are constantly reshuffled. On Saturday, the college football game between Clemson and Florida State was called off three hours before kickoff. Dodger Stadium, home of the World Series champions, is a massive testing site, with lines of cars snaking across the parking lot.
Sports, in other words, aren’t a distraction from a polarized nation and its response to a global pandemic. They have become a constant reminder of them.And when some nurses turn to sports for an attempt at escape, instead it’s just one more image of who gets priority for tests and, often, who does not.
“There is a disconnect when you watch sports now. It’s not the same. Covid changed everything,” says Gutierrez Vo, who works for Kaiser Permanente in Fremont, Calif. “I try not to think about it.”
Sandoval tries the same, telling herself that watching a game is among the few things that make it feel like February again. Back then, the coronavirus was a distant threat and the 49ers were in the Super Bowl.
That night, Sandoval had a shift in the ER, and between patients, she would duck into the break room or huddle next to a colleague checking the score on the phone. The 49ers were playing the Kansas City Chiefs, and Sandoval would recall that her favorite team blowing a double-digit lead represented the mightiest stress that day.
Now during shifts, Sandoval sometimes argues with patients who insist the virus that has infected them is a media-driven hoax. She masks up and wears a face shield even if a patient hasn’t been confirmed with the coronavirus, though she can’t help second-guessing herself.
“Did I wash my hands? Did I touch my glasses? Was I extra careful?” she says.
If Sandoval suspects she has been exposed, she says, she doesn’t bother requesting a test. She says the hospital will say there aren’t enough. So instead she self-monitors and loads up on vitamin C and zinc, hoping the tickle in her throat disappears. If symptoms persist, which she says hasn’t happened yet, she plans to locate a testing site on her own. But that would mean taking unpaid time, paying for costs out of pocket and staying home — and forfeiting a paycheck — until results arrive.
National Nurses United says some of its members are being told to report to work anyway as they wait for results that can take three to five days. Sutter Health, the hospital system that oversees California Pacific Medical Center, said in a statement to The Washington Post that it offers tests to employees whose exposure is deemed high-risk and to any employee experiencing symptoms. Symptomatic employees are placed on paid leave while awaiting test results, according to the statement.
“As long as an essential healthcare worker is asymptomatic,” Sutter’s statement read, “they can continue to work and self-monitor while awaiting the test result.”
Sandoval said employees have been told the hospital’s employee health division will contact anyone who has been exposed. Though she believes she’s exposed during every shift, Sandoval says employee health has never contacted her to offer a test or conduct contact tracing.
“If you feel like you need to get tested, you do that on your own,” she says. Sandoval suspects the imbalance is economic. In September, Forbes reported NFL team revenue was up 7 percent despite the pandemic. Last week Sutter Health reported a $607 million loss through the first nine months of 2020.
Sandoval tries to avoid thinking about that, so she keeps heading back to work and hoping for the best. Though she says her passion for sports is less intense now, she nonetheless likes to talk sports when a patient wears a team logo. She asks about a star player or a recent game. She says she is looking forward to the 49ers’ next contest and the 2021 baseball season.
Sometimes, Sandoval says, patients ask about her job and the ways she avoids contracting the coronavirus. She must be tested most every day, Sandoval says the patients always say.
And she just rolls her eyes and chuckles. That, she says, only happens if you’re an athlete.