Were you better off in 2022 than you were in 2017? I was for a lot of reasons. One thing that didn’t change over those five years, though, was my health insurance status. I had health insurance in 2017, and I had health insurance in 2022. And I still have health insurance today.
So do most Americans. In fact, according to the U.S. Census Bureau’s latest report on health insurance coverage in the U.S., 92.1% of us had some form of health insurance in 2022. That’s about 304 million people, per the report.
Conversely, 7.9% of us were uninsured last year. That’s a little more than 25.9 million people. That’s down from 8.3% and about 27.2 million people in 2021.
Some may see the decrease in both the percentage and number of uninsured as good news. And it is. Any time the uninsured figures go down, that’s good.
The bad news is, we’re back where we were in 2017. That’s also when 7.9% of us, or about 25.6 million people, were uninsured. Five years of trying to get more people insured and nothing to show for it.
The number of people with any type of private health insurance (employer-based or direct-purchase) crept up to 216.5 million last year from 216.4 million in 2021. The number of people with any type of public health insurance (Medicare, Medicaid, etc.) rose to 119.1 million last year from 117.1 million in 2021. Both headed in the right direction but too slow to push the uninsured rate significantly down.
If we want to get serious about achieving universal coverage, let’s get serious about it. If we don’t want to get serious about it because most of us already have health insurance, the only useful purpose of the Census Bureau’s annual reports on health insurance is to show us how little we really care.
It feels as though November 5, 2024 is far away, but for both Democrats and Republicans, the election is now. On the issue of healthcare, the two parties’ approaches differ sharply.
Think back to the behemoth effort by Republicans to “repeal and replace” the Affordable Care Act six years ago, an effort that left them floundering for a replacement, basically empty-handed. Recall the 2022 midterms, when their candidates in 10 of the tightest House and Senate races uttered hardly a peep about healthcare.
That reticence stood in sharp contrast to Democrats who weren’t shy about reiterating their support for abortion rights, simultaneously trying hard to ensure that Americans understood and applauded healthcare tenets in the Inflation Reduction Act.
As The Hill noted in early August, sounds like the same thing is happening this time around as America barrels toward November 2024. The publication said it reached to 10 of the leading Republican candidates about their plans to reduce healthcare costs and make healthcare more affordable, and only one responded: Rep. Will Hurd (R-Texas).
Healthcare ‘A Very Big Problem’
Maybe the party thinks its supporters don’t care. But, a Pew Research poll from June showed 64% of us think healthcare affordability is a “very big problem,” superseded only by inflation. In that research, 73% of Democrats and 54% of Republicans thought so.
Chuck Coughlin, president and CEO of HighGround, an Arizona-based public affairs firm, told The Hill that the results aren’t surprising.
“If you’re a Republican, what are you going to talk about on healthcare?” he said.
Observers note that the party has homed in on COVID-lockdowns, transgender medical rights, and yes, abortion.
Plans won’t offer coverage for preexisting conditions, maternity care, or prescription drugs, and they can set limits on coverage. The plans will make it easier for small employers to self-insure, so they don’t have to adhere to ACA or state insurance rules.
CHOICE would let large groups come together to buy Association Health Plans, said NPR, which noted that in the past, there have been “issues” with these types of plans.
Insurance experts say that the act takes a swing at the very foundation of the ACA. As one analyst described it, the act intends to improve America’s healthcare “through increased reliance on the free market and decreased reliance on the federal government.”
Democrats Tout Reduce-Price Prescriptions
Meanwhile, on Aug. 29, President Joe Biden spoke proudly in The White House: “Folks, there’s a lot of really great Republicans out there. And I mean that sincerely…But we’ll stand up to the MAGA Republicans who have been trying for years to get rid of the Affordable Care Act and deny tens of millions of Americans access to quality, affordable healthcare.” Current ACA enrollment is higher than 16 million.
He said that Big Pharma charges Americans more than three times what other countries charge for medications. And on that date, he announced that “the (Inflation Reduction Act) law finally gave Medicare the power to negotiate lower prescription drug prices.” He wasn’t shy about saying that this happened without help from “the other team.”
The New York Times said it feels this push for lower healthcare costs will be the centerpiece of his re-election campaign. The announcement confirmed that his administration will negotiate to lower prices on 10 popular—and expensive drugs—that treat common chronic illnesses.
It said previous research shows that as many as 80% of Americans want the government to have the power to negotiate.
The president also said that “Next year, Medicare will select more drugs for negotiation.” He added that his administration “is cracking down on junk health insurance plans that look like they’re inexpensive but too often stick consumers with big hidden fees.” And it’s tackling the extensive problem of surprise medical bills.
Earlier, on August 11, Biden and fellow Democrats celebrated the first anniversary of the PACT Act, legislation that provides healthcare to veterans exposed to toxic burn pits while serving. He said more than 300,000 veterans and families have received these services, with more than 4 million screened for toxic exposure conditions.
Push for High-Deductible Plans
Republicans want to reduce risk of high-deductible plans and make them more desirable—that responsibility is on insurers. According to Politico, these plans count more than 60 million people as members, and feature low premiums and tax advantages. The party said plans will also help lower inflation when people think twice about seeking unneeded care.
The plans’ low monthly premiums offer comprehensive preventive care coverage: physicals, vaccinations, mammograms, and colonoscopies, and have no co-payments, Politico said. The “but” in all this is that members will pay their insurers’ negotiated rate when they’re sick, and for medicines and surgeries. Minimum deductible is $1,500 or $3,000 for families—and can be even higher.
Members can fund health savings accounts but can’t fund flexible spending accounts. Proponents cite more access to care, and reduced costs due to promotion of preventive care. Nay-sayers worry about lower-income members facing costly bills due to insufficient coverage.
Republican Candidates Diverge on Medicaid
The American Hospital Association (AHA) doesn’t love these high deductible plans. It explained that members “find they can’t manage the gap between what their insurance pays and what they themselves owe as a result,” and that, AHA said, contributes to medical debt—something the association wants to change.
An Aug. 3 Opinion in JAMA Health Forum pointed out other ways the two parties diverge on healthcare. For example, the piece cited Biden’s incentives for Medicaid expansion. In contrast, Florida Governor Ron DeSantis, a Republican presidential candidate, has not worked to offer Medicaid to all lower-income residents under the ACA. Former Governor Nikki Haley of South Carolina feels the same, doing nothing. However, former New Jersey Governor Chris Christie has expanded it, as did former Vice President Mike Pence, when he governed Indiana.
Undoubtedly, as in presidential elections past, healthcare will be at least a talking point, with Democrats likely continuing to make it a central focus, as before.
The GOP Presidential debate marked the unofficial start of the 2024 Presidential campaign. With the exception of continued funding for Ukraine, style points won over issue distinctions as each of the 8 White House aspirants sought to make the cut to the next debate September 27 at the Reagan Library in Simi Valley, CA.
For the candidates in Milwaukee, it’s about “Stayin’ Alive” per the BeeGee’s hit song: that means avoiding self-inflicted harm while privately raising money to keep their campaigns afloat. And, based on Debate One, with the exception of abortion, that means they’ll not face questions about their positions on the litany of issues that dominate healthcare these days i.e., drug prices, hospital consolidation, price transparency, workforce burnout and many others. In Milwaukee, healthcare was essentially ‘out of sight our of mind’ to the moderators and debaters despite being 18% of the U.S. economy and its biggest employer.
For now, each will enlist ghostwriters to produce position papers for their websites, and, on occasion, reporters will press for specifics to test their grasp on a topic but that’s about it. Based on last Wednesday’s 2-hour event, it’s unlikely general media outlets like Fox News (which also hosts Debate Two) will explore healthcare issues except for abortion.
That means healthcare will be subordinated to the economy, inflation, immigration and crime—the top issues to GOP voters—for most of the Presidential primary season.
Next November, voters will also elect 34 US Senators, 435 members of the House of Representatives, 11 Governors and their representatives in 85 state legislative bodies. This will be the first election cycle after reapportionment of votes in the United States Electoral College following the 2020 United States census. Swing states (WI, MI, PA, NV, AZ, GA, FL, OH, CO, VA) will again be keys to the Presidential results since demographics and population shifts have increased the concentrations of each party’s core voters in so-called Blue States and Red States:
The Democratic voter core is diverse, educated and culturally liberal with its strongest appeal to African-Americans, Latinos, women, educated professionals and urban voters. Blue States are predominantly in the Northeast, Upper Midwest and West Coast regions.
The Republican voter core consists of rural white voters, evangelicals, the elderly, and non-college educated adults. Red States are predominantly in the South and Southwest.
The increased concentrations of Blue or Red voters in certain states and regions has contributed to political polarization in the U.S. electorate and presents an unusual challenge to healthcare. Per Gallup: “Political polarization since 2003 has increased most significantly on issues related to federal government power, global warming and the environment, education, abortion, foreign trade, immigration, gun laws, the government’s role in providing healthcare, and income tax fairness. Increased polarization has been less evident on certain moral issues and satisfaction with the state of race relations.”
Thus, healthcare issues are increasingly subject to hyper partisanship and often misinformation.
Given the limited knowledge voters have on most health issues and growing prevalence of social media fueled misinformation, political polarization creates echo chambers in healthcare—one that thinks the system works for those who can afford it and another that thinks that’s wrong.
It’s dicey for politicians: it’s political malpractice to offer specific solutions on anything, especially healthcare. It’s safer to attack its biggest vulnerabilities—affordability and equitable access—even though they mean something different in every echo chamber.
My take:
Barring a second Covid pandemic or global conflict with Russia/China, it’s unlikely healthcare issues will be prominent in Campaign 2024 at the national level except for abortion. At least through the May primary season, here’s the political landscape for healthcare:
Affordability and inequitable access will be the focus of candidate rhetoric at the national level: Trust and confidence in the U.S. health system has eroded. That’s fertile political turf for critics.
In Congress, the fiercest defenders of the status quo have joined efforts to impose restrictions on consolidation and price transparency for hospitals and price controls for prescription drugs. There’s Bipartisan acknowledgement that inequities in accessing care are significant and increasing, especially in minority and low income populations. They differ over the remedy. Employers expect their health costs to increase at least 8% next year and blame hospitals and drug companies for price gauging and want Congress to do more. 85% of Democrats think “the government should insure everyone” vs. 33% of Republican voters which calcifies inaction in a divided Congress though. Opposition to the Affordable Care Act (2010) has softened and Medicaid expansion has passed in 40 Blue and Red states.
In the 2024 election cycle, remedies for increased access and more affordability will pit Republicans calling for more competition, consumerism and transparency and Democrats calling for more government funding, regulation and fairness.
But more important, voter and employer frustration with partisan bickering sans solutions will set the stage for the vigorous debate about a single payer system in 2026 and after,
State elections will give more attention to healthcare issues than the Presidential race: That’s because Governors and state legislators set direction on issues like abortion rights, drug price controls, Medicaid funding, scope of practice allowances and others.
Increasingly, state Attorney’s General and Treasurers are weighing in on consolidation and spending. States referee workforce issues like nurse staffing requirements and others. And ballot referenda on healthcare issues trail only public education as a focus of grassroots voter activity. At the top of that list is abortion rights:
In 25 states and DC, there are no restrictions on access; in 14 states, abortion is banned and in 11 abortions—both procedures and medication—are legal, but with gestational limits from 6 weeks (GA), to between 12 and 22 weeks (AZ, UT, NE, KS, IA, IN, OH, NC, SC, FL). It’s an issue that divides legislators and increasingly delineates Blue and Red states and in many states remains unsettled.
Other healthcare issues, like ageism, will surface in Campaign 2024 in the context of other topics: Finally, healthcare will factor into other issues: Example: The leading Presidential candidates are seniors: President Biden was the oldest person to assume the office at age 78 and would be would be 86 at the end of his second term. Former President Trump was 70 when elected in 2016 and would be 81 if elected when his second term ends.
The majority of Americans are concerned about the impact of age on fitness to serve among aspirants for high office: cognitive impairment, dementia, physical limitations et al. will be necessary talking points in campaigns and media coverage. Similarly, cybersecurity looms as a focus where healthcare’s data-rich dependence is directly impacted. Growing concern about climate and the food supply, sourcing of raw good and materials from China used in drug manufacturing and many other headlines will infer healthcare context.
Summary:
Healthcare will be on the ballot in 2024 and might very well make the difference in who wins and loses in many state and local elections.
It will make a difference in the Presidential campaign as part of the economy and a major focus of government spending. Beyond abortion, the lack of attention to other aspects of the health system in the Milwaukee debate last week should in no way be interpreted as a pass for healthcare insiders.
Voters are restless and healthcare is contributing. Healthcare is far from ‘out of sight, out of mind’ in Campaign 2024.
Albert Einstein determined that time is relative. And when it comes to healthcare, five years can be both a long and a short amount of time.
In August 2018, I launched the Fixing Healthcare podcast. At the time, the medium felt like the perfect auditory companion to the books and articles I’d been writing. By bringing on world-renowned guests and engaging in difficult but meaningful discussions, I hoped the show would have a positive impact on American medicine. After five years and 100 episodes, now is an opportune time to look back and examine how healthcare has improved and in what ways American medicine has become more problematic.
Here’s a look at the good, the bad and the ugly since episode one of Fixing Healthcare:
The Good
Drug breakthroughs and government actions headline medicine’s biggest wins over the past five years.
At first, health experts expressed doubts that Pfizer, Moderna and others could create a safe and effective Covid-19 vaccine with messenger RNA (mRNA) technology. After all, no one had succeeded in more than two decades of trying.
Thanks in part to Operation Warp Speed, the government-funded springboard for research, our nation produced multiple vaccines within less than a year. Previously, the quickest vaccine took four years to develop (mumps). All others required a minimum of five years.
The vaccines were pivotal in ending the coronavirus pandemic, and their success has opened the door to other life-saving drugs, including those that might prevent or fight cancer. And, of course, our world is now better prepared for when the next viral pandemic strikes.
Weight-Loss Drugs
Originally designed to help patients manage Type 2 diabetes, drugs like Ozempic have been helping people reverse obesity—a condition closely correlated with diabetes, heart disease and cancer.
For decades, America’s $150 billion a year diet industry has failed to curb the nation’s continued weight gain. So too have calls for increased exercise and proper nutrition, including restrictions on sugary sodas and fast foods.
In contrast, these GLP-1 medications are highly effective. They help overweight and obese people lose 15 to 25 pounds on average with side effects that are manageable for nearly all users.
The biggest stumbling block to their widespread use is the drug’s exorbitant price (upwards of $16,000 for a year’s supply).
Drug-Pricing Laws
With the Inflation Reduction Act of 2022, Congress took meaningful action to lower drug prices, a move the CBO estimates would reduce the federal deficit by $237 billion over 10 years.
It’s a good start. Americans today pay twice as much for the same medications as people in Europe largely because of Congressional legislation passed in 2003.
That law, the Medicare Prescription Drug Price Negotiation Act, made it illegal for Health and Human Services (HHS) to negotiate drug prices with manufacturers—even for the individuals publicly insured through Medicare and Medicaid.
Now, under provisions of the new Inflation Reduction Act, the government will be able to negotiate the prices of 10 widely prescribed medications based on how much Medicare’s Part D program spends. The lineup is expected to include prescription treatments for arthritis, cancer, asthma and cardiovascular disease. Unfortunately, the program won’t take effect until 2026. And as of now, several legal challenges from both drug manufacturers and the U.S. Chamber of Commerce are pending.
The Bad
Spiking costs, ongoing racial inequalities and millions of Americans without health insurance make up three disappointing healthcare failures of the past five years.
Cost And Quality
The U.S. spends nearly twice as much on healthcare per citizen as other countries, yet our nation lags 10 of the wealthiest countries in medical performance and clinical outcomes. As a result, Americans die younger and experience more complications from chronic diseases than people in peer nations.
As prices climb ever-higher, at least half of Americans can’t afford to pay their out-of-pocket medical bills, which remain the leading cause of U.S. bankruptcy. And with rising insurance premiums alongside growing out-of-pocket expenses, more people are delaying their medical care and rationing their medications, including life-essential drugs like insulin. This creates a vicious cycle that will likely prolong today’s healthcare problems well into the future.
Health Disparities
Inequalities in American medicine persist along racial lines—despite action-oriented words from health officials that date back decades.
Today, patients in minority populations receive unequal and inequitable medical treatment when compared to white patients. That’s true even when adjusting for differences in geography, insurance status and socioeconomics.
Racism in medical care has been well-documented throughout history. But the early days of the Covid-19 pandemic provided several recent and deadly examples. From testing to treatment, Black and Latino patients received both poorer quality and less medical care, doubling and even tripling their chances of dying from the disease.
The problems can be observed across the medical spectrum. Studies show Black women are still less likely to be offered breast reconstruction after mastectomy than white women. Research also finds that Black patients are 40% less likely to receive pain medication after surgery. Although technology could have helped to mitigate health disparities, our nation’s unwillingness to acknowledge the severity of the problem has made the problem worse.
Uninsurance
Although there are now more than 90 million Americans enrolled in Medicaid, there are still 30 million people without any health insurance. This disturbing reality comes a full decade after the passage of the Affordable Care Act.
On Capitol Hill, there is no plan in place to reduce the number of uninsured.
Moreover, many states are looking to significantly rollback their Medicaid enrollment in the post-Covid era. Kaiser Family Foundation estimates that between 8 million and 24 million people will lose Medicaid coverage during the unwinding of the continuous enrollment provisions implemented during the pandemic. Without coverage, people have a harder time obtaining the preventive services they need and, as a result, they suffer more chronic diseases and die younger.
The Ugly
An overall decrease in longevity, along with higher maternal mortality and a worsening mental-health crisis, comprise the greatest failures of U.S. healthcare over the past five years.
Life Expectancy
Despite radical advances in medical science over the past five years, American life expectancy is back to where it was at the turn of the 20th century, according to CDC data.
Alongside environmental and social factors are a number of medical causes for the nation’s dip in longevity. Research demonstrated that many of the 1 million-plus Covid-19 deaths were preventable. So, too, was the nation’s rise in opioid deaths and teen suicides.
Regardless of exact causation, Americans are living two years less on average than when we started the Fixing Healthcare podcast five years ago.
Maternal Mortality
Compared to peer nations, the United States is the only country with a growing rate of mothers dying from childbirth. The U.S. experiences 17.4 maternal deaths per 100,000 live births. In contrast, Norway is at 1.8 and the Netherlands at 3.0.
The risk of dying during delivery or in the post-partum period is dramatically higher for Black women in the United States. Even when controlling for economic factors, Black mothers still suffer twice as many deaths from childbirth as white women.
And with growing restrictions on a woman’s right to choose, the maternal mortality rate will likely continue to rise in the United States going forward.
Mental Health
Finally, the mental health of our country is in decline with rates of anxiety, depression and suicide on the rise.
These problems were bad prior to Covid-19, but years of isolation and social distancing only aggravated the problem. Suicide is now a leading cause of death for teenagers. Now, more than 1 in every 1,000 youths take their own lives each year. The newest data show that suicides across the U.S. have reached an all-time high and now exceed homicides.
Even with the expanded use of telemedicine, mental health in our nation is likely to become worse as Americans struggle to access and afford the services they require.
The Future
In looking at the three lists, I’m reminded of a baseball slugger who can occasionally hit awe-inspiring home runs but strikes out most of the time. The crowd may love the big hitter and celebrate the long ball, but in both baseball and healthcare, failing at the basics consistently results in more losses than wins.
Over the past five years, American medicine has produced a losing record. New drugs and surgical breakthroughs have made headlines, but the deeper, more systemic failures of American healthcare have rarely penetrated the news cycle.
If our nation wants to make the next five years better and healthier than the last five, elected officials and healthcare leaders will need to make major improvements. The steps required to do so will be the focus of my next article.
On July 1st, Georgia will launch its Pathways to Coverage program, which partially expands its Medicaid program to enroll individuals with incomes up to 100 percent of the federal poverty line (FPL), but only if they demonstrate at least 80 hours a month of work, education, job training, or community service.
This expansion is only projected to extend Medicaid coverage to an additional 50K state residents, far short of the 400K that full Medicaid expansion (without work requirements, to individuals earning up to138 percent of the FPL) would have covered. Georgia’s plan was approved by the Trump administration in 2020, but the Biden administration rescinded its waiver prior to implementation. Georgia then sued the Biden administration, and a Federal District Court sided with the state, allowing the partial expansion with work requirements to proceed. The Biden administration chose not to appeal.
The Gist: Though Georgia’s implementation is more limited in scope compared with other states which are currently pursuing Medicaid work requirements, Georgia sets a precedent to motivate those states that are looking to pursue similar strategies.
Research has shown that most adults on Medicaid who do not face barriers to work are already working,and that the cost of systems to monitor beneficiary work status likely offsets any savings in reduced Medicaid spending.
The burden of having to report work status is onerous for potential Medicaid enrollees, discouraging some from seeking coverage altogether.
April 1st marked the start date of a one-year window for state Medicaid offices to reassess their beneficiary rolls, as Medicaid’s continuous enrollment policy sunsets. Since the early days of the pandemic, the federal government has boosted state Medicaid funding by 6.2 percent, in exchange for a requirement that current Medicaid beneficiaries maintain eligibility, regardless of changes to their income or other qualifiers. This policy helped grow national Medicaid enrollment to a record 90M, but a projected 15M may now lose coverage through the redetermination process.
The Gist: After the US uninsured rate recently hit a record low, millions of Americans will now lose insurance coverage, at least temporarily.Of those no longer eligible for Medicaid, an estimated 2.7M will qualify for subsidized exchange plans, while around 400K in non-expansion states will have incomes too high for Medicaid and too low for exchange subsidies. The impact will vary in each state, both in terms of how quickly and how many Medicaid beneficiaries are disenrolled.
But in over half of states,at least one-fifth of those who will lose Medicaid coverage are projected to remain uninsured—a significant step backward in the effort to ensure universal coverage.
Communication from Medicaid offices and exchange plan navigators will be key to preventing as many people as possible from becoming uninsured.
At a meeting with hospital system CEOs last Wednesday, one asked: “has healthcare reached the tipping point?” I replied ‘not yet but it’s getting close.’
I iterated factors that make these times uniquely difficult in every sector:
An uncertain economy that’s unlikely to fully recover until next year.
The growth of Medicaid and Medicare coverage that shifts their financial shortfall to employers and taxpayers who are fed up and pushing back.
A vicious political environment that rewards partisan brinksmanship and focus-group tested soundbites to manipulate voters on complex issues in healthcare.
The growing domination of Big Business in each sector that have used acquisitions + corporatization to their advantage.
The widening role of private equity in funding non-conventional solutions that disrupt the status quo (and the uncertain future for many of these).
The federal courts system that’s increasingly the arbiter over access, fairness, quality and freedoms in healthcare.
The lingering impact of the pandemic.
And growing public disgust and distrust as the system’s altruism and good will is undermined by pervasive concern for profit.
Unprecedented! But events like those last week prompt hitting the pause button: not everyone pays attention to healthcare like many of us. The slaughter of 6 innocents in Nashville hit close to home: it’s about guns, mental health and life and death. The appeal of tech-giants to press the pause button on Generative AI for at least 6 months was sobering. The ravage of tornados that left thousands insecure without food, housing or hope seemed unfair. Mounting tensions with Russia and complex negotiations with China that reminded us that the U.S. competes in a global economy. And President Trump’s court appearance tomorrow will stoke doubt about our justice system at a time when it’s role in healthcare and society is expanding.
I am a healthcare guy. I am prone to see the world through the lens of the U.S. health industry and keen to understand its trends, tipping points and future. There’s plenty to watch: this week will be no exception. The punch list is familiar:
Medicaid coverage: Many will be watching the fallout of from state redetermination requirements for Medicaid coverage starting as soon as this week with disenrollment in Arizona, Arkansas, Idaho, New Hampshire and South Dakota.
Medicare Advantage: Health insurers will be modifying their Medicare Advantage strategies to adapt to CMS’ risk adjustment and Value-based Insurance Design modifications announced last week.
Prescription drug prices: PBMs and drug companies will face growing skepticism as Senate and House committees continue investigations about price gauging and collusion. Hospitals will be making adjustments to higher operating losses as states cut their Medicaid rolls.
Technology: The 7500 VIVA attendees will be doing follow-up to secure entrées for their technologies and solutions among prospective buyers.
Physicians: And physicians will intensify campaigns against insurers and hospitals now seen as adversaries while lobbying Congress for more money and greater income opportunities i.e., physician-owned hospitals.
Hospitals: On the offense against site-neutral payments, physician owned hospitals, drug prices and inadequate reimbursement from health insurers.
All will soldier on but the food fights in healthcare and broader headwinds facing the industry suggest a tipping point might be near.
I am not a fatalist: the future for healthcare is brighter than its past, but not for everyone. Strategies predicated on protecting the past are obsolete. Strategies that consider consumers incapable of active participation in the delivery and financing of their care are archaic. Strategies that depend on unbridled consolidation and opaque pricing are naïve. And strategies that limit market access for non-traditional players are artifacts of the gilded age gone by when each sector protected its own against infidels outside.
These times call for two changes in every board room and C Suite in of every organization in healthcare:
Broader vision: Understanding healthcare’s future in the broader context of American society, democracy and capitalism: Beltway insiders and academics prognosticate based on lag indicators that are decreasingly valid for forecasting. Media pundits on healthcare fail to report context and underpinnings. Management teams are operating under short-term financial incentives lacking longer-term applicability. Consultants are telling C suites what they want to hear. And boards are being mis-educated about trends of consequence that matter. Understanding the future and building response scenarios is out of sight and out of mind to insiders more comfortable being victims than creators of the new normal.
Board leadership: Equipping boards to make tough decisions: Governance in healthcare is not taken seriously unless an organization’s investors are unhappy, margins are shrinking or disgruntled employees create a stir. Few have a systematic process for looking at healthcare 10 years out and beyond their business. Every Board must refresh its thinking about what tomorrow in healthcare will be and adjust. It’s easier for board to approve plans for the near-term than invest for the long-term: that’s why outsiders today will be tomorrow’s primary incumbents.
So, is U.S healthcare near its tipping point? I don’t know for sure, but it seems clear the tipping point is nearer than at any point in its history. It’s time for fresh thinking and new players.
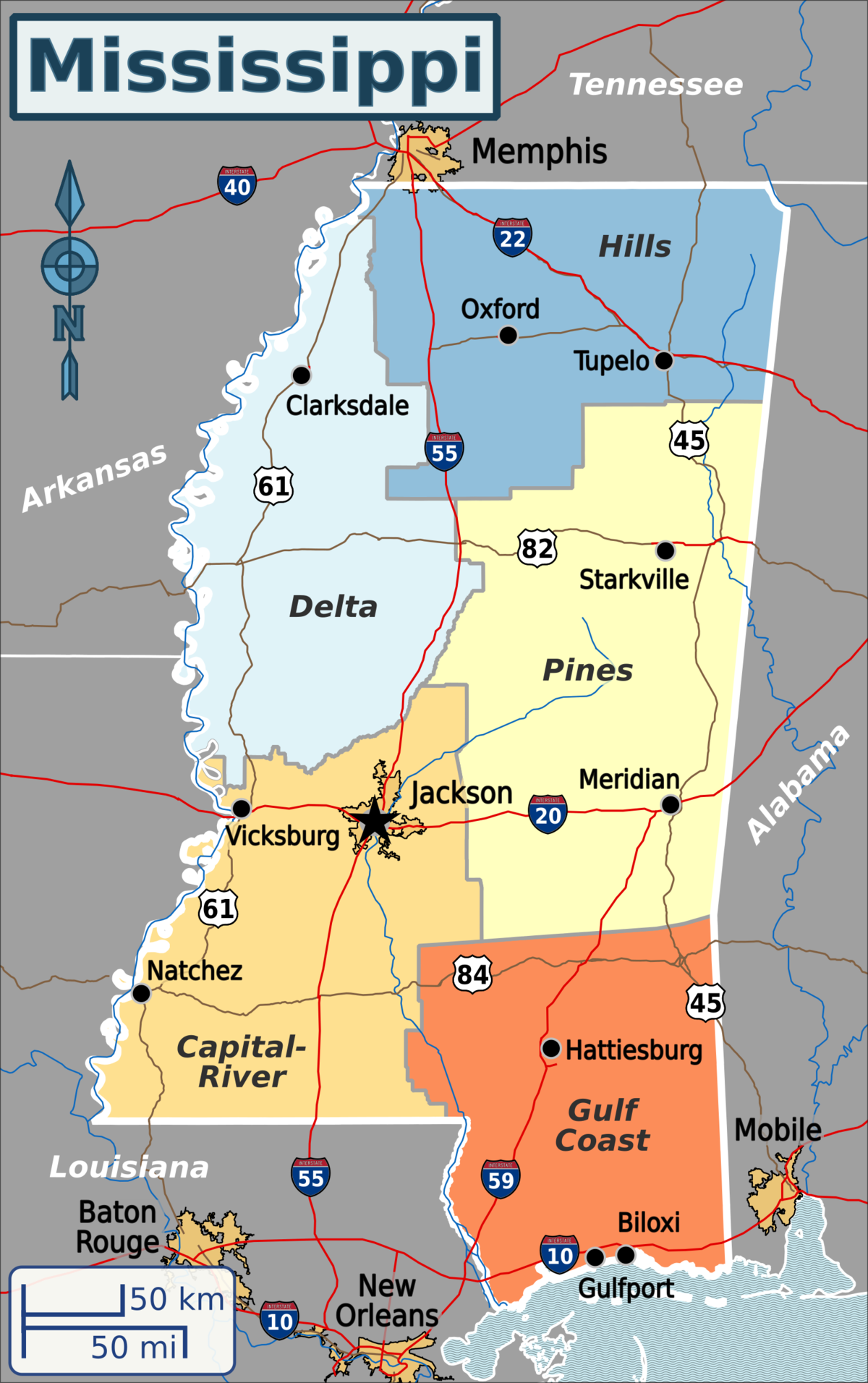
Published this week in the New York Times, this article describes the decaying state of Greenwood Leflore Hospital, a 117 year-old facility in the Mississippi Delta that may be within months of closure. While rural hospitals across the country are struggling, Mississippi’s firm opposition to Medicaid expansion has exacerbated the problem in that state, by depriving providers of an additional $1.4B per year in federal funds. Instead, only a few of the state’s 100-plus hospitals actually turn an annual profit, and uncompensated care costs are almost 10 percent of the average hospital’s operating costs.
Despite a dozen or more hospitals at imminent risk of closure, Mississippi officials would rather use the state’s $3.9B budget surplus to lower or eliminate the state income tax.
The Gist:Expanding Medicaid doesn’t just reduce rates of uncompensated care provided by hospitals, it changes the volume and type of care they provide.
Further, Medicaid expansion has been found to result in significant reductions in all-cause mortality.
Ensuring that low-income residents in Mississippi and other non-expansion states have access to Medicaid would allow providers to administer more preventive care and manage chronic diseases more effectively, before costly exacerbations require hospitalization.
Researchers estimate 15 million people will lose their Medicaid starting April 1 when states begin removing people from the low-income health insurance program for the first time in three years.
In March 2020, Congress banned states from removing people from Medicaid during the pandemic in exchange for more federal funding for state Medicaid programs. Medicaid enrollment is usually tied to people’s incomes, and individuals normally have to regularly prove they still qualify in what’s known as a redetermination. (In the 39 states and Washington, D.C., that have expanded Medicaid, a family of four has to make less than $40,000 to qualify. In non-expansion states, the cutoff is even lower.)
With redeterminations paused, Medicaid enrollment nationwide has grown from 71 million in February 2020 to an estimated 95 million in March 2023.Research shows Medicaid coverage is associated with better access to care, more financial security, better health and lower mortality. During the pandemic, beneficiaries have been able to enjoy these benefits without worrying about confirming their eligibility.
In December, Congress voted to let states restart the process of clearing their rolls on April 1, what’s sometimes referred to as “unwinding.”Lawmakers are giving states 14 months to redetermine millions of people’s eligibility — an unprecedented task made even more difficult by serious staffing and experience shortages in many Medicaid offices.
“It’s going to be a big lift,” said Sayeh Nikpay, a health policy researcher at the University of Minnesota and Tradeoffs Senior Research Advisor. “States have never had to do this many redeterminations this quickly before, and there’s a lot of uncertainty about what will happen.”
We asked Nikpay to pick out a few relevant studies to help us understand what is happening and how states and employers could keep more people insured. Here are three she identified as particularly helpful.
Two types of people will lose coverage
The Office of the Assistant Secretary for Planning and Evaluation, which provides research for the U.S. Department of Health and Human Services, released a report in August 2022 that estimated 15 million people will lose Medicaid coverage as a result of the unwinding. (The estimate is similar to another analysis by the independent Urban Institute.)
ASPE breaks those 15 million people into two groups. In the first group are people who make too much money to qualify for Medicaid. ASPE estimates there are about 8 million people in that category, and they should be able to get insurance through work or the Obamacare exchanges.
In the second group are roughly 7 million people ASPE estimates are still eligible but will lose coverage because of what’s called “administrative churn.”This can happen if the Medicaid office can’t get in touch with someone to confirm their eligibility because they’ve moved or changed their phone number or if they’re unable to make an in-person appointment because of work or child care responsibilities. (The Urban Institute projects about 4 million people will be in this group.)
These two groups represent a key tension to the unwinding process: States want to shed people who make too much money, but officials also know eligible people often lose coverage during redeterminations, and that danger is heightened given the scale and speed of this process.
Making the switch from Medicaid to private insurance
This next paper looks at the first group: the roughly 8 million people expected to move from Medicaid to private coverage, and specifically the roughly 4 million who are expected to get coverage through the Obamacare exchanges. Adrianna McIntyre, an assistant professor of health policy at Harvard, wrote in JAMA Health Forum in October 2022 about the most effective ways to move people from Medicaid onto private Obamacare plans.
There’s limited data on this, but based on the few studies available, McIntyre found that only 3 to 5 percent of people who leave Medicaid end up getting an Obamacare plan. Many policymakers are relying on the Obamacare exchanges to provide a life preserver to millions of people losing Medicaid coverage, but the research cited by McIntyre shows getting people into these plans is not guaranteed and will take focused effort by states.
McIntyre’s review cites several randomized controlled trials where states tested different ways of increasing enrollment in Obamacare plans. These studies found simple reminders from the state – like physical letters, emails and phone calls help – boost sign-ups anywhere from 7 to 16 percent.
But what really seems to make a difference is reminders plus connecting people to someone who can get them signed up while they are on the phone. In one of those trials published in 2022, people in California who got a reminder email and a call connecting them to enrollment assistance were almost 50% more likely to sign up for a plan. Such extra effort is obviously costly, and it may not be a priority or financially feasible for some states.
McIntyre’s review did not include any research on what employers can do to help their workers transition from Medicaid to work-based coverage, but based on the studies McIntyre cited, Nikpay said she thinks it’s a good idea for employers to make sure people know Medicaid could be going away and provide as much help as possible in getting new coverage.
Making it easier to stay on Medicaid can have other benefits
The final study looks at the second group of people expected to lose Medicaid coverage: the 7 million people who may lose coverage due to administrative churn even though they are still eligible.
Some states have tried to limit that churn, and researchers at the RAND Corporation evaluated New York’s effort. Starting in 2014, New York allowed people to stay on Medicaid without any redeterminations for 12 months once enrolled.
In addition to keeping more people on Medicaid for longer, researchers found that after this policy was in place, hospital admissions and monthly costs per beneficiary went down. The researchers can’t say whether the continuous enrollment policy directly caused these improved outcomes, but the findings suggest that avoiding administrative churn can help people stay covered without ballooning costs.
“It seems reasonable to me,” Nikpay said of the findings, “that making it easier to stay on Medicaid, even outside of a global pandemic, could benefit people’s health given what we know about how Medicaid affects people.”
Since its opening in a converted wood-frame mansion 117 years ago, Greenwood Leflore Hospital had become a medical hub for this part of Mississippi’s fertile but impoverished Delta, with 208 beds, an intensive-care unit, a string of walk-in clinics and a modern brick-and-glass building.
But on a recent weekday, it counted just 13 inpatients clustered in a single ward. The I.C.U. and maternity ward were closed for lack of staffing and the rest of the building was eerily silent, all signs of a hospital savaged by too many poor patients.
Greenwood Leflore lost $17 million last year alone and is down to a few million in cash reserves, said Gary Marchand, the hospital’s interim chief executive. “We’re going away,” he said. “It’s happening.”
Rural hospitals are struggling all over the nation because of population declines, soaring labor costs and a long-term shift toward outpatient care. But those problems have been magnified by a political choice in Mississippi and nine other states, all with Republican-controlled legislatures.
They have spurned the federal government’s offer to shoulder almost all the cost of expanding Medicaid coverage for the poor. And that has heaped added costs on hospitals because they cannot legally turn away patients, insured or not.
Opponents of expansion, who have prevailed in Texas, Florida and much of the Southeast, typically say they want to keep government spending in check. States are required to put up 10 percent of the cost in order for the federal government to release the other 90 percent.
But the number of holdouts is dwindling. On Monday, North Carolina became the 40th state to expand Medicaidsince the option to cover all adults with incomes below 138 percent of the poverty line opened up in 2014 under the terms of the 2010 Affordable Care Act. The law, a major victory for President Barack Obama, has continued to defy Republican efforts to kill or limit it.
“This argument about rural hospital closures has been an incredibly compelling argument to voters,” said Kelly Hall, the executive director of the Fairness Project, a national nonprofit that has successfully pushed ballot measures to expand Medicaid in seven states.
In Mississippi, one of the nation’s poorest states, the missing federal health care dollars have helped drive what is now a full-blown hospital crisis. Statewide, experts say that no more than a few of Mississippi’s 100-plus hospitals are operating at a profit. Free care is costing them about $600 million a year, the equivalent of 8 percent to 10 percent of their operating costs — a higher share than almost anywhere else in the nation, according to the state hospital association.
Expanding Medicaid would uncork a spigot of about $1.35 billion a year in federal funds to hospitals and health care providers, according to a 2021 report by the office of the state economist.
And it would guarantee medical coverage to some 100,000 uninsured adults making less than $20,120 a year in a state whose death rates are at or near the nation’s highest for heart disease, stroke, diabetes, cancer, kidney disease and pneumonia. Infant mortality is also sky-high, and the Delta has the nation’s highest rate of foot and leg amputations because of diabetes or hypertension.
Health officials blame those numbers in part on the high rate of uninsured residents who miss out on preventive care.
“I can tell you I have a number of patients who are on dialysis with renal failure for the rest of their life because they couldn’t afford the medication for their blood pressure, and that caused their kidneys to go bad,” said Dr. John Lucas, a Greenwood Leflore surgeon.
Among Mississippi adults, only disabled people and parents with extremely low incomes, along with most pregnant women, are eligible for Medicaid. Many of the ineligible are also too poor to qualify for the tax credits for insurance under the Affordable Care Act, leaving them without affordable options.
The same is true for close to two million other Americans who live in the states that have not expanded Medicaid. Three in five are adults of color, according to a 2021 study by the Center on Budget and Policy Priorities, a nonprofit research group. In Mississippi, more than half are Black.
Gov. Tate Reeves, a Republican, and key G.O.P. state lawmakers argue that a bigger Mississippi program is not in taxpayers’ best interest. The governor says the state’s $3.9 billion surplus would be best used to help eliminate Mississippi’s income tax.
“Don’t simply cave under the pressure of Democrats and their allies in the media who are pushing for the expansion of Obamacare, welfare and socialized medicine,” Mr. Reeves said in his annual State of the State address in January.
Opponents also argue that the newly insured would become dependent on Medicaid and therefore be less likely to work. “I believe we should be working to get people off Medicaid as opposed to adding more people to it,” said Philip Gunn, the powerful Republican House speaker.
Yet in Mississippi’s Delta, a flat swath of fields of corn, soybeans and other crops nearly as big as Delaware, access to any kind of medical care is drying up for lack of money. More than 300,000 people live here, nearly 35 percent of them Black. About the same percentage live in poverty, a rate three times the national average.
Dr. Daniel P. Edney, the state’s top health officer, said he did not set Medicaid policy, and he has been careful not to take sides. But he predicted emerging health care deserts where women would have to travel long distances to deliver babies and more sick people would die because they could not gain access to care.
Of the state’s hospitals, “I have maybe heard of two that are generating any profit,” he said. When he asks hospital executives if Medicaid expansion would help their balance sheets, he said, “they say it’s a game changer.”
He predicted that five hospitals would soon downgrade into mere emergency rooms, where doctors work to stabilize patients, then transfer them to the nearest hospital.
If that happens, some of the sickest will not make it, said Dr. Jeff Moses, an emergency room physician at Greenwood Leflore.
“Where are they going? Davy Jones’s locker,” he said. “It is very dark, and I’m not exaggerating this. I just can’t imagine what will happen to this community if this hospital closes.”
Nine years after states began expanding Medicaid, evidence is growing that broader coverage saves lives. In a 2021 analysis, researchers for the National Bureau of Economic Research estimated that in one four-year period, 19,200 more adults aged 55 to 64 survived because of expanded coverage, and nearly 16,000 more would have lived if that coverage was nationwide.
Other studies suggest why: Making medical care more affordable led to increases in regular checkups, cancer screenings, diagnoses of chronic diseases and prescriptions for needed medicines.
Especially during the first six years of the Medicaid expansion, when the federal government picked up 95 to 100 percent of the cost, many states found that the program was a net fiscal gain. Some states have imposed taxes on hospitals or health care providers to cover their share of the expense, the same strategy used to help fund other Medicaid costs.
Now the federal government is offering a new incentive for the holdouts: As part of a 2021 pandemic relief measure, it agreed to temporarily pay a higher proportion of costs for some existing Medicaid patients if states broadened eligibility.
Mississippi’s office of the state economist has estimated that for at least the first decade, those savings and others would fully cover the roughly $200 million a year that Medicaid expansion would cost the state government.
Tim Moore, the president of the Mississippi Hospital Association, said expansion was “a no-brainer.” The state is so poor, he said, that for every dollar it spends on Medicaid, the federal government pumps four back in.
Polls, including by Mississippi Today and Siena College, appear to show Mississippians support Medicaid expansion, regardless of their political affiliation. Brandon Presley, the Democratic candidate for governor, is highlighting hospital closures as a reason to deny Mr. Reeves a second term in elections this November.
In a possible sign of political nervousness, the governor and the legislature recently agreed to extend Medicaid coverage to pregnant women for 12 months after they give birth, prolonging a federal pandemic-era policy.
The legislators are also trying to prop up the hospitals with a one-time infusion of $83 million or more. But that is a pittance compared with what the state has given up in Medicaid payments.
The state has lost four hospitals since 2008, according to the hospital association, and Dr. Edney, the state health officer, said that it would inevitably lose more. He said he worried most about health care access in the Delta, where he grew up, the child of working-class parents with no health insurance.
On Saturday, Representative Bennie Thompson, Democrat of Mississippi, said victims of a tornado that struck the Delta last week had to be ferried 50 miles away for medical treatment because the local hospital had no power. More Medicaid dollars, he said, would have equipped it with an emergency generator.
An hour due west from Greenwood Leflore, another major hospital, run by Delta Health System, is also in serious trouble. Licensed for more than 300 beds, the hospital one day last month held just 72 inpatients.
Thirty-two of them were kept in the emergency department, partly because of nursing cuts. One upshot is that patients seeking emergency care now wait an average of two hours, four times as long as they should, according to Amy Walker, the chief nursing officer. Some simply walk out.
The neonatal intensive care unit closed last July. Now babies in trouble must be ferried by ambulance or helicopter 125 miles south to Jackson.
Iris Stacker, the chief executive, said the hospital could remain open through the end of the year; after that, she makes no promises. She is hoping federal grants will help keep the doors open, despite the state’s failure to expand Medicaid.
But she said, “It’s very hard to ask the federal government for more money when you have this pot of money sitting here that we won’t touch.”
A top message on Greenwood Leflore’s website is now a request for donations. So far, the hospital has raised less than $12,000.
Mike Hardin, a 70-year-old retiree, was one of a handful of inpatients one recent day. He had come to the emergency room two days before with slurred speech. Doctors quickly diagnosed a stroke and now were sending him home with revised medications.
“They have to do something to keep this hospital open,” he said as he was wheeled out of his room. “The people around this area wouldn’t have any place else to go.”
The hospital’s outpatient clinics are largely still in business, and doctors there say their caseloads are full of impoverished patients who should have been treated earlier.
Dr. Abhash Thakur, a cardiologist, said he routinely saw patients in the late stages of congestive heart failure who had never seen a cardiologist or been prescribed heart medication. Some have as little as 10 percent of their heart function left.
“They are not the exception,” he said, before examining a 52-year-old man who uses a wheelchair because of his heart disease. “Every day, probably, I will see a few of them.”
Dr. Raymond Girnys, a general surgeon, had just treated a man in his late 50s. He said that a week earlier, the man had punctured his foot on a sharp stick while walking in his tennis shoes in a field.
The man did not seek medical attention until the foot became infected because he was poor and uninsured. Dr. Girnys pointed out the irony: If his patient lost his foot, he would become eligible for Medicaid because then he would be disabled.
“If they had insurance, they wouldn’t be afraid to seek care,” he said.
Experts say that no more than a few of Mississippi’s 100-plus hospitals are operating at a profit.