Studies show healthcare affordability is an issue to voters as medical debt soars (KFF) and public disaffection for the “medical system” (per Gallup, Pew) plummets. But does it really matter to the hospitals, insurers, physicians, drug and device manufacturers and army of advisors and trade groups that control the health system?
Each sector talks about affordability blaming inflation, growing demand, oppressive regulation and each other for higher costs and unwanted attention to the issue.
Each play their victim cards in well-orchestrated ad campaigns targeted to state and federal lawmakers whose votes they hope to buy.
Each considers aggregate health spending—projected to increase at 5.4%/year through 2031 vs. 4.6% GDP growth—a value relative to the health and wellbeing of the population. And each thinks its strategies to address affordability are adequate and the public’s concern understandable but ill-informed.
As the House reconvenes this week joining the Senate in negotiating a resolution to the potential federal budget default October 1, the question facing national and state lawmakers is simple: is the juice worth the squeeze?
Is the US health system deserving of its significance as the fastest-growing component of the total US economy (18.3% of total GDP today projected to be 19.6% in 2031), its largest private sector employer and mainstay for private investors?
Does it deserve the legal concessions made to its incumbents vis a vis patent approvals, tax exemptions for hospitals and employers, authorized monopolies and oligopolies that enable its strongest to survive and weaker to disappear?
Does it merit its oversized role, given competing priorities emerging in our society—AI and technology, climate changes, income, public health erosion, education system failure, racial inequity, crime and global tension with China, Russia and others.
In the last 2 weeks, influential Republicans leaders (Burgess, Cassidy) announced plans to tackle health costs and the role AI will play in the future of the system. Last Tuesday, CMS announced its latest pilot program to tackle spending: the States Advancing All-Payer Health Equity Approaches and Development Model (AHEAD Model) is a total cost of care budgeting program to roll out in 8 states starting in 2026. The Presidential campaigns are voicing frustration with the system and the spotlight on its business practices intensifying.
So, is affordability to the federal government likely to get more attention?
Yes. Is affordability on state radars as legislatures juggle funding for Medicaid, public health and other programs?
Yes, but on a program by program, non-system basis.
Is affordability front and center in CMS value agenda including the new models like its AHEAD model announced last week? Not really.
CMS has focused more on pushing hospitals and physicians to participate than engaging consumers. Is affordability for those most threatened—low and middle income households with high deductible insurance, the uninsured and under-insured, those with an expensive medical condition—front of mind? Every minute of every day.
Per CMS, out-of-pocket spending increased 4.3% in 2022 (down from 10.4% in 2021) and “is expected to accelerate to 5.2%, in part related to faster health care price growth. During 2025–31, average out-of-pocket spending growth is projected to be 4.1% per year.” But these data are misleading. It’s dramatically higher for certain populations and even those with attractive employer-sponsored health benefits worry about unexpected household medical bills.
So, affordability is a tricky issue that’s front of mind to 40% of the population today and more tomorrow.
Legislation that limits surprise medical bills, requires drug, hospital and insurer price transparency, expands scope of practice opportunities for mid-level professionals, avails consumers of telehealth services, restricts aggressive patient debt collection policies and others has done little to assuage affordability issues for consumers.
Ditto CMS’ value agenda which is more about reducing Medicare spending through shared savings programs with hospitals and physicians than improving affordability for consumers. That’s why outsiders like Walmart, Best Buy and others see opportunity: they think patients (aka members, enrollees, end users) deserve affordability solutions more than lip service.
Affordability to consumers is the most formidable challenge facing the US healthcare industry–more than burnout, operating margins, reimbursement or alternative payment models. Today, it is not taken seriously by insiders. If it was, evidence would be readily available and compelling. But it’s not.
Issue: Medical debt negatively affects many Americans, especially people of color, women, and low-income families. Federal and state governments have set some standards to protect patients from medical debt.
Goal: To evaluate the current landscape of medical debt protections at the federal and state levels and identify where they fall short.
Methods: Analysis of federal and state laws, as well as discussions with state experts in medical debt law and policy. We focus on laws and regulations governing hospitals and debt collectors.
Key Findings and Conclusion: Federal medical debt protection standards are vague and rarely enforced. Patient protections at the state level help address key gaps in federal protections. Twenty states have their own financial assistance standards, and 27 have community benefit standards. However, the strength of these standards varies widely. Relatively few states regulate billing and collections practices or limit the legal remedies available to creditors. Only five states have reporting requirements that are robust enough to identify noncompliance with state law and trends of discriminatory practices. Future patient protections could improve access to financial assistance, ensure that nonprofit hospitals are earning their tax exemption, and limit aggressive billing and collections practices.
Introduction
Medical debt, or personal debt incurred from unpaid medical bills, is a leading cause of bankruptcy in the United States. As many as 40 percent of U.S. adults, or about 100 million people, are currently in debt because of medical or dental bills. This debt can take many forms, including:
past-due payments directly owed to a health care provider
ongoing payment plans
money owed to a bank or collections agency that has been assigned or sold the medical debt
credit card debt from medical bills
money borrowed from family or friends to pay for medical bills.
This report discusses findings from our review of federal and state laws that regulate hospitals and debt collectors to protect patients from medical debt and its negative consequences. First, we briefly discuss the impact and causes of medical debt. Then, we present federal medical debt protections and discuss gaps in standards as well as enforcement. Then, we provide an overview of what states are doing to:
strengthen requirements for financial assistance and community benefits
regulate hospitals’ and debt collectors’ billing and collections activities
limit home liens, foreclosures, and wage garnishment
develop reporting systems to ensure all hospitals are adhering to standards and not disproportionately targeting people of color and low-income communities.
(See the appendix for an overview of medical debt protections in all 50 states and the District of Columbia.)
Impact of Medical Debt
More than half of people in medical and dental debt owe less than $2,500, but because most Americans cannot cover even minor emergency expenses, this debt disrupts their lives in serious ways. Fear of incurring medical debt also deters many Americans from seeking medical care. About 60 percent of adults who have incurred medical debt say they have had to cut back on basic necessities like food or clothing, and more than half the adults from low-income households (less than $40,000) report that they have used up their savings to pay for their medical debt.
A significant amount of medical debt is either sold or assigned to third-party debt-collecting agencies, who often engage in aggressive efforts to collect on the debt, creating stress for patients. Both hospitals and debt collectors have won judgments against patients, allowing them to take money directly from a patient’s paycheck or place liens on a patient’s home. In some cases, patients have also lost their homes. Medical debt can also have a negative impact on a patient’s credit score.
Key Terms Related to Medical Debt
Financial assistance policy: A hospital’s policy to provide free or discounted care to certain eligible patients. Eligibility for financial assistance can depend on income, insurance status, and/or residency status. A hospital may be required by law to have a financial assistance policy, or it may choose to implement one voluntarily. Financial assistance is frequently referred to as “charity care.”
Bad debt: Patient bills that a hospital has tried to collect on and failed. Typically, hospitals are not supposed to pursue collections for bills that qualify for financial assistance or charity care, so bad debt refers to debt owed by patients ineligible for financial assistance.
Community benefit requirements: Nonprofit hospitals are required by federal law and some state laws to provide community benefits, such as financial assistance and other investments targeting community need, in exchange for a tax exemption.
Debt collectors or collections agencies: Entities whose business model primarily relies on collecting unpaid debt. They can either collect on behalf of a hospital (while the hospital still technically holds the debt) or buy the debt from a hospital.
Sale of medical debt: Hospitals sometimes sell the debt patients owe them to third-party debt buyers, who can be aggressive in seeking repayment of the debt.
Creditor: A party that is owed the medical debt and often wants to collect on the medical debt. This can be a hospital, a debt collector acting on behalf of a hospital, or a third-party debt buyer.
Debtor: A patient who owes medical debt over unpaid medical bills.
Wage garnishment: The ability of a creditor to get a court order that would allow them to deduct a portion of a debtor-patient’s paycheck before it reaches the patient. Federal law limits how much can be withheld from a debtor’s paycheck, and some states exceed this federal protection.
Placing a lien: A legal claim that a creditor can place on a patient’s home, prohibiting the patient from selling, transferring, or refinancing their home without first paying off the creditor. Most states require creditors to get a court order before placing a lien on a home.
Foreclosure or forced sale: A creditor can repossess and sell a patient’s home to pay off their medical debt. Often, creditors are required to obtain a court order to do so.
Perhaps what is most troubling is that the burden of medical debt is not borne equally: Black and Hispanic/Latino adults and women are much more likely to incur medical debt. Black adults also tend to be sued more often as a result. Uninsured patients, those from low-income households, adults with disabilities, and young families with children are all at a heightened risk of being saddled with medical debt.
Causes of Medical Debt
Most people — 72 percent, according to one estimate — attribute their medical debt to bills from acute care, such as a single hospital stay or treatment for an accident. Nearly 30 percent of adults who owe medical debt owe it entirely for hospital bills.
Although uninsured patients are more likely to owe medical debt than insured patients, having insurance does not fully shield patients from medical debt and all its consequences. More than 40 percent of insured adults report incurring medical debt, likely because they either had a gap in their coverage or were enrolled in insurance with inadequate coverage. High deductibles and cost sharing can leave many exposed to unexpected medical expenses.
The problem of medical debt is further exacerbated by hospitals charging increasingly high prices for medical care and failing to provide adequate financial assistance to uninsured and underinsured patients with low income.
Key Findings
Federal Medical Debt Protections Have Many Gaps
At the federal level, the tax code, enforced by the Internal Revenue Service (IRS), requires nonprofit hospitals to broadly address medical debt. However, these requirements do not extend to for-profit hospitals (which make up about a quarter of U.S. hospitals) and have other limitations.
Further, the IRS does not have a strong track record of enforcing these requirements. In the past 10 years, the IRS has not revoked any hospital’s nonprofit status for noncompliance with these standards.
The Consumer Financial Protection Bureau and the Federal Trade Commission have additional oversight authority over credit reporting and debt collectors. The Fair Credit Reporting Act regulates credit reporting agencies and those that provide information to them (debt collectors and hospitals). Consumers have the right to dispute any incomplete or inaccurate information and remove any outdated, negative information. In some cases, patients can directly sue hospitals or debt collectors for inaccurately reporting medical debt to credit reporting agencies. In addition, the Federal Debt Collection Practices Act limits how aggressive debt collectors can be by restricting the ways and times in which they can contact debtors, requiring certain disclosures and notifications, and prohibiting unfair or deceptive practices. Patients can directly sue debt collectors in violation of the law. This law, however, does not limit or prohibit the use of certain legal remedies, like wage garnishment or foreclosure, to collect on a debt.
Many states have taken steps to fill the gaps in federal standards. Within a state, several agencies may play a role in enforcing medical debt protections. Generally speaking:
state departments of health are the primary regulators of hospitals and set standards for them
state departments of taxation are responsible for ensuring nonprofit hospitals are earning their exemption from state taxes
state attorneys general protect consumers from unfair and deceptive business practices by hospitals and debt collectors.
Fewer Than Half of States Exceed Federal Requirements for Financial Assistance, Protections Vary Widely
Federal law requires nonprofit hospitals to establish and publicize a written financial assistance policy, but these standards leave out for-profit hospitals and lack any minimum eligibility requirements. As the primary regulators of hospitals, states have the ability to fill these gaps and require hospitals to provide financial assistance to low-income residents. Twenty states require hospitals to provide financial assistance and set certain minimum standards that exceed the federal standard.
All but three of these 20 states extend their financial assistance requirements to for-profit hospitals. Of these 20 states, four states — Connecticut, Georgia, Nevada, and New York — apply their financial assistance requirements only to certain types of hospitals.
Policies also vary among the 31 states that do not have statutory or regulatory financial assistance requirements for hospitals. For example, the Minnesota attorney general has an agreement in place with nearly every hospital in the state to adhere to certain patient protections, though it falls short of requiring hospitals to provide financial assistance. Massachusetts operates a state-run financial assistance program partly funded through hospital assessments. Other states use far less prescriptive mechanisms to try to ensure that patients have access to financial assistance, such as placing the onus of treating low-income patients on individual counties or requiring hospitals to have a plan for treating low-income and/or uninsured patients without setting any specific requirements.
Enforcement of state financial assistance standards.
The only way to enforce the federal financial assistance requirement is to threaten a hospital’s nonprofit status, and the IRS has been reluctant to use this authority. Among the 20 states that have their own state financial assistance standards, 10 require compliance as a condition of licensure or as a legal mandate. These mandates are often coupled with administrative penalties, but some states have established additional consequences. For example, Maine allows patients to sue noncompliant hospitals.
Six states make compliance with their financial assistance standards a condition of receiving funding from the state. Two other states use their certificate-of-need process (which requires hospitals to seek the state’s approval before establishing new facilities or expanding an existing facility’s services) to impose their financial assistance mandates.
Setting eligibility requirements for financial assistance.
The federal financial assistance standard sets no minimum eligibility requirements for hospitals to follow. However, the 20 states with financial assistance standards define which residents are eligible for aid.
One way for states to ensure that financial assistance is available to those most in need is to prevent hospitals from discriminating against undocumented immigrants. Four states explicitly prohibit such discrimination in statute and regulation. Most states, however, are less explicit. Thirteen states define eligibility broadly, basing it most frequently on income, insurance status, and state residency. However, it is unclear how hospitals are interpreting this requirement when it comes to patients’ immigration status. In contrast, three states explicitly exclude undocumented immigrants from eligibility.
States also vary widely in terms of which income brackets are eligible for financial assistance and how much financial assistance they may receive.
At least three of the 20 states with financial assistance standards allow certain patients with heavy out-of-pocket medical expenses from catastrophic illness or prior medical debt to access financial assistance. Many states also require hospitals to consider a patient’s insurance status when making financial assistance determinations. At least six states make financial assistance available for uninsured patients only, while at least eight others also make financial assistance available to underinsured patients.
Standardizing the application process.
Cumbersome applications can discourage many patients from applying for financial assistance. Five states have developed a uniform application form, while three others have set minimum standards for financial assistance applications. Eleven states require hospitals to give patients the right to appeal a denial of financial assistance.
States Split in Requiring Nonprofit Hospitals to Invest in Community Benefits
Federal and state policymakers also can require nonprofit hospitals to invest in community benefits in return for tax exemptions. Federal law requires nonprofit hospitals to produce a community health needs assessment every three years and have an implementation strategy. Almost all states exempt nonprofit hospitals from a host of state taxes, including income, property, and/or sales taxes. However, only 27 impose community benefit requirements on nonprofit hospitals.
Community benefits frequently include financial assistance but also investments that address issues like lack of access to food and housing. In the long run, these investments can reduce medical debt burden by improving population health and the financial stability of a community. Most states that require nonprofit hospitals to provide community benefits allow nonprofit hospitals to choose how they invest their community benefit dollars. This hands-off approach has given rise to concerns about the lack of transparency in community benefit spending as well as questions about whether hospitals are investing this money in ways that are most helpful to the community, such as in providing financial assistance.
Applicability of community benefit standards.
Nineteen states impose community benefit requirements on all nonprofit hospitals in the state, but three states further limit these requirements to hospitals of a certain size. At least six states have extended these requirements to for-profit hospitals as well. Of these six, the District of Columbia, South Carolina, and Virginia have incorporated community benefit requirements into their certificate-of-need laws instead of their tax laws. As a result, any hospital seeking to expand in these states becomes subject to their community benefit requirement.
Interaction between financial assistance and community benefits.
The federal standard allows nonprofit hospitals to report financial assistance as part of their community benefit spending. Most states with community benefit requirements also allow hospitals to do this. However, only seven states require hospitals to provide financial assistance to satisfy their community benefit obligations.
Setting quantitative standards for community benefit spending.
Only seven states set minimum spending thresholds that hospitals must meet or exceed to satisfy state community benefit standards. For example, Illinois and Utah require nonprofit hospitals’ community benefit contributions to equal what their property tax liability would have been. Unique among states, Pennsylvania gives taxing districts the right to sue nonprofit hospitals for not holding up their end of the bargain, which has proven to be a strong enforcement mechanism.
Fewer Than Half the States Exceed Federal Standards for Billing and Collections
Hospital billing and collections practices can significantly increase the burden of medical debt on patients. However, the current federal standard does not regulate these practices beyond imposing waiting periods and prior notification requirements for certain extraordinary collections actions (ECAs), such as garnishing wages or selling the debt to a third party.
Requiring hospitals to provide payment plans.
Federal standards do not require hospitals to make payment plans available. However, a few states do require hospitals to offer payment plans, particularly for low-income and/or uninsured patients. For example, Colorado requires hospitals to provide a payment plan and limit monthly payments to 4 percent of a patient’s monthly gross income and to discharge the debt once the patient has made 36 payments.
Limiting interest on medical debt.
Federal law does not limit the amount of interest that can be charged on medical debt. However, eight states have laws prohibiting or limiting interest for medical debt. Some states like Arizona have set a ceiling for interest on all medical debt. Others like Connecticut further prohibit charging interest to patients who are at or below 250 percent of the federal poverty level and are ineligible for public insurance programs.
Though many states do not have specific laws prohibiting or limiting interest that hospitals or debt collectors can charge on medical debt, all states do have usury laws, which limit the amount of interest than can be charged on any oral or written agreement. Usury limits are set state-by-state and can range anywhere from 5 percent to more than 20 percent, but most limits fall well below the average interest rate for a credit card (around 24%). At least one state, Minnesota, has sued a health system for charging interest rates on medical debt that exceeded the allowed limit in the state’s usury laws.
Interactions between hospitals, third-party debt collectors, and patients.
Unlike hospitals, debt collectors do not have a relationship with patients and can be more aggressive when collecting on the debt. Federal law neither limits when a hospital can send a bill to collections, nor does it require hospitals to oversee the debt collectors it uses. Most states (37) also do not regulate when a hospital can send a bill to collections, although some states have developed more protective approaches.
For example, Connecticut prohibits hospitals from sending the bills of certain low-income patients to collections, and Illinois requires hospitals to offer a reasonable payment plan first. Additionally, five states require hospitals to oversee their debt collectors.
Sale of medical debt to third-party debt buyers.
Hospitals sometimes sell old unpaid debt to third-party debt buyers for pennies on the dollar. Debt buyers can be aggressive in their efforts to collect, and sometimes even try to collect on debt that was never owed. Federal law considers the sale of medical debt an ECA and requires nonprofit hospitals to follow certain notice and waiting requirements before initiating the sale. Most states (44) do not exceed this federal standard.
Only three states prohibit the sale of medical debt. Two other states — California and Colorado — regulate debt buyers instead. For example, California prohibits debt buyers from charging interest or fees, and Colorado prohibits them from foreclosing on a patient’s home.
Reporting medical debt to credit reporting agencies.
Federal law considers reporting medical debt to a credit reporting agency to be an ECA and requires nonprofit hospitals to follow certain notice and waiting requirements beforehand. Most states (41) do not exceed this federal standard.
Of the 10 states that do go beyond the federal standard, a few like Minnesota fully prohibit hospitals from reporting medical debt. Most others require hospitals, debt collectors, and/or debt buyers to wait a certain amount of time before reporting the debt to credit agencies (Exhibit 8). Two states directly regulate credit agencies: Colorado prohibits them from reporting on any medical debt under $726,200, while Maine requires them to wait at least 180 days from the date of first delinquency before reporting that debt.
States Vary Widely on Patient Protections from Medical Debt Lawsuits
Federal law considers initiating legal action to collect on unpaid medical bills to be an extraordinary collections action and also limits how much of a debtor’s paycheck can be garnished to pay a debt.
In most states, hospitals and debt buyers can sue patients to collect on unpaid medical bills. Three states limit when hospitals and/or collections agencies can initiate legal action. Illinois prohibits lawsuits against uninsured patients who demonstrate an inability to pay. Minnesota prohibits hospitals from giving “blanket approval” to collections agencies to pursue legal action, and Idaho prohibits the initiation of lawsuits until 90 days after the insurer adjudicates the claim, all appeals are exhausted, and the patient receives notice of the outstanding balance.
Liens and foreclosures.
Most states (32) do not limit hospitals, collections agencies, or debt buyers from placing a lien or foreclosing on a patient’s home to recover on unpaid medical bills. However, almost all states provide a homestead exemption, which protects some equity in a debtor’s home from being seized by creditors during bankruptcy. The amount of homestead exemption available to debtors varies from state to state, ranging from just $5,000 to the entire value of the home. Seven states have unlimited homestead exemptions, allowing debtors to fully shield their primary homes from creditors during bankruptcy. Additionally, Louisiana offers an unlimited homestead exemption for certain uninsured, low-income patients with at least $10,000 in medical bills.
Ten states prohibit or set limits on liens or foreclosures for medical debt. For example, New York and Maryland fully prohibit both liens and foreclosures because of medical debt, while California and New Mexico only prohibit them for certain low-income populations.
Wage garnishment.
Under federal law, the amount of wages garnished weekly may not exceed the lesser of: 25 percent of the employee’s disposable earnings, or the amount by which an employee’s disposable earnings are greater than 30 times the federal minimum wage. Twenty-one states exceed the federal ceiling for wage garnishment. Only a few states go further to prohibit wage garnishment for all or some patients. For example, New York fully prohibits wage garnishment to recover on medical debt for all patients, yet California only extends this protection for certain low-income populations. While New Hampshire does not prohibit wage garnishment, it requires the creditor to keep going back to court every pay period to garnish wages, which significantly limits creditors’ ability to garnish wages in practice.
Many States Have Hospital Reporting Requirements, But Few Are Robust
Federal law requires all nonprofit hospitals to submit an annual tax form including total dollar amounts spent on financial assistance and written off as bad debt. However, these reporting requirements do not extend to for-profit hospitals and lack granularity. States, as the primary regulators of hospitals, would likely benefit from more robust data collection processes to better understand the impact of medical debt and guide their oversight and enforcement efforts.
Currently, 32 states collect some of the following:
financial data, including the total dollar amounts spent on financial assistance and/or bad debt
financial assistance program data, including the numbers of applications received, approved, denied, and appealed
demographic data on the populations most affected by medical debt
information on the number of lawsuits and types of judgments sought by hospitals against patients.
Fifteen states explicitly require hospitals to report total dollar amounts spent on financial assistance and/or bad debt, while 11 states also require hospitals to report certain data related to their financial assistance programs. Most of these 11 states limit the data they collect to the numbers of applications received, approved, denied, and appealed. However, a handful of them go further and ask hospitals to report on the amount of financial assistance provided per patient, number of financial assistance applicants approved and denied by zip code, number of payment plans created and completed, and number of accounts sent to collections.
Five states require hospitals to further break down their financial assistance data by race, ethnicity, gender, and/or preferred or primary language. For example, Maryland requires hospitals to break down the following data by race, ethnicity, and gender: the bills hospitals write off as bad debt and the number of patients against whom the hospital or the debt collector has filed a lawsuit.
Only Oregon asks hospitals to report on the number of patient accounts they refer for collections and extraordinary collections actions.
Discussion and Policy Implications
In 2022, the federal government announced administrative measures targeting the medical debt problem, which included launching a study of hospital billing practices and prohibiting federal government lenders from considering medical debt when making decisions on loan and mortgage applications. Although these measures will help some, only federal legislation and enhanced oversight will likely address current gaps in federal standards.
States can also fill the gaps in federal patient protections by improving access to financial assistance, ensuring that nonprofit hospitals are earning their tax exemption, and protecting patients against aggressive billing and collections practices. States also can leverage underutilized usury laws to protect their residents from medical debt.
Finding the most effective ways to enforce these standards at the state level could also protect patients. Absent oversight and enforcement, patients from underserved communities continue to face harm from medical debt, even when states require hospitals to provide financial assistance and prohibit them from engaging in aggressive collections practices. Bolstering reporting requirements alone would not likely ensure compliance, but states could protect patients by strengthening their penalties, providing patients with the right to sue noncompliant hospitals, and devoting funding to increase oversight by state agency officials.
To develop a comprehensive medical debt protection framework, states could also bring together state agencies like their departments of health, insurance, and taxation, as well as their state attorney general’s office. Creating an interagency office dedicated to medical debt protection would allow for greater efficiency and help the state build expertise to take on the well-resourced debt collection and hospital industries.
Still, these measures only address the symptoms of the bigger problem: the unaffordability of health care in the United States. Federal and state policymakers who want to have a meaningful impact on the medical debt problem could consider the protections discussed in this report as part of a broader plan to reduce health care costs and improve coverage.
Over the past 20 years, we’ve seen an evolution in payor contracts from fee-for-service to value-based care (VBC). This evolution is occurring across payor types: Commercial, Medicare, and Medicaid. In recent years, many providers have signed VBC contracts, which often provide better reimbursement rates as a reward for improvements in care delivery and care outcomes.
Specifically, a significant number of providers signed incentive-laden 5-10-year VBC contracts in 2020 moving away from traditional fee-for-service models, which helped improve their financial positioning throughout the pandemic. However, recent economic shifts have changed the landscape in which these contracts exist. Current contracts fail to take into account the rate of inflation and heightened financial distress we are seeing in the industry today. They also do not take into consideration the fact that many COVID-19-era government relief options — such as the CARES Act, Provider Relief Fund, and American Rescue Plan of 2021 — are sunsetting.
Simply stated, VBC contracts negotiated pre-pandemic are not only obsolete but likely contain pricing provisions that do not consider either unprecedented cost increases or difficulty in meeting performance incentives due to changes in patient behaviors. The result is an urgent need to reassess payor contracts of all types across all payor types.
However, before you renegotiate your contracts, you need to carefully consider your organization’s structure and business model so that you can ensure you’re working toward the best possible outcome.
To begin, take some time to examine the following considerations:
· Market Position: Having greater market share often leads to better-negotiated rates. Your organization should understand its market position before renegotiating its VBC contracts to understand what advantages you may have.
· Total Reimbursement & Total Value: Assess your total reimbursement rates, base reimbursement, and incentive reimbursement opportunity.
· Current Yield: Determine the percentage of total cost and the value of your denials and write-offs.
· Fee-for-service vs. Risk-based Models: Fee-for-service-based models should assess their steerage. Risk-based models should identify actuarily sound allocations, percentage of premium reconciliations, and risk adjustments/risk scores.
· IT Infrastructure: Evaluate your IT infrastructure. For example, is your EHR system set up for data analysis and able to benchmark KPIs? It’s important that your systems are designed to provide this information for negotiations and to ensure you have a complete picture of your patient population.
· Business Structure: Some provider organizations benefit from VBC models more than others. For example, a primary care provider (PCP) is more likely to coordinate along the continuum of care than a specialist. This enables the PCP to potentially have more control over the cost of care and revenue streams than specialists, making them a better candidate for a risk-based contract.
Carefully considering these six factors is a crucial first step to renegotiating your value-based contracts. Once you’ve made these considerations, you’re ready to move forward.
Ready to get started renegotiating your value-based contracts? Read our insight to get five tips for negotiation success.
Healthcare expenses declined in July, but not by enough to offset revenue losses, Kaufman Hall said in its latest National Hospital Flash Report.
Key Takeaways
Hospital performance declined on a month-over-month basis in July. All volume indicators registered declines this month. However, when compared to 2022, there is some slight improvement in operating margins.
Outpatient volumes decreased slightly more than inpatient. Some of this decline may be attributed to less patients seeking elective procedures in summer.
Expenses declined, but not enough to offset revenue losses. Labor continues to be the biggest share of hospital expenses, and expenses will likely continue to fluctuate due to inflation.
Bad debt and charity care rose month-over-month. Medicaid eligibility redetermination continues to affect hospitals and patients, with more than 30 states disenrolling people in June and July.
Action Steps
In an environment where hospitals continue to feel the effects of Medicaid disenrollment and labor expenses, those that have been more successful have made care transition a priority.
Hospitals should consider:
Starting off right by obtaining the necessary pre-certifications and payer authorizations before the patient comes in the door, as well as planning for discharge as soon as they are admitted.
Collecting data and using it to inform process improvement. Hospitals need to quantify lengths-of-stay and related data, and more importantly, use this data to make change.
Establishing relationships with post-acute care settings and having a clear pathway for patients’ post-discharge transition.
Last Monday, four U.S. Senators took aim at the tax exemption enjoyed by not-for-profit (NFP) hospitals in a letter to the IRS demanding detailed accounting for community benefits and increased agency oversight of NFP hospitals that fall short.
Last Tuesday, the Elevance Health Policy Institute released a study concluding that the consolidation of hospitals into multi-hospital systems (for-profit/not-for-profit) results in higher prices without commensurate improvement in patient care quality. “
Friday, Kaiser Health News Editor in Chief Elizabeth Rosenthal took aim at Ballad Health which operates in TN and VA “…which has generously contributed to performing arts and athletic centers as well as school bands. But…skimped on health care — closing intensive care units and reducing the number of nurses per ward — and demanded higher prices from insurers and patients.”
And also last week, the Pharmaceuticals’ Manufacturers Association released its annual study of hospital mark-ups for the top 20 prescription drugs used on hospitals asserting a direct connection between hospital mark-ups (which ranged from 234% to 724%) and increasing medical debt hitting households.
(Excerpts from these are included in the “Quotables” section that follows).
It was not a good week for hospitals, especially not-for-profit hospitals.
In reality, the storm cloud that has gathered over not-for-profit health hospitals in recent months has been buoyed in large measure by well-funded critiques by Arnold Ventures,Lown Institute, West Health, Patient Rights Advocate and others. Providence, Ascension, Bon Secours and now Ballad have been criticized for inadequate community benefits, excessive CEO compensation, aggressive patient debt collection policies and price gauging attributed to hospital consolidation.
This cloud has drawn attention from lawmakers: in NC, the State Treasurer Dale Folwell has called out the state’s 8 major NFP systems for inadequate community benefit and excess CEO compensation.
In Indiana, State Senator Travis Holdman is accusing the state’s NFP hospitals of “hoarding cash” and threatening that “if not-for-profit hospitals aren’t willing to use their tax-exempt status for the benefit of our communities, public policy on this matter can always be changed.” And now an influential quartet of U.S. Senators is pledging action to complement with anti-hospital consolidation efforts in the FTC leveraging its a team of 40 hospital deal investigators.
In response last week, the American Hospital Association called out health insurer consolidation as a major contributor to high prices and,
in a US News and World Report Op Ed August 8, challenged that “Health insurance should be a bridge to medical care, not a barrier.
Yet too many commercial health insurance policies often delay, disrupt and deny medically necessary care to patients,” noting that consumer medical debt is directly linked to insurer’ benefits that increase consumer exposure to out of pocket costs.
My take:
It’s clear that not-for-profit hospitals pose a unique target for detractors: they operate more than half of all U.S. hospitals and directly employ more than a third of U.S. physicians.
But ownership status (private not-for-profit, for-profit investor owned or government-owned) per se seems to matter less than the availability of facilities and services when they’re needed.
And the public’s opinion about the business of running hospitals is relatively uninformed beyond their anecdotal use experiences that shape their perceptions. Thus, claims by not-for-profit hospital officials that their finances are teetering on insolvency fall on deaf ears, especially in communities where cranes hover above their patient towers and their brands are ubiquitous.
Demand for hospital services is increasing and shifting, wage and supply costs (including prescription drugs) are soaring, and resources are limited for most.
The size, scale and CEO compensation for the biggest not-for-profit health systems pale in comparison to their counterparts in health insurance and prescription drug manufacturing or even the biggest investor-owned health system, HCA…but that’s not the point.
NFPs are being challenged to demonstrate they merit the tax-exempt treatment they enjoy unlike their investor-owned and public hospital competitors and that’s been a moving target.
Thus, the methodology for consistently defining and accounting for community benefits needs attention. That would be a good start but alone it will not solve the more fundamental issue: what’s the future for the U.S. health system, what role do players including hospitals and others need to play, and how should it be structured and funded?
The issues facing the U.S. health industry are complex. The role hospitals will play is also uncertain. If, as polls indicate, the majority of Americans prefer a private health system that features competition, transparency, affordability and equitable access, the remedy will require input from every major healthcare sector including employers, public health, private capital and regulators alongside others.
It will require less from DC policy wonks and sanctimonious talking heads and more from frontline efforts and privately-backed innovators in communities, companies and in not-for-profit health systems that take community benefit seriously.
No sector owns the franchise for certainty about the future of U.S. healthcare nor its moral high ground. That includes not-for-profit hospitals.
The darkening cloud that hovers over not-for-profit health systems needs attention, but not alone, despite efforts to suggest otherwise.
Clarifying the community-benefit standard is a start, but not enough.
Are NFP hospitals a problem? Some are, most aren’t but all are impacted by the darkening cloud.
Last week, six notable associations representing health insurers and large employers announced Better Solutions for Healthcare (BSH):“An advocacy organization dedicated to bringing together employers, consumers, and taxpayers to educate lawmakers on the rising cost of healthcare and provide ideas on how we can work together to find better solutions that lower healthcare costs for ALL Americans.”
BSH, which represents 492 large employers, 34 Blue Cross plans, 139 insurers and 42 business coalitions, blames hospitals asserting that “over the last ten years alone, the cost of providing employee coverage has increased 47% with hospitals serving as the number one driver of healthcare costs.”
Its members, AHIP, the Blue Cross Blue Shield Association, the Business Group on Health, Public Sector Health Care Roundtable, National Alliance of Healthcare Purchaser Coalitions and the American Benefits Council, pledge to…
Promote hospital competition
Enforce Federal Price Transparency Laws for Hospital Charges
Rein in Hospital Price Mark-ups
Insure Honest Billing Practices
And, of particular significance, BSH calls out “the growing practice of corporate hospitals establishing local monopolies and leveraging their market dominance to charge patients more…With hospital consolidation driving down competition, there’s no pressure for hospitals to bring costs back within reach for employees, retirees and their families…prices at monopoly hospitals are 12% higher than in markets with four or more competitors.”
The BSH leadership team is led by DC-based healthcare policy veterans with notable lobbying chops: Adam “Buck” Buckalew, a former Sen. Lamar Alexander (R-TN) staffer who worked on the Health Education, Labor and Pensions (HELP) committee and is credited with successfully spearheading the No Surprises Act legislation that took effect in January 2022, and Kathryn Spangler, another former HELP staffer under former Sen. Mike Enzi (R-WY) who most recently served as Senior Policy Advisor at the American Benefits Council.
It’s a line in the sand for hospitals, especially large not-for-profit systems that are on the defensive due to mounting criticism.
Examples from last week: Atrium and Caremont were singled in NC by the state Treasurer for their debt collection practices based on a Duke study that got wide media coverage. Allina’s dispute with 550 of its primary care providers seeking union representation based on their concerns about patient safety. Jefferson Health was called out for missteps under its prior administration’s “growth at all costs” agenda and the $35 million 2021 compensation for Common Spirit’s CEO received notice in industry coverage.
My take:
BSH represents an important alignment of health insurers with large employers who have shouldered a disproportionate share of health costs for years through the prices imposed for the hospitals, prescriptions and services their employees and dependents use.
Though it’s too early to predict how BSH vs. Corporate Hospitals will play out, especially in a divided Congress and with 2024 elections in 14 months, it’s important to inject a fair and balanced context for this contest as the article of war are unsealed:
Health insurers and hospitals share the blame for high health costs along with prescription drug manufacturers and others. The U.S. system feasts on opaque pricing, regulated monopolies and supply-induced demand. Studies show unit costs for hospitals along with prescription drug costs bear primary responsibility for two-thirds of health cost increases in recent years—the result of increased demand and medical inflation. But insurers are complicit: benefits design strategies that pre-empt preventive health and add administrative costs are parts of the problem.
Corporatization of the U.S. system cuts across every sector: Healthcare’s version of Moneyball is decidedly tilted toward bigger is better: in healthcare, that’s no exception. 3 of the top 10 in the Fortune 100 are healthcare (CVS-Aetna, United, McKesson)) and HCA (#66) is the only provider on the list. The U.S. healthcare industry is the largest private employer in the U.S. economy: how BSH addresses healthcare’s biggest employers which include its hospitals will be worth watching. And Big Pharma companies pose an immediate challenge: just last week, HHS called out the U.S. Chamber of Commerce for siding with Big Pharma against implementation of drug price controls in the Inflation Reduction Act—popular with voters but not so much in Big Pharma Board rooms.
The focus will be on Federal health policies. BSH represents insurers and employers that operate across state lines–so do the majority of major health systems. Thus, federal rules, regulations, administrative actions, executive orders, and court decisions will be center-stage in the BSH v. corporate hospitals war. Revised national policies around Medicare and federal programs including military and Veterans’ health, pricing, equitable access, affordability, consolidation, monopolies, data ownership, ERISA and tax exemptions, patent protections and more might emerge from the conflict. As consolidation gets attention, the differing definitions of “markets” will require attention: technology has enabled insurers and providers to operate outside traditional geographic constraints, so what’s next? And, complicating matters, federalization of healthcare will immediately impact states as referenda tackle price controls, drug pricing, Medicaid coverage and abortion rights—hot buttons for voters and state officials.
Boards of directors in each healthcare organization will be exposed to greater scrutiny for their actions: CEO compensation, growth strategies, M&A deals, member/enrollee/patient experience oversight, culture and more are under the direct oversight of Boards but most deflect accountability for major decisions that pose harm. Balancing shareholder interests against the greater good is no small feat, especially in a private health system which depends on private capital for its innovations.
8.6% of the U.S. population is uninsured, 41% of Americans have outstanding medical debt, and the majority believe health costs are excessive and the U.S. system is heading in the wrong direction.
Compared to other modern systems in the world, ours is the most expensive for its health services, least invested in social determinants that directly impact 70% of its costs and worst for the % of our population that recently skipped needed medical care (39.0% (vs. next closest Australia 21.2%), skipped dental care (36.2% vs. next closest Australia 31.7%) and had serious problems/ were unable to pay medical bills (22.4% next closest France 10.1%). Thus, it’s a system in which costs, prices and affordability appear afterthoughts.
Who will win BSH vs. Corporate Hospitals? It might appear a winner-take all showdown between lobbyists for BSH and hospital hired guns but that’s shortsighted. Both will pull out the stops to win favor with elected officials but both face growing pushback in Congress and state legislatures where “corporatization” seems more about a blame game than long-term solution.
Each side will use heavy artillery to advance their positions discredit the other. And unless the special interests that bolster efforts by payers are hospitals are subordinated to the needs of the population and greater good, it’s not the war to end all healthcare wars. That war is on the horizon.
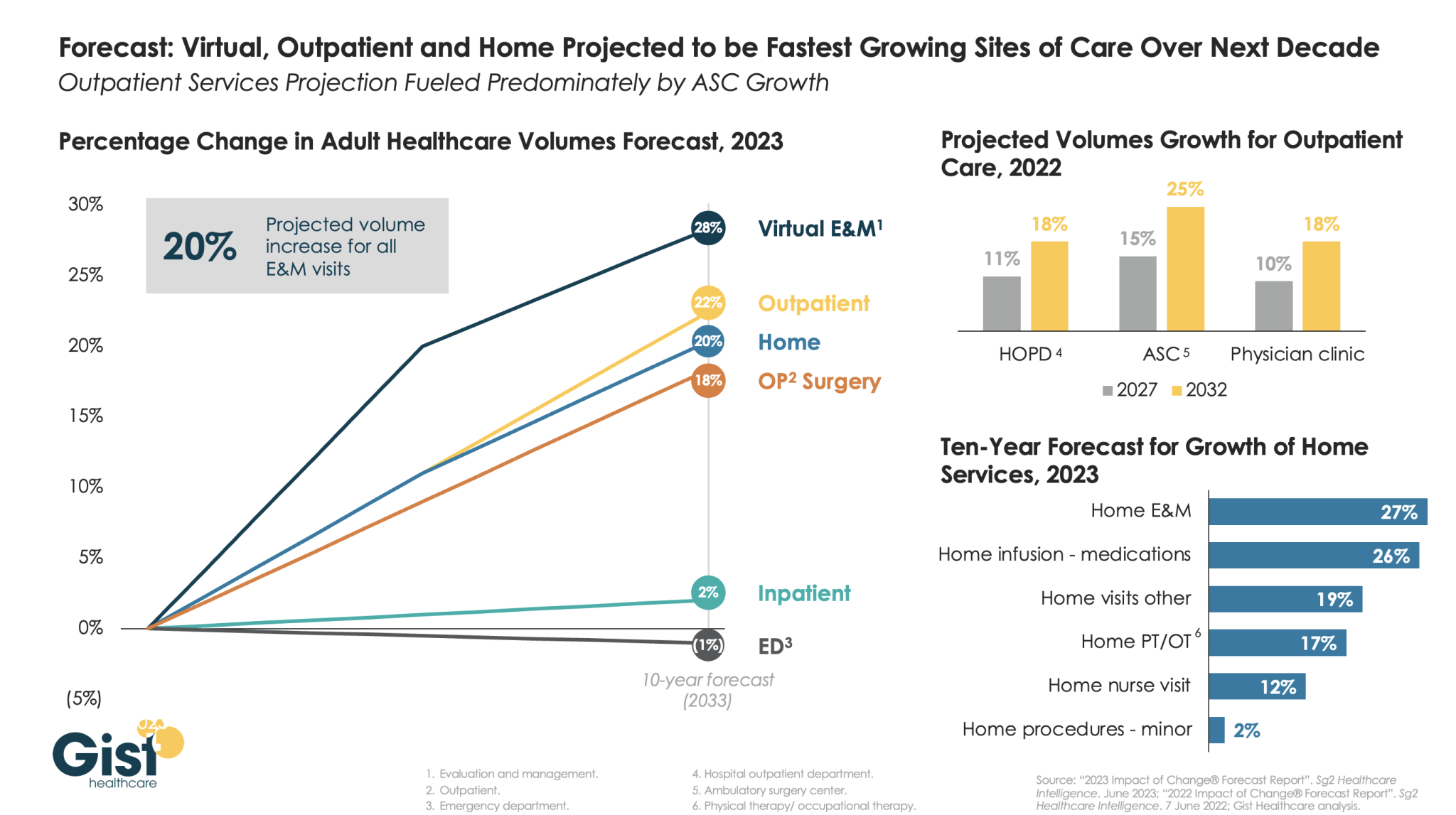
The pandemic accelerated the outpatient shift, which had been progressing steadily for decades, into a new gear, as safety-minded consumers avoided inpatient settings.
Using the latest forecasting data from strategic healthcare consulting firm Sg2, the graphic above illustrates how the outpatient shift will continue to accelerate in the coming years. With each projected to grow by 20 percent or more, outpatient, virtual, and home-based care services will continue far outpace growth in hospital-based care over the next decade.
Ambulatory surgery centers (ASCs) will be at the center of this care shift, reflected by a projected 25 percent rise in ASC volumes by 2032.
The breadth of care available at home will also expand as care delivery technology improves. With the population becoming older and sicker, higher incidence of chronic disease will be met by a rapid expansion of home evaluation and management services (E&M),reflecting a shift away from hospitals and doctors’ offices as hubs for complex care management.
Instead, the patients still coming to hospitals will present with increasingly acute conditions, driving up demand for resource-intensive critical care, as broader inpatient volume remains relatively flat.
As 41% of American adults face medical debt, residents of this southern Colorado city contend their local nonprofit hospitals aren’t providing enough charity care to justify the millions in tax breaks they receive.
The two hospitals in Pueblo, Parkview Medical Center and Centura St. Mary-Corwin, do not pay most federal or state taxes. In exchange for the tax break, they are required to spend money to improve the health of their communities, including providing free care to those who can’t afford their medical bills. Although the hospitals report tens of millions in annual community benefit spending, the vast majority of that is not spent on the types of things advocates and researchers contend actually create community benefits, such as charity care.
And this month, four U.S. senators called on the Treasury’s inspector general for tax administration and the Internal Revenue Service to evaluate nonprofit hospitals’ compliance with tax-exempt requirements and provide information on oversight efforts.
The average hospital in the U.S. spends 1.9% of its operating expenses on charity care, according to an analysis of 2021 data by Johns Hopkins University health policy professor Ge Bai. Last year, Parkview provided 0.75% of its operating expenses, about $4.2 million, in free care.
Centura Health, a chain of 20 tax-exempt hospitals, reports its community benefit spending to the federal government in aggregate and does not break out specific numbers for individual hospitals. But St. Mary-Corwin reported $2.3 million in charity care in fiscal year 2022, according to its state filing. The filing does not specify the hospital’s operating expenses.
The low levels of charity care have translated into more debt for low-income residents.
About 15% of people in Pueblo County have medical debt in collections, compared with 11% statewide and 13% nationwide, according to 2022 data from the Urban Institute. Those Puebloans have median medical debt of $975, about 40% higher than in Colorado and the U.S. as a whole. And all of those numbers are worse for people of color.
“How far into debt do people have to go to get any kind of relief?” said Theresa Trujillo, co-executive director at the Center for Health Progress’ Pueblo office. “Once you understand that there are tens of millions of dollars every single year that hospitals are extracting from our communities that are meant to be reinvested in our communities, you can’t go back from that without saying, ‘Oh my gosh, that is a thread we need to pull on.’”
Trujillo is organizing a group of fed-up residents to engage both hospitals on their community benefit spending. The group of at least a dozen residents believe the hospitals are ignoring the needs identified by the community — things like housing, addiction treatment, behavioral health care, and youth activities — and instead spending those dollars on things that mainly benefit the hospitals and their staffs.
For the fiscal year ending June 2022, with total revenue of $593 million, Parkview reported $100 million in community benefit spending. But most of that — more than $77 million — represented the difference between the hospital’s cost of providing care and what Medicaid paid for it.
IRS guidelines allow hospitals to claim Medicaid shortfall as a community benefit, but many academics and health policy experts argue such balance sheet shifts aren’t the same as providing charity care to patients.
Parkview also reported $4.7 million for educating its medical staff and $143,000 in incentives to recruit health professionals as community benefit. The hospital spent only $44,000 on community health improvement projects, which appear to have consisted mainly of launching a new mobile app to streamline appointments and referrals.
Meanwhile, the hospital recently spent $58 million on a new orthopedic facility and $43 million on a new cancer center. Parkview also wrote off $39 million in bad debt in fiscal 2022, although that is different from charity care. The bad debt is money the hospitals tried to collect from patients and ultimately decided they’d never get. But by that time, those patients would likely have been sent to collections and potentially had their credit damaged. And outstanding debt often keeps patients from seeking other needed care.
There is a disconnect between what the community said its biggest health needs were and where Parkview directed its spending. The hospital’s community needs assessment pegged access to care as the top concern, and the hospital said it launched the phone app in response.
The second-largest perceived health need was addressing alcohol and drug use. Yet, the only initiative Parkview cited in response was posting preventive health videos online, including some on alcohol and drug use. Meanwhile, the hospital shut down its inpatient psychiatric unit.
Parkview declined to answer questions about its charity care spending, but hospital spokesperson Todd Seip emailed a statement saying the hospital system “has been committed to providing extensive charity care to our community.”
Seip noted that 80% of Parkview’s patients are covered by Medicare or Medicaid, which pay lower rates than commercial insurance. The hospital posted a net loss of $6.7 million in the 2022 fiscal year, although its charity care wasn’t appreciably higher in previous years in which it posted a net gain.
Centura St. Mary-Corwin reported $16 million in Medicaid shortfall and $2 million in medical staff education in 2022, according to its state filing. The hospital spent about $38,000 for its community health improvement projects, primarily on emergency medical services outreach programs in rural areas. The hospital provided another $96,000 in services, mainly to promote covid-19 vaccination.
Centura also declined to answer questions about its charity care spending. Hospital spokesperson Lindsay Radford emailed a statement saying St. Mary-Corwin was aligning its community health needs assessment process with the Pueblo Department of Public Health and Environment “to develop shared implementation strategies for our community benefit funds, ensuring the resources are targeting the highest needs.”
Trujillo questioned how the hospital has conducted its community health assessments, relying on a social media poll to identify needs. After community members identified 12 concerns, she said, hospital leaders chose their priorities from the list.
“They talk about a community garden like they’re feeding the whole south side of the community,” Trujillo said. The hospital established a community garden in 2021, with 20 beds that could be adopted by residents to grow vegetables. Trujillo did praise the hospital for converting part of its building into dorms for a community college nursing program.
Trujillo’s group has spent much of the summer researching hospital charity spending and showing up at public meetings to have their views heard. They are working to gain seats on hospital and other state boards that influence how community benefit dollars are spent, and are urging hospitals to reconfigure their boards to better represent the demographics of their communities.
“We’ve made folks now aware that we want to be a part of those processes,” Trujillo said. “We’re willing to help them reach deeper into the community.”
Tax-exempt hospitals have been under increased state scrutiny for their charitable spending, especially after the Affordable Care Act and Medicaid expansion drove down the uninsured rate. That in turn cut the amount of care hospitals had to provide without being paid, potentially freeing up money to help more people without insurance or with high-deductible plans.
In Colorado, hospitals’ charity care spending and bad debt write-offs dropped from an average of $680 million a year in the five years prior to the ACA being fully implemented in 2014 to an average of $337 million in the years after, according to the Colorado Healthcare Affordability and Sustainability Enterprise Board, a state advisory group.
In states like Colorado, which used federal funding to expand the number of people covered by Medicaid, hospitals shifted more of their community benefit spending to cover Medicaid reimbursement shortfalls.
A January report from Colorado’s Department of Health Care Policy & Financing concluded that payments from public and private health plans help the state’s hospitals make more than enough money to offset lower Medicaid rates and still turn a profit while providing more true charity care.
Colorado has enacted two bills in the past five years to increase the transparency of hospitals’ charitable efforts with new reporting requirements.
“I think overall, we’re pleased with the amount of money that hospitals are reporting they spent,” said Kim Bimestefer, the executive director of the Department of Health Care Policy & Financing. “Is that money being expended in meaningful ways, ways that improve health and well-being of the community? Our reports right now can’t determine that.”
Shorter contracts, noncompete agreements and increased emphasis on value-based components are among the shifts occurring in physician contracts as hospitals and medical groups build recruitment pipelines and offer incentives to retain physicians.
Changes in how physician contracts are layered echoes a trend that has been occurring in the labor market itself. Physicians are increasingly opting for employed opportunities and contracts within those models are changing accordingly.
From 2019 to 2021, more than 108,700 physicians left private practice for employment opportunities, with 58,200 physicians joining hospitals. About three in four physicians are now employed by hospitals, health systems, private-equity-owned groups, payers or other corporate entities.
The rising costs of private practice, increasing administrative burdens and reimbursement hurdles are also making solo practice a challenging model for many physicians today.
Fewer large medical groups are offering salaries with production bonuses, according to an AMN Healthcare report on physician and advanced practitioner recruiting incentives. The company’s 2017 report found that 75 percent of contracts featured a salary with production bonus, while only 17 percent had a straight salary.
Some medical groups have stopped offering production bonuses because they found that the straight salary model has less ambiguity and is less likely to cause friction with physicians, according to the report.
AMN also found that a relatively high percentage of academic medical centers do not offer the salary with production bonus model, which may account for the decline in the use of this compensation structure in its report.
Income guarantees, which are essentially loans that must be repaid generally (but can be forgiven over time) are used to establish physicians in solo or small independent practices. Income guarantees were once the standard contract model, but as the number of private practices has declined, so has the use of income guarantees, according to the report..
Health systems continue to rethink physician contracts as healthcare continues its shift away from fee for service, but challenges remain when it comes to compensation in these models. Systems at the forefront of this shift are developing ways to incentivize physicians in value-based care as the trend towards team-based compensation gains traction and fosters collaboration among providers.
Epic was named the top EHR for acute care hospitals with 251 beds or more by Black Book Research.
The research group based its results on surveys of 18 performance indicators conducted between the second quarter of 2022 and the third quarter of 2023.
Here are the top six EHRs for large hospitals, according to the report: