Legacy health brands are losing their significance as healthcare consumers place higher value on convenience than reputation. That’s the idea behind a July 1 tweet by Sachin Jain, MD, the CEO of Scan Group and Scan Health Plan.
“We are in an era of the declining significance of big healthcare brands,” he said.
To Dr. Jain, big healthcare brands are the ones commonly known for being the best in a specific specialty or renowned in their region. While many big healthcare brands have high quality performance metrics to hang their clout on, Dr. Jain believes reliance on name alone is problematic.
“There’s been an arrogance by a lot of healthcare organizations that have kind of sold on brand. There’s going to be a reckoning for some of those organizations. My personal view is that the next generation of healthcare consumers is going to be less aligned to think about brands in the same way,” Dr. Jain told Becker’s.
Today’s patients are paying more attention to convenience, digital access and price than reputation. Cost of care, ease of scheduling and accessibility are beating out recognition, Dr. Jain said.
At Scan, Dr. Jain said the Long Beach, Calif.-based Medicare Advantage insurer that serves more than 220,000 members is hyperfocused on staying as human as possible and fulfilling unmet needs for its community.
“Elite healthcare brands are entering this fun phase where they are becoming underdogs. They need to have a chip on their shoulders almost to thrive and perform in this next phase,” Dr. Jain said. “Because I’m not sure payers are necessarily going to continue to pay the same premiums per brand.”
Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
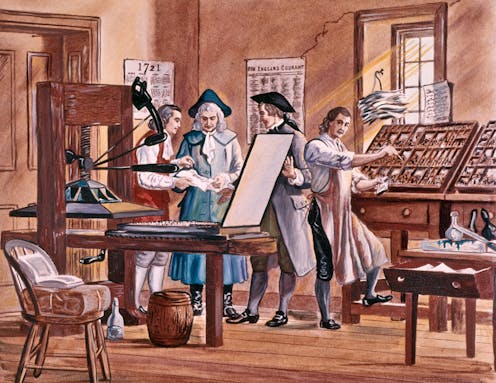
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
It’s “a trickle that will become a torrent,” Ashish Jha, dean at Brown University’s School of Public Health, tweeted.
More hospitals are likely to require employees receive a COVID-19 vaccine, experts said, to further protect the sick and vulnerable patients who rely on them for care.
A Houston-area hospital captured headlines after taking a firm stance on requiring vaccines that prevent severe illness of the coronavirus, which has killed more than 600,000 in the U.S. and ravaged the economy.
Houston Methodist employees who refused the vaccine were either terminated or resigned. A judge earlier this month sided with the hospital and tossed out an employee lawsuit that was seeking to block the mandated inoculation. The ruling may give other hospitals the green light to require the jab, and as more facilities put a similar policy in place, others are likely to follow, experts said.
It’s “a trickle that will become a torrent,” Ashish Jha, professor and dean at Brown University’s School of Public Health, posted Thursday on Twitter.
3 large health systems in Massachusetts to require all workers to be vaccinated.
Given the critical need to protect vulnerable patients, its critical all hospitals do this.
Some of the nation’s largest health systems have yet to mandate the shot, including Kaiser Permanente and CommonSpirit Health.
“Vaccination will only be required for Kaiser Permanente employees if a state or county where we operate mandates the vaccine for health care workers,” the company said in an email.
The American Hospital Association continues to hear that a growing number of its members are requiring the vaccine, with some exemptions. However, many member hospitals are waiting until the FDA grants full approval, a time when more safety and efficacy data will be made available.
“Getting vaccinated is especially critical for health care professionals because they work with patients with underlying health conditions whose immune systems may be compromised,”AHA, which has not taken on stance on the requirement, said in a statement.
The mandates raise ethical questions, some say, pointing to the profession’s promise to “do no harm.”
Arthur Caplan, head of medical ethics at New York University School of Medicine, said the codes of ethics that doctors and nurses says to put patients first, do no harm and protect the vulnerable.
“Of course they should be vaccinated,” he said. “If they don’t want to get vaccinated, I think they’re in the wrong profession.”
The Equal Employment Opportunity Commission said employment law does not prohibit employers from requiring the jab, essentially giving the green light to employers to put incentives and requirements in place for their workers. The EEOC is the federal agency tasked with ensuring that workplaces do not discriminate.
Some states are going against the tide and signing legislation that bars vaccine mandates, including Florida. The city of San Francisco will require hospital employees and workers in high-risk settings to get the vaccine. San Francisco, like other employers and universities, will require all city workers get inoculated.
The differing policy stances across the country creates additional hurdles for corporations with a large footprint.
In our work over the years advising health systems on M&A, we’ve been struck by how often “social issues” cause deals that are otherwise strategically sound to go off the rails.
Of course, it’s an old chestnut that “culture eats strategy for breakfast”, but what’s been notable, especially recently, is how early in the process hot-button governance and leadership issues enter the discussions.
Where is the headquarters going to be? Who’s going to be the CEO of the combined entity? And most vexingly, how many board seats is each organization going to get? That last issue is particularly troublesome, as it’s often where negotiations get bogged down. But as one health system board member recently pointed out to us, getting hung up on whether board seats are split 7-6 or 8-5 is just silly—in her words, “If you’re in a position where board decisions turn on that close of a margin, you’ve got much bigger strategic problems.”
It’s an excellent point. While boards shouldn’t just rubber stamp decisions made by management, it’s incumbent on the CEO and senior leaders to enfranchise and collaborate with the board in setting strategy, and critical decisions should rarely, if ever, come down to razor-thin vote tallies.
If a merger makes sense on its merits, and the strategic vision for the combined organization is clear, quibbling over how many seats each legacy system “gets” seems foolish. No board should go into a merger anticipating a future in which small majorities determine the outcome of big decisions.











{kind=link}