A key Medicare advisory panel is calling for a 2% bump to Medicare payments for acute care hospitals for 2022 but no hike for physicians.
The report, released Monday from the Medicare Payment Advisory Commission (MedPAC)—which recommends payment policies to Congress—bases payment rate recommendations on data from 2019. However, the commission did factor in the pandemic when evaluating the payment rates and other policies in the report to Congress, including whether policies should be permanent or temporary.
“The financial stress on providers is unpredictable, although it has been alleviated to some extent by government assistance and rebounding service utilization levels,” the report said.
MedPAC recommended that targeted and temporary funding policies are the best way to help providers rather than a permanent hike for payments that gets increased over time.
“Overall, these recommendations would reduce Medicare spending while preserving beneficiaries’ access to high-quality care,” the report added.
MedPAC expects the effects of the pandemic, which have hurt provider finances due to a drop in healthcare use, to persist into 2021 but to be temporary.
It calls for a 2% update for inpatient and outpatient services for 2022, the same increase it recommended for 2021.
The latest report recommends no update for physicians and other professionals. The panel also does not want any hikes for four payment systems: ambulatory surgical centers, outpatient dialysis facilities, skilled nursing facilities and hospices.
MedPAC also recommends Congress reduce the aggregate hospice cap by 20% and that “ambulatory surgery centers be required to report cost data to [Centers for Medicare & Medicaid Services (CMS)],” the report said.
But it does call for long-term care hospitals to get a 2% increase and to reduce payments by 5% for home health and inpatient rehabilitation facilities.
The panel also explores the effects of any policies implemented under the COVID-19 public health emergency, which is likely to extend through 2021 and could continue into 2022.
For instance, CMS used the public health emergency to greatly expand the flexibility for providers to be reimbursed for telehealth services. Use of telehealth exploded during the pandemic after hesitancy among patients to go to the doctor’s office or hospital for care.
“Without legislative action, many of the changes will expire at the end of the [public health emergency],” the report said.
MedPAC recommends Congress temporarily continue some of the telehealth expansions for one to two years after the public health emergency ends. This will give lawmakers more time to gather evidence on the impact of telehealth on quality and Medicare spending.
“During this limited period, Medicare should temporarily pay for specified telehealth services provided to all beneficiaries regardless of their location, and it should continue to cover certain newly-covered telehealth services and certain audio-only telehealth services if there is potential for clinical benefit,” according to a release on the report.
After the public health emergency ends, Medicare should also return to paying the physician fee schedule’s facility rate for any telehealth services. This will ensure Medicare can collect data on the cost for providing the services.
“Providers should not be allowed to reduce or waive beneficiary cost-sharing for telehealth services after the [public health emergency],” the report said. “CMS should also implement other safeguards to protect the Medicare program and its beneficiaries from unnecessary spending and potential fraud related to telehealth.”
In their recent Health Affairs paper, Sungchul Park and coauthors examine rates of switching from Medicare Advantage (MA) to traditional Medicare by patient characteristics. MA plans are the private insurance alternative to traditional fee-for-service Medicare overseen by the Centers for Medicare and Medicaid Services. While enrollment in MA has doubled over the past decade, Park and coauthors find that the needs of certain enrollees are not being met by MA plans.
Park and coauthors report that rural enrollees switch from MA to traditional Medicare at an adjusted annual rate of 10.5 percent, significantly higher than metropolitan residents, who switch at a rate of 5.0 percent.
This phenomenon was more pronounced among those who required the use of costly services such as facility stays or hospitalizations, those who had poor self-reported health, and individuals who reported lower satisfaction with their access to care.
The payment gap was $63,000 for primary care doctors, $178,000 for medical specialists and $150,000 for surgeons.
Doctors who work for hospital outpatient facilities get much higher payments for their services from Medicare than doctors who practice independently, according to a new study.
The research, based on Medicare claims data from 2010-2016,found that the program’s payments for doctors’ work were, on average, $114,000 higher per doctor per year when billed by a hospital than when billed by a doctor’s independent practice.
Published in Health Services Research, results found that the amount Medicare would pay for outpatient care at doctors’ offices would have been 80% higher if the services had been billed by a hospital outpatient facility. In 2010, the average set of Medicare services independent doctors performed annually for patients was worth $141,000, but charging for the same group of services would have grossed $240,000 if a hospital outpatient facility billed for them.
The payment difference varied by specialty. The payment gap was $63,000 for primary care doctors, $178,000 for medical specialists and $150,000 for surgeons.
Moreover, the study found the differential grew over time. From 2010-2016, the average difference between hospital outpatient and private practice payments grew from 80% higher to 99% higher.
WHAT’S THE IMPACT?
The main reason for these large payment differences: facility fees. For each service a doctor performs, Medicare pays hospital outpatient facilities both a fee for the doctor’s work and a fee for the facility, whereas private practices receive only doctor fees.
Although the doctor fees are a bit lower in hospital outpatient locations, the facility fees more than make up for the difference, and the total payments to hospitals are reflected in higher doctor salaries and bonuses.
The Centers for Medicare and Medicaid Services has been trying to correct this imbalance for years with policies that would pay both sites the same amount. In 2015, the Bipartisan Budget Act authorized CMS to impose site-neutral payments but grandfathered existing hospital outpatient facilities. Later, CMS expanded the equal payments to other hospital outpatient facilities, but the American Hospital Association sued to overturn this regulation.
In July 2020, the Appeals Court sided with HHS. The American Hospital Association and the Association of American Medical Colleges said they would seek to have the ruling overturned.
The groups filed for a petition for a rehearing, which was denied.
In February, the Supreme Court acknowledged the AHA’s request for judicial review. The government response was due by March 15, but on March 3, Norris Cochran, acting Secretary of Health and Human Service asked for an extension until April 14 to file the government’s response, according to court documents.
The significant difference between Medicare payments to hospital outpatient facilities and independent offices has encouraged hospitals and health systems to buy doctor practices, but the study noted that good research about this has been lacking up to now.
It found little evidence of a direct relationship linking the size of the pay gap between hospital outpatient facilities and independent offices, with hospitals buying doctor practices, in particular medical specialties. But it did find that doctors whose services had larger pay gaps were more likely to have a hospital buy their practice than doctors whose services had a smaller pay gap.
In an accompanying commentary, Dr. Michael Chernew of Harvard Medical School in Boston said the study had found that the ability of hospitals and employed doctors to earn more from Medicare had resulted in a greater amount of integration.
THE LARGER TREND
However, the authors pointed out that the Medicare payment difference is only one of many factors that have contributed to the huge increase in the share of doctors employed at hospitals over the past decade. For example, they found a higher probability of a doctor going to work for a hospital in highly concentrated hospital markets and rural areas.
Other studies, they said, have established that some health systems use integration with doctors’ offices as a bargaining chip with commercial health insurance plans. Also, some doctors may find that independent practice is less viable than it used to be for a variety of reasons.
It has also been suggested that many younger doctors prefer hospital employment to private practice because they crave economic security and work-life balance.
It’s been estimated that even the payments to hospitals vs. doctors could save CMS $11 billion over 10 years. But the paper illustrates that the payment disparities can also create broader market distortions because consolidation of hospitals and doctors’ offices has been shown to lead to higher prices overall.
The Medicare Act “prohibits Medicare payment for services that are not furnished within the United States,” according to the filing.
RemoteICU, a telemedicine provider group, is suing the Department of Health and Human Services and the Centers for Medicare and Medicaid Services for not reimbursing telehealth services provided by physicians who are located outside the United States, according to a federal lawsuit filed last week in Washington.
RICU wants reimbursement for telehealth services provided within the U.S., but not necessarily by a physician who lives within its borders.
The company employs physicians who live outside the country, but are U.S. board-certified critical-care specialists and licensed in one or more U.S. jurisdictions. With RICU’s telecommunications system, these physicians can provide critical-care services in U.S. hospital ICUs, the lawsuit said.
“Although RICU’s physicians live abroad, they serve as full-time, permanent staff members of the U.S. hospitals at which they serve patients,” the company said in the court filing.
“By employing U.S.-licensed intensivists who live overseas, RICU has enabled the American healthcare system to recapture talent that would otherwise be lost to it – and this has helped to alleviate the ongoing shortage of intensivists in American hospitals.“
When CMS expanded the list of telehealth services for which it reimbursed in December 2020 to include critical care services, RICU began offering its physicians to hospitals that couldn’t afford ICU telehealth without Medicare reimbursement, the court filing said.
However, after the company reached out to several officials from HHS and CMS, it was notified that Medicare could not reimburse the client hospitals for RICU’s services, because the Medicare Act “prohibits Medicare payment for services that are not furnished within the United States,” according to the filing.
The company is seeking a preliminary injunction to stop HHS and CMS from denying Medicare reimbursement for telehealth services on the basis of a provider’s physical location outside of the United States at the time of service.
WHAT’S THE IMPACT?
RICU claims that, by failing to reimburse for the critical care telehealth services provided by its physicians, HHS and CMS are causing “immediate harm both to RICU and to the public.”
It argues that it’s filling a gap in critical care that has been exacerbated by the pandemic.
“There remains [a] significant unmet need for critical care services, as desperately sick patients have overwhelmed ICU resources across the country,” RICU said in the court filing.
“In some cases, lack of adequate care can mean the difference between life or death. And one of the groups most at risk from death and serious illness due to COVID-19 is the elderly – the very same population that relies upon Medicare.”
Without reimbursement, RICU says that some of its current clients, as well as potential customers, will not be able to offer its services.
The company argues that this causes “significant, unrecoverable monetary damages” because tele-ICU providers that use physicians located within the U.S. are eligible for reimbursement and therefore have a competitive edge over RICU.
Further, it says that it has already begun losing business because of hospitals’ inability to receive Medicare reimbursement.
THE LARGER TREND
CMS has widely expanded the list of telehealth services it will reimburse for during the pandemic to include services such as emergency department visits, initial inpatient and nursing facility visits, and discharge-day management.
While only 14 states currently have true “payment parity” for telehealth, 43 states and D.C. have implemented a telemedicine coverage law, according to Foley & Lardner report.
That report, among others, claims telehealth will continue to grow as an integral part of healthcare as time goes on.
Last year, Geisinger health system in Danville, Pennsylvania, implemented telehealth ICU technology in several of its hospitals to support its in-person clinical staff.
ON THE RECORD
“The Critical Care Ban is causing irreparable harm to RICU, which is suffering ongoing financial and reputational harms that cannot be remedied in the future,” the court filing said.
“The balance of the equities favors an injunction, because Defendants have already admitted that there is a desperate medical need for the critical care that RICU would provide but for the Critical Care Ban.
“And, finally, preliminary injunction would be in the public interest because, across the United States, Americans stricken by the COVID-19 pandemic are in desperate need of critical care – a need that RICU can help meet. It is not hyperbole to say that the requested injunctive relief is in the public interest because it could save lives.”
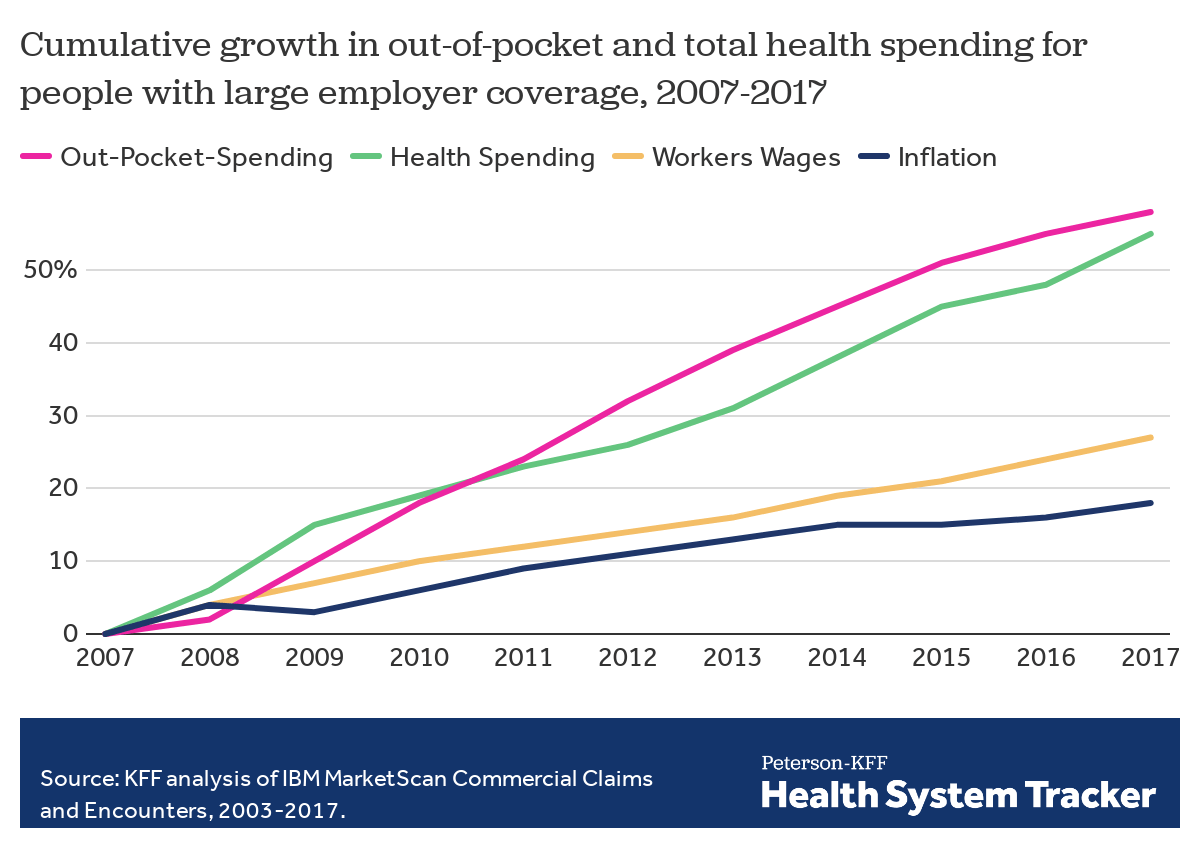
Employers — including companies, state governments and universities — purchase health care on behalf of roughly 150 million Americans. The cost of that care has continued to climb for both businesses and their workers.
For many years, employers saw wasteful care as the primary driver of their rising costs. They made benefits changes like adding wellness programs and raising deductibles to reduce unnecessary care, but costs continued to rise. Now, driven by a combination of new research and changing market forces — especially hospital consolidation — more employers see prices as their primary problem.
By amassing and analyzing employers’ claims data in innovative ways, academics and researchers at organizations like the Health Care Cost Institute (HCCI) and RAND have helped illuminate for employers two key truths about the hospital-based health care they purchase:
1) PRICES VARY WIDELY FOR THE SAME SERVICES
Data show that providers charge private payers very different prices for the exact same services — even within the same geographic area.
For example, HCCI found the price of a C-section delivery in the San Francisco Bay Area varies between hospitals by as much as:$24,107
Data show that hospitals charge employers and private insurers, on average, roughly twice what they charge Medicare for the exact same services. A recent RAND study analyzed more than 3,000 hospitals’ prices and found the most expensive facility in the country charged employers:4.1xMedicare
Hospitals claim this price difference is necessary because public payers like Medicare do not pay enough. However, there is a wide gap between the amount hospitals lose on Medicare (around -9% for inpatient care) and the amount more they charge employers compared to Medicare (200% or more).
Employer Efforts
A small but growing group of companies, public employers (like state governments and universities) and unions is using new data and tactics to tackle these high prices. (Learn more about who’s leading this work, how and why by listening to our full podcast episode in the player above.)
Note that the employers leading this charge tend to be large and self-funded, meaning they shoulder the risk for the insurance they provide employees, giving them extra flexibility and motivation to purchase health care differently. The approaches they are taking include:
Steering Employees
Some employers are implementing so-called tiered networks, where employees pay more if they want to continue seeing certain, more expensive providers. Others are trying to strongly steer employees to particular hospitals, sometimes know as centers of excellence, where employers have made special deals for particular services.
Purdue University, for example, covers travel and lodging and offers a $500 stipend to employees that get hip or knee replacements done at one Indiana hospital.
Negotiating New Deals
There is a movement among some employers to renegotiate hospital deals using Medicare rates as the baseline — since they are transparent and account for hospitals’ unique attributes like location and patient mix — as opposed to negotiating down from charges set by hospitals, which are seen by many as opaque and arbitrary. Other employers are pressuring their insurance carriers to renegotiate the contracts they have with hospitals.
In 2016, the Montana state employee health plan, led by Marilyn Bartlett, got all of the state’s hospitals to agree to a payment rate based on a multiple of Medicare. They saved more than $30 million in just three years. Bartlett is now advising other states trying to follow her playbook.
In 2020, several large Indiana employers urged insurance carrier Anthem to renegotiate their contract with Parkview Health, a hospital system RAND researchers identified as one of the most expensive in the country. After months of tense back-and-forth, the pair reached a five-year deal expected to save Anthem customers $700 million.
Legislating, Regulating, Litigating
Some employer coalitions are advocating for more intervention by policymakers to cap health care prices or at least make them more transparent. States like Colorado and Indiana have passed price transparency legislation, and new federal rules now require more hospital price transparency on a national level. Advocates expect strong industry opposition to stiffer measures, like price caps, which recently failed in the Montana legislature.
Other advocates are calling for more scrutiny by state and federal officials of hospital mergers and other anticompetitive practices. Some employers and unions have even resorted to suing hospitals like Sutter Health in California.
Employer Challenges
Employers face a few key barriers to purchasing health care in different and more efficient ways:
Provider Power
Hospitals tend to have much more market power than individual employers, and that power has grown in recent years, enabling them to raise prices. Even very large employers have geographically dispersed workforces, making it hard to exert much leverage over any given hospital. Some employers have tried forming purchasing coalitions to pool their buying power, but they face tricky organizational dynamics and laws that prohibit collusion.
Sophistication
Employers can attempt to lower prices by renegotiating contracts with hospitals or tailoring provider networks, but the work is complicated and rife with tradeoffs. Few employers are sophisticated enough, for example, to assess a provider’s quality or to structure hospital payments in new ways.Employers looking for insurers to help them have limited options, as that industry has also become highly consolidated.
Employee Blowback
Employers say they primarily provide benefits to recruit and retain happy and healthy employees. Many are reluctant to risk upsetting employees by cutting out expensive providers or redesigning benefits in other ways. A recent KFF survey found just 4% of employers had dropped a hospital in order to cut costs.
The Tradeoffs
Employers play a unique role in the United States health care system, and in the lives of the 150 million Americans who get insurance through work. For years, critics have questioned the wisdom of an employer-based health care system, and massive job losses created by the pandemic have reinforced those doubts for many.
Assuming employers do continue to purchase insurance on behalf of millions of Americans, though, focusing on lowering the prices they pay is one promising path to lowering total costs. However, as noted above, hospitals have expressed concern over the financial pressures they may face under these new deals. Complex benefit design strategies, like narrow or tiered networks, also run the risk of harming employees, who may make suboptimal choices or experience cost surprises. Finally, these strategies do not necessarily address other drivers of high costs including drug prices and wasteful care.
The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers(about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providersdon’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment.That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services.The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
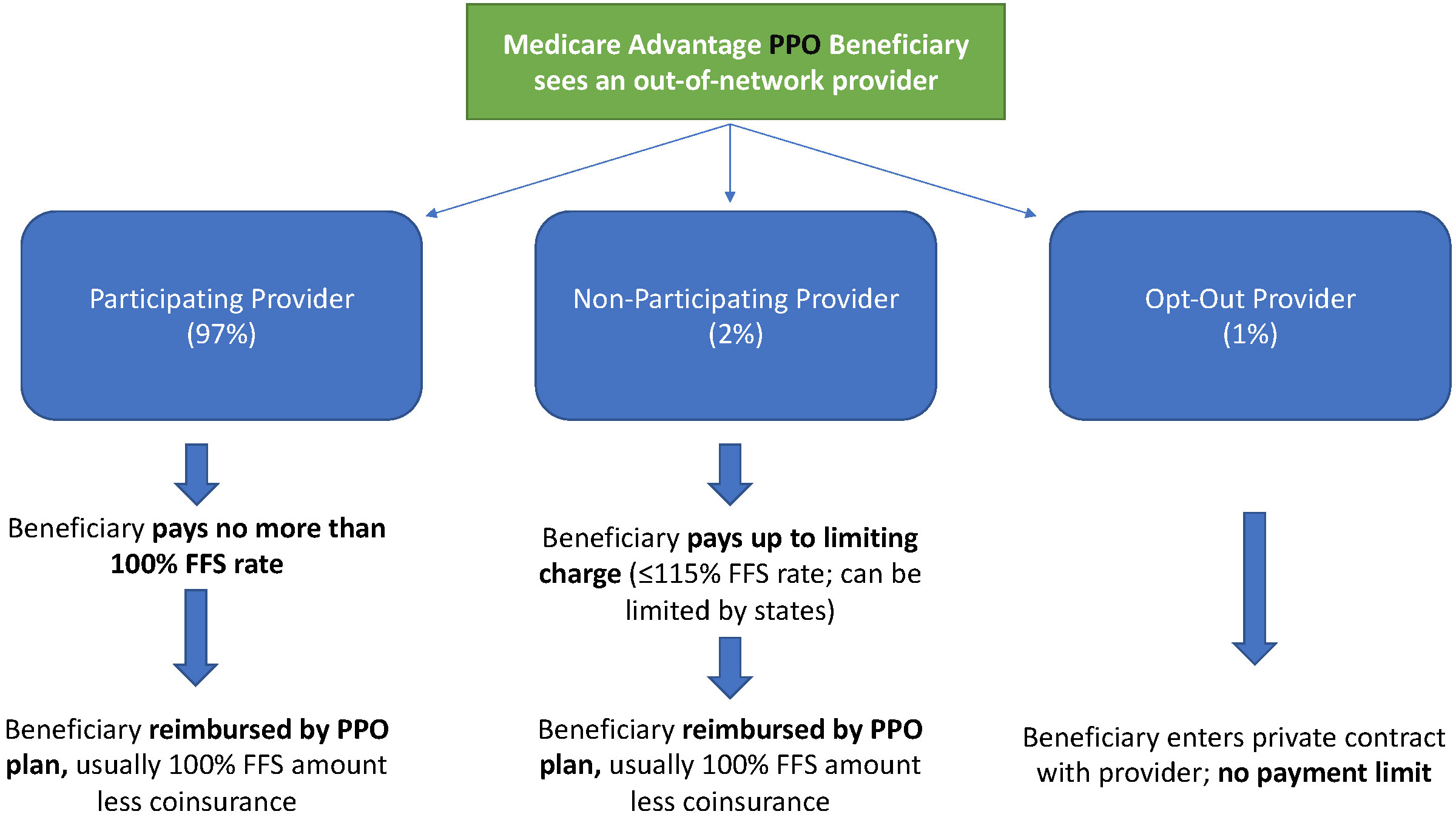
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (SeeFigure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.
The federal government has penalized 774 hospitals for having the highest rates of patient infections or other potentially avoidable medical complications.Those hospitals, which include some of the nation’s marquee medical centers, will lose 1% of their Medicare payments over 12 months.
The penalties, based on patients who stayed in the hospitals anytime between mid-2017 and 2019, before the pandemic, are not related to covid-19. They were levied under a program created by the Affordable Care Act that uses the threat of losing Medicare money to motivate hospitals to protect patients from harm.
On any given day, one in every 31 hospital patients has an infection that was contracted during their stay, according to the Centers for Disease Control and Prevention. Infections and other complications can prolong hospital stays, complicate treatments and, in the worst instances, kill patients.
“Although significant progress has been made in preventing some healthcare-associated infection types, there is much more work to be done,” the CDC says.
Now in its seventh year, the Hospital-Acquired Condition Reduction Program has been greeted with disapproval and resignation by hospitals, which argue that penalties are meted out arbitrarily. Under the law, Medicare each year must punish the quarter of general care hospitals with the highest rates of patient safety issues. The government assesses the rates of infections, blood clots, sepsis cases, bedsores, hip fractures and other complications that occur in hospitals and might have been prevented. The total penalty amount is based on how much Medicare pays each hospital during the federal fiscal year — from last October through September.
Hospitals can be punished even if they have improved over past years — and some have. At times, the difference in infection and complication rates between the hospitals that get punished and those that escape punishment is negligible, but the requirement to penalize one-quarter of hospitals is unbending under the law. Akin Demehin, director of policy at the American Hospital Association, said the penalties were “a game of chance” based on “badly flawed” measures.
Some hospitals insist they received penalties because they were more thorough than others in finding and reporting infections and other complications to the federal Centers for Medicare & Medicaid Services and the CDC.
“The all-or-none penalty is unlike any other in Medicare’s programs,” said Dr. Karl Bilimoria, vice president for quality at Northwestern Medicine, whose flagship Northwestern Memorial Hospital in Chicago was penalized this year. He said Northwestern takes the penalty seriously because of the amount of money at stake, “but, at the same time, we know that we will have some trouble with some of the measures because we do a really good job identifying” complications.
Other renowned hospitals penalized this year include Ronald Reagan UCLA Medical Center and Cedars-Sinai Medical Center in Los Angeles; UCSF Medical Center in San Francisco; Beth Israel Deaconess Medical Center and Tufts Medical Center in Boston; NewYork-Presbyterian Hospital in New York; UPMC Presbyterian Shadyside in Pittsburgh; and Vanderbilt University Medical Center in Nashville, Tennessee.
There were 2,430 hospitals not penalized because their patient complication rates were not among the top quarter. An additional 2,057 hospitals were automatically excluded from the program, either because they solely served children, veterans or psychiatric patients, or because they have special status as a “critical access hospital” for lack of nearby alternatives for people needing inpatient care.
The penalties were not distributed evenly across states, according to a KHN analysis of Medicare data that included all categories of hospitals. Half of Rhode Island’s hospitals were penalized, as were 30% of Nevada’s.
All of Delaware’s hospitals escaped punishment.Medicare excludes all Maryland hospitals from the program because it pays them through a different arrangement than in other states.
Over the course of the program, 1,978 hospitals have been penalized at least once, KHN’s analysis found. Of those, 1,360 hospitals have been punished multiple times and 77 hospitals have been penalized in all seven years, including UPMC Presbyterian Shadyside.
The Medicare Payment Advisory Commission, which reports to Congress, said in a 2019 report that “it is important to drive quality improvement by tying infection rates to payment.” But the commission criticized the program’s use of a “tournament” model comparing hospitals to one another. Instead, it recommended fixed targets that let hospitals know what is expected of them and that don’t artificially limit how many hospitals can succeed.
Although federal officials have altered other ACA-created penalty programs in response to hospital complaints and independent critiques — such as one focused on patient readmissions — they have not made substantial changes to this program because the key elements are embedded in the statute and would require a change by Congress.
Boston’s Beth Israel Deaconess said in a statement that “we employ a broad range of patient care quality efforts and use reports such as those from the Centers for Medicare & Medicaid Services to identify and address opportunities for improvement.”
UCSF Health said its hospital has made “significant improvements” since the period Medicare measured in assessing the penalty.
“UCSF Health believes that many of the measures listed in the report are meaningful to patients, and are also valid standards for health systems to improve upon,” the hospital-health system said in a statement to KHN. “Some of the categories, however, are not risk-adjusted, which results in misleading and inaccurate comparisons.”
Cedars-Sinai said the penalty program disproportionally punishes academic medical centers due to the “high acuity and complexity” of their patients, details that aren’t captured in the Medicare billing data.
“These claims data were not designed for this purpose and are typically not specific enough to reflect the nuances of complex clinical care,” the hospital said. “Cedars-Sinai continually tracks and monitors rates of complications and infections, and updates processes to improve the care we deliver to our patients.”
The American Hospital Association, other trade groups and individual hospitals filed petitions Feb. 10 asking the U.S. Supreme Court to reverse appeals court decisions in two cases involving outpatient payment cuts to hospitals.
One lawsuit hospitals are asking the Supreme Court to hear challenges HHS’ payment reductions in 2019 for certain outpatient off-campus provider-based departments.
Under the 2019 Medicare Outpatient Prospective Payment System final rule, CMS made payments for clinic visits site-neutral by reducing the payment rate for evaluation and management services provided at off-campus provider-based departments by 60 percent.
In an attempt to overturn the rule, the AHA, the Association of American Medical Colleges and dozens of hospitals across the nation sued HHS. They argued CMS exceeded its authority when it finalized the payment cut in the OPPS rule. They further claimed the site-neutral payment policy violates the Medicare statute’s mandate of budget neutrality.
HHS argued that under the Bipartisan Budget Act of 2015 it has authority to develop a method for controlling unnecessary increases in outpatient department services. Since “method” is not defined in the statute, the government argued its approach satisfies generic definitions of the term. U.S. District Judge Rosemary M. Collyer rejected that argument and set aside the regulation implementing the rate reduction in September 2019.
HHS filed an appeal in the case, and the appellate court reversed the lower court’s decision July 17.
The second lawsuit hospitals are asking the Supreme Court to hear challenges HHS’ nearly 30 percent cut to 2018 and 2019 outpatient drug payments for certain hospitals participating in the 340B Drug Pricing Program.
A district court sided with hospitals and found the payment reductions were unlawful. Two members of a three-judge panel of the U.S. Court of Appeals overturned that ruling in July.
The hospitals argue in both petitions that the Supreme Court should review the cases because of the “excessive deference” the appeals court gave to HHS’ interpretation of the respective governing statutes.
As the oft-cited 10,000 Baby Boomers continue to age into Medicare each day, Medicare Advantage (MA) enrollment keeps accelerating. The graphic above highlights growth in the MA ranks across the last decade, showing that enrollment has more than doubled since 2010. By the end of this year, an estimated 42 percent of Medicare beneficiaries will get their benefits through a private health insurer.
While seniors like MA plans for the growing number of supplemental benefits they can offer—which now include adult day care services, home-based palliative care, and in-home support services—health insurers are gravitating to these plans due to their attractive economics.
Health insurers’ average gross margin per member, per month (PMPM) for MA plans is significantly higher than in individual or group market plans, a spread that increased in 2020 due to reduced utilization. PMPM margins for MA plans were up an average of 35 percent through September 2020 compared to 2019.
Payers have been blanketing the market with plan options in recent years;the number of MA plans offered has increased 49 percent since 2017, although the MA market is increasingly concentrated. In spite of numerous headlines about venture-backed startups like Oscar, Bright Health Plan, and Devoted Health posting double- or triple-digit growth numbers, the MA market is still dominated by UnitedHealthcare and Humana, which together account for 44 percent of all MA enrollees nationwide.
Members of an influential congressional advisory committee on Medicare are torn on how best to regulate telehealth after the COVID-19 public health emergency, hinting at the difficulty Washington faces as it looks to impose guardrails on virtual care without restricting its use after the pandemic ends.
During a Thursday virtual meeting, the Medicare Payment Advisory Commission expressed its support of telehealth broadly, but many members noted snowballing use of the new modality could create more fraud and abuse in the system down the line.
Key questions of how much Medicare reimburses for telehealth visits and what type of visits are paid for won’t be easily answered, MedPAC commissioners noted. “This is a really, really difficult nut to crack,” Michael Chernew, MedPAC chairman and a healthcare policy professor at Harvard Medical School, said.
Dive Insight:
Virtual care has kept much of the industry running during the coronavirus pandemic, allowing patients to receive needed care at home. Much of this was possible due to the declaration of a public health emergency early 2020, allowing Medicare to reimburse for a greater swath of telehealth services and nixing other restrictions on virtual care.
However, much of that freedom is only in place for the duration of the public health emergency, leaving regulators and legislators scrambling to figure which new flexibilities they should codify, and which perhaps are best left in the past along with COVID-19.
It’s a tricky debate as Washington looks to strike a balance between keeping access open and costs low.
In a Thursday meeting, MedPAC debated a handful of policy proposals to try and navigate this tightrope. Analysts floated ideas like making some expansions permanent for all fee-for-service clinicians; covering certain telehealth services for all beneficiaries that can be received in their homes; and covering telehealth services if they meet CMS’ criteria for an allowable service.
But many MedPAC members were wary of making any concrete near-term policy changes, suggesting instead the industry should be allowed to test drive new telehealth regulations after COVID-19 without baking them in permanently.
“I don’t think what we’ve done with the pandemic can be considered pilot testing. I think a lot of this is likely to go forward no matter what we do because the gate has been opened, and it’s going to be really hard to close it,” Marjorie Ginsburg, founder of the Center for Healthcare Decisions, said. But “I see this just exploding into more fraud and abuse than we can even begin imagining.”
Paul Ginsburg, health policy chair at the Brookings Institution, suggested a two-year pilot of any changes after the public health emergency ends.
However, it would be “regressive” to roll back all the gains virtual care has made over the past year, according to Jonathan Perlin, CMO of health system HCA.
“These technologies are such a part of the environment that at this point, I fear [it] would be anachronistic not to accept that reality,” Perlin said.
Among other questions, commissioners were split on how much Medicare should pay for telehealth after the pandemic ends.
That parity debate is perhaps the biggest question mark hanging over the future of the industry. Detractors argue virtual care services involve lower practice costs, as remote physicians not in an office don’t need to shell out for supplies and staff. Paying at parity could distort prices, and cause fee-for-service physicians to prioritize delivering telehealth services over in-person ones, some commissioners warned.
Other MedPAC members pointed out a lower payment rate could stifle technological innovation at a pivotal time for the healthcare industry.
MedPAC analysts suggested paying lower rates for virtual care services than in-person ones, and paying less for audio-only services than video.
Commissioners agreed audio-only services should be allowed, but that a lower rate was fair. Commissioner Dana Gelb Safran, SVP at Well Health, suggested CMS should consider outlining certain services where video must be used out of clinical necessity.
Previously, telehealth services needed a video component to be reimbursed. Proponents argue expanded access to audio-only services will improve care access, especially for low-income populations that might not have the broadband access or technology to facilitate a video visit.
Another major concern for commissioners is how permanently expanding telehealth access would affect direct-to-consumer telehealth giants like Teladoc and Amwell. If all telehealth services delivered at home are covered, that could allow the private companies to “really take over the industry,” Larry Casalino, health policy chief in the Weill Cornell Department of Healthcare Policy and Research, said.
Because of the lower back-end costs for virtual care than in-office services, paying vendors the same rate as in-office physicians could drive a lot of brick-and-mortar doctors out of business, commissioners warned.